
Abstract
The health, economic, and social burden of neglected tropical diseases (NTDs) in Africa remains substantial, with elimination efforts hindered by persistent sociopolitical instability, including ongoing conflicts among political and ethnic groups that lead to internal displacement and migration. Here, we explore how innovative technologies can support Africa in addressing NTDs amidst such instability, through analysis of WHO and UNHCR data and a systematic literature review. Countries in Africa facing sociopolitical instability also bear a high burden of NTDs, with the continent ranking second globally in NTD burden (33%, 578 million people) and first in internal displacement (50%, 31.6 million people) in 2023. Studies have investigated technologies for their potential in NTD prevention, surveillance, diagnosis, treatment and management. Integrating the evidence, we discuss nine promising technologies—artificial intelligence, drones, mobile clinics, nanotechnology, telemedicine, augmented reality, advanced point-of-care diagnostics, mobile health Apps, and wearable sensors—that could enhance Africa’s response to NTDs in the face of persistent sociopolitical instability. As stability returns, these technologies will evolve to support more comprehensive and sustainable health development. The global health community should facilitate deployment of health technologies to those in greatest need to help achieve the NTD 2030 Roadmap and other global health targets.
Similar content being viewed by others


Introduction
Sociopolitical instability disrupts the lives of millions globally, impeding progress towards global health targets. According to the 2024 United Nations High Commissioner for Refugees (UNHCR) report, 2023 witnessed forced displacement of 117.3 million people worldwide1, disrupting global health initiatives, particularly those that already lacked political attention and resources, including programs focused on neglected tropical diseases (NTDs). Disruptive and unfavorable conditions in a country’s political and social structures, such as armed conflicts, civil unrest, governance issues, and social cohesion, are destabilizing the overall stability and functionality of society, including its health systems and health infrastructure. Such sociopolitical instability, characterized mainly by ongoing conflicts among diverse political or ethnic groups leading to extensive internal displacements and migrations, has significantly imped global health progress and posing a threat to global health security. NTDs, comprising a diverse range of 20 viral, bacterial, parasitic, fungal, and non-infectious diseases officially recognized by the World Health Organization (WHO), result in severe health, economic, and social consequences, affecting over one billion individuals annually2. The WHO NTDs Roadmap 20303 endeavors to address these challenges, but countries grappling with simultaneous sociopolitical and NTD challenges face substantial barriers to achieving Roadmap goals.
Africa, the second most populous continent in the world, represents an opportunity for health research and development (R&D) owing to its high rate of disease, susceptibility to emerging and infectious diseases, wealth of natural resources, and workforce capital. Despite the significant burden of diseases prevalent in the region4,5, African Ministries of Health are actively working towards the improvement of health systems and services. However, their endeavors are consistently impeded by ongoing sociopolitical instability. The number of people displaced internally due to conflict and violence in the continent has been rising consistently for the past five years6. This instability extends beyond national borders, forcing displaced people to migrate and potentially act as conduits of NTDs to low-incidence countries.
In today’s era, the healthcare sector is undergoing a profound transformation driven by technologies7,8,9,10. Innovations such as artificial intelligence (AI), robotics, and nanotechnology are evolving rapidly and drawing the attention of Ministries of Health, global partners, academia, and research institutions globally. There is a focused effort to investigate their potential contributions in eradicating, managing, preventing, diagnosing, monitoring, and treating a range of diseases and health conditions. For NTDs, efforts are underway to harness these technologies, aiming to address NTDs that have historically been overlooked by the global health community11,12. Significant efforts have been placed towards decentralizing NTD diagnostics, allowing testing to take place closer to NTD-affected populations rather than relying on distant laboratories. To this end, recently in 2024, the WHO released target product profiles (TPPs) for NTDs diagnostic tests to expedite the development of high-quality, user-friendly, and affordable NTD diagnostic tools13,14. In the realm of NTD drug and vaccine research and development, there has been notable progress, driven by the integration of science and technology. This shift has moved research strategies beyond conventional methods to include modern approaches such as phenotypic and molecular assays, multiparameter optimization, medicinal chemistry, and omics techniques15,16.
However, there remains insufficient evidence to fully understand the effectiveness of technologies in the NTD sector and their impact during periods of sociopolitical instability. Global health investments have inadequately prioritized effort to combat NTDs, and there remains a limited and insufficiently analyzed pool of knowledge and evidence to inform future interventions. These gaps are especially sensitive in African countries confronting a dual burden of sociopolitical instability and NTDs. There is a notable lack of comprehensive evidence on how technologies can help African meet global NTD targets in the face of persistent sociopolitical vacuums.
Therefore, this study explores the potential of technologies to address NTDs amidst sociopolitical instability. It aims to bridge the knowledge gap regarding how these technologies can support Africa in its efforts to meet the NTDs Roadmap 2030 within unstable sociopolitical environments.
Results
The findings of this study are based on an analysis of two distinct datasets. The first set involves a secondary analysis of WHO and UNHCR data focusing on: (I) Africa’s share of the global burden of NTDs, (II) Africa’s share of the global sociopolitical instability, and (III) the dual burden of NTDs and sociopolitical instability. The second set consists of a systematic review of the literature on technologies relevant to NTDs.
Analysis from WHO and UNHCR global data
Africa’s share of the global burden of NTDs
The analysis of data, drawing from WHO databases2,4,5, indicates that as a continent, Africa ranks second globally in the number of individuals affected by one of the 20 NTDs, with 33% (578 million individuals) affected, placing Africa behind Southeast Asia (54%, 939 million). Africa bears a significant proportion of cases for many of the NTDs, including 100% of dracunculiasis and African trypanosomiasis, 99% of onchocerciasis, 95% of buruli ulcer, 66% of visceral leishmaniasis, and 50% of podoconiosis cases globally (Fig. 1). The countries with the highest need for NTD interventions are Nigeria, Ethiopia, the Democratic Republic of the Congo (DRC), the United Republic of Tanzania (Tanzania), and Uganda. Of the 47 countries on the continent, 19 (40%) that were previously endemic have been officially validated or certified for the elimination of at least one NTD by the end of 2023. Forty-six countries (98%) have reached the threshold for eliminating leprosy as a public health problem at national level, with assistive technology devices for people with disabilities have also been developed. Twelve countries (26%) that were previously considered non-endemic for yaws are now suspected to be free from the disease. Although they are still awaiting formal certification2.

Burden of NTDs in WHO African Region compared with other WHO Regions, represented by (a) People need NTD interventions (number), (b) Trachoma prevalence (rate/100,000 people), (c). Lymphatic filariasis cases (number), (d) Onchocerciasis cases treated (number), (e) Cysticercosis cases (number/100,000 people), (f) Dengue fever cases (number), (g) Visceral leishmaniasis cases, (h) Cutaneous leishmaniasis cases (number). SE Asia: South-East Asia Region (WHO); Africa: African Region (WHO); E Mediter.; Eastern Mediterranean Region (WHO); W Pacific: Western Pacific Region (WHO); Americas: Region of the Americas (WHO); Europe: European Region (WHO).
Africa’s share of global sociopolitical instability
The analysis of data from UNHCR and WHO databases indicates that Africa hosted 83% of the 6.8 million people newly displaced globally between January and June 2023, with the majority being internally displaced1. Among the top 10 countries with the highest numbers of internally displaced people receiving UNHCR assistance, five were African: DRC, Somalia, Nigeria, Sudan, and Ethiopia. Five African countries, namely South Sudan, Sudan, DRC, Somalia, and Central African Republic, were among the top 10 global countries from which refugees originated, though 52% of refugees were from non-African countries (Afghanistan, Syria, Ukraine) (Fig. 2). Africa hosted 1 in 5 global refugees in 2022, led by Uganda (1.5 million), Sudan (1.1 million), Ethiopia (879,600), Chad (592,800), Cameroon (473,900), Niger (255,300), and DRC (520,500). For instance, Ethiopia ranks as the third largest host country for refugees in Africa, accommodating over 958,016 refugees and asylum-seekers, primarily from South Sudan, Somalia, and Eritrea1,6.

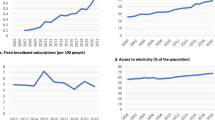
Sociopolitical instability in African Region compared with other global Regions, represented by (a) Refugees in top-10 countries (number), (b) IDPs assisted by UNHCR in top-10 countries, (c) Deaths in armed conflicts (number), (d) Refugees (per 100,000 population), (e) Healthy life expectancy at birth (years), (f) Current health expenditure as % of GDP. DR Congo: Democratic Republic of the Congo; C. Africa Rep.: Central African Republic; SE Asia: South-East Asia Region (WHO); Africa: African Region (WHO); E Mediter.; Eastern Mediterranean Region (WHO); W Pacific: Western Pacific Region (WHO); Americas: Region of the Americas (WHO); Europe: European Region (WHO); N America: Northern America (UN); Oceania: Oceania (UN); E & SE Asia: Eastern & South-Eastern Asia (UN); C & S Asia: Central & Southern Asia (UN); N Africa: Northern Africa (UN); Eur & N Am: Europe & Northern America (UN); SS Africa: Sub-Saharan Africa (UN); Europe: Europe (UN); L Am & Car: Latin America & Caribbean (UN).
Africa faced the highest number of deaths from armed conflict (53% of the global total) in 2022, led by Sudan, DRC, Somalia, and South Sudan. Armed conflicts involving the Sudanese Armed Forces and Rapid Support Forces in Sudan, M23 armed groups and Congolese armed forces in DRC, the Somali Government and al-Shabaab armed groups in Somalia, and the South Sudanese government and opposition groups in South Sudan were the primary drivers of internal displacements in Africa from January to June 2023. By 2024, East Africa, particularly the Horn of Africa, and the Great Lake region of Africa are predicted to host 23.6 million displaced people, while West and Central Africa could see a 9% increase to 13.6 million, including 8.4 million who are internally displaced1,6.
Dual burden of NTDs and sociopolitical instability in Africa
The analysis of data from WHO and UNHCR1,2,4,5,6 demonstrates that several politically unstable African countries are also burdened by a high burden of NTDs (Table 1). Nigeria, Ethiopia, and the DRC are the top three countries with the highest number of individuals in need of interventions against NTDs (Nigeria: 139,910,337; Ethiopia: 71,787,220; and DRC: 52,044,663). These countries also harbor a substantial number of internally displaced persons (IDPs), with Nigeria hosting 3,578,996, Ethiopia 4,385,789, and DRC 6,298,436. Additionally, they accommodate a notable count of refugees and asylum-seekers, with Nigeria recording 99,832, Ethiopia 994,563, and DRC 522,260. In South Sudan, out of its total population of 11 million, 8,758,494 individuals require interventions against NTDs, and 2,027,331 are IDPs. Similarly, Somalia, with a total population of 18 million, has 3,698,691 people in need of NTD interventions and 2,967,500 IDPs.
Systematic review of technologies relevant to NTDs
Characteristics of included studies
In the systematic review, out of the 22,541 articles screened, 2397 were excluded through subsequent steps, resulting in the identification of 46 studies that met the inclusion criteria17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62. Figure 3 provides PRISMA flow diagram of included studies and the selection criteria. The NTDs studied include leishmaniasis, lymphatic filariasis, scabies, dengue, trypanosomiasis, leprosy, onchocerciasis, chikungunya, echinococcosis, trachoma, soil-transmitted helminthiases, schistosomiasis, and others. The studies represented all study designs, including randomized controlled trials.

The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrates the study selection process, indicating the databases searched, the total number of records identified, the number of records screened, the number of studies assessed for eligibility, and the final number of studies included in the systematic review.
The selected studies investigated technologies for NTD prevention, prediction, surveillance, diagnosis, treatment, and management. With detailed analysis of the included studies, the paper is organized to explore and elaborate on nine promising technologies in the NTDs sector: artificial intelligence, drones, mobile clinics, nanotechnology, telemedicine, augmented reality, advanced point-of-care diagnostics, mobile health Apps, and wearable sensors (Fig. 4). This elaboration focuses on how these technologies could enhance Africa’s response to NTDs in the context of sociopolitical instability.

Nine promising technologies in the NTDs sector: artificial intelligence, drones, mobile clinics, nanotechnology, telemedicine, augmented reality, advanced point-of-care diagnostics, mobile health Apps, and wearable sensors.
Artificial intelligence and machine learning
Twelve studies17,18,19,20,21,22,23,24,25,26,27,28 evaluated the potential applications and benefits of AI and Machine Learning (ML) in the NTDs sector (Table 2).
Milad et al.17 assessed Automated Machine Learning (AutoML) for trachoma diagnosis from conjunctival images, achieving high accuracy (87% sensitivity, 88% specificity for trachomatous inflammation-follicular (TF); 95% sensitivity, 92% specificity for trachomatous inflammation-intense (TI). The study highlights the potential for widespread AI support for offline diagnosis. Yotsu et al.18 applied ML to diagnose skin NTDs (e.g., Buruli ulcer, leprosy) using ResNet-50 and VGG-16 convolutional neural networks (CNN) on clinical images. Models achieved over 70% accuracy, with ResNet-50 surpassing VGG-16, suggesting AI’s role in complementing clinical diagnosis of skin NTDs and addressing the unmet needs where access to medical care is limited. Wang et al.19 present a hepatic echinococcosis diagnostic AI system (EDAM) that supports rural clinicians in detection and subtyping using plain CT images. Outperforming radiologists, it distinguished and subtyped echinococcosis and demonstrated promising potential for clinical use in underdeveloped settings. Yang et al.20 introduced a ResNet-50-based deep CNN for automated hepatic echinococcosis detection, demonstrating high accuracy and outperforming other diagnostic tools, with the potential to enhance diagnosis in vast high-endemic and remote regions. De Souza et al.21 have developed a cross-platform AI app for leprosy screening, offering 93.97% sensitivity and 87.09% specificity. This tool has proven valuable in remote areas, complementing diagnostics where specialist access is limited. Ward et al.22 presented an AI-based digital pathology device for helminth egg detection in Kato-Katz stool samples, achieving 94.9% precision and 96.1% recall. The device enhances affordable soil-transmitted helminth diagnostics and offers the ability to detect multiple infections simultaneously, with minimal reliance on prior knowledge of prevalence in affected areas. Lin et al.23 propose a novel approach, using crowd-sourced annotations from a video game, to train AI models for soil-transmitted helminthiasis detection. The models show comparable performance to expert annotations, indicating their potential to supplement or even replace the traditional stool microscopy, which is time-consuming, requires specialized training, and demands high expertise.
The literature investigated the potential of AI algorithms in predicting and analyzing NTD outbreaks and NTD-vector dynamics. Kumar et al.24 employed a Radial Basis Function (RBF) kernel-based Support Vector Regression (SVR) model to assess the impact of changing climate on Visceral leishmaniasis (VL) outbreaks. The model efficiently predicts VL cases, outperforming both linear regression and multilayer perceptron models. It enables rapid case detection even with limited data, helping public health authorities understand the climate impacts on outbreaks and ensuring more timely health services. Yang et al.25 utilized an AI approach, combining XGBoost and SHAP methods, to analyze dengue fever spatial patterns. The findings reveal insights into complex transmission dynamics, guiding precise prediction and resource allocation in high-risk zones.
The literature investigated how AI facilitates NTD case management and patient retention in care in conditions where patients’ regular follow-up is not possible. Rodrigues et al.26 presented an AI system that assesses the risk of leprosy patients developing reactions by integrating clinical, demographic, and genetic data. The system achieved 82.7% accuracy and offers the potential to prevent permanent disabilities through its user-friendly, online, and free-access platform that could positively impact the quality of life of patients and enhance leprosy control programs. Singh et al.27 introduced an AI-based cyber-physical system (CPS) for Chikungunya severity classification, incorporating a superior adaptive crossover-based genetic algorithm – random forest (ACGA-RF) model. The system outperformed other models, enabling remote services and reducing hospital visits. Brito et al.28 evaluated an AI-enabled digital ECG algorithm’s ability to detect left ventricular systolic dysfunction (LVSD) in patients with Trypanosoma cruzi, revealing an Area Under the Curve (AUC) of 0.838. This finding demonstrates the algorithm’s potential for identifying LVSD in these patients and suggests it could serve as a universal, cost-effective tool that optimizes the use of public health resources.
Drones
Four studies29,30,31,32 investigated the role of drones in the NTDs sector. Annan et al.29 explored the acceptance and willingness of communities regarding the use of drones for mosquito surveillance in dengue prevention programs. Tech-savvy communities demonstrated a high willingness to download a mosquito surveillance app, highlighting widespread support for drone use in mosquito control. The research suggests a strong prospect of involving local communities in drone-based mosquito surveillance, while also highlighting the need for ongoing discussions and qualitative research to address concerns related to privacy and community expectations.
Valdez-Delgado et al.30 utilized drones to assess larval breeding sites in the roofs and backyards of houses as a consequence of the COVID-19 pandemic affecting Aedes aegypti control programs. This proved more effective in detecting inaccessible containers, such as plastic buckets, than traditional ground surveillance. Implementing drone-based surveillance could significantly enhance Aedes aegypti monitoring in household environments, contributing to more effective vector control in dengue-endemic countries.
Mushi31 proposes the use of drone-based remote sensing technology for Simulium surveillance, emphasizing its potential to identify breeding sites, map microenvironments, and recommend control measures, facilitating the integration of Simulium control with the longstanding Community-Directed Treatment with Ivermectin used for sustainable onchocerciasis control. The findings demonstrate that drone-based technology can provide crucial insights into inaccessible parts of rivers and streams, aiding decision-making regarding larviciding or ground control efforts like slashing and clearing.
Nisingizwe et al.32 assessed the drone delivery that Rwanda implemented to enhance blood product accessibility, demonstrating a reduction in delivery times of 49.6 min compared to traditional road methods. The study also revealed a 67% reduction in expiry of blood units in health facilities, suggesting that drone delivery not only improves efficiency but also minimizes blood component wastage. The paper suggests that drones could also be used for delivering time-sensitive medical supplies in Africa, and the high number of completed deliveries indicates that drone delivery is feasible in other resource-limited settings with remote facilities.
Mobile clinics
Two studies33,34 demonstrate the potential of mobile clinics in the NTDs sector. Gnimavo et al.33 assessed the use of mobile clinics for early detection and treatment of patients with skin NTD manifestations, reporting that mobile clinic teams offered an efficient and sustainable strategy for integrated screening and could contribute to reducing the burden of NTDs in resource-limited countries.
Frade et al.34 established a mobile clinic at the main bus terminal to detect new leprosy cases in a district which has been considered a non-endemic area. The results revealed unexpected high percentage of leprosy cases and high number of individuals with positive serological responses to M. leprae antigens, with a 10.1% positivity rate for leprosy among evaluated individuals. The study suggests that this approach holds promise for screening and identifying people at high risk of such NTDs who could benefit from regular monitoring.
Nanotechnology
Seven studies35,36,37,38,39,40,41 investigated the potential application of nanotechnology in the NTDS sector, aiming to explore alternative treatment options for NTDs that offer shorter durations and improved safety profiles. Rolon et al.35, Branquinho et al.36, and Sposito et al.37 found encouraging early-stage results in utilizing nanotechnologies for the development of new drugs for T. cruzi or strategies to enhance the effectiveness of benznidazole and nifurtimox. Similarly, Ibrahim et al.38, Eissa et al.39, and Silva et al.40 have demonstrated that nano-combinations can enhance the therapeutic profiles of drugs against Schistosoma mansoni. Nanotechnology: A promising strategy for the control of parasitic infections.
AlGabbani41 demonstrates the promise of nanotechnology for the control of parasitic infections, spanning from the efficient purification of water, decontamination of polluted sites, and the development of chemical insecticides targeting NTD vectors. The paper reports that nanotechnology may play a critical role in advancing vaccines and diagnostics for NTDs. Nanoparticle-based diagnostic biosensors offer a means to achieve accurate and timely laboratory results, while nanoparticle-based vaccine delivery systems enhance immunogenicity, fostering a long-lasting immune response41.
Telemedicine
Three studies42,43,44 investigated the potential of telemedicine in the NTDs sector, determining its utility in remote NTD consultations among clinicians and between clinicians and patients (Table 3). Pedrott et al.42 evaluated telemedicine consultations during a dengue outbreak to reduce the need for face-to-face consultations. Among 4626 suspected dengue patients, 2003 tested positive for dengue, 1978 were classified as low-moderate risk, and 267 underwent telemedicine evaluation. Following telemedicine assessment, 252 patients (94.4%) were discharged, and only 15 (5.6%) were referred for immediate face-to-face medical evaluation, demonstrating the potential of telemedicine as a cost-effective strategy during epidemiological outbreaks in a field hospital setting.
Messagier et al.43 assess the effectiveness of telemedicine in dermatology in a region with scattered settlements and limited healthcare access. The system demonstrated high utility, with over 85% of peripheral centers finding it fast, useful, and educationally beneficial, indicating its potential to provide specialized dermatology care in remote areas.
Campanella et al.44 assess a teleconsultation system used by primary healthcare clinicians seeking remote support for diagnosing skin conditions. While high turnover and lack of e-health training of clinicians result in low quality of teleconsultation, the system shows a high presumptive diagnosis agreement (72%) with dermatologist consultants, highlighting the need for enhanced e-health tool training to improve teleconsultation quality in regions with limited access to specialists.
Augmented reality
Three studies45,46,47 demonstrate the promise of augmented reality in the NTDs sector, despite it is a relatively recent development in skill-based training for healthcare professionals. Naufal et al.45 developed a hands-free augmented reality smartphone camera system to document the prevalence of active trachoma. This system facilitates users to evert the eyelid and take, store, and upload photographs to a virtual Reading Center for standardized grading. Examining 1305 children aged 1–9 years for trachomatous inflammation-follicular in Tanzania, the system demonstrated potential in eliminating the costly grader standardization typically required in trachoma prevalence studies. Bazian et al.46 employed augmented reality combined with mobile web geographical information system to design and develop a geospatial dengue information system aimed at improving analytical functions and data management for dengue outbreaks. The augmented reality component manages and visualizes epidemiological data, offering valuable visualization and predictive simulation capabilities. Interactive dengue maps enable users to identify patterns, trends, and distributions of dengue outbreaks while disseminating epidemic information to the public through web-based and mobile applications. Schnabel et al.47 developed and evaluated three-dimensional transfers to represent skin conditions in simulation-based health professions education. The authors successfully developed and deployed over 40 different three-dimensional transfers, including one for scabies that shows various clinical findings. Feedback from students and examiners after the objective structured clinical examinations was largely positive, leading healthcare educators to adapt and replicate these transfers for their own use.
Advanced point-of-care diagnostics
Six studies48,49,50,51,52,53 investigated advanced point-of-care diagnostics for their potential in NTD diagnosis, including technologies such as loop-mediated isothermal amplification (LAMP) and polymerase chain reaction (PCR) that allow for the precise identification of specific NTDs (Table 4).
Salas-Coronas et al.48 evaluated the LAMP technique’s effectiveness for diagnosing schistosomiasis in migrants from African countries, showing higher sensitivity but lower specificity than microscopy. Taslimi et al.49 developed a non-invasive tape disc-LAMP method for detecting Leishmania tropica kinetoplast DNA, demonstrating (97%) and specificity (100%) in skin samples. It presents a rapid and non-invasive diagnostic tool for cutaneous leishmaniasis in disease-endemic settings. Longhi et al.50 assessed LAMP for rapid congenital T. Cruzi DNA diagnosis in dried blood spots, resulting in a limit of detection of 5 and 20 parasites/mL for heparinized fluid blood and dried blood spots, respectively, encouraging further studies for operational evaluation. Febrer-Sendra et al.51 introduced a colorimetric LAMP assay for Loa loa DNA detection, demonstrating potential as a rapid and accurate screening tool for loiasis in low-resource settings.
The integration of microfluidics and lab-on-a-chip technologies advances POC diagnostics to provide rapid, accurate, and affordable tests [Table 4]. Maeno et al.52 explored the sensitivity of a 3D microfluidic ELISA in detecting severe dengue biomarkers (soluble CD163, sCD163) in serum matrix. The unmodified 3D Stack exhibited reduced analyte recovery, but modification with 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide - N-hydroxysuccinimide (EDC-NHS) coupling improved sensitivity, demonstrating potential for further development. Nielsen et al.53 utilized a custom stereolithography 3D printer to create microfluidic devices for chikungunya oligonucleotide and viral RNA detection, suggesting efficiency for rapid case detection. Integrating biosensors and immunochromatographics into POC diagnostic devices will simplify and speed up NTD detection, automating laboratory procedures.
Mobile phone-based health technologies
Seven studies54,55,56,57,58,59,60 investigated the potential of mobile health (mHealth) technologies in a wide range of NTD-related services [Table 5]. Ali et al.54 employed a smartphone app for screening individuals with suspected scabies symptoms, finding high prevalence of itch (90%) and rash (76%). The app accurately identified 5% of screened cases as having a high risk of scabies, highlighting its utility for scabies screening in primary care settings. Debrah et al.55 assessed the efficacy of a mobile phone-based Interactive Voice Response System (mIVRS) for reporting lymphatic filariasis and acute dermatolymphangioadenitis cases by community health volunteers, revealing higher recorded numbers compared to paper-based records. The system holds promise in addressing underreporting of cases in endemic communities. Swathi et al.56 developed a user-friendly mobile app (RabiApp) designed for healthcare professionals to deliver information on rabies. The app proved to be highly usable and reliable, aiding healthcare professionals in making informed decisions regarding rabies wound management, treatment, and prophylaxis, particularly in areas with limited access to post-exposure prophylaxis.
Chewi et al.57 employed mobile phone cameras to capture urine colour for assessing dehydration severity in patients with dengue fever. The study revealed robust correlations between urine colour index values and urine osmolality and specific gravity, suggesting the potential of urine colorimetry using mobile phones for evaluating hydration status in patients with dengue fever. Snyder et al.58 validated smartphone photography for trachoma conjunctival examination in preschool children, demonstrating high agreement with field grading. The results highlight the potential utility of smartphone photography for assessing and monitoring trachoma elimination programs, especially in resource-constrained settings. Bhattarai et al.59 evaluated the effectiveness of a mobile SMS intervention to enhance knowledge and practices of dengue-affected communities, revealing significant improvements in individuals who used the intervention, indicating its promise as a tool for health education in dengue prevention. Koydemir et al.60, utilized a smartphone 3D-printed microscope to rapidly capture images of stool or urine specimens for S. mansoni and S. haematobium egg detection. The study emphasized the broad clinical and public health applications of this innovative technology for schistosomiasis diagnosis.
Wearable sensors
Two studies61,62 explored the potential of wearable sensors for NTD interventions. Martins et al.61 introduced an electrochemical immunosensor for the diagnosis of visceral leishmaniasis, addressing limitations like low antibody concentration and cross-reactions. Utilizing a screen-printed carbon electrode modified with gold nanoparticles, the immunosensor demonstrates high selectivity (100%) and specificity, outperforming ELISA, with a detection limit of 200 ng mL-1 for distinguishing various leishmaniasis types.
Arshad et al.62 presented a molecularly-imprinted polymer-based impedimetric sensor for early detection of dengue infection, achieving a linear response in the concentration range of 1–200 ng/mL for the specific biomarker non-structural protein 1 (NS1), with 100% selectivity and a low detection limit of 0.3 ng/mL. These sensors could be directly attached to human skin or connected via devices to offer an alternative approach for diagnosing, monitoring, or following up with patients with NTDs, while also being integrated with information technology to remotely provide clinicians with relevant information.
Discussion
This paper examines the interplay between NTDs and sociopolitical instability in Africa and explores innovative technologies in the NTD sector that Africa can leverage amidst such instability. Key findings indicate that African countries experiencing sociopolitical instability are also heavily burdened by NTDs, with the continent ranking second globally in NTD prevalence and first in internal displacement in 2023. The systematic review identified 46 relevant studies examining technologies for their potential in preventing, predicting, surveilling, diagnosing, treating, and managing NTDs. Classified by technology type, the studies investigated nine innovative technologies: AI, drones, mobile clinics, nanotechnology, telemedicine, augmented reality, advanced point-of-care diagnostics, mobile health solutions, and wearable sensors.
The analysis of the two study datasets demonstrates that NTDs are predominantly concentrated in low- and middle-income countries (LMICs), including those in Africa. It also shows that technologies for NTDs are being studied and developed specifically to address the needs of these NTD-endemic LMICs, aiming to reach most-affected, disadvantaged, vulnerable, and hard-to-reach populations as outlined in the WHO NTD 2030 Roadmap3. Considering Africa’s vulnerability to a double burden of NTDs and sociopolitical instability, discussions of the paper heavily relay on providing analysis of how Innovative technologies in the NTDs sector could be cultivated to address NTDs in African settings with persistent sociopolitical instability.
The systematic review demonstrates that AI holds significant promise in the NTDs sector for rapid and accurate NTD diagnosis17,18,19,20,21,22,23, predicting and analyzing potential NTD outbreaks and vector dynamics24,25, and enhancing case management and patient retention in hard-to-reach and underdeveloped areas26,27,28 Consistent with current findings, previous studies highlight the potential of AI-based tools to assist underserved and war-affected communities by serving as psychiatric aids, predicting mental health disorders early, detecting subtle patterns, and providing timely and accurate interventions through analysis of neuro-psycho-physiological and linguistic features63,64,65. Similarly, previous studies show AI’s potential to deploy surgical robots in conflict zones66 make decisions in case of severe trauma in hospitals of higher roles67, and reduce care inequalities by optimizing resource allocation and expanding access to medical care in underserved communities when designed effectively68,69,70. AI shows potential enhancing emergency management by rapidly processing and analyzing diverse data sources to improve public health response and streamline decision-making71. In Africa, studies underscore the considerable potential of AI to transform and improve healthcare systems on the continent, despite it still being in the developmental and exploratory phases72,73,74,75,76. Triangulating this evidence, AI-enabled NTD diagnostic platforms could be crucial for African countries facing dual burden of NTDs and sociopolitical instability, enabling rapid detection, predicting outbreaks, and improving case management and patient retention in conflict-affected areas.
Findings of the systematic review reveal that drones can enhance NTD surveillance by engaging local communities29, facilitate detection of NTD vectors in hard-to-reach areas like rivers and streams30,31, and provide efficient and timely delivery of time-sensitive essential products such as blood in African contexts32. In agreement with the findings, previous literature demonstrate drone functionalities in crisis response, where they can provide critical information through mapping of crisis-affected areas and timely delivery of aid supplies to populations in need77,78,79. Various studies also emphasize the potential of drones in African countries80,81,82,83. Given this potential, Ministries of Health in conflict-affected African regions—where healthcare infrastructure and transportation networks are often disrupted—could employ drones to ensure the efficient delivery of essential NTD diagnostic, therapeutic, and preventative products. In situations where the routine logistics systems of the government are disrupted and public health concerns are jeopardized, drones could be mobilized by development partners and other responsible entities to bridge the gap. These technologies could also help to enhance NTD surveillance in such settings, and, equipped with advanced imaging and sensing technologies, could monitor NTD vectors and environmental conditions to provide real-time data for epidemiological analysis and prompt interventions. However, considering the nascent nature of this technology in African settings, there is a need for additional feasibility studies, local expert training, and community awareness initiatives to ensure effective implementation. Studies underscore the importance of addressing concerns about privacy, security, safety, and technical efficiency, along with community apprehensions about drones as military weapons, in order to successfully adopt drone technology for specialized healthcare delivery77,78,79,84,85. These issues must be thoroughly examined in African contexts to ensure the effective use of drones in the continent.
The systematic review highlights the vital role of mobile clinic technology in the NTDs sector for early detection and treatment of patients33, as well as identifying new cases in non-endemic areas34, thereby contributing to the elimination of NTDs and the goals of the NTD 2030 Roadmap. Recent studies show that in fragile and conflict-affected settings, mobile clinics can effectively deliver essential healthcare to vulnerable and isolated populations who lack access to regular services86,87. In Africa, examples such as the mobile clinic with emergency mobile medical teams deployed by the WHO in South Sudan88, mobile clinics providing differentiated HIV services in conflict-affected regions of Cameroon89, and mobile clinics addressing health issues in conflict-affected regions of Niger90 illustrate the significant potential of mobile clinics across the continent. Taking these potentials into account, mobile clinics could have a vital role in the prevention and control of NTDs amid periods of instability in African settings. By providing necessary NTD healthcare services to displaced populations, acting as fast response units during NTD outbreaks, and launching health education and awareness campaigns about NTDs, they can address issues resulting from the disruption of healthcare infrastructure and processes.
The systematic review found that nanotechnology can enhance the efficacy and safety of anti-NTD drugs and facilitate the prevention and control of NTDs and NTD vectors35,36,37,38,39,40,41. Several NTDs require prolonged drug treatments due to their chronic nature or the risk of recurrence. While these medications are essential for managing NTDs, there are associated challenges such as side effects, drug resistance, non-adherence to treatment, drug discontinuation, out-of-pocket costs, and reduced quality of life for patients. These are exacerbated by disruptions linked to political instability. Nanotechnology has emerged as a promising avenue for the discovery and development of drugs, vaccines, and diagnostics91,92. and LMICs are working to cultivate its applications in various sectors93. In Africa, R&D in nanotechnology is progressing, with countries like Nigeria, Ethiopia, Kenya, South Africa, and Egypt exploring its potential within their specific contexts94,95,96,97,98,99. For Africa, it is crucial to engage in continuous research and collaboration with the global scientific community to fully harness the potential of nanotechnologies in the fight against NTDs. By understanding the unique properties of nanotechnologies, NTD interventions in African settings can be made more adaptive, efficient, and sustainable. African scientists need to be part of this technology, which is about strengthening the capacity of human resources and developing the necessary R&D infrastructure.
The systematic review highlighted the potential of telemedicine for facilitating remote NTD consultations. In conflict-affected countries like Somalia100, Palestine101, Ukraine102, Pakistan103, Syria104, and others105,106,107,108, telemedicine has shown promise in facilitating access to health services, information, and training amidst sociopolitical instability. In Africa, the technology has gained prominence as a key health innovation in research and development, with various governments, international partners, and health organizations working to enhance the capacity of African countries to study and implement telemedicine systems effectively109,110,111,112,113. Given this evidence and potential, telemedicine holds the promise of maintaining essential NTD services in Africa during periods of sociopolitical instability, when access to health facilities and professionals is limited or disrupted.
Augmented reality platforms have been shown to facilitate NTD interventions by documenting the prevalence of active trachoma45, designing and developing geospatial NTD information systems46, and representing skin conditions in simulation-based health professions education47. The findings align with studies that highlight the potential of augmented reality technology in various areas, including health emergency management114 and enhancing the training of healthcare professionals115,116,117. In Africa, augmented reality has shown promise in improving surgical access and quality, particularly its favorable use in Somalia by the United States Army Special Operations Forces to stabilize life-threatening injuries118 and its application in Africa in reducing reliance on external short-term surgical experts’ visits while enhancing surgical education and mentorship119. Hence, in African settings where traditional training and education programs are compromised due to instability, augmented reality technology can facilitate NTD skills development for a large number of healthcare professionals. Through simulations, professionals can interact with three-dimensional models and observe simulated medical scenarios, all without the need for off-site training, thereby gaining deeper decision-making and coordination skills to respond effectively and efficiently.
Analysis of the systematic review emphasizes the potential of advanced point-of-care NTD diagnostics, impowered by molecular assays, microfluidics, and biosensors48,49,50,51,52,53, to quickly and effectively analyze specimens without expert interventions, combined with their affordability, precision, and appropriateness for use in LMICs. Previous studies have examined the utility of point-of-care and rapid diagnostic tests in conflict-affected and humanitarian emergency settings, yielding promising results that encourage vulnerable countries and development agencies to incorporate these tests into their essential diagnostics as part of national preparedness and response plans120,121,122. In Africa, where conventional laboratory diagnostics are unlikely to close the diagnostic gap123, there is a pressing need to develop and assess the effectiveness and utility of advanced point-of-care diagnostics, especially for NTDs that receive minimal attention in the global diagnostic landscape. Such diagnostics are crucial in sociopolitically unstable African settings duly overburdened by NTDs.
mHealth has shown to enhance NTD-related screening and disease monitoring54,57,58,60, information exchange and reporting55,56, and community health education59. The effectiveness of mHealth in reaching populations in conflict-affected areas is well established107,124. Studies conducted in regions experiencing armed conflict, forced migrations, or other sociopolitical instability—such as Somalia125, Ethiopia126, Uganda127, Nigeria128, and Ukraine129—highlights the potential of mHealth technology to monitor the health and well-being of affected individuals and gather essential health data. Hence, mHealth may empower Africa to extend NTD services to individuals facing challenges in traveling or accessing physical healthcare facilities amidst sociopolitical instability. The technology will enable remote NTD diagnosis and medication prescription, while also supporting self-management of chronic NTD treatments by providing patients with information and reminders for medications and appointments to ensure person-centered care.
Wearable sensors have shown to provide timely and accurate diagnosis of NTDs61,62. In conflict-affected settings, humanitarian wearables are conceptualized as smart devices that can be placed on or inside the bodies of aid beneficiaries for tracking and protecting health, safety and nutrition130. In Africa, studies have explored the potential of wearable sensors as a viable alternative to traditional patient monitoring131,132 and large datasets generation among vulnerable populations133. Thus, wearable sensors can serve as a flexible alternative technology for NTD interventions in Africa, providing a dynamic approach to monitoring and managing these diseases in contexts of sociopolitical instability.
Although these innovative technologies hold much promise in NTD interventions in Africa, studies highlight valid concerns in the health technology implementation ecosystem that require careful consideration for successful deployment134,135,136. Technological advancement is closely linked to economic development, skilled workforce, and a strong commitment to change. Hence, a number of obstacles impede the effective implementation and integration of health technologies in Africa137,138. These challenges include the continent’s inadequate infrastructure, financial constraints, cybersecurity concerns, and inequities in healthcare access139,140. Investing in robust and modular technologies such as solar-powered energy sources141 and portable devices may bridge these gaps. The initial technology and expertise expenses associated with acquiring and implementing the technologies may pose substantial challenges as many African countries are already facing budget constraints and competing priorities. To overcome this, African Ministries of Health should proactively leverage partnerships with funding agencies, non-governmental organizations, research institutions, and the private sector. These include their role in shaping NTD policies, developing guidelines, implementing targeted programs, and ensuring the resilience of health systems. These partnerships would also aim to secure funding, facilitate resource-sharing, promote joint initiatives, and engage in negotiations to obtain favorable pricing, thereby overcoming financial barriers. Undertaking further research into the cost benefits of implementing these health technologies and prioritize based on specific contexts and needs may demonstrate health and economic efficiencies in the longer term and enable securement of investment. Cybersecurity concerns add a layer of complexity to the successful deployment of health technologies142. Maintaining the confidentiality and integrity of health information is of utmost importance, even more so in conflict-affected areas, necessitating the implementation of robust cybersecurity measures, including collaborative initiatives with international experts, the establishment of secure data management protocols, and the adoption of state-of-the-art encryption technologies. African governments are seeing promising results from their efforts to develop policies and legislation aimed at addressing cybersecurity concerns143.
African scientists must be actively involved in advancing these technologies, which not only enhances human resource capacity but also fosters the development of essential infrastructure across the continent. NTDs might not be prioritized since they primarily affect low-income countries2,11,12. However, with African scientists taking the lead in collaboration with the global scientific community, significant breakthroughs and effective knowledge translation are more likely to occur. Studies indicate that building expertise capacity for well-designed longitudinal studies are critical for successful evaluation and return on investment in health technology144,145,146. The NTD 2030 Roadmap3 emphasizes the critical importance of incorporating safer and effective technologies to accelerate NTD programmatic action, with a clear directive to ensure that no one is left behind.
In summary, this paper explores how innovative technologies can help Africa address NTDs amidst such instability. The analysis reveals that African countries facing sociopolitical instability also bear a high burden of NTDs, with the continent ranking higher globally in NTDs and internal displacement. By integrating insights from various datasets and a systematic review of the literature, the paper discusses nine promising technologies—artificial intelligence, drones, mobile clinics, nanotechnology, telemedicine, augmented reality, advanced point-of-care diagnostics, mobile health Apps, and wearable sensors—that could enhance Africa’s response to NTDs amidst sociopolitical instability. The paper suggests that African Ministries of Health assess the feasibility of implementing these technologies within their specific contexts, incorporating them into their National NTD Masterplans, and actively participating in the ongoing dialogue regarding their translation into health systems. By doing so, African Ministries of Health can establish resilient health systems driven by technology, ensuring the effective deployment of health technologies to those in greatest need, thereby contributing to the achievement of the NTD Roadmap and other global health goals. As stability gradually returns, the technologies can transition to supporting more comprehensive healthcare services, thereby laying the groundwork for sustainable health developments.
Methods
This study employed multiple approaches, including secondary data analysis, a systematic review of existing literature, and the authors’ expertise and experience to enhance and triangulate the findings. Data were drown from the WHO Global Health Observatory4, WHO Mortality Database5, WHO Global Report on NTDs 20232, and the United Nations High Commissioner for Refugees (UNHCR)6, to establish a foundation of evidence on the comparative burden of NTDs and sociopolitical instability in Africa. Through review of studies in major databases, the paper identifies technological advancements in the NTD sector. Triangulating insights from these sources and the authors’ extensive expertise and experience, the paper reviews promising solutions for African Ministries of Health to combat NTDs during periods of instability.
Secondary data analysis
We conducted a review of UNHCR global data portals and UNHCR global reports to gather the most current data available on sociopolitical instability. Data were collected on eight key variables: refugees (per 100,000 population), refugees (number), forcibly displaced (number), internally displaced (number), asylum-seekers (number), deaths in armed conflicts (number), countries (name), regions (name). Data from officially released recent reports of the UNHCR were reviewed to supplement the data obtained from UNHCR portals. With descriptive analysis, we summarized the findings, both globally and with a particular emphasis on Africa. We compared Africa’s status with that of other regions worldwide and identified the most affected countries, assessing African countries’ positions relative to the global scenario. Trends were summarized in figures and described narratively. UNHCR works with data and statistics to gain important insights that aid in saving, protecting, and enhancing the lives of refugees and other forcibly displaced and stateless individuals.
Similarly, we conducted a review of WHO data portals to gain a comprehensive understanding of the current global burden of NTDs, with a specific emphasis on Africa. Key portals reviewed included the WHO Global Health Observatory for credible data on priority health issues, the WHO Mortality Database for data on causes of death, and the WHO Global Report on NTDs 2023 for updated global, regional, and national data on NTDs. This involved abstraction and assessment of key variables including the number of people in need of NTD interventions and the disease burden attributed to each NTD. We compared Africa’s standing in relation to other regions and identified prevalent NTDs in current times. Additionally, we reviewed WHO’s different NTD reports to gain more insights into the efforts being made by Ministries of Health in Africa to mitigate the NTD burden and their progress thus far.
Through integrated analysis of data from these sources, we made further analysis of the dual burden posed by NTDs and sociopolitical instability in Africa to assess the potential impact of this dual burden on Ministries of Health. Using WHO data portals, we identified the top 15 African countries with significant NTD intervention needs, and cross-referenced this data descriptively with number of refugees, asylum-seekers, and IDPs in each country. With further analysis of the findings from the reviewed literature and data portals, and triangulating all the findings with our own extensive experiences and expertise, we proposed and described potential NTD technological breakthroughs during sociopolitical instability in Africa.
Systematic review and analysis of the literature
We conducted a systematic review of scientific literature utilizing the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2021 guidelines.
Search strategy
We systematically searched PubMed/MEDLINE, Embase, Scopus, and Google Scholar to identify studies investigating the effectiveness, efficacy, feasibility, acceptability, usability, or impact of health technological breakthroughs on NTDs. We used predefined MeSH or free-text terms referring to “neglected tropical disease” AND “technology,” OR “innovation,” OR “digital,” OR “advance,” searching from January 1, 2015, to January 1, 2024, with no language, study design, setting and comparator restrictions. We manually searched the WHO website, Google search engine, and reference lists of included studies to gather additional potential articles. The Supplementary Information presents a flow diagram summarizing the study process.
Eligibility
Based on the PICOS criteria, studies were eligible for inclusion if they met the following criteria:
-
Participants: Eligible participants included patients, healthcare professionals, data collectors, or healthy individuals of any gender and age. There were no restrictions on participant demographics.
-
Interventions: Studies focusing on health technologies and innovations in the NTDs sector were considered.
-
Comparisons: Studies did not need to include a comparison condition to be eligible for inclusion.
-
Outcome: Studies assessing potential accuracy, efficacy, safety, feasibility, usability, affordability, acceptability, or related outcomes were included without specific restrictions.
-
Study design: All types of study designs were eligible.
Study selection
Two reviewers individually screened the titles and abstracts of all articles found in the initial search for eligibility. Duplicates and publications that did not meet the inclusion criteria based on their title and abstract were excluded. The full texts of the remaining publications were then thoroughly examined. Any disagreements between the authors were resolved through consensus, and if necessary, a third author was consulted for arbitration.
Data extraction and analysis
Key variables of interest, including the technology under investigation, NTD studied, participant characteristics, study design, outcome measures, major findings, first author’s surname, country, and year of publication, were extracted and summarized in a table. Selected studies were categorized according to the type of technology assessed. A qualitative content analysis of all studies was conducted, with each article summarized and data reported descriptively. The review placed less emphasis on assessing the quality of the included literature, as it was not the primary objective.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The authors declare that all data generated and analyzed during the current research are included in this article. The data that support the findings of this study were derived from the following open-access public domain resources: the WHO Global Health Observatory, WHO Mortality Database, WHO Global Report on NTDs 2023, and the United Nations High Commissioner for Refugees (UNHCR). Data from available literature triangulates the findings.
References
The United Nations High Commissioner for Refugees (UNHCR), the UN Refugee Agency. UNHCR Global Report 2023. (UNHCR 2023, Copenhagen, Denmark, accessed 09 September 2024); https://reporting.unhcr.org/global-report-2023.
World Health Organization (WHO). Global Report on Neglected Tropical Diseases 2023. (WHO 2023, Jeneva, Switzerland, accessed 15 September 2023); https://www.who.int/publications/i/item/9789240067295.
World Health Organization (WHO). Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. WHO 2021, Geneva, Switzerland, accessed 12 September 2023); https://www.who.int/publications/i/item/9789240010352.
World Health Organization (WHO). WHO Global Health Observatory. (WHO 2023, Geneva, Switzerland, accessed 03 September 2023); https://www.who.int/data/gho.
World Health Organization (WHO). WHO Mortality Database. (WHO 2023, Geneva, Switzerland, accessed 03 September 2023); https://platform.who.int/mortality.
The United Nations High Commissioner for Refugees (UNHCR), the UN Refugee Agency. UNHCR Global Appeal 2024. (UNHCR 2023, Copenhagen, Denmark. accessed 05 December 2023); https://reporting.unhcr.org/global-appeal-2024.
Zhai, J. et al. Drug screening on digital microfluidics for cancer precision medicine. Nat. Commun. 15, 4363 (2024).
Tan, R. et al. A digital health algorithm to guide antibiotic prescription in pediatric outpatient care: a cluster randomized controlled trial. Nat. Med. 30, 76–84 (2024).
Bălăet et al. Online cognitive monitoring technology for people with Parkinson’s disease and REM sleep behavioural disorder. NPJ Digit. Med. 7, 118 (2024).
Choi, J. Y. et al. Information technology-supported integrated health service for older adults in long-term care settings. BMC Med. 22, 212 (2024).
Rust, J. et al. Innovate to eliminate: a prerequisite in NTD programmes. Int. Health 14, ii20–ii24 (2022).
Webel, M. K. Parasites and priorities: the early evolution of ‘neglected disease’ initiatives and the history of a global health agenda. Med. Humanit. 48, 177–189 (2022).
World Health Organization (WHO). Target Product Profile for a Diagnostic Test to Confirm Cure of Visceral Leishmaniasis. (WHO 2024, Geneva, Switzerland, accessed 30 June 2024); https://www.who.int/publications/i/item/9789240091818.
World Health Organization (WHO). Target Product Profile to Detect “Dracunculus Medinensis” Presence in Environmental Samples. (WHO 2024, Geneva, Switzerland, accessed 28 April 2024); https://www.who.int/publications/i/item/9789240090781.
Ferreira, L. L. G., de Moraes, J. & Andricopulo, A. D. Approaches to advance drug discovery for neglected tropical diseases. Drug Discov. Today 27, 2278–2287 (2022).
Mohan et al. Estimating the global demand curve for a leishmaniasis vaccine: a generalisable approach based on global burden of disease estimates. PLoS Negl. Trop. Dis. 16, e0010471 (2022).
Milad, D., Antaki, F., Robert, M. C. & Duval, R. Development and deployment of a smartphone application for diagnosing trachoma: leveraging code-free deep learning and edge artificial intelligence. Saudi J. Ophthalmol. 37, 200–206 (2023).
Yotsu, R. R., Ding, Z., Hamm, J. & Blanton, R. E. Deep learning for AI-based diagnosis of skin-related neglected tropical diseases: a pilot study. PLoS Negl. Trop. Dis. 17, e0011230 (2023).
Wang, Z. et al. Detection and subtyping of hepatic echinococcosis from plain CT images with deep learning: a retrospective, multicentre study. Lancet Digit. Health 5, e754–e762 (2023).
Yang, Y. et al. Ultrasound identification of hepatic echinococcosis using a deep convolutional neural network model in China: a retrospective, large-scale, multicentre, diagnostic accuracy study. Lancet Digit. Health 5, e503–e514 (2023).
De Souza, M. L. M., Lopes, G. A., Branco, A. C., Fairley, J. K. & Fraga, L. A. O. Leprosy screening based on artificial intelligence: development of a cross-platform app. JMIR Mhealth Uhealth 9, e23718 (2021).
Ward, P. et al. Affordable artificial intelligence-based digital pathology for neglected tropical diseases: a proof-of-concept for the detection of soil-transmitted helminths and Schistosoma mansoni eggs in Kato-Katz stool thick smears. PLoS Negl. Trop. Dis. 16, e0010500 (2022).
Lin, L. et al. Combining collective and artificial intelligence for global health diseases diagnosis using crowdsourced annotated medical images. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 3344–3348 (2021).
Kumar, S., Srivastava, A. & Maity, R. Modeling climate change impacts on vector-borne disease using machine learning models: case study of Visceral leishmaniasis (Kala-azar) from Indian state of Bihar. Expert Syst. Appl. 237, 121490 (2024).
Yang, H., Nguyen, T. N. & Chuang, T. W. An integrative explainable artificial intelligence approach to analyze fine-scale land-cover and land-use factors associated with spatial distributions of place of residence of reported dengue cases. Trop. Med. Infect. Dis. 8, 238 (2023).
de Andrade Rodrigues, R. S. et al. Prediction of the occurrence of leprosy reactions based on Bayesian networks. Front. Med. 10, 1233220 (2023).
Singh, D., Kaur, M., Kumar, V., Jabarulla, M. Y. & Lee, H. N. Artificial intelligence-based cyber-physical system for severity classification of chikungunya disease. IEEE J. Transl. Eng. Health Med. 10, 3700109 (2022).
Brito, B. O. F. et al. Left ventricular systolic dysfunction predicted by artificial intelligence using the electrocardiogram in Chagas disease patients-The SaMi-Trop cohort. PLoS Negl. Trop. Dis. 15, e0009974 (2021).
Annan, E. et al. Community acceptability of dengue fever surveillance using unmanned aerial vehicles: a cross-sectional study in Malaysia, Mexico, and Turkey. Travel Med. Infect. Dis. 49, 102360 (2022).
Valdez-Delgado, K. M. et al. Field effectiveness of drones to identify potential aedes aegypti breeding sites in household environments from Tapachula, a Dengue-Endemic City in Southern Mexico. Insects 12, 663 (2021).
Mushi, V. Simulium surveillance and control in Mahenge, Tanzania: time to think bigger and utilize drone-based remote sensing technology. Bull. Natl. Res. Cent. 47, 38 (2023).
Nisingizwe, M. P. et al. Effect of unmanned aerial vehicle (drone) delivery on blood product delivery time and wastage in Rwanda: a retrospective, cross-sectional study and time series analysis. Lancet Glob. Health 10, e564–e569 (2022).
Gnimavo, R. S. et al. Importance of consultations using mobile teams in the screening and treatment of neglected tropical skin diseases in Benin. PLoS Negl. Trop. Dis. 17, e0011314 (2023).
Frade, M. A. et al. Unexpectedly high leprosy seroprevalence detected using a random surveillance strategy in midwestern Brazil: a comparison of ELISA and a rapid diagnostic test. PLoS Negl. Trop. Dis. 11, e0005375 (2017).
Rolon, M. et al. Solid nanomedicines of nifurtimox and benznidazole for the oral treatment of chagas disease. Pharmaceutics 14, 1822 (2022).
Branquinho, R. T. et al. Lychnopholide in Poly(d,l-Lactide)-block-polyethylene glycol nanocapsules cures infection with a drug-resistant trypanosoma cruzi strain at acute and chronic phases. Antimicrob. Agents Chemother. 64, e01937–19 (2020).
Spósito, P. Á. et al. Higher oral efficacy of ravuconazole in self-nanoemulsifying systems in shorter treatment in experimental chagas disease. Exp. Parasitol. 228, 108142 (2021).
Ibrahim, E. I. et al. A single oral dose of celecoxib-loaded solid lipid nanoparticles for treatment of different developmental stages of experimental schistosomiasis mansoni. Acta Trop. 229, 106342 (2022).
Eissa, M. M. et al. Evaluation of prophylactic efficacy and safety of praziquantel-miltefosine nanocombination in experimental Schistosomiasis mansoni. Acta Trop. 212, 105714 (2020).
Silva, L. M. et al. Licochalcone A-loaded solid lipid nanoparticles improve antischistosomal activity in vitro and in vivo. Nanomedicine 16, 1641–1655 (2021).
AlGabbani, Q. Nanotechnology: a promising strategy for the control of parasitic infections. Exp. Parasitol. 250, 108548 (2023).
Pedrotti, C. H. S. et al. Telemedicine medical evaluation of low-risk patients with dengue during an outbreak may be an option in reducing the need for on-site physicians. Int. J. Infect. Dis. 121, 106–111 (2022).
Messagier, A. L., Blaizot, R., Couppié, P. & Delaigue, S. Teledermatology use in remote areas of french guiana: experience from a long-running system. Front. Public Health 7, 387 (2019).
Dias, L. C. et al. Teleconsultation on skin diseases: the challenge of providing health care to isolated populations in the amazon rainforest. Divers. Equal. Health Care. 14, 257–263 (2017).
Naufal, F. et al. A hands-free, augmented-reality, smartphone camera system to document the prevalence of active trachoma. Investig. Ophthalmol. Vis. Sci. 62, 2623 (2021).
Bazlan, M. J., Rasam, A. R. & Ghazali, R. Web-based augmented reality mobile GIS for disease prevention and control programme. Test Eng. Manag. 82, 12018–12028 (2020).
Schnabel, K. P. et al. Development and evaluation of three-dimensional transfers to depict skin conditions in simulation-based education. GMS J. Med. Educ. 41, Doc14 (2024).
Salas-Coronas, J. et al. Evaluation of loop-mediated isothermal amplification (LAMP) in urine samples for the diagnosis of imported schistosomiasis. Trop. Med. Infect. Dis. 8, 518 (2023).
Taslimi, Y. et al. Tape-disc-loop-mediated isothermal amplification (TD-LAMP) method as noninvasive approach for diagnosis of cutaneous leishmaniasis caused by L. tropica. Heliyon 9, e21397 (2023).
Longhi, S. A., García Casares, L. J., Muñoz-Calderón, A. A., Alonso-Padilla, J. & Schijman, A. G. Combination of ultra-rapid DNA purification (PURE) and loop-mediated isothermal amplification (LAMP) for rapid detection of Trypanosoma cruzi DNA in dried blood spots. PLoS Negl. Trop. Dis. 17, e0011290 (2023).
Febrer-Sendra, B. et al. Colorimetric and real-time loop-mediated isothermal amplification (LAMP) for detection of loa loa DNA in human blood samples. Diagnostics 12, 1079 (2022).
Maeno, H. et al. A 3D microfluidic ELISA for the detection of severe dengue: sensitivity improvement and vroman effect amelioration by EDC-NHS surface modification. Micromachines) 12, 1503 (2021).
Nielsen, J. B. et al. Monolithic affinity columns in 3D printed microfluidics for chikungunya RNA detection. Anal. Bioanal. Chem. 415, 7057–7065 (2023).
Ali, Z., Bourlioux, M. & Thomsen, S. F. Smartphone app to screen individuals with scabies symptoms. Dan. Med. J. 270, 09220515 (2023).
Debrah, L. B. et al. Morbidity management and surveillance of lymphatic filariasis disease and acute dermatolymphangioadenitis attacks using a mobile phone-based tool by community health volunteers in Ghana. PLoS Negl. Trop. Dis. 14, e0008839 (2020).
Swathi, M. et al. Development and evaluation of a mobile app for guiding rabies prophylaxis among health-care professionals in India. Indian J. Community Med. 45, 473–477 (2020).
Chew, N. et al. Assessing dehydration status in dengue patients using urine colourimetry and mobile phone technology. PLoS Negl. Trop. Dis. 14, e0008562 (2020).
Snyder, B. M. et al. Smartphone photography as a possible method of post-validation trachoma surveillance in resource-limited settings. Int. Health 11, 613–615 (2019).
Bhattarai, A. H., Sanjaya, G. Y., Khadka, A., Kumar, R. & Ahmad, R. A. The addition of mobile SMS effectively improves dengue prevention practices in community: an implementation study in Nepal. BMC Health Serv. Res. 19, 699 (2019).
Koydemir, H. C., Coulibaly, J. T., Tseng, D., Bogoch, I. I. & Ozcan, A. Design and validation of a wide-field mobile phone microscope for the diagnosis of schistosomiasis. Travel Med. Infect. Dis. 30, 128–129 (2019).
Martins, B. R. et al. Development of an electrochemical immunosensor for specific detection of visceral leishmaniasis using gold-modified screen-printed carbon electrodes. Biosensors 10, 81 (2020).
Arshad, R. et al. MIP-based impedimetric sensor for detecting dengue fever biomarker. Appl. Biochem. Biotechnol. 191, 1384–1394 (2020).
Cosic, K., Kopilas, V. & Jovanovic, T. War, emotions, mental health, and artificial intelligence. Front. Psychol. 15, 1394045 (2024).
Ćosić, K., Popović, S., Šarlija, M. & Kesedžić, I. Impact of human disasters and covid-19 pandemic on mental health: potential of digital psychiatry. Psychiatr. Danub. 32, 25–31 (2020).
Lekkas, D. & Jacobson, N. C. Using artificial intelligence and longitudinal location data to differentiate persons who develop posttraumatic stress disorder following childhood trauma. Sci. Rep. 11, 10303 (2021).
Hamilton, A. The future of artificial intelligence in surgery. Cureus 16, e63699 (2024).
Lurin, I. et al. Application of artificial intelligence in civil and military medicine. Georgian Med. News 348, 94–98 (2024).
Garcia-Saiso, S. et al. Artificial Intelligence as a potential catalyst to a more equitable cancer care. JMIR Cancer 10, e57276 (2024).
Dankwa-Mullan, I. & Weeraratne, D. Artificial intelligence and machine learning technologies in cancer care: addressing disparities, bias, and data diversity. Cancer Discov. 12, 1423–1427 (2022).
Gao, Y. & Cui, Y. Deep transfer learning for reducing health care disparities arising from biomedical data inequality. Nat. Commun. 11, 6444 (2020).
Chumachenko, D. et al. Editorial: artificial intelligence solutions for global health and disaster response: challenges and opportunities. Front. Public Health 12, 1439914 (2024).
Owoyemi, A. et al. Artificial intelligence for healthcare in Africa. Front. Digit. Health 2, 6 (2020).
Njei, B. et al. Artificial intelligence for healthcare in Africa: a scientometric analysis. Health Technol. 13, 947–955 (2023).
Bockarie, M. J. et al. Transformative potential of artificial intelligence on health care and research in Africa. Int. J. Infect. Dis. 143, 107011 (2024).
Botwe, B. O. et al. The integration of artificial intelligence in medical imaging practice: perspectives of African radiographers. Radiography 27, 861–866 (2021).
Ugar, E. T. & Malele, N. Designing AI for mental health diagnosis: challenges from sub-Saharan African value-laden judgements on mental health disorders. J. Med. Ethics 50, 592–595 (2024).
Wang, N., Christen, M. & Hunt, M. Ethical considerations associated with “humanitarian drones”: a scoping literature review. Sci. Eng. Ethics 27, 51 (2021).
van Wynsberghe, A. & Comes, T. Drones in humanitarian contexts, robot ethics, and the human–robot interaction. Ethics Inf. Technol. 22, 43–53 (2020).
Edwards, D. et al. Use of delivery drones for humanitarian operations: analysis of adoption barriers among logistics service providers from the technology acceptance model perspective. Ann. Oper. Res. 335, 1645–1667 (2024).
Olatunji, G. et al. Exploring the transformative role of drone technology in advancing healthcare delivery in Africa; a perspective. Ann. Med. Surg. 85, 5279–5284 (2023).
Nyaaba, A. A. & Ayamga, M. Intricacies of medical drones in healthcare delivery: Implications for Africa. Technol. Soc. 66, 101624 (2021).
Haula, K. & Agbozo, E. A systematic review on unmanned aerial vehicles in Sub-Saharan Africa: A socio-technical perspective. Technology in Society 63, 101357 (2020).
Wang, N. As it is Africa, it is ok”? Ethical considerations of development use of drones for delivery in Malawi. IEEE Trans. Technol. Soc. 2, 20–30 (2021).
Jeyabalan, V. et al. Context-specific challenges, opportunities, and ethics of drones for healthcare delivery in the eyes of program managers and field staff: a multi-site qualitative study. Drones 4, 44 (2020).
Lammers, D. T. et al. Airborne! UAV delivery of blood products and medical logistics for combat zones. Transfusion 63, S96–S104 (2023).
Santa et al. Analysis of mobile clinic deployments in conflict zones. J. Humanit. Logist. Supply Chain Manag. 14, 181–207 (2024).
McGowan, C. R. et al. Mobile clinics in humanitarian emergencies: a systematic review. Confl. Health 14, 4 (2020).
González, R. S. et al. Use of mobile medical teams to fill critical gaps in health service delivery in complex humanitarian settings, 2017-2020: a case study of South Sudan. Pan. Afr. Med. J. 42, 8 (2022).
Omam, L. A. et al. Mobile clinics in conflict-affected communities of North West and South West regions of Cameroon: an alternative option for differentiated delivery service for internally displaced persons during COVID-19. Confl. Health 15, 90 (2021).
Doutchi, M. et al. Health transformation toward universal healthcare coverage amidst conflict: examining the impact of international cooperation in Niger. Front. Public Health 12, 1303168 (2024).
Gomez-Marquez, J. & Hamad-Schifferli, K. Local development of nanotechnology-based diagnostics. Nat. Nanotechnol. 16, 484–486 (2021).
Rangayasami, A. et al. Influence of nanotechnology to combat against COVID-19 for global health emergency: a review. Sens. Int. 2, 100079 (2021).
Abbas, J. J. et al. Improving health-care delivery in low-resource settings with nanotechnology: challenges in multiple dimensions. Nanobiomedicine 4, 1849543517701158 (2017).
Muhammad, I. D. A comparative study of research and development related to nanotechnology in Egypt, Nigeria and South Africa. Technol. Soc. 68, 101888 (2022).
Lateef, A. et al. A decade of nanotechnology research in Nigeria (2010–2020): a scientometric analysis. J. Nanoparticle Res. 23, 1–27 (2021).
Masara, B. et al. A nanotechnology-foresight perspective of South Africa. J. Nanoparticle Res. 23, 1–22 (2021).
Chufa, B. M. et al. Graphene oxide nanoadsorbent for the removal of fluoride ion from groundwater: adsorbent performance and adsorption mechanism. J. Nanotechnol. 2022, 7371227 (2022).
Kasera, O. A. et al. Governing emerging technologies: a systematic exploration of Kenya’s biotechnology and LMO-Specific policy documents for adoption and implementation of synthetic biology. Int. J. InnovSci, Res. Technol. 6, 946–974 (2021).
Kahn, M. J. The status of science, technology and innovation in Africa. Sci. Technol. Soc. 27, 327–350 (2022).
Wahba, H. M. et al. The feasibility of the ‘treat and teach’telemedicine package: the Somali pilot. Health Technol. 10, 1515–1523 (2020).
Alser, K. et al. Trauma care supported through a global telemedicine initiative during the 2023-24 military assault on the Gaza Strip, occupied Palestinian territory: a case series. Lancet 404, 874–886 (2024).
Lee, J. et al. Rapid deployment of telehealth in a conflict zone: supporting the humanitarian needs in Ukraine. NEJM Catalyst Innovat. Care Deliv. 4, CAT-22 (2023).
Mahdi, S. S. et al. The promise of telemedicine in Pakistan: a systematic review. Health Sci Rep. 5, e438 (2022).
Moughrabieh, A. & Weinert, C. Rapid deployment of international tele-intensive care unit services in War-Torn Syria. Ann. Am. Thorac. Soc. 13, 165–172 (2016).
Parkes, P. et al. Telemedicine interventions in six conflict-affected countries in the WHO Eastern Mediterranean region: a systematic review. Confl. Health 16, 64 (2022).
Al-Samarraie, H. et al. Telemedicine in Middle Eastern countries: Progress, barriers, and policy recommendations. Int. J. Med. Inform. 141, 104232 (2020).
Bowsher, G. et al. eHealth for service delivery in conflict: a narrative review of the application of eHealth technologies in contemporary conflict settings. Health Policy Plan. 36, 974–981 (2021).
Ugwu, O. P. et al. Harnessing technology for infectious disease response in conflict zones: challenges, innovations, and policy implications. Medicine 103, e38834 (2024).
Dodoo, J. E. et al. The development of telemedicine programs in Sub-Saharan Africa: progress and associated challenges. Health Technol. 12, 33–46 (2022).
Dodoo, J. E. et al. Telemedicine use in Sub-Saharan Africa: barriers and policy recommendations for Covid-19 and beyond. Int. J. Med. Inform. 151, 104467 (2021).
Akintunde, T. Y. et al. Expanding telemedicine to reduce the burden on the healthcare systems and poverty in Africa for a post-coronavirus disease 2019 (COVID-19) pandemic reformation. Glob. Health J. 5, 128–134 (2021).
Rodríguez-Ortega, M. et al. Telemedicine as a counselling tool for nurses in Central Africa. J. Adv. Nurs. Published online. https://doi.org/10.1111/jan.16406 (2024).
Dauda, B. J. et al. Adopting telemedicine in the fight against antimicrobial resistance in West Africa. Int. J. Health Plann. Manage 39, 1626–1632 (2024).
Asadzadeh, A. et al. Applications of virtual and augmented reality in infectious disease epidemics with a focus on the COVID-19 outbreak. Inform. Med. Unlocked 24, 100579 (2021).
Uymaz, P. & Uymaz, A. O. Assessing acceptance of augmented reality in nursing education. PLoS ONE 17, e0263937 (2022).
Domínguez-Velasco, C. F. et al. Augmented reality simulation as training model of ventricular puncture: evidence in the improvement of the quality of punctures. Int. J. Med. Robot. 19, e2529 (2023).
Romalee, W. et al. Effectiveness of mobile augmented reality-integrated oral health education for community-dwelling older adults: A randomized controlled trial. Arch. Gerontol. Geriatr. 117, 105277 (2024).
Mehta, A. et al. Telesurgery’s potential role in improving surgical access in Africa. Ann. Med. Surg. 82, 104511 (2022).
Watson, G. et al. Stone disease in low- and middle-income countries: could augmented reality have a role in its management? BJU Int. 130, 400–407 (2022).
Chadwick, S. et al. Utility of point of care and rapid diagnostics in humanitarian emergencies. J. Appl. Lab. Med. 6, 236–246 (2021).
Wilson, M. L. & Plebani, M. Improving access to diagnostic testing in conflict-affected areas: what is needed? Clin. Chem. Lab. Med. 61, 957–959 (2023).
Bashir, I. M. et al. Strengthening laboratories in response to outbreaks in humanitarian emergencies and conflict settings: results, challenges and lessons from expanding PCR diagnostic capacities for COVID-19 testing in Yemen. PLoS ONE 19, e0298603 (2024).
Hermans, L. E. et al. Point-of-care diagnostics for infection and antimicrobial resistance in sub-Saharan Africa: a narrative review. Int. J. Infect. Dis. 142, 106907 (2024).
Madsen, C. Telehealth in the military health system: impact, obstacles, and opportunities. Mil. Med. 188, 15–23 (2023).
Ahmed, M. M. et al. Advancing digital healthcare in Somalia: a review of modern technologies and their implications. BMC Digit. Health 2, 49.127 (2024).
Eba, K. et al. Mobile health service as an alternative modality for hard-to-reach pastoralist communities of Afar and Somali regions in Ethiopia. Pastoralism 13, 17 (2023).
Logie, C. H. et al. Findings from the Tushirikiane mobile health (mHealth) HIV self-testing pragmatic trial with refugee adolescents and youth living in informal settlements in Kampala, Uganda. J. Int. AIDS Soc. 26, e26185 (2023).
Mustapha, B. M. & Utulu, S. C. Realist evaluation of the early-stage implementation of a smartphone-based disease surveillance project in two armed-conflict communities in Nigeria. Afr. J. Inf. Syst. 13, 1 (2021).
Kazlou, A. et al. Effects of stress on pain in females using a mobile health app in the Russia-Ukraine conflict. Npj Ment. Health Res. 3, 2 (2024).
Sandvik, K. B. in Ethics of Medical Innovation Experimentation and Enhancement in Military and Humanitarian Contexts (eds Messelken, D. & Winkler, D.) 87–104 (Springer, 2020).
Ghomrawi, H. M. et al. Clinicians’ perspectives on wearable sensor technology as an alternative bedside monitoring tool in two West African countries. Int. J. Med. Inform. 175, 105046 (2023).
Walle, A. D. et al. Intention to use wearable health devices and its predictors among diabetes mellitus patients in Amhara region referral hospitals, Ethiopia: using modified UTAUT-2 model. Inform. Med. Unlocked 36, 101157 (2023).
Huhn, S. et al. Using wearable devices to generate real-world, individual-level data in rural, low-resource contexts in Burkina Faso, Africa: a case study. Front. Publ. Health 10, 972177 (2022).
Manyazewal, T., Woldeamanuel, Y., Blumberg, H. M., Fekadu, A. & Marconi, V. C. The potential use of digital health technologies in the African context: a systematic review of evidence from Ethiopia. NPJ Digit. Med. 4, 125 (2021).
Looking towards the future of MRI in Africa. Nat. Commun. 15, 2260 (2024).
Manyazewal, T. et al. Mapping digital health ecosystems in Africa in the context of endemic infectious and non-communicable diseases. NPJ Digit. Med. 6, 97 (2023).
Nsengimana, J. P. & Kaseya, J. The new Africa digital health deal. J. Publ. Health Afr. 14, 2865 (2023).
Manyazewal, T. et al. Patient-reported usability and satisfaction with electronic medication event reminder and monitor device for tuberculosis: a multicentre, randomised controlled trial. EClinicalMedicine 56, 101820 (2023).
Mynhardt, M. et al. Empowering Africa’s healthcare future: the crucial role of human capital development in bio- and pharmaceutical manufacturing. J. Publi. Health Afr. 14, 2866 (2023).
Tanui, C. K., Ndembi, N., Kebede, Y. & Tessema, S. K. Artificial intelligence to transform public health in Africa. Lancet Infect. Dis. S1473-3099, 00435–3 (2024).
Duke, T. et al. Solar-powered oxygen, quality improvement and child pneumonia deaths: a large-scale effectiveness study. Arch. Dis. Child. 106, 224–230 (2021).
Brand, D. et al. Data sharing governance in sub-Saharan Africa during public health emergencies: gaps and guidance. S. Afr. J. Sci. 118, https://doi.org/10.17159/sajs.2022/13892 (2022).
Mabunda, S. Cybersecurity in South Africa: towards best practices. In CyberBRICS: Cybersecurity Regulations in the BRICS Countries (ed Belli, L.) pp. 227–270. (Cham: Springer International Publishing, 2021).
O’Sullivan, K., Clark, S., Marshall, K. & MacLachlan, M. A just digital framework to ensure equitable achievement of the sustainable development goals. Nat Commun 12, 6345 (2021).
Manyazewal, T. et al. Effectiveness of a digital medication event reminder and monitor device for patients with tuberculosis (SELFTB): a multicenter randomized controlled trial. BMC Med. 20, 310 (2022).
Ginsburg, G. S., Picard, R. W., Friend, S. H. Key issues as wearable digital health technologies enter clinical care. N. Engl. J. Med. 390, 1118–1127 (2024).
Acknowledgements
The work was supported by the UK National Institute for Health and Care Research (Global Health Research 131996). The content is solely the responsibility of the authors and does not necessarily represent the official views of the UK National Institute for Health Research. For the purposes of open access, the author has applied a Creative Commons Attribution (CC BY) license to any Accepted Author Manuscript version arising from this submission. The World Bank financially supports the Centre for Innovative Drug Development and Therapeutic Trials for Africa (CDT-Africa).
Author information
Authors and Affiliations
Contributions
Study conception: T.M., A.F. Study design: T.M., A.F., G.D. Analysis: T.M., A.F., G.D., C.H., M.J.N., M.H., J.W., A.S., S.B., L.M., E.A. Funding acquisition: M.J.N., A.F., G.D., T.M. Draft the manuscript: T.M. Reviewed and revised the manuscript: T.M., A.F., G.D., C.H., M.J.N., M.H., J.W., A.S., S.B., L.M., E.A. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Binyam Tilahun, Judd Walson, who co-reviewed with Rohan Michael Ramesh, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Manyazewal, T., Davey, G., Hanlon, C. et al. Innovative technologies to address neglected tropical diseases in African settings with persistent sociopolitical instability. Nat Commun 15, 10274 (2024). https://doi.org/10.1038/s41467-024-54496-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-024-54496-4
This article is cited by
-
Strengthening funding and integration for NTD elimination: insights from the 2025 Annual Meeting of National NTD Programme Managers in the WHO African Region
BMC Proceedings (2026)
-
Development, implementation, and evaluation of an innovative clinical trial operations training program for Africa (ClinOps)
BMC Medical Education (2025)
-
AI-driven analysis by identifying risk factors of VL relapse in HIV co-infected patients
Scientific Reports (2025)
