
Abstract
Pulmonary hypertension (PH) is responsible for premature death caused by progressive and severe heart failure. A simple, feasible, and reproducible animal model of PH is essential for the investigation of the pathogenesis and treatment of this condition. Previous studies have demonstrated that the vascular endothelial growth factor receptor 2 (VEGFR-2) inhibitor SU5416 combined with hypoxia could establish an animal model of PH. Here, we investigated whether SU5416 itself could induce PH in rats. The effects of SU5416 treatment followed by 5 weeks of normoxia were examined. Hemodynamic measurements and histological assessments of the pulmonary vasculature and the heart were conducted to evaluate the physiological and pathophysiological characteristics of PH. Compared with the control rats, the SU5416-treated rats showed significantly increased right ventricle systolic pressure, right ventricle mass, total pulmonary vascular resistance, and total pulmonary vascular resistance index, while the cardiac output and cardiac index were substantially decreased. Moreover, the degree of occlusion and the muscularization levels of the distal small pulmonary vessels and the medial wall thickness of larger vessels (OD > 50 μm) simultaneously increased. SU5416 inhibited pulmonary vascular endothelial cell apoptosis in rats, as shown by immunostaining of cleaved caspase-3. Furthermore, changes in the right ventricle, myocardial hypertrophy, myocardial edema, myocardial necrosis, striated muscle cell atrophy, vessel muscularization, neointimal occlusion, and increased collagen deposition were observed in the SU5416 group compared with the control group. Thus, treatment with SU5416 alone plus 5 weeks of normoxia could be sufficient to induce PH in rats, which may provide a good and convenient model for future investigation of PH.
Similar content being viewed by others


Introduction
Pulmonary hypertension (PH) is a severe disease characterized by progressive elevation in pulmonary vascular resistance (PVR) and a consequent increase in pulmonary arterial pressure, which leads to right-side heart failure and eventually death [1]. According to the latest Chinese guidelines released in 2018, a resting mean pulmonary artery pressure > 20 mmHg measured by right-sided heart catheterization is considered PH. To our knowledge, with the improvement of diagnostic techniques, PH is no longer a rare disease. Although people have a better understanding of the pathophysiology and pathogenesis of PH, the mechanism of PH is complicated, and the etiology is still not fully understood. Many studies have shown that multiple risk factors are involved in the pathogenesis of PH. The major pathological alteration of PH is pulmonary vascular remodeling, including changes in adventitia, media and intima thickness (plexiform lesion), muscularization of the distal vessels, and in situ thrombosis, resulting in arterial wall stiffening and luminal stenosis [2]. The pathological alterations in combination with sustained vasoconstriction give rise to elevated PVR. Currently, there are no noninvasive technologies for directly obtaining lung tissue samples from human patients. In most cases, tissues are obtained from end-stage patients who received lung transplantation or from deceased donors who were autopsied. Given the difficulty in isolating lung tissue samples directly from PH patients, well-established animal models are the primary source for mechanistic investigations of PH.
It has been reported that vascular endothelial growth factor (VEGF) and VEGF receptor 2 (VEGFR-2) are critical factors for endothelial cell (EC) survival [3, 4] and angiogenesis [5, 6]. VEGFR-2 is selectively and potently inhibited by the small molecule 3-(3,5-dimethyl-1H-pyrrol-2-ylmethylene)-1,3-dihydroindol-2-one (SU5416) [7], which was the first VEGFR-2 inhibitor to enter clinical trials for cancer therapy [8]. It has been well established that a single injection of SU5416 followed by 3–4 weeks of hypoxia or hypobaric hypoxia and then 2 or more weeks of normoxia can successfully establish a severe angioproliferative rat model of PH, and this model shows plexiform-like lesions and neointimal occlusion lesions that resemble the pulmonary arteriopathy of human PH in the late stages [9,10,11,12]. However, it remains controversial whether injection of SU5416 without hypoxia or hypobaric hypoxia treatment can lead to PH in rats. Here, we showed that a single injection of SU5416 followed by 5 weeks of normoxia could also establish PH in rats, which was characterized by the typical physiological and pathophysiological changes observed in PH. Our results indicated that a gene mutation caused by cellular regulation and/or VEGFR-2 gene dysfunction, which led to decreased VEGFR-2 expression, may at least partially be responsible for PH development. This model is easier to manipulate than the Sugen/hypoxia (SuHx) model but has similar disease severity and thus may be an ideal animal model for future investigation of PH.
Materials and methods
Reagents
The VEGFR inhibitor semaxinib (SU5416; HY-10374/CS-1225) was purchased from MedChem Express (Long Branch, NJ, USA). Dimethyl sulfoxide (DMSO) was purchased from GBCBIO Technologies, Inc. (Guangzhou, China). Antibodies for Hif-1α, PCNA and Hif-2α were purchased from Abcam (Cambridge, MA, USA). Anti-β-actin antibody was purchased from Santa Cruz (Dallas, TX, USA).
Animal treatment
All procedures were approved by the Animal Care and Use Committee of Guangzhou Medical University. Animals were housed at 24 °C in a 12-h light-dark cycle. Food and water were accessible ad libitum. Adult-specific pathogen-free male Sprague-Dawley rats (n = 10 per group, 190–220 g, provided by the Medical Experimental Animal Center of Guangdong Province) received a single subcutaneous injection of 20 mg/kg SU5416 (10 mg SU5416 dissolved in 1 mL of DMSO). The control rats were injected with an equal amount of vehicle (DMSO). Subsequently, all the rats were kept under normoxic conditions for 5 weeks.
Hemodynamic measurements
All rats were anesthetized with pentobarbital sodium (30 mg/kg, intraperitoneal injection), and then placed on controlled heating pads. Hemodynamic measurements were performed under normoxic conditions at room temperature. After the right jugular vein was found, a polyvinyl catheter was inserted into the right ventricle (RV) for measurement of RV systolic pressure (RVSP). The RVSP was measured instead of the pulmonary arterial systolic pressure owing to the undetectable pulmonary artery. Next, the skin along the right paraxial line was cut to expose the third and fourth ribs. Subsequently, the third and fourth ribs were removed to expose the heart and dissociated aortic root to ~0.2 cm. Then, a flowmeter probe was set in the dissected aortic segment to record the real-time blood flow waveforms using an MP150 physiological Recorder Acknowledge Software system, and the cardiac output (CO) was calculated accordingly. Next, the needle attached to the baroreceptor was inserted into the RV, and the RV time–pressure waveform was acquired by the software. Thirty seconds were needed for the system to reach equilibrium. In addition to RVSP and real-time blood flow waveforms, the cardiac index (CI) was calculated by the ratio of CO to body weight. Total pulmonary vascular resistance (TPR) was calculated by the ratio of RVSP to CO. The TPR index was estimated by the ratio of RVSP to CI. RV hypertrophy was evaluated by the wet weight ratio of the RV to the left ventricle + septum (RV/LV + S) and RV to body weight (RV/BW).
Histopathology
Intrapulmonary vessels were examined by the treatment of formalin-fixed and paraffin-embedded lung cross sections (5 μm) with various techniques, including hematoxylin and eosin (H&E) staining, Masson’s trichrome staining, Verhoeff–Van Gieson staining, and caspase-3 immunostaining. Heart tissue pathology was observed by H&E staining and Masson’s trichrome staining. For immunofluorescence staining, primary monoclonal antibodies against endothelial von Willebrand factor (vWF, Sigma, St. Louis, MO, USA), α-smooth muscle actin (α-SMA, Abcam) and CD31 (Abcam) and FITC-conjugated (excitation 488 nm) and CY3-conjugated secondary antibodies (excitation 543 nm) were applied. Finally, the slides were observed using a laser-scanning confocal fluorescence microscope (Nikon, Tokyo, Japan).
Morphological and histological analyses
Pulmonary vessel occlusion rate
Quantitative analysis of pulmonary vessel luminal obstruction was performed as described by Toba et al. with minor modifications [11]. Briefly, all small circular pulmonary vessels with an outer diameter (OD) < 100 μm per entire right posterior lobe cross section were counted. The vessels were assessed for occlusive lesions in Verhoeff-van Gieson-stained slides and scored as follows: no evidence of neointimal formation (grade 0), partial luminal occlusion (<50%; grade 1), and severe luminal occlusion (>50%; grade 2).
Muscularization
As most vessels < 50 μm in the control rats were nonmuscularized or partially muscularized, the degree of muscularization was assessed by counting all pulmonary vessels < 50 μm in each tissue section using immunofluorescence staining for vWF and α-SMA. The vessels were classified into three groups: nonmuscularized (only vWF-positive cells), partially muscularized (both vWF and α-SMA-positive cells but α-SMA not fully surrounding vWF), and fully muscularized (with both vWF and α-SMA-positive cells and α-SMA fully surrounding vWF).
Medial wall thickness
All the circular muscular arteries with an OD of 50–100 μm in each tissue section with immunofluorescence staining for vWF and α-SMA were analyzed. To minimize the measurement error, we used the medial wall thickness and medial wall area values to assess the medial wall thickness, i.e., the ratio of the circumference or area between the outer and inner α-SMA staining boundary to the circumference or area of the outer α-SMA staining boundary. The circumference and area were measured by the APP Case Viewer (3DHISTECH, Budapest, Hungary).
Right ventricle thickness
The cross-sectional area was used to assess the hypertrophy of the RV. We measured 50 H&E-stained cardiomyocytes from the right-side heart that were cross-sectioned, round, and not obviously small by iViewer 6.0 (Unic Technologies Inc., Beijing, China).
Western blot analysis
The rat distal pulmonary artery was sonicated in RIPA lysis buffer (Beyotime, Shanghai, China) containing protease inhibitor cocktail and phenylmethanesulfonylfluoride for protein extraction. Protein expression was measured by immunoblotting as described previously [13]. The protein lysate was quantified using the bicinchoninic acid protein assay (Pierce, Rockford, IL, USA). Protein aliquots were denatured by adding 5× SDS-PAGE loading buffer and heating at 100 °C for 5 min, and then resolved by 10% SDS-PAGE. Separated proteins were transferred onto polyvinylidene difluoride membranes (pore size 0.45 μM; Bio-Rad, Hercules, CA, USA). Membranes were blocked with 5% nonfat dry milk in Tris-buffered saline containing 0.2% Tween 20 and blotted with affinity-purified rabbit polyclonal antibodies specific for Hif-1α and Hif-2α or mouse monoclonal antibodies for PCNA and β-actin.
Statistical analysis
The statistical software SPSS 16.0 was used for analysis. Data are represented as the means ± SE. Body weight was analyzed using the Kruskal–Wallis test followed by the Mann–Whitney U-test with a Bonferroni correction. The pairwise comparison of means was conducted with Student’s t test if the data satisfied the test of normality by Shapiro–Wilk test and with the Mann–Whitney U-test if not. “n” is the number of animals from which pulmonary arteries or heart tissues were obtained. Differences were considered significant when P < 0.05 (*P < 0.05 vs the control group; **P < 0.01 vs the control group).
Results
Hemodynamic changes and body weight growth rate in the Sugen-treated rat model
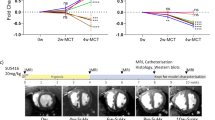
We found that at 5 weeks, the RVSP was significantly elevated in the SU5416 group compared with the control group (52.82 ± 5.31 and 26.90 ± 2.31 mmHg, respectively, P < 0.01). Here, the hypoxia- and Sugen-induced PH (SuHx) group, as the recognized animal model of PH, developed significant PH at 5 weeks, as determined by the increased RVSP (65.66 ± 8.20 mmHg, P < 0.01) (Fig. 1a-a, b). In contrast, the CO index at 5 weeks was 111.77 ± 8.02 ml/min (P < 0.05) in the SU5416 group and 104.91 ± 6.00 ml/min (P < 0.05) in the SuHx group, which was lower than that of the control group (159.58 ± 16.05 ml/min) (Fig. 1b-a, b). However, the TRPI was significantly increased in the SU5416 group compared with the control group (Fig. 1c, 1.15 ± 0.91 vs 0.10 ± 0.01, P < 0.05). The TRPI of the SU5416 group was 1.15 ± 0.91 and that of the SuHx group was 0.77 ± 0.07 (P < 0.01), while that of the control group was 0.10 ± 0.01. In addition, compared with that of the control group, the body weight growth rate was significantly decreased in the SuHx group (71.78 ± 4.61, P < 0.01), while there was no significant difference between the Sugen group (119.04 ± 5.30, P < 0.01) and the control group (125.32 ± 3.67) (Fig. 1d).

Comparison of hemodynamics and the body weight growth rate of the three groups. a Representative traces of right ventricular pressure (RVP) and summarized data (mean ± SE) showing right ventricular systolic pressure (RVSP) of each group. b Representative traces of cardiac output (CO) and summarized data (mean ± SE) showing the CO of each group (mean ± SE). c, d Summarized data (mean ± SE) showing TRPI and the BW growth rate of each group. (Animals were randomly allocated to one of the three groups: the control group (CTL) with no treatment, the SU5416-treated (SU5416) group, and the SU5416-treated following hypoxia (SuHx) group. There were 5–8 rats in each group. *P < 0.05, **P < 0.01.)
Small pulmonary arteries of the SU5416-treated rats show medial thickening
As shown in Fig. 2a, remodeled small PA with medial thickening was observed in the small PA of the SU5416-treated rats and the SuHx rats. In addition to medial thickening in the small PA, the ratio of vessel wall thickness (0.24 ± 0.03 vs 0.12 ± 0.01, P < 0.05, 0.34 ± 0.04 vs 0.12 ± 0.01, and P < 0.01, respectively) and the vessel wall area (0.54 ± 0.54 vs 0.21 ± 0.02, P < 0.05, 0.67 ± 0.57 vs 0.21 ± 0.02, and P < 0.05, respectively) were also significantly increased in the SU5416 group and the SuHx group compared with the control group (Fig. 2b).

Effects of SU5416 on pulmonary vascular medial wall thickness in rats. a (a, b, and c) Lung tissues from the control rats, the SU5416-treated rats, and the SuHx rats were stained with hematoxylin and eosin, which showed small PA with an OD of 50–100 μm. a (d, e, and f) Images showing the lung tissues from the control group, the SU5416 group, and the SuHx group representing small PA with an OD of 50–100 μm (red: α-SMA; green: vWF; blue: DAPI). b (a and b) Ratios of vessel wall thickness and vessel wall area in the small PA of each group with an OD of 50–100 μm. Representative pictures of one of five rats from the control group, the SU5416 group, and the SuHx group are shown. A total of 78 arteries in the SU5416 group, 80 in the SuHx group, and 50 in the control group were analyzed. (mean ± SE, *P < 0.05, **P < 0.01. n = 5–7)
Distal pulmonary vessels of the SU5416-treated rats exhibit increased pulmonary arterial occlusion
Because occlusion was more obvious in vessels with an OD < 50 μm, we only evaluated the degree of occlusion in this range. In total, 1550 vessels in twelve lobes from the three groups (SU5416 group, n = 5; SuHx group, n = 5; control group, n = 3) were assessed. More than half of the vessels in the SU5416 group developed some degree of luminal occlusion, while no luminal occlusion was observed in the control group. Approximately 13.5% and 45.3% of the vessels exhibited severe occlusion (grade 2) and 38.8% and 29.1% showed partial luminal occlusion (grade 1) in the SU5416 group and SuHx group, respectively (Fig. 3a, b).

Influence of SU5416 on distal pulmonary arterial occlusion and muscularization in rats. a Representative photomicrographs of PA in the rat cross sections from grades 0 to 2. a (a, c and e) H&E staining of the PA cross sections from the lung slides. a (b, d, and f) Verhoeff–Van Gieson staining of the PA cross sections from the lung slides. b Summarized data (mean ± SE) showing the comparison of pulmonary vascular luminal occlusion in vessels with OD < 50 μm among the control, SU5416, and SuHx groups. Grade 0 (no luminal occlusion). Grade 1 (luminal occlusion < 50%). Grade 2 (luminal occlusion > 50%). c Immunofluorescence images of the small PA labeled with α-SMA (green) and vWF (red) showing representative nonmuscularized, partially muscularized, and fully muscularized vessels. d Bar chart of pulmonary vascular muscularization of OD < 50 μm comparing the three groups. (*P < 0.05, **P < 0.01, SU5416 and SuHx compared with the control group; &#P < 0.05, SuHx compared with the control group, &#P < 0.05, SuHx compared with the SU5416 group. outer diameter (OD) < 50 μm. mean ± SE, n = 5)
Distal pulmonary vessels of the SU5416-treated rats exhibit a significant elevation in muscularization
Muscularization is another potential contributing factor to the rise in PVR and pulmonary arterial pressure. In total, 987 vessels (OD < 50 μm) in five lobes from the control group (n = 5) and 2600 vessels from the SU5416 group (n = 5) and SuHx group (n = 5) were assessed. As there were some difficulties in distinguishing nonmuscularized vessels in other vWF-positive tissues, the nonmuscularized group may have been underestimated in these three groups. As shown in Fig. 3c, a dramatic enhancement in muscularization was observed in the distal PA of the SU5416-treated rats and the SuHx rats. Most of the vessels in the control group were nonmuscularized (22.9%), and fully muscularized vessels accounted for only 15%, whereas the proportion of muscularized vessels (both partially and fully) was 94.2% and 97.5% in the SU5416 group and SuHx group, respectively (Fig. 3d).
Increased apoptosis of pulmonary vascular endothelial cells in the SU5416-treated rats
It has been reported that VEGFR-2 blockade and VEGFR-2 blockade combined with hypoxia led to apoptosis of pulmonary vascular ECs in vitro and in vivo [9, 14]; thus, we examined whether pulmonary vascular EC apoptosis occurs in this model. Immunostaining of the lungs from the SU5416-treated rats and the control rats indicated that caspase-3 was mainly increased in the intima layer (endothelium) (Fig. 4), which revealed that there was increased apoptosis of the pulmonary vascular ECs in the rats exposed to SU5416 treatment.

Effects of SU5416 on endothelial cell apoptosis shown by caspase-3 immunohistochemistry. An arrow indicates caspase-3-positive endothelium. a (a, b) Representative vessels of OD < 20 μm in a comparison of the control and SU5416 groups. a (c, d) Representative vessels of OD < 50 μm in a comparison of the control and SU5416 groups. b Summarized data (mean ± SE) showing the comparison of the mean optical density of caspase-3 in ECs from the control and SU5416-treated rats. **P < 0.01
Pulmonary arteries of the SU5416-treated rats express a strong elevation in PCNA, Hif-1α, and Hif-2α
To further investigate the regulation of medial thickening and increased apoptosis of the intima observed in the SU5416-treated rats, we detected the expression of related proteins. In the pulmonary arteries of the SU5416-treated rats, the expression of PCNA was strongly upregulated compared with that of the control group (Fig. 5), which indicated increased proliferation of pulmonary artery smooth muscle cells (PASMCs). Hypoxia is an important factor for muscularization or medial wall thickness, and thus, we tested Hif-1α and Hif-2α expression in the pulmonary arteries by western blotting. The protein expression levels of Hif-1α and Hif-2α were higher in the pulmonary arteries of the SU5416 model than those of the control group (Fig. 5).

Effects of SU5416 on PCNA, Hif-1α, and Hif-2α protein expression in PA. Representative western blot images (a) and summarized data (b) (mean ± SE; n = 6 in each group) showing the protein levels of PCNA, Hif-1α, and Hif-2α in the PA isolated from the rats treated with or without SU5416. **P < 0.01, compared with the control group
The influence of the right ventricle in the SU5416-treated rats
Similar to the observations in the SuHx group, myocardial edema, myocardial necrosis, and striated muscle cell atrophy were detected in the SU5416 group compared with the control group (Fig. 6a, b). Furthermore, the RV showed more deposition of collagen in the SU5416 group, as well as the SuHx group, than the control group (Fig. 6a, b). In addition, compared with those of the control group, the cross-sectional areas of right ventricular cardiomyocytes and RV/(LV + S) were increased in both the SU5416 group and the SuHx group (Fig. 6c, d).

Influence of SU5416 on right ventricle lesions in rats. a Right ventricles from the control rats, the SU5416-treated rats, and the SuHx rats were stained with H&E, showing cardiomyocyte hypertrophy, myocardial edema, myocardial necrosis, and striated muscle cell atrophy in the SU5416 and SuHx groups compared with the control group. b Right ventricles from the three groups were stained with Masson’s trichrome showing more deposition of collagen in the SU5416 and SuHx groups than the control group. c Summarized data (mean ± SE) showing the comparison of the cross-sectional area of right ventricle cardiomyocytes among the control, SU5416, and SuHx groups. (There were 5–6 rats in each group, *P < 0.05, **P < 0.01). d Summarized data (mean ± SE) showing the comparison of RV/(LV + S) among the control, SU5416, and SuHx groups. (There were 8–13 rats in each group. *P < 0.05)
The development of pulmonary vascular pathology and hemodynamic changes in the rats treated with SU5416 following normoxia
To test whether SU5416 following normoxia contributes to the development of PH, we exposed the rats treated with SU5416 to normoxia for 1, 3, 5, and 8 weeks. As shown in Fig. 7a, vascular remodeling, especially the thickness of the medial layers, was detected after 3 weeks and was significantly aggravated in the subsequent weeks (Fig. 7a). Elevation in PVSP was clearly evident in the SU5416-treated rats after 3 weeks, and RV/(LV + S) was obviously increased after 5 weeks (Fig. 7b, c).

Time course changes in pulmonary vascular pathology, RVSP, and heart weight ratios in the rats at 1, 3, 5, and 8 weeks after Sugen 5416 injection. a H&E staining of the lungs from the SU5416-treated rats showing small PA with an OD of 50–100 μm. b, c Comparisons of RVSP and RV/(LV + S) between the control and SU5416 groups after 1, 3, 5, and 8 weeks are shown. There were 5–6 rats in each group. *P < 0.05, **P < 0.01
Discussion
Previous studies have reported three rodent models that are frequently used for preclinical investigation of PH: chronic hypoxia-induced PH (CHPH), monocrotaline (MCT)-induced PH (MCT-PH), and SuHx-induced PH (SuHx-PH). The CHPH model was produced to investigate type 3 PH due to lung diseases and/or hypoxia. MCT has been reported to cause acute lung injury [15, 16], interstitial pulmonary fibrosis [17, 18], necrotizing pulmonary arteritis [19, 20], myocarditis [21], and hepatic veno-occlusive disease [22, 23]. The MCT-PH model represents a type of severe PH; however, its strong toxicity and unique pathological changes in the lung differ from those observed in PH patients and the other PH models, limiting the use of this model in the preclinical investigation of the PH mechanism. Recently, it has been reported that the SuHx-PH model, which includes a single injection of SU5416 plus 3–4 weeks of hypoxic exposure, followed by 2 weeks of normoxic exposure, caused neointimal occlusive lesions and plexiform lesions in rats, which resemble the pathology of severe PH patients [9,10,11, 24]. Therefore, the SuHx-PH rat model is widely used to mimic the pathogenesis of severe PH. In our study, we observed that a single injection of SU5416 followed by 5 weeks of normoxic exposure (without hypoxia) was sufficient to induce PH in rats, which was characterized by significantly increased pulmonary arterial pressure, occlusive lesions in pulmonary vessels, RV hypertrophy, and heart failure. Notably, on the one hand, PH patients are not exposed to hypoxic conditions, indicating that the characteristics of the SU5416 plus normoxia group are closer to those in the actual situation; on the other hand, compared with the SuHx-PH model, the Sugen plus normoxia model eliminates the influence of hypoxia, which is a factor that contributes to PH, thus enabling us to better elucidate the contribution and mechanism of dysfunctional VEGF signaling in the pathogenesis of PH, especially in the process of neointimal occlusive lesions, pulmonary vascular muscularization, and medial wall remodeling. This study provides an ideal model for the study of PH development, especially for the type with severe endothelial dysfunction and abnormality of the PA, and will specifically promote the development of effective treatments against these types of PH. Finally, this model is more convenient to establish and more reliable and stable than the previous model, as only one element needs to be considered.
The classical SuHx-PH model was established by a single injection of SU5416 combined with 3 weeks of hypoxia exposure and 2 weeks of normoxic exposure [12]. The symptoms become more severe with longer normoxic exposure since plexiform lesions could develop after 10–11 weeks of normoxia [10, 11]. This model may be associated with the death of pulmonary ECs, followed by abnormal extensive proliferation of apoptosis-resistant cells, which develop into complex vascular lesions [9]. In fact, early in 2001, Taraseviciene-Stewart et al. showed that there was a significant increase in pulmonary arterial pressure and medial wall thickness in the SU5416-treated rats followed by normoxia compared with the control rats at sea level [9]. Consistently, Ciuclan et al. revealed that the pulmonary arterial pressure was higher in the SU5416/normoxia group than in the control group in mice but was not significant [25]. Multiple studies have indicated that VEGF is an essential factor for EC mitogenesis and survival [7, 26], and blockage of the VEGF signaling pathway (by specific VEGFR inhibitors such as SU5416) induces severe EC apoptosis [3, 27, 28]. Previous studies found that persistent blockade of the VEGF receptor induced apoptosis of alveolar cells, which eventually led to emphysema in rats [29, 30]. As mentioned above, apoptosis of PAECs and pulmonary endothelial dysfunction were observed in both the CHPH and SuHx rat models [9]. These results are consistent with our findings of obvious EC apoptosis in the lungs of the rats treated with SU5416 plus 5 weeks of normoxic exposure compared with the control rats, suggesting that persistent VEGFR-2 blockade by SU5416 without hypoxia is sufficient for inducing EC apoptosis and PA endothelial dysfunction during PH. We hypothesize that increased apoptosis of ECs plays a vital role in the development of SU5416-induced PH. VEGFR-2 inhibited by SU5416 caused significant EC apoptosis and dysfunction, leading to decreased production of nitric oxide (NO) [31,32,33] or prostacyclin [33], which subsequently results in uncontrolled contraction and proliferation of vascular smooth muscle cells [14] and finally promotes the thickening and remodeling of PA and vasoconstriction, contributing to the development of severe PH.
Considering our data, over 50% of the distal vessels (OD < 50 μm) had occlusive lesions to some extent (grades 1 and 2) in the SU5416 model, illustrating that vascular luminal occlusion in pulmonary vessels may be the reason for the elevation of RVSP and TRPI. In addition, according to the immunofluorescence staining of vWF and α-SMA in lung tissues from the SU5416 group, the proliferation of both PASMCs and PAECs contributed to pulmonary vascular remodeling. These results are similar to the data reported by Toba et al. [11]. Severely occluded vessels with plexiform-type neointima in the OD size range of 50–100 μm were observed at the 13-week time point in the SU5416/hypoxia model. In contrast, more neointimal lesions in distal smaller vessels (OD < 50 μm) were detected in our 5-week SU5416 model, while less occlusive lesions were observed in larger vessels with an OD size range of 50–100 μm than those in the controls. Further exploration is needed to determine whether large vessels develop occlusive lesions with longer normoxia exposure times. Furthermore, in the SU5416 model, there were more muscularized vessels in the distal vessels (OD < 50 μm) compared with those in the control group, and the medial wall was significantly thicker in the arteries with an OD size range of 50–100 μm. Vasoconstriction and pulmonary vascular luminal stenosis are affected by the degree of muscularization and medial wall thickness, which are related to PASMC proliferation. In contrast to the systemic circulatory system, vasoconstriction occurs in pulmonary vessels under hypoxic conditions [34]. Muscularization or medial wall thickness makes pulmonary vessels more vulnerable to hypoxia-induced pulmonary vasoconstriction. In the SU5416 model, Hif-1α and Hif-2α were upregulated in the pulmonary arteries, which may indicate the occurrence of hypoxia in the PA of SU5416 rats. However, further research is required to determine whether hypoxia occurs in the PA of the SU5416 model, as Hif-1α and Hif-2α are not only upregulated by hypoxic conditions. We also compared the hemodynamics and pulmonary vessel remodeling of the mono-SU5416-treated rats and the rats that underwent traditional SU5416 treatment following hypoxic exposure at 1, 3, 5, and 8 weeks. Our observations indicated that the development and severity of PH in the SU5416 group was less severe than that of the SuHx group, but the pathologic changes of the SU5416 group were largely similar to those observed in clinical PH patients, suggesting that the mono-SU5416 treatment group might also be an ideal model to mimic clinical PH pathology, with less severe symptoms and lower mortality than those of the SuHx group.
As RV function is the most important determinant of longevity in patients with PH, we carried out hemodynamics and histological assessments of the heart. RV/LV + S was significantly increased in the SU5416 model, while the CO was decreased in this model. These results suggested that RV dysfunction developed in the SU5416 model. Further RV histological assessments showed that myocardial hypertrophy, myocardial edema, myocardial necrosis, and striated muscle cell atrophy developed in the RV in the SU5416 model. There was more collagen deposition in the RV in the SU5416 model than the controls. This finding confirmed that RV dysfunction was established in the SU5416 model. Therefore, not only elevated pulmonary arterial pressure but also the VEGFR-2 inhibitor SU5416 itself may contribute to RV dysfunction. Cardiac hypertrophy occurs as an adaptive response to increased workload aiming to maintain cardiac function [35]. However, prolonged cardiac hypertrophy causes heart failure. In general, the mechanisms of heart dysfunction are unclear, but they are considered to be related to cardiac fibrosis, cardiomyocyte apoptosis, and a mismatch between the number of capillaries and the size of cardiomyocytes [36]. As VEGF is an angiogenic inducer, VEGFR-2 inhibitors may affect angiogenesis in the heart. Overall, RV hypertrophy, cardiomyocyte apoptosis, atrophy and stenosis, together with cardiac collagen deposition and vascular luminal occlusion in the RV, contributed to RV dysfunction.
Conclusion
In this study, rats treated with a single injection of the VEGFR-2 blocker SU5416, followed by 5 weeks of normoxic exposure, exhibited neointimal occlusive PH, corresponding to human PH. Neointimal luminal occlusion (OD < 50 μm), muscularization of nonmuscularized pulmonary vessels and medial wall thickness of muscularized pulmonary vessels may have contributed to the elevated RVSP and TRPI. Muscularization and medial wall thickness of pulmonary vessels may be associated with apoptosis of pulmonary ECs. This hypothesis is based on the proliferation of pulmonary VSMCs shown by the upregulation of PCNA observed in PH, together with previous studies demonstrating that apoptosis of pulmonary ECs was associated with the proliferation of pulmonary VSMCs. RV hypertrophy, cardiomyocyte apoptosis, atrophy, and stenosis, together with cardiac collagen deposition and vascular luminal occlusion in the right heart, contributed to the decreased CO/CI. In summary, rats with a single injection of the VEGFR-2 blocker SU5416, followed by 5 weeks of normoxic exposure, exhibited the characteristics of human PH. Furthermore, the lack of hypoxia treatment made it a more appropriate preclinical model of occlusive PH than the SuHx-PH model.
References
Hoeper MM, Bogaard HJ, Condliffe R, Frantz R, Khanna D, Kurzyna M, et al. Definitions and diagnosis of pulmonary hypertension. Turk Kardiyol Dern Ars. 2014;42 Suppl 1:55–66.
Kuhr FK, Smith KA, Song MY, Levitan I, Yuan JX. New mechanisms of pulmonary arterial hypertension: role of Ca(2)(+) signaling. Am J Physiol Heart Circ Physiol. 2012;302:H1546–62.
Gerber HP, McMurtrey A, Kowalski J, Yan M, Keyt BA, Dixit V, et al. Vascular endothelial growth factor regulates endothelial cell survival through the phosphatidylinositol 3’-kinase/Akt signal transduction pathway. Requirement for Flk-1/KDR activation. J Biol Chem. 1998;273:30336–43.
Sundberg C, Nagy JA, Brown LF, Feng D, Eckelhoefer IA, Manseau EJ, et al. Glomeruloid microvascular proliferation follows adenoviral vascular permeability factor/vascular endothelial growth factor-164 gene delivery. Am J Pathol. 2001;158:1145–60.
Voelkel NF, Gomez-Arroyo J. The role of vascular endothelial growth factor in pulmonary arterial hypertension. The angiogenesis paradox. Am J Respir Cell Mol Biol. 2014;51:474–84.
Baluk P, Lee CG, Link H, Ator E, Haskell A, Elias JA, et al. Regulated angiogenesis and vascular regression in mice overexpressing vascular endothelial growth factor in airways. Am J Pathol. 2004;165:1071–85.
Fong TA, Shawver LK, Sun L, Tang C, App H, Powell TJ, et al. SU5416 is a potent and selective inhibitor of the vascular endothelial growth factor receptor (Flk-1/KDR) that inhibits tyrosine kinase catalysis, tumor vascularization, and growth of multiple tumor types. Cancer Res. 1999;59:99–106.
Glade-Bender J, Kandel JJ, Yamashiro DJ. VEGF blocking therapy in the treatment of cancer. Expert Opin Biol Ther. 2003;3:263–76.
Taraseviciene-Stewart L, Kasahara Y, Alger L, Hirth P, Mc Mahon G, Waltenberger J, et al. Inhibition of the VEGF receptor 2 combined with chronic hypoxia causes cell death-dependent pulmonary endothelial cell proliferation and severe pulmonary hypertension. FASEB J. 2001;15:427–38.
Abe K, Toba M, Alzoubi A, Ito M, Fagan KA, Cool CD, et al. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation. 2010;121:2747–54.
Toba M, Alzoubi A, O’Neill KD, Gairhe S, Matsumoto Y, Oshima K, et al. Temporal hemodynamic and histological progression in Sugen5416/hypoxia/normoxia-exposed pulmonary arterial hypertensive rats. Am J Physiol Heart Circ Physiol. 2014;306:H243–50.
Nicolls MR, Mizuno S, Taraseviciene-Stewart L, Farkas L, Drake JI, Al Husseini A, et al. New models of pulmonary hypertension based on VEGF receptor blockade-induced endothelial cell apoptosis. Pulm Circ. 2012;2:434–42.
Wang J, Chen Y, Lin C, Jia J, Tian L, Yang K, et al. Effects of chronic exposure to cigarette smoke on canonical transient receptor potential expression in rat pulmonary arterial smooth muscle. Am J Physiol Cell Physiol. 2014;306:C364–73.
Sakao S, Taraseviciene-Stewart L, Wood K, Cool CD, Voelkel NF. Apoptosis of pulmonary microvascular endothelial cells stimulates vascular smooth muscle cell growth. Am J Physiol Lung Cell Mol Physiol. 2006;291:L362–8.
Schermuly RT, Kreisselmeier KP, Ghofrani HA, Yilmaz H, Butrous G, Ermert L, et al. Chronic sildenafil treatment inhibits monocrotaline-induced pulmonary hypertension in rats. Am J Respir Crit Care Med. 2004;169:39–45.
Klein M, Schermuly RT, Ellinghaus P, Milting H, Riedl B, Nikolova S, et al. Combined tyrosine and serine/threonine kinase inhibition by sorafenib prevents progression of experimental pulmonary hypertension and myocardial remodeling. Circulation. 2008;118:2081–90.
Molteni A, Ward WF, Ts’ao CH, Solliday NH, Dunne M. Monocrotaline-induced pulmonary fibrosis in rats: amelioration by captopril and penicillamine. Proc Soc Exp Biol Med. 1985;180:112–20.
Molteni A, Ward WF, Ts’ao CH, Solliday NH. Monocrotaline-induced cardiopulmonary damage in rats: amelioration by the angiotensin-converting enzyme inhibitor CL242817. Proc Soc Exp Biol Med. 1986;182:483–93.
Wilson DW, Segall HJ, Pan LC, Lame MW, Estep JE, Morin D. Mechanisms and pathology of monocrotaline pulmonary toxicity. Crit Rev Toxicol. 1992;22:307–25.
Kay JM, Harris P, Heath D. Pulmonary hypertension produced in rats by ingestion of Crotalaria spectabilis seeds. Thorax. 1967;22:176–9.
Campian ME, Hardziyenka M, de Bruin K, van Eck-Smit BL, de Bakker JM, Verberne HJ, et al. Early inflammatory response during the development of right ventricular heart failure in a rat model. Eur J Heart Fail. 2010;12:653–8.
Mingatto FE, Maioli MA, Bracht A, Ishii-Iwamoto EL. Effects of monocrotaline on energy metabolism in the rat liver. Toxicol Lett. 2008;182:115–20.
Gomez-Arroyo JG, Farkas L, Alhussaini AA, Farkas D, Kraskauskas D, Voelkel NF, et al. The monocrotaline model of pulmonary hypertension in perspective. Am J Physiol Lung Cell Mol Physiol. 2012;302:L363–9.
de Raaf MA, Schalij I, Gomez-Arroyo J, Rol N, Happe C, de Man FS, et al. SuHx rat model: partly reversible pulmonary hypertension and progressive intima obstruction. Eur Respir J. 2014;44:160–8.
Ciuclan L, Bonneau O, Hussey M, Duggan N, Holmes AM, Good R, et al. A novel murine model of severe pulmonary arterial hypertension. Am J Respir Crit Care Med. 2011;184:1171–82.
Millauer B, Shawver LK, Plate KH, Risau W, Ullrich A. Glioblastoma growth inhibited in vivo by a dominant-negative Flk-1 mutant. Nature. 1994;367:576–9.
Gerber HP, Hillan KJ, Ryan AM, Kowalski J, Keller GA, Rangell L, et al. VEGF is required for growth and survival in neonatal mice. Development. 1999;126:1149–59.
Alon T, Hemo I, Itin A, Pe’er J, Stone J, Keshet E. Vascular endothelial growth factor acts as a survival factor for newly formed retinal vessels and has implications for retinopathy of prematurity. Nat Med. 1995;1:1024–8.
Kasahara Y, Tuder RM, Taraseviciene-Stewart L, Le Cras TD, Abman S, Hirth PK, et al. Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J Clin Investig. 2000;106:1311–9.
Jiang X, Li T, Sun J, Liu J, Wu H. SETD3 negatively regulates VEGF expression during hypoxic pulmonary hypertension in rats. Hypertens Res. 2018;41:691–8.
Liang X, Xu F, Li X, Ma C, Zhang Y, Xu W. VEGF signal system: the application of antiangiogenesis. Curr Med Chem. 2014;21:894–910.
Morbidelli L, Chang CH, Douglas JG, Granger HJ, Ledda F, Ziche M. Nitric oxide mediates mitogenic effect of VEGF on coronary venular endothelium. Am J Physiol. 1996;270:H411–5.
Murohara T, Horowitz JR, Silver M, Tsurumi Y, Chen D, Sullivan A, et al. Vascular endothelial growth factor/vascular permeability factor enhances vascular permeability via nitric oxide and prostacyclin. Circulation. 1998;97:99–107.
Lumb AB, Slinger P. Hypoxic pulmonary vasoconstriction: physiology and anesthetic implications. Anesthesiology. 2015;122:932–46.
Frey N, Olson EN. Cardiac hypertrophy: the good, the bad, and the ugly. Annu Rev Physiol. 2003;65:45–79.
Sano M, Minamino T, Toko H, Miyauchi H, Orimo M, Qin Y, et al. p53-induced inhibition of Hif-1 causes cardiac dysfunction during pressure overload. Nature. 2007;446:444–8.
Acknowledgements
This work was supported in part by grants from the National Natural Science Foundation of China (81630004, 81800061, 81970057, 81520108001, 81770043, 81800057, 81700048, 81900046, and 81800054), the Department of Science and Technology of China Grants (2016YFC0903700, 2016YFC1304102, and 2018YFC1311900), Changjiang Scholars and Innovative Research Team in University grant IRT0961, the Local Innovative and Research Teams Project of Guangdong Pearl River Talents Program (2017BT01S155), Guangdong Department of Science and Technology Grants (2016A030311020, 2016A030313606, 2017A020215114, 2019A1515010615, 2019A050510046, 2019A1515010672, and 2019B030316028), a Guangzhou Department of Education Scholarship (1201630095), the Guangdong Province Universities, the Colleges Pearl River Scholar Funded Scheme of China, the Inner Mongolia Autonomous Region Science and Technology Innovation Guidance Project and the Inner Mongolia Autonomous Region Science and Technology Project (20160298), and the Independent Project of State Key Laboratory of Respiratory Disease (SKLRD-QN-201704). This work was also supported in part by the grants from the National Heart, Lung, and Blood Institute of the National Institutes of Health (R35HL135807 and U01HL125208) and an Actelion ENTELLIGENCE Young Investigator Award.
Author information
Authors and Affiliations
Contributions
YC, MK, JC, GZ, HC, HY, YL, YZ and QZ performed the experiments; WH, JL, CH and QJ analyzed the data; XL and YC prepared the figures; SL and KY drafted the manuscript; WL, and JW were responsible for the conception and design of the research; YC, MK, HT, XD, GZ, and JW edited and revised the manuscript; and JW approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chen, Y., Kuang, M., Liu, S. et al. A novel rat model of pulmonary hypertension induced by mono treatment with SU5416. Hypertens Res 43, 754–764 (2020). https://doi.org/10.1038/s41440-020-0457-6
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-020-0457-6
Keywords
This article is cited by
-
Comprehensive chemical analysis of polyphenols in the ethyl acetate extract from the roots of Ephedra sinica Stapf and evaluation of its therapeutic effects on SU5416/hypoxia-induced pulmonary arterial hypertension rats
Bioresources and Bioprocessing (2025)
-
Echocardiographic evaluation of right heart failure which might be associated with DNA damage response in SU5416-hypoxia induced pulmonary hypertension rat model
Respiratory Research (2023)
-
The need for hypoxic exposure in experimental PAH - Comment on Chen et al.: a novel rat model of pulmonary hypertension induced by mono treatment with SU5416
Hypertension Research (2020)
