
Abstract
Lifetime risk (LTR) evaluates the absolute risk of developing a disease during the remainder of one’s life. It can be a useful tool, enabling the general public to easily understand their risk of stroke. No study has been performed to determine the LTR of cardiovascular disease in patients with chronic kidney disease (CKD) with or without hypertension; therefore, we performed this study in an Asian population. We followed 1525 participants (66.0% women; age 63.1 years) in the general population of Ohasama, Japan. We defined CKD as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 and/or proteinuria. Hypertension was defined as a systolic/diastolic blood pressure ≥140/≥90 mmHg and/or the use of antihypertensive medication. We calculated the sex-specific LTR of stroke adjusted for the competing risk of death. During the mean follow-up period of 16.5 years, a first stroke occurred in 238 participants. The 10-year risk of stroke at the age of 45 years was 0.0% for men and women. The LTRs of stroke at the index age of 45 years (men/women) were 20.9%/14.5% for participants without CKD and hypertension, 34.1%/29.8% for those with CKD but not hypertension, 37.9%/27.3% for those with hypertension but not CKD, and 38.4%/36.4% for those with CKD and hypertension. The LTRs of stroke tended to be higher in younger participants than in older participants with CKD and/or hypertension. CKD contributed to the LTR of stroke, as did hypertension. The prevention of CKD and hypertension can reduce the LTR of stroke, especially in young populations.
Similar content being viewed by others

Introduction
Stroke is one of the leading causes of death and disability worldwide [1, 2]. Hypertension is a major risk factor for stroke [3, 4]. Chronic kidney disease (CKD) and decreased kidney function also increase the risk of stroke [5, 6]. Since CKD and hypertension are related to each other [7, 8], a study investigating the combination of CKD and hypertension is needed to accurately estimate the risk of stroke.
As an index of risk, the absolute risk is more easily understood by the general population than the relative risk [9]. Although short-term risks such as the 10-year risk have been widely used, short-term risk estimates tend to be low in young people [10] and could be insufficient to encourage young people to adopt healthy lifestyles or initiate treatment.
Lifetime risk (LTR) is the cumulative incidence of disease from a given age (index age) until the end of life and estimates the absolute risk of developing a disease during the remainder of one’s life [11]. LTR can evaluate the long-term risk resulting from the accumulation of damage due to the presence of risk factors such as CKD and hypertension. LTR can be beneficial for communicating the risk of stroke to the general public, thereby contributing to the early prevention of stroke [12]. The atherosclerotic cardiovascular disease (ASCVD) risk estimator, which was released by the American College of Cardiology and is used for risk stratification [13], calculates the LTR for each patient aged 40–75 years. However, there is no information about the LTR of cardiovascular disease in patients with CKD. Although the LTR of stroke in patients with hypertension was reported in previous epidemiological studies [14,15,16,17,18], that estimate could have been affected by kidney dysfunction.
Asian populations have a higher risk of end-stage kidney disease [19] and stroke [20] than Western populations. Therefore, we examined the LTR and intermediate-term risk of stroke stratified by the combination of CKD and hypertension in a general Asian population.
Methods
Study population
This study was a part of the Ohasama study, which is an ongoing cohort study that began in 1986 in Ohasama, Iwate Prefecture, Japan. Most of the adult population is engaged in growing fruit, and the remaining adults work in offices or factories in Ohasama or neighboring cities. The climate, nutritional habits and per capita income are similar to those in other areas of northeastern Japan. The socioeconomic and demographic characteristics of this region and the details of the study have been described previously [5, 21,22,23]. The Institutional Review Boards of Teikyo University, Tohoku Medical and Pharmaceutical University, and Tohoku University approved the study protocol.
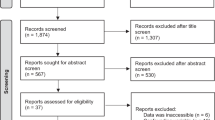
The flowchart of participant selection is shown in Supplementary Fig. 1. In Japan, annual health checkups are available to individuals aged ≥35 years, including farmers, self-employed individuals, pensioners, and dependents. The annual health checkup data collected between 1992 and 1997 were used in the present analysis and set as the baseline exposure. We used the data obtained during the first year of the annual health check-up as baseline data. In 1995, the midpoint of the baseline study period, the population of Ohasama residents aged ≥35 years was 5013. During the baseline period, 2,934 individuals participated in annual health checkups and gave informed consent for participation in the present study. Eighty-six participants with a history of stroke were excluded. In addition, we excluded 32 participants who were lost to follow-up under 45 years of age (25 transfers, 1 stroke, and 6 deaths). We excluded 1291 individuals because of the lack of data for the level of serum creatinine (SCr) (n = 796), the presence of proteinuria (n = 12), or the use of antihypertensive treatment (n = 483). As a result, 1,525 participants were analyzed. Although SCr was measured in participants aged ≥60 years, the test was only performed on request for residents aged <60 years. Compared with the group of participants aged <60 years who requested SCr measurement, the group of participants who did not request those measurements were younger; had higher proportions of participants who were men, smokers, and drinkers; had a lower proportion of participants with proteinuria; and had a higher proportion of participants who had hypercholesterolemia (Supplementary Table 1).
Data collection
Information on smoking status, alcohol consumption, the administration of antihypertensive medication, diabetes mellitus history, and hypercholesterolemia was verified in medical records or through a questionnaire survey. We classified smoking status and alcohol consumption into current or former/never. In accordance with the guidelines of the Japan Diabetes Society (JDS), we defined diabetes mellitus based on a non-fasting blood glucose level ≥11.1 mmol/L (≥200 mg/dL), a fasting blood glucose level ≥7.0 mmol/L (≥126 mg/dL), an HbA1c level (JDS) ≥6.1%, treatment with insulin/oral hypoglycemic agents, or a history of diabetes mellitus. Hypercholesterolemia was defined based on a total cholesterol level ≥5.7 mmol/L (≥220 mg/dL), the use of anti-hypercholesterolemia agents, or a history of hypercholesterolemia. Since the numbers of participants who lacked data for diabetes (n = 11 [0.72%]) and hypercholesterolemia (n = 7 [0.46%]) were small, we classified these participants into the groups without diabetes or hypercholesterolemia. Blood pressure was measured twice by trained nurses at local medical centers using a semiautomatic blood pressure measuring device in the seated position after resting for ≥2 min. The average of the two readings was recorded. Hypertension was defined by a systolic blood pressure (SBP) ≥140 mmHg, a diastolic blood pressure (DBP) ≥90 mmHg, and/or the use of antihypertensive medication [3, 4]. In the sensitivity analysis, we assessed the LTR of stroke stratified by CKD and hypertension using the threshold of SBP/DBP ≥130/≥80 mmHg, which was used for the diagnosis of hypertension in the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) hypertension guidelines [24].
We determined renal function according to the estimated glomerular filtration rate (eGFR) calculated from the SCr using the modified Japanese equation: eGFR (mL/min/1.73 m2) = 194 × (SCr in enzymatic method)−1.094 × age−0.287 (×0.739, if female) [25]. We also calculated the eGFR using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation modified for the Japanese population with the Japanese coefficient, as follows: eGFRCKD-EPI (mL/min/1.73 m2) = 141 × min (Cr/κ, 1)α × max (Cr/κ, 1)−1.209 × 0.993Age × 1.018 (if female) × 0.813 (Japanese coefficient). κ and α are 0.7 and −0.329 in females and 0.9 and −0.411 in males, respectively; min indicates the minimum SCr/κ or 1; and max indicates the maximum SCr/κ or 1 [26, 27]. Proteinuria was determined with a dipstick spot test for urine; the results were considered positive when the dipstick showed 1+ or more, which corresponds to a urinary protein level above 30 mg/dL. We defined CKD as an eGFR <60 mL/min/1.73 m2 and/or proteinuria.
Follow-up and outcomes
Follow-up was continued until the occurrence of one of the following censoring events: stroke incidence, death, loss to follow-up due to relocation, or the end of the follow-up period (August 31, 2014). Stroke incidence was determined by reviewing the Stroke Registration System of Iwate Prefecture, death certificates, National Health Insurance receipts, and questionnaires sent to each household at the time of health checkups. This information was confirmed by checking the medical charts in hospitals and clinics around Ohasama town, including the Ohasama regional clinical center, which was the only clinic in town. Almost all cases of stroke (≥90%) were diagnosed based on magnetic resonance imaging or computed tomography of the brain. The diagnostic criteria for stroke and its subtypes were based on the Classification of Cerebrovascular Disease III by the National Institute of Neurological Disorders and Stroke [28]. A transient ischemic attack was not considered a stroke in this study.
Statistical analysis
To compare means and proportions, we used Student’s t tests or analysis of variance and the chi-square test, respectively. To estimate LTR, age (in years) was used as the timescale, and follow-up started at baseline or age at the time of study entry. Participants who were below the index age of interest at the beginning of the study period entered the analysis when they reached the required age. The age categories began at 45 years, and the highest age category was set as age 85 years and older. The participants were divided into four groups according to whether they had CKD and/or hypertension. We calculated the sex-specific 10-, 20-, 30-, and 40-year risks of stroke at the age of 45 years. The LTRs of stroke were calculated at the index ages of 45, 55, 65, and 75 years according to these groups using a double decrement model, taking into consideration both the occurrence of the outcome of interest and all-cause mortality [11, 14,15,16]. In the sensitivity analysis, we assessed the intermediate-term risk and LTR of stroke at an index age of 45 years using the eGFRCKD-EPI. We evaluated the LTR of stroke, excluding the participants who had a history of heart disease, including arterial fibrillation, and including the participants who lacked medical data for antihypertensive treatment, at the index age of 45 years. In addition, we calculated the LTRs of cerebral infarction and hemorrhage separately. The calculations were performed using the Practical Incidence Estimator macro [11]. Moreover, the adjusted hazard ratio (HR) for stroke in participants with CKD and/or hypertension was assessed using the Cox proportional hazards model, which included sex, age, body mass index (BMI), current or ex-smoker status, current or ex-drinker status, diabetes mellitus, and hypercholesterolemia as covariates. We evaluated the proportional hazard assumption by creating time-dependent variables. All statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Cary, North Carolina, USA). A P value < 0.05 was considered statistically significant.
Results
Characteristics
The participants (66.0% women; mean age 63.1 years) consisted of 51.4% who did not have either CKD or hypertension, 7.1% who had CKD but not hypertension, 32.2% who had hypertension but not CKD, and 9.3% who had CKD and hypertension. When compared with the 1291 who were excluded due to the lack of data, the 1525 included in the analysis were older; had lower BMI, DBP, and SCr values; had lower proportions of individuals who were men, smokers, and drinkers; had higher proportion of individuals with hypercholesterolemia and diabetes mellitus; and had a higher proportion of individuals who used antihypertensive medication; however, after adjusting for age and sex, there was no difference in the risk of stroke between the excluded and included participants (P = 0.49) (Supplementary Table 2). The baseline characteristics of the participants who did not receive antihypertensive treatment and those who did not provide baseline data regarding antihypertensive treatment are shown in Supplementary Table 3.
The distribution of participants across CKD stages is shown in Supplementary Table 4. Significant differences were observed in age, BMI, blood pressure, SCr level, eGFR, the proportions of participants with hypercholesterolemia and diabetes mellitus, the use of antihypertensive medication, and proteinuria (Table 1). After stratification by sex, significant differences in the proportions of patients with hypercholesterolemia and diabetes mellitus disappeared in men, although significant differences remained in other variables (Supplementary Table 5). Age, proportion of patients who smoked, proportion of patients who consumed alcohol, blood pressure, proportion of patients with proteinuria, and SCr level were higher among men than women (Supplementary Table 6).
LTRs and intermediate-term risks of stroke
During the mean follow-up period of 16.5 years (27748.5 person-years), a first stroke occurred in 238 participants: 170 had cerebral infarction, 52 had intracerebral hemorrhage, and 14 had subarachnoid hemorrhage. The numbers of strokes and the duration of follow-up in person-years according to age groups are shown in Supplementary Table 7.
Figure 1 shows the cumulative incidence of stroke in each group starting from 45 years of age. Although the incidence of stroke was 0.0% in men and women until 55 years of age, the incidence increased starting at 56 years old. The cumulative stroke incidence was consistently low in participants without CKD and hypertension starting from 65 years of age. The highest cumulative stroke incidence was identified in women with CKD and hypertension starting from 60 years of age among the four groups (Fig. 1). The 10-, 20-, 30-, and 40-year risks with 95% confidence intervals at the index age of 45 years are shown in Supplementary Table 8.

Curves of the cumulative stroke incidence from 45 to 85 years of age in men and women after considering the competing risk of death. CKD chronic kidney disease, HT hypertension
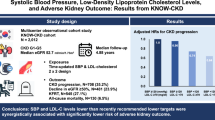
Figure 2 shows the LTRs for stroke in men and women at the index ages of 45, 55, 65, and 75 years. The highest LTRs of stroke at the index age of 45 years (men/women) were 38.4%/36.4% for participants with CKD and hypertension. The LTRs of stroke in participants with either CKD or hypertension were 1.6 times higher than in those without either condition at the age of 45 years (Fig. 2). Although the additive effect of CKD and hypertension on stroke was confirmed in men and women, the amplitude of the additive effect was greater in women than in men at the index age of 45 years. The LTRs of stroke tended to be higher in younger people than in older people among the participants with CKD and/or hypertension (Fig. 2). In addition, the LTR of stroke was the highest in participants with CKD and hypertension among the four groups when the threshold of SBP/DBP ≥130/≥80 mmHg was used for the diagnosis of hypertension (Supplementary Table 9).

The LTRs (95% confidence intervals) of stroke at the index ages of 45, 55, 65, and 75 years in men and women. CKD chronic kidney disease, LTR lifetime risk
When we also evaluated the LTR of stroke using eGFRCKD-EPI in the sensitivity analysis, the LTRs of stroke at the index age of 45 years (men/women) (95% CI) were 20.7% (11.6–27.1)/16.0% (10.9–19.6) for participants without CKD or hypertension, 38.6% (7.5–63.4)/22.0% (2.0–34.4) for those with CKD but without hypertension, 37.7% (28.1–46.3)/28.2% (21.1–34.6) for those with hypertension but without CKD, and 39.7% (20.1–60.0)/36.5% (16.9–52.5) for those with CKD and hypertension (intermediate-term risks are shown in Supplementary Table 10); the highest LTR of stroke was observed in those with CKD and hypertension. Moreover, we also calculated the LTR of stroke, excluding the participants with a history of heart disease, and similar results were observed, whereby the LTR of stroke at the index age of 45 years in men/women (95% CI) was 20.6% (11.1–27.1)/14.1% (9.1–17.8) for participants without CKD or hypertension; 34.1% (7.2–54.5)/30.1% (13.9–41.8) for those with CKD but without hypertension; 38.9% (28.9–48.0)/27.3% (19.6–34.1) for those with hypertension but without CKD; and 39.9% (21.0–58.9)/36.8% (22.1–49.8) for those with CKD and hypertension. When we calculated the LTR of stroke, including the 483 participants who lacked data regarding antihypertensive treatment, the LTRs (95% CI) of a stroke at the index age of 45 years in men/women were 21.0% (13.2–26.4)/17.2% (12.5–20.6) for participants without CKD or hypertension; 29.0% (7.0–44.3)/22.8% (9.4–31.5) for those with CKD but without hypertension; 35.0% (26.7–42.3)/35.0% (19.6–51.7) for those with hypertension but without CKD; and 52.4% (37.0–71.1)/38.6% (24.4–52.5) for those with CKD and hypertension. The association of CKD and hypertension with the LTR of cerebral infarction was similar to the main results (Supplementary Table 11), while the LTR of cerebral hemorrhage was not clear, owing to the limited number of patients with cerebral hemorrhage (n = 26 for men and n = 40 for women) (Supplementary Table 12).
When the group without CKD or hypertension was treated as a reference, the HR (95% CI, P value) for stroke was 2.09 (1.23–3.57, P = 0.0067) in the group with CKD but without hypertension, 1.97 (1.44–2.70, P < 0.0001) in the group with hypertension but without CKD, and 2.84 (1.83–4.40, P < 0.0001) in the group with hypertension and CKD after adjusting for confounding factors. The time-dependent variables were not significantly associated with the incidence of stroke (P ≥ 0.11). There were no significant interactions between CKD and hypertension in the total population (P for interaction =0.27) or either sex (P for interaction ≥0.30).
Discussion
This is the first study to indicate the LTR and intermediate-term risk of stroke based on the presence of CKD and hypertension in a general Asian population. The participants without CKD or hypertension had a lower cumulative incidence of stroke than those with CKD and/or hypertension (Fig. 1). The LTR of stroke was the highest in participants with CKD and hypertension among the four groups. The LTR of stroke in participants with only CKD was approximately equal to that in those with only hypertension (Fig. 2). Our findings imply that CKD contributes to the LTR of stroke, as does hypertension.
The type of cardiovascular disease differs between Asian and Western populations. Asian populations have a higher incidence of stroke and a lower incidence of coronary heart disease than Western populations [20]. In the results based on 17 US cohorts, the LTR of stroke at the age of 55 years was ~10%, even in Western individuals with ≥2 major cardiovascular risk factors [29]. Meanwhile, the LTR of stroke beyond 50 years was 21.4–33.2% for hypertensive individuals in previous Japanese studies [15, 16]. These previous studies did not assess the LTR of stroke in patients with CKD. Our study showed a higher LTR of stroke than those reported in previous Japanese studies [15, 16]. Our study, for the first time, suggested that CKD influenced the LTR of stroke similar to hypertension.
The highest LTR of stroke was observed in both men and women with both hypertension and CKD. It seems that there was an additive effect of CKD and hypertension on the LTR of stroke (Fig. 2), while the Cox model that was adjusted for possible confounding factors did not show a synergistic effect of CKD and hypertension on stroke (P for interaction ≥0.27). This might be because CKD and hypertension have not only common mechanisms, such as arteriosclerosis, but also several other mechanisms leading to stroke in individuals with CKD. For instance, oxidative stress, endothelial dysfunction, inflammation, hyperhomocysteinemia, intracranial artery calcification, dyslipidemia, or coagulation promotion, which are caused by kidney dysfunction [30,31,32,33], could cause a stroke regardless of hypertensive status. These factors could explain the additive effect of CKD and hypertension on stroke. However, the amplitude of the additive effect of CKD and hypertension on stroke was small in men. The LTR could reach the peak value when the participants had either CKD or hypertension, especially in men.
Young people have a low short-term risk but a high LTR of cardiovascular disease. This suggests that LTR is useful for encouraging younger people to modify their lifestyles or receive treatment. In previous studies, the LTR of stroke for hypertensive patients was higher in young adults than in older individuals [14,15,16, 18]. We further indicated the LTRs of stroke in patients with CKD, suggesting the necessity of preventing CKD and hypertension in younger populations. Our results provide useful information that can be used to encourage the young population to pay attention to not only their blood pressure but also their kidney function to prevent stroke.
There were some limitations of the present study. First, our study was performed using baseline data collected between 1992 and 1997 in a limited area in Japan, and the number of stroke cases was small. A larger and more recent study is needed to obtain more accurate risk estimates. However, the present study provides new information regarding the epidemiology of CKD. Second, we excluded 1291 individuals due to the lack of data in the present study. However, it is unlikely that this exclusion affected the LTR estimation in the present study since there was no difference in the risk of stroke between the excluded and included participants (Supplementary Table 1 and Supplementary Table 2). Marked differences also exist in the epidemiology of cardiovascular disease between Asian and Western populations. Further research in other ethnicities and cultures would help confirm the generalizability of our findings. Third, after including participants without data on antihypertensive treatment, the LTR of stroke at the index age of 45 years in men increased from 38.4% to 52.4% for those with CKD and hypertension. This increase indicates that excluding the 483 participants who lacked data resulted in the underestimation of the LTR. Fourth, we did not collect data on the causes of CKD. Some diseases, such as hypertension, diabetes mellitus, polycystic kidney disease, and systemic lupus erythematosus, can cause CKD, and stroke occurs as a complication of those diseases. The definition of CKD in the present study was dependent on the value of creatinine or positive proteinuria on only 1 occasion. The current guidelines define CKD as the presence of kidney damage or a GFR <60 mL/min/1.73 m2 for ≥3 months [34]. However, we used the same criteria to diagnose CKD in previous epidemiological studies [7, 22, 23]. Fifth, almost all participants had CKD stage G3a in the present study, and the LTR of stroke could be higher in the participants with advanced CKD stage G3b-5. Sixth, the baseline status was assumed to remain unchanged throughout the follow-up period in our model. For instance, while individuals without any disease at baseline were classified into the group with neither CKD nor hypertension, new CKD or hypertension could have developed during follow-up. In this case, the LTR of stroke might have been overestimated. Furthermore, we did not consider the effects of treatment, including the use of antiplatelet and anticoagulant drugs during follow-up. The LTR of stroke also did not take into consideration individual risk factors. However, these limitations are present in the ASCVD risk estimator and existed in other studies [13,14,15,16,17,18].
In conclusion, the present study showed that CKD was a risk factor for stroke, as is hypertension. The prevention of CKD and hypertension is important in younger populations to reduce the incidence of stroke. LTR is a useful approach to informing younger people about their cardiovascular risk. LTR has not been focused on in the present international guidelines for the evaluation and management of CKD [34], while European guidelines for the management of dyslipidemia have already stated the importance of LTR [12]. The LTR of stroke for individuals with CKD in our study could generate meaningful information that could be used to promote the prevention of CKD. The utilization of this information to guide individuals’ choices regarding healthy practices could enable the general public, especially young individuals, to understand the risk of stroke, contributing to the early prevention of stroke.
References
Naghavi M, Abajobir AA, Abbafati C, Abbas KM, Abd-Allah F, Abera SF, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1151–210.
Hay SI, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1260–344.
Williams B, Mancia G, Spiering W, Rosei EA, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). G Ital Cardiol (Rome). 2018;19:3–73.
Umemura S, Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens Res. 2019;42:1235–481.
Nakayama M, Metoki H, Terawaki H, Ohkubo T, Kikuya M, Sato T, et al. Kidney dysfunction as a risk factor for first symptomatic stroke events in a general Japanese population–the Ohasama study. Nephrol Dial Transpl. 2007;22:1910–5.
Cherng YG, Lin CS, Shih CC, Hsu YH, Yeh CC, Hu CJ, et al. Stroke risk and outcomes in patients with chronic kidney disease or end-stage renal disease: two nationwide studies. PLoS One. 2018;13:e0191155.
Yamagata K, Ishida K, Sairenchi T, Takahashi H, Ohba S, Shiigai T, et al. Risk factors for chronic kidney disease in a community-based population: a 10-year follow-up study. Kidney Int. 2007;71:159–66.
Campese VM, Mitra N, Sandee D. Hypertension in renal parenchymal disease: why is it so resistant to treatment? Kidney Int. 2006;69:967–73.
Fortin JM, Hirota LK, Bond BE, O’Connor AM, Col NF. Identifying patient preferences for communicating risk estimates: a descriptive pilot study. BMC Med Inf Decis Mak. 2001;1:2.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–104.
Beiser A, D’Agostino RB Sr, Seshadri S, Sullivan LM, Wolf PA. Computing estimates of incidence, including lifetime risk: Alzheimer’s disease in the Framingham Study. The Practical Incidence Estimators (PIE) macro. Stat Med. 2000;19:1495–522.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37:2999–3058.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596–646.
Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Au R, Kannel WB, et al. The lifetime risk of stroke: estimates from the Framingham Study. Stroke. 2006;37:345–50.
Takahashi I, Geyer SM, Nishi N, Ohshita T, Takahashi T, Akahoshi M, et al. Lifetime risk of stroke and impact of hypertension: estimates from the adult health study in Hiroshima and Nagasaki. Hypertens Res. 2011;34:649–54.
Turin TC, Okamura T, Afzal AR, Rumana N, Watanabe M, Higashiyama A, et al. Hypertension and lifetime risk of stroke. J Hypertens. 2016;34:116–22.
Satoh M, Ohkubo T, Asayama K, Murakami Y, Sugiyama D, Yamada M, et al. Lifetime Risk of Stroke and Coronary Heart Disease Deaths According to Blood Pressure Level: EPOCH-JAPAN (Evidence for Cardiovascular Prevention From Observational Cohorts in Japan). Hypertension. 2019;73:52–9.
Wang Y, Liu J, Wang W, Wang M, Qi Y, Xie W, et al. Lifetime risk of stroke in young-aged and middle-aged Chinese population: the Chinese Multi-Provincial Cohort Study. J Hypertens. 2016;34:2434–40.
Hall YN, Hsu CY, Iribarren C, Darbinian J, McCulloch CE, Go AS. The conundrum of increased burden of end-stage renal disease in Asians. Kidney Int. 2005;68:2310–6.
Ueshima H, Sekikawa A, Miura K, Turin TC, Takashima N, Kita Y, et al. Cardiovascular disease and risk factors in Asia: a selected review. Circulation. 2008;118:2702–9.
Imai Y, Nagai K, Sakuma M, Sakuma H, Nakatsuka H, Satoh H, et al. Ambulatory blood pressure of adults in Ohasama, Japan. Hypertension. 1993;22:900–12.
Kanno A, Kikuya M, Asayama K, Satoh M, Inoue R, Hosaka M, et al. Night-time blood pressure is associated with the development of chronic kidney disease in a general population: the Ohasama Study. J Hypertens. 2013;31:2410–7.
Kanno A, Kikuya M, Ohkubo T, Hashimoto T, Satoh M, Hirose T, et al. Pre-hypertension as a significant predictor of chronic kidney disease in a general population: the Ohasama Study. Nephrol Dial Transpl. 2012;27:3218–23.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e13–115.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12.
Horio M, Imai E, Yasuda Y, Watanabe T, Matsuo S. Modification of the CKD epidemiology collaboration (CKD-EPI) equation for Japanese: accuracy and use for population estimates. Am J Kidney Dis. 2010;56:32–8.
Special report from the National Institute of Neurological Disorders and Stroke. Classification of cerebrovascular diseases III. Stroke. 1990;21:637–76.
Berry JD, Dyer A, Cai X, Garside DB, Ning H, Thomas A, et al. Lifetime risks of cardiovascular disease. N Engl J Med. 2012;366:321–9.
Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects on the cardiovascular system. Circulation. 2007;116:85–97.
Bugnicourt JM, Chillon JM, Massy ZA, Canaple S, Lamy C, Deramond H, et al. High prevalence of intracranial artery calcification in stroke patients with CKD: a retrospective study. Clin J Am Soc Nephrol. 2009;4:284–90.
Muntner P, Hamm LL, Kusek JW, Chen J, Whelton PK, He J. The prevalence of nontraditional risk factors for coronary heart disease in patients with chronic kidney disease. Ann Intern Med. 2004;140:9–17.
Madore F. Uremia-related metabolic cardiac risk factors in chronic kidney disease. Semin Dial. 2003;16:148–56.
Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63:713–35.
Acknowledgements
We are grateful to the residents and staff members in Ohasama and staff members of the Hanamaki City Government, Iwate Prefectural Central Hospital Attachment Ohasama Regional Clinical Center, Iwate Prefectural Stroke Registry, General Hanamaki Hospital, Teikyo University, Tohoku Medical and Pharmaceutical University, and Tohoku University for their valuable support of the Ohasama study project.
Funding
This study was supported by Grants for Scientific Research (16H05243, 16H05263, 16K09472, 16K11850, 16K15359, 17H04126, 17H06533, 17K15853, 17K19930, 18K09674, 18K09904, 18K17396, 19K19466, 19H03908, 19K10662, and 20K08612) from the Ministry of Education, Culture, Sports, Science, and Technology, Japan; a Grant-in-Aid for Young Scientists of Showa Pharmaceutical University H28-4; the Japan Arteriosclerosis Prevention Fund; Grant–in–aid from the Ministry of Health, Labor, and Welfare, Japan (H26-Junkankitou [Seisaku]-Ippan-001, H29–Junkankitou–Ippan–003 and 20FA1002); A Scheme to Revitalize Agriculture and Fisheries in Disaster Area through Deploying Highly Advanced Technology (NouEi 2-02) from the Ministry of Agriculture, Forestry and Fisheries, Japan; the internal research grants from Keio University; Advanced Comprehensive Research Grants of Teikyo University; the Academic Contributions from Pfizer Japan Inc.; scholarship donations from Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd.; research supports from Astellas Pharma Inc. and Takeda Pharmaceutical Co., Ltd.; the Health Care Science Institute Research Grant; and the Health Science Center Research Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H.M., K.A., Y.I., and T.O concurrently held the position of director of the Tohoku Institute for Management of Blood Pressure, supported by Omron Healthcare Co., Ltd.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Nakayama, S., Satoh, M., Metoki, H. et al. Lifetime risk of stroke stratified by chronic kidney disease and hypertension in the general Asian population: the Ohasama study. Hypertens Res 44, 866–873 (2021). https://doi.org/10.1038/s41440-021-00635-z
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-021-00635-z
Keywords
This article is cited by
-
The Japanese Society of Hypertension Guidelines for the management of elevated blood pressure and hypertension 2025 (JSH2025)
Hypertension Research (2026)
-
Current hypertension epidemiology and contemporary approaches using the “Real-World Evidence Cycle” framework
Hypertension Research (2026)
-
Nighttime blood pressure in patients with chronic kidney disease: ambulatory blood pressure monitoring status in Japan and future implementation
Hypertension Research (2025)
-
Long-term risk of cardiovascular mortality according to age group and blood pressure categories of the latest guideline
Hypertension Research (2025)
-
Cross-classification by systolic and diastolic blood pressure levels and chronic kidney disease, proteinuria, or kidney function decline
Hypertension Research (2023)
