
Abstract
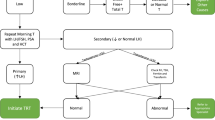
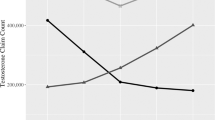
The American Urological Association and Endocrine Society published guidelines for the management of testosterone deficiency in 2018. Testosterone prescription patterns have varied widely recently, owing to increased public interest and emerging data on the safety of testosterone therapy. The effect of guideline publication on testosterone prescribing is unknown. Thus, we aimed to assess testosterone prescription trends using Medicare prescriber data. Specialties with over 100 testosterone prescribers from 2016–2019 were analyzed. Nine specialties were included (in order of descending prescription frequency): family practice, internal medicine, urology, endocrinology, nurse practitioners, physician assistants, general practice, infectious disease, and emergency medicine. The number of prescribers grew by a mean of 8.8% annually. There was a significant increase in average claims per provider from 2016 to 2019 (26.4 to 28.7, p < 0.0001), with the steepest increase occurring between 2017 and 2018 when the guidelines were released (27.2 to 28.1, p = 0.015). The largest increase in claims per provider was among urologists. Advanced practice providers comprised 7.5% of Medicare testosterone claims in 2016 and 11.6% in 2019. While no causation can be established, these results suggest that professional society guidelines are associated with increasing numbers of testosterone claims per provider, especially among urologists. The changing demographics of prescribers justifies targeted education and further research.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

Data availability
Data used in this study was extracted from the CMS Part D Prescriber Public Use File which is publicly available at https://data.cms.gov/.
References
Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Aging BLSo. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001;86:724–31.
Auerbach JM, Moghalu OI, Das R, Horns J, Campbell A, Hotaling J, et al. Evaluating incidence, prevalence, and treatment trends in adult men with hypogonadism in the United States. Int J Impot Res. 2021;34:762–8. https://doi.org/10.1038/s41443-021-00471-2.
Kumar P, Kumar N, Thakur DS, Patidar A. Male hypogonadism: symptoms and treatment. J Adv Pharm Technol Res. 2010;1:297–301.
Zhou CK, Advani S, Chaloux M, Gibson JT, Yu M, Bradley M, et al. Trends and patterns of testosterone therapy among U.S. male medicare beneficiaries, 1999 to 2014. J Urol. 2020;203:1184–90.
Baillargeon J, Kuo YF, Westra JR, Urban RJ, Goodwin JS. Testosterone prescribing in the United States, 2002–2016. JAMA. 2018;320:200–2.
Corona G, Rastrelli G, Di Pasquale G, Sforza A, Mannucci E, Maggi M. Testosterone and cardiovascular risk: meta-analysis of interventional studies. J Sex Med. 2018;15:820–38.
Carter IV, Callegari MJ, Jella TK, Mahran A, Cwalina TB, Muncey W, et al. Trends in testosterone prescription amongst medical specialties: a 5-year CMS data analysis. Int J Impot Res. 2022. https://doi.org/10.1038/s41443-021-00497-6.
Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, et al. Testosterone therapy in men with hypogonadism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2018;103:1715–44.
Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200:423–32.
Goldstick JE, Guy GP, Losby JL, Baldwin G, Myers M, Bohnert AS. Changes in initial opioid prescribing practices after the 2016 release of the CDC guideline for prescribing opioids for chronic pain. JAMA Netw Open. 2021;4:e2116860.
Zucker IJ, Masterson TA. Comparison of American Urological Association and Endocrine Society guidelines on testosterone replacement. Int J Impot Res. 2022;34:626–9. https://doi.org/10.1038/s41443-021-00477-w.
Colby SL, Ortman JM. Projections of the Size and Composition of the U.S. Population: 2014 to 2060. Population Estimates and Projections. Current Population Reports. P25-1143 [Internet]. US Census Bureau; 2015 [cited 2023 Mar 27]. Available from: https://eric.ed.gov/?id=ED578934.
Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. J Clin Endocrinol Metab. 2001;86:724–31. https://doi.org/10.1210/jcem.86.2.7219.
Bandari J, Ayyash OM, Emery SL, Wessel CB, Davies BJ. Marketing and testosterone treatment in the USA: a systematic review. Eur Urol Focus. 2017;3:395–402.
Kresch E, Patel M, Lima TF, Ramasamy R. An update on the available and emerging pharmacotherapy for adults with testosterone deficiency available in the USA. Expert Opin Pharmacother. 2021;22:1761–71.
García LM, Sanabria AJ, Álvarez EG, Trujillo-Martín MM, Etxeandia-Ikobaltzeta I, Kotzeva A, et al. The validity of recommendations from clinical guidelines: a survival analysis. CMAJ. 2014;186:1211–9.
McKibben MJ, Kirby EW, Langston J, Raynor MC, Nielsen ME, Smith AB, et al. Projecting the urology workforce over the next 20 years. Urology. 2016;98:21–6.
Iyeke LO, Richman MJ. Evaluating decreased libido: the lowdown on low T. J Urgent Care Med. 2021;16:33–4.
Jesse E, Sellke N, Rivero MJ, Muncey W, Ghayda RA, Loeb A, et al. Practice comparison and cost analysis of direct-to-consumer telemedicine platforms offering testosterone therapy. J Sex Med. 2022;19:1608–15.
Dubin JM, Jesse E, Fantus RJ, Bennett NE, Brannigan RE, Thirumavalavan N, et al. Guideline-discordant care among direct-to-consumer testosterone therapy platforms. JAMA Intern Med. 2022;182:1321–3.
Author information
Authors and Affiliations
Contributions
All authors meet all four criteria for authorship, including. (1) Conceived and/or designed the work that led to the submission, acquired data, and/or played an important role in interpreting the results. (2) Drafted or revised the manuscript. (3) Approved the final version. (4) Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sellke, N., Omil-Lima, D., Sun, H.H. et al. Trends in testosterone prescription during the release of society guidelines. Int J Impot Res 36, 380–384 (2024). https://doi.org/10.1038/s41443-023-00709-1
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41443-023-00709-1
This article is cited by
-
Testosterone replacement therapy and spermatogenesis in reproductive age men
Nature Reviews Urology (2025)
-
Response to comment on: Low serum testosterone is associated with an increased risk of first-time renal calculi in men without testosterone replacement therapy
International Journal of Impotence Research (2025)
-
Temporal trends in serum testosterone and luteinizing hormone levels indicate an ongoing resetting of hypothalamic-pituitary-gonadal function in healthy men: a systematic review
Journal of Endocrinological Investigation (2025)
