
Abstract
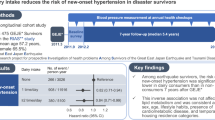
The aim of this study was to determine the relationship between eating before bed and the development of hypertension in a general Japanese population. We conducted a population-based retrospective cohort study using annual health check-up data collected from the residents of Iki City, Nagasaki Prefecture, Japan. In total, 2930 participants without hypertension at baseline (mean age 57.0 years, male 42.8%) were included in the present analysis. Eating before bed was defined as eating within 2 h of bedtime. The outcome of this study was incident hypertension (blood pressure ≥140/90 mmHg or initiation of blood pressure-lowering medications). Multivariable-adjusted hazard ratios and 95% confidence intervals (CIs) were estimated using Cox proportional hazards models. During an average follow-up of 4.5 years, 909 participants developed hypertension. The incidence (per 1000 person-years) of hypertension in the group of individuals who ate before bed was 82.8, whereas that in the group of individuals who did not eat before bed was 65.8. The association was significant even after adjusting for other risk factors, including age, sex, current smoking status, current alcohol intake, regular exercise, obesity, elevated blood pressure, diabetes mellitus, and dyslipidemia, with a hazard ratio of 1.23 (95% CI: 1.05–1.44) for the group of individuals who ate before bed compared with the group of individuals who did not eat before bed (P = 0.01 for trend). Eating before bed was correlated with a future risk of developing hypertension in the general Japanese population.
Similar content being viewed by others
Introduction
Cardiovascular disease is one of the leading causes of premature death in Japan and other countries [1, 2]. It is estimated that 50% of fatalities from cerebrovascular disease and 59% of fatalities from coronary artery disease are attributable to hypertension [2, 3]. In Japan, the average blood pressure (BP) of the population has decreased, mainly owing to an increase in the number of people taking BP-lowering medications and continued improvements in patient management protocols; however, the prevalence of hypertension has not noticeably decreased in the past few decades [2,3,4,5]. For the effective prevention of hypertension and subsequent cardiovascular disease, the development of strategies based on up-to-date knowledge of current risk factors in Japan is necessary.
Recently, eating before bed has been suggested to be associated with an increased risk of hypertension and obesity. However, current evidence supporting the association between eating before bed and the incidence of hypertension was derived from a worksite-based observational study of 735 Japanese workers with a short follow-up period [6].
The purpose of the present large-scale population-based study with long-term follow-up was to determine the relationship between eating before bed and the future development of hypertension among the general Japanese population.
Methods
Study design and participants
The Iki Epidemiological Study of Atherosclerosis and Chronic Kidney Disease (ISSA-CKD) is a population-based retrospective cohort investigation of the residents of Iki city, Nagasaki Prefecture, Japan. Details of the ISSA-CKD study have been previously described [7,8,9,10]. Iki City is a group of islands located in the north of Nagasaki Prefecture with a total population of ~27,000. Between 2008 and 2017, 7895 residents aged ≥30 years underwent annual health check-ups conducted by the local government of Iki City. After excluding 1881 residents with follow-up durations <1 year, 2812 individuals with hypertension (BP ≥ 140/90 mm Hg or use of BP-lowering medications) at baseline and 272 individuals with missing information on eating behaviors at baseline, a total of 2930 participants (mean age 57.0 years, male 42.8%) were included in the present analysis (Fig. 1).

Flow chart of participants.
This study was approved by the Fukuoka University Clinical Research & Ethics Centre (No. 2017M010).
Data collection
Health check-ups were carried out at hospitals and clinics in Iki City using guidance from the Ministry of Health, Labor and Welfare of Japan [11]. At baseline, details concerning eating habits, smoking habits, alcohol intake, and regular exercise were obtained using a standard questionnaire. Eating before bed was defined as eating dinner within 2 h of going to sleep 3 times or more each week. Current smoking status was defined as having smoked at least 100 cigarettes or having smoked regularly for >6 months at baseline. Alcohol intake was classified as daily consumption or nondaily consumption. Participation in regular exercise was defined as exercising for ≥30 min per day ≥2 times per week. Participants’ height and weight were measured while they wore light clothes without shoes, and their body mass index (BMI: BMI was calculated by dividing body weight (kg) by height in square meters) was calculated. Obesity was defined as a BMI ≥ 25 kg/m2 [12]. At each health check-up, BP was measured by trained staff on the right upper arm using mercury, automated, or aneroid sphygmomanometers with appropriately sized cuffs after the participant had rested for at least 5 min in a sitting position in accordance with standardized guidelines [13]. BP was measured twice, and the mean of the two values was used in the present analysis. Elevated BP was defined as BP of 130–139/80–89 mmHg [2]. Casual blood and urine samples were also collected. The plasma glucose concentration was determined using an enzymatic method, and the glycated hemoglobin (HbA1c) concentration (National Glycohemoglobin Standardization Program value) was determined using high-performance liquid chromatography. The presence of diabetes mellitus was defined as a fasting glucose concentration of ≥7.0 mmol/L, a nonfasting glucose concentration of ≥11.1 mmol/L, an HbA1c concentration of ≥6.5%, or the use of glucose-lowering therapy. Serum low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride concentrations were enzymatically determined, and dyslipidemia was defined as an LDL cholesterol level of ≥3.62 mmol/L, an HDL cholesterol level of <1.03 mmol/L, a triglyceride level of ≥1.69 mmol/L [2], or the use of lipid-lowering medications.
Definition of the outcome
The outcome of the present analysis was the development of hypertension (BP ≥ 140/90 mmHg or initiation of BP-lowering medications) confirmed by the end of the follow-up period.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation and were tested using a t test for continuous variables. Categorical variables are expressed as the number of participants (percentage) and were tested using the chi-squared test. The incidence rate of hypertension was calculated using the person–year approach. Crude and multivariable-adjusted hazard ratios and their 95% confidence intervals (CIs) were estimated using Cox proportional hazards models. The multivariable Cox model included age, sex, current smoking status, current daily alcohol intake, regular exercise, obesity, elevated blood pressure, diabetes mellitus and dyslipidemia as covariates. The effects of eating before bed on the development of hypertension were compared between subgroups defined by other risk factors (i.e., age, sex, smoking, alcohol, exercise, and obesity) by adding an interaction term to the statistical model. Overall differences in follow-up BP levels were compared using a linear mixed model. A two-tailed P < 0.05 was considered statistically significant. All data analyses were performed using SAS version 9.4.
Results
Table 1 shows the baseline characteristics of participants according to the habit of eating before bed. Participants who reported a habit of eating before bed were more likely to be male, current smokers, current daily alcohol drinkers, and obese and to have higher triglyceride levels than those who did not report a habit of eating before bed.
During an average follow-up period of 4.5 years, a total of 909 participants developed hypertension. Table 2 presents the risk of hypertension according to the habit of eating before bed. Participants who ate before bed had a higher incidence of hypertension (82.8 per 1000 person-years) than those who did not eat before bed (65.8 per 1000 person-years) (P = 0.0040). This association remained significant even after adjustment for other risk factors, including age, sex, current smoking status, current daily alcohol intake, regular exercise, obesity, elevated BP, diabetes, and dyslipidemia (hazard ratio: 1.23, 95% CI: 1.05–1.44; P = 0.010). When follow-up systolic blood pressure levels were used as continuous variables, follow-up blood pressure values were 123.2 mmHg in the “eating before bed” group versus 121.9 mmHg in the control group at 1 year, 123.9 versus 122.9 mmHg at 2 years, 124.1 versus 123.0 mmHg at 3 years, 125.3 versus 123.9 mmHg at 4 years, 125.5 versus 124.0 mmHg at 5 years, 125.7 versus 123.9 mmHg at 6 years, 125.8 versus 125.0 mmHg at 7 years, 127.5 versus 125.5 mmHg at 8 years, and 129.4 versus 128.4 mmHg at 9 years (Fig. 2). The overall difference in systolic blood pressure during the follow-up period between the groups was statistically significant (1.1 mmHg, 95% confidence interval 0.1–2.1, P = 0.037), although the difference became nonsignificant after adjustment for other confounders (0.6 mmHg, 95% confidence interval 0.2–1.5, P = 0.155).

Follow-up systolic blood pressure levels (A) in all participants and (B) according to the habit of eating before bed. ※Vertical lines represent standard error
Table 3 summarizes the results of the subgroup analysis. There were no clear differences in the effects of eating before bed on the development of hypertension between subgroups defined by age, sex, smoking, alcohol, exercise, or obesity (all P > 0.1 for interactions).
Discussion
The present large-scale observational study of a general Japanese population revealed the existence of a close association between eating before bed and the future development of hypertension. This association was significant even after adjustment for confounding factors such as age, sex, current smoking status, current alcohol intake, regular exercise, obesity, elevated BP, diabetes, and dyslipidemia. Similar associations were also identified between eating before bed and hypertension across subgroups defined by age, sex, smoking, alcohol, exercise, and obesity.
A few previous studies have investigated the relationship between the length of time between dinner and bedtime and the incidence of hypertension. A birth cohort study of 1253 residents in the UK reported that an increase in energy intake at the age of 43 years was linearly associated with an increase in systolic blood pressure levels during a 10-year follow-up period [14]. Nakamoto et al. conducted a cross-sectional study on 722 male and female workers aged >20 years in Japan. The results showed that among participants who had dinner after 21:00, those who went to bed ≥3 h after eating had a 0.69 times lower risk of hypertension than those who went to bed <2 h after eating [6]. The present population-based observational study of 2930 Japanese individuals of both sexes confirmed these findings from the previous study and clearly showed an increased incidence of hypertension among participants who ate within 2 h before bed.
Another important finding from the present analysis was that the natural increase in systolic blood pressure levels among normotensive people was ~0.5 mmHg/year (except for the last year, which had a limited number of participants) (Fig. 2). These findings are compatible with those of the National Nutritional Survey conducted in 2016, which demonstrated that systolic blood pressure levels increased by ~5 mmHg for each 10-year increase in age [2, 15, 16]. Our results are also comparable with the estimated systolic blood pressure slope with age of ~0.6 mmHg/year according to the INTERSALT study [17] and a sodium intake level of 170 mmol/day based on the National Nutritional Survey conducted in 2016 [16]. Based on the above results, the natural increase in systolic blood pressure levels associated with aging among normotensive people is estimated to be 0.5–0.6 mmHg/year, although this number might have been affected by the initiation of blood pressure-lowering treatment among people who developed hypertension.
The mechanisms underlying the relationship between eating before bed and the incidence of hypertension remain unclear. One possible mechanism is that eating before bed causes nocturnal hyperinsulinemia, which increases BP through enhanced sympathetic nerve activity, proliferation of vascular smooth muscle cells, and sodium retention [18,19,20]. Another possible mechanism is that a decrease in the quality of sleep associated with a short time between dinner and bedtime may increase sympathetic nerve activity and, subsequently, BP [21].
Our study was a large-scale investigation in a general Japanese population. This survey is potentially generalizable because of the large number of subjects included and the long average follow-up period. However, there are also some limitations that should be noted. First, because of the retrospective nature of the study, the findings of the present analysis may be affected by selection bias. Another limitation is that people with healthy lifestyles are more likely to attend health check-ups conducted by the local government than those with unhealthy lifestyles. Third, different kinds of sphygmomanometers were used, and their measurement bias can affect the results. However, similar findings were observed when hypertension was defined based only on the initiation of BP-lowering medications (not using BP values that might be affected by the limitation of various blood pressure devices) (multivariable-adjusted hazard ratio 1.43, 95% confidence interval 1.17–1.77, p < 0.001). Although the measurement bias owing to the use of different kinds of sphygmomanometers is a major limitation of this study, the bias is unlikely to invalidate the findings of this study. Fourth, there was no information on dietary habits and lifestyle factors except for smoking, alcohol intake and physical activity. Although we attempted to control the confounding effects of smoking, alcohol intake and physical activity, eating before bed might be a surrogate marker of another unhealthy dietary habit or lifestyle whose information was not collected in this study. Furthermore, information on the content of the meal before bed, which could be an important factor, was not available in this study. Fifth, the findings of this study might be affected by information bias because information on eating before bed was collected using a standard questionnaire. Some participants might have underreported or were uncertain about their eating habits at baseline examination.
Conclusion
In conclusion, eating before bed was clearly associated with the development of hypertension in the future in a general Japanese population. Strategies to avoid late dinners may ensure better prevention of the future development of hypertension and subsequent cardiovascular diseases.
References
GBD. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858.
Umemura S, Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, et al. The Japanese society of hypertension guidelines for the management of hypertension (JSH 2019). Hypertens Res.2019;42:1235–481.
Kinoshita M, Yokote K, Arai H, Iida M, Ishigaki Y, Ishibashi S, et al. Japan Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases 2017. J Atheroscler Thromb.2018;25:846–984.
Satoh A, Arima H, Ohkubo T, Nishi N, Okuda N, Ae R, et al. Associations of socioeconomic status with prevalence, awareness, treatment, and control of hypertension in a general Japanese population: NIPPON DATA2010. J Hypertens.2017;35:401–8.
Fujiyoshi A, Ohkubo T, Miura K, Murakami Y, Nagasawa SY, Okamura T, et al. Blood pressure categories and long-term risk of cardiovascular disease according to age group in Japanese men and women. Hypertens Res.2012;35:947–53.
Nakamoto MST, Shuto E, Aki N, Kosugi C, Hata A, et al. Preiod between dinnerand bedtime is related to hypertension. J Jpn Soc Nutr Food Sci.2013;66:185–93.
Maeda T, Yoshimura C, Takahashi K, Ito K, Yasuno T, Abe Y, et al. Usefulness of the blood pressure classification in the new 2017 ACC/AHA hypertension guidelines for the prediction of new-onset chronic kidney disease. J Hum Hypertens.2019;33:873–8.
Yasuno T, Maeda T, Tada K, Takahashi K, Ito K, Abe Y, et al. Effects of HbA1c on the development and progression of chronic kidney disease in elderly and middle-aged Japanese: Iki epidemiological study of atherosclerosis and chronic kidney disease (ISSA-CKD). Intern Med.2020;59:175–80.
Miyabayashi I, Mori S, Satoh A, Kawazoe M, Funakoshi S, Ishida S, et al. Uric acid and prevalence of hypertension in a general population of Japanese: ISSA-CKD Study. J Clin Med Res.2020;12:431–5.
Ito K, Maeda T, Tada K, Takahashi K, Yasuno T, Masutani K, et al. The role of cigarette smoking on new-onset of chronic kidney disease in a Japanese population without prior chronic kidney disease: Iki epidemiological study of atherosclerosis and chronic kidney disease (ISSA-CKD). Clin Exp Nephrol.2020;24:919–26.
Ministry of Health, Labour and Welfare. Standard program of health check-up & health guidance. Tokyo: Ministry of Health, Labour and Welfare; 2007.
Examination Committee of Criteria for ‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity. New criteria for ‘obesity disease’ in Japan. Circ J. 2002;66:987–92.
The Japanese Society of Cardiovascular Disease Prevention. Handbook for cardiovascular prevention. Tokyo: Hokendojinsha; 2014.
Meier P, Messerli FH, Baumbach A, Lansky AJ. Pre-hypertension: another ‘pseudodisease’? BMC Med.2013;11:211.
Hisamatsu T, Segawa H, Kadota A, Ohkubo T, Arima H, Miura K. Epidemiology of hypertension in Japan: beyond the new 2019 Japanese guidelines. Hypertens Res.2020;43:1344–51.
Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan, 2016. Tokyo: Ministry of Health, Labour and Welfare; 2007.
Intersalt an international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. INTERSALT Cooperative Research Group. BMJ. 1988;297:319–28.
Lembo G, Napoli R, Capaldo B, Rendina V, Iaccarino G, Volpe M, et al. Abnormal sympathetic overactivity evoked by insulin in the skeletal muscle of patients with essential hypertension. J Clin Invest.1992;90:24–9.
Hsueh WA, Law RE. Insulin signaling in the arterial wall. Am J Cardiol.1999;84:21j–4j.
DeFronzo RA. The effect of insulin on renal sodium metabolism. A review with clinical implications. Diabetologia. 1981;21:165–71.
Hsieh SD, Muto T, Murase T, Tsuji H, Arase Y. Association of short sleep duration with obesity, diabetes, fatty liver and behavioral factors in Japanese men. Intern Med. 2011;50:2499–502.
Acknowledgements
We thank Edanz Group (https://en-author-services.edanzgroup.com/ac) for editing a draft of this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Funakoshi, S., Satoh, A., Maeda, T. et al. Eating before bed and new-onset hypertension in a Japanese population: the Iki city epidemiological study of atherosclerosis and chronic kidney disease. Hypertens Res 44, 1662–1667 (2021). https://doi.org/10.1038/s41440-021-00727-w
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-021-00727-w
Keywords
This article is cited by
-
Relationship between abdominal circumference and the incidence of hyperuricemia in the general Japanese population
Scientific Reports (2024)
-
Fluid homeostasis induced by sodium-glucose cotransporter 2 inhibitors: novel insight for better cardio-renal outcomes in chronic kidney disease
Hypertension Research (2023)
-
Current topic of vascular function in hypertension
Hypertension Research (2023)
-
Serum triglyceride levels and incidence of hypertension in a general Japanese population: ISSA-CKD study
Hypertension Research (2023)
-
Update on Hypertension Research in 2021
Hypertension Research (2022)
