
Abstract
This open-label phase II trial (NCT04542837) aimed to evaluate the efficacy and safety of KN046 combined with lenvatinib in patients with advanced hepatocellular carcinoma (HCC), and explore the potential response biomarkers. Participants received KN046 5 mg/kg every 3 weeks and lenvatinib 12 or 8 mg once daily. The primary endpoints were safety, tolerability, dose-limiting toxicity (DLT), and objective response rate (ORR) according to RECIST v1.1. A total of fifty-five participants were enrolled. The results meet the pre-specified primary endpoints. No DLT was observed in the safety run-in period. The incidence of serious adverse events and grade ≥3 treatment-related adverse events (TRAEs) was 30.9% and 47.3%, respectively. Grade ≥3 immunotherapy-related adverse events occurred in 3 (5.5%) participants. Five (9.1%) participants discontinued treatment due to TRAEs, all of which were grade 1-2. The ORR was 45.5% (95% CI, 31.97-59.45). The median progression-free survival was 11.0 (95% CI, 8.21-15.24) months. The median overall survival (OS) was 16.4 (95% CI, 11.20-not estimable) months, and 12-month OS rate was 60.0% (95% CI, 45.87-71.55). Circulating tumor DNA status before the third cycle of treatment was associated with prognosis. In conclusion, First-line KN046 plus lenvatinib shows promising efficacy for advanced unresectable or metastatic HCC.
Similar content being viewed by others

Introduction
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer, with established treatment including surgical resection, liver transplantation, and ablation therapy1. Unfortunately, the onset of HCC is insidious, and most patients are in intermediate or advanced stages at diagnosis, usually ineligible for radical surgeries2. Rapid development of interventional therapy and systemic drug therapy has prolonged survival for patients with advanced HCC, but the lack of predictive biomarkers necessitates the need for novel treatment combinations, effective in broader patient populations3,4.
Immune checkpoint inhibitors (ICIs) play major roles in immune escape by inhibiting immune responses and promoting immune tolerance toward tumor cells5. Among these, cytotoxic T lymphocyte antigen 4 (CTLA-4), programmed death 1 (PD-1), and its ligand (PD-L1) have been identified as promising targets6. The combined blockade of ICIs may provide potentially synergistic effects due to the differences in the timing and location of their reactions7. For instance, CTLA-4 binds to CD80/86 and prevents the stimulation of T cell proliferation during the priming phase, typically in lymph nodes7,8. On the other hand, the PD-1 pathway regulates activated T cells in peripheral tissues, which impairs proliferation and activation at the later stages of immune response7,8.
Several phase II/III trials showed promising efficacy of ICIs in unresectable HCC9,10. Consequently, ICIs have been a first-line treatment for advanced HCC in multiple guidelines. Unfortunately, in immunotherapy-naïve patients with advanced HCC, the objective response rate (ORRs) of ICI monotherapy was reported to be lower than 20%11. As a result, combination therapies have been investigated to improve patient survival. Phase III trials demonstrated the efficacy of different combinations of dual therapy: atezolizumab plus bevacizumab (IMbrave150 trial)12, nivolumab plus ipilimumab (Checkmate 9DW trial)13, and tremelimumab plus durvalumab (HIMALAYA trial)14, which showed a median OS ranging from 16.4 to 23.7 months and ORR ranging from 20.1% to 36%12,13,14. Additionally, the LEAP-002 trial has shown that pembrolizumab combined with a vascular endothelial growth factor receptor (VEGFR) inhibitor can achieve ORRs of 26.1%, and a median OS of 21.2 months in patients with HCC15. Despite the proven efficacy of dual immunotherapy, there were safety considerations associated with the administration. The HIMALAYA trial showed that dual immunotherapy (durvalumab + tremelimumab) led to high incidences of grade ≥3 adverse events (AEs), with many patients not tolerating the long-term treatment14,16. Hence, the addition of antiangiogenic agents to dual traditional immunotherapy in order to achieve better treatment efficacy might not be feasible17,18,19. Therefore, minimizing the AEs while ensuring the efficacy of dual immunotherapy combined with a VEGFR inhibitor is pivotal.
The KN046 is a bispecific antibody targeting the PD-1/PD-L1 and CTLA-4/B7 immune checkpoint pathways20. Preclinical study showed that KN046 has a higher affinity for PD-L1 and reduced side effects due to its specific structural modification, making it a potential candidate for further development as an immunotherapy agent20. Recent clinical trials showed that KN046 is well tolerated as a monotherapy in patients with advanced solid tumors21 or in combination with chemotherapy in patients with triple-negative breast cancer22. Levatinib, a VEGFR inhibitor, has been shown to provide potential synergistic effects when used in conjunction with ICIs by inhibiting angiogenesis and immunosuppressive responses of the tumor microenvironment23. Additionally, study has suggested that this combination may potentially mitigate the risk associated with the slow onset of immunotherapy24. The preliminary results of the prospective phase II trial showed encouraging antitumor activity and a favorable AE profile of KN046 combined with lenvatinib in unresectable or metastatic HCC25.
In this work, we evaluate the efficacy and safety of KN046 combined with lenvatinib in patients with advanced HCC. Furthermore, previous research has indicated that combining the analysis of circulating tumor DNA (ctDNA) with tumor tissue analysis may increase the detection rate of specific mutations in HCC patients, potentially leading to more personalized treatment options26. Therefore, this study also sought to explore potential prognosis biomarkers using the next-generation sequencing (NGS). The combination of first-line KN046 and lenvatinib shows promising efficacy for advanced unresectable or metastatic hepatocellular carcinoma. Additionally, ctDNA status before the third cycle of treatment is associated with prognosis.
Results
Characteristics of the participants
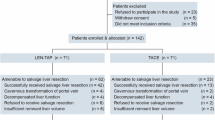
Seventy-three patients were screened, of which 16 did not meet the eligibility criteria, and two withdrew their consent before enrollment. Finally, 55 participants were enrolled, and as of the data cut-off date (November 30, 2022), two participants were still receiving treatment (Fig. 1).

A total of 55 participants were enrolled, and as of the data cut-off date (November 30, 2022), two participants were still receiving treatment. QD once every day, AE adverse event, PD progressive disease, SS safety set, EAS efficacy analysis set.
The mean age of participants was 60.3 ± 6.93 years, 80.0% of participants were male, 39 (70.9%) had hepatitis B, one (1.8%) had hepatitis C, and 35 (63.6%) had liver cirrhosis. Fifty-one (92.7%) were in Barcelona Clinic Liver Cancer (BCLC) stage C, and 53 (96.4%) had Child-Pugh A liver function. Twenty-eight (50.9%) participants had extrahepatic metastases (Table 1).
Safety
No dose-limiting toxicity (DLT) was observed in the safety run-in period. As of the data cut-off date, the median exposure duration was 7.1 (range, 0.7–23.4) months for KN046 and 7.7 (range, 0.3–25.0) months for lenvatinib. The summary of safety analysis is presented in Table 2 and the most common (≥10%) treatment-emergent AEs (TEAEs) are listed in Supplementary Table 1. Serious AEs (SAEs) occurred in 17 (30.9%) participants, of which 8 (14.5%) were considered to be treatment-related. Treatment-related AEs (TRAEs) occurred in 100% of participants, of which grade ≥3 occurred in 26 (47.3%). Thirteen (23.6%) participants experienced immunotherapy-related AEs (irAEs). TRAEs leading to treatment discontinuation were observed in 5 (9.1%) participants and one (5.3%) participant had TRAEs leading to death (interstitial lung disease). The most common TRAEs (>30%) were decreased platelet count (26 [47.3%]), fatigue (22 [40.0%]), hypertension (22 [40.0%]), proteinuria (21 [38.2%]), elevated blood bilirubin (19 [34.5%]), and elevated aspartate transaminase (18 [32.7%]). The most common grade ≥3 TRAEs (>2%) were hypertension (7 [12.7%]), elevated blood pressure (5 [9.1%]), decreased platelet count (3 [5.5%]), fatigue (2 [3.6%]), elevated aspartate aminotransferase (2 [3.6%]), weight loss (2 [3.6%]), and hyponatremia (2 [3.6%]) (Table 2). In addition, the most common grade ≥3 TEAEs (>5%) were hypertension (7 [12.7%]), elevated blood pressure (5 [9.1%]), decreased platelet count (3 [5.5%]), and hyponatremia (3 [5.5%]) (Supplementary Table 2).
Efficacy
As of November 30, 2022, the median follow-up duration was 13.8 (range, 0.03–20.93) months. The tumor response is presented in Fig. 2. Based on Response Evaluation Criteria in Solid Tumors (RECIST) v1.1, the ORR was 45.5% (95% confidence interval [CI], 31.97–59.45). The disease control rate (DCR) was 89.1% (95% CI, 77.75–95.89), the median time to response (TTR) was 2.6 (95% CI, 1.31–2.69) months, and the median duration of response (DOR) was not reached (NR) (95% CI, 9.33-NR). A total of 29 (52.7%) progression-free survival (PFS) events occurred, and the median PFS was 11.0 (95% CI, 8.21–15.24) months (Fig. 3A).

A The spider plot showing patient responses by week based on RECIST v1.1. B The spider plot showing patient responses by week based on mRECIST. C The waterfall plot showing the percentage change in target lesions from baseline based on RECIST v1.1. D The waterfall plot showing the percentage change in target lesions from baseline based on mRECIST. E The swimming plot showing tumor responses during treatment based on RECIST v1.1. F The swimming plot showing tumor responses during treatment based on mRECIST. QD once every day, CR complete response, PR partial response, SD stable disease, PD progressive disease, NE not evaluable.

The Kaplan–Meier survival curve showing the cumulative progression-free survival (PFS) and overall survival (OS) probabilities according to different evaluation criteria. A PFS in the safety set (SS) based on RECIST v1.1. B PFS in the SS based on mRECIST. C OS in the SS. The Kaplan–Meier survival curve was utilized to analyze PFS. The Brookmeyer–Crowley method was used to calculate the median time with a 95% confidence interval. Source data are provided as a Source Data file.
Based on modified RECIST (mRECIST), the ORR was 56.4% (95% CI, 42.32–69.70), the DCR was 89.1% (95% CI, 77.75–95.89), the median TTR was 1.3 (95% CI, 1.31–1.58) months, and the median DOR was 11.2 (95% CI, 6.77-NR) months. A total of 32 (58.2%) PFS events occurred, and the median PFS was 8.2 (95% CI, 5.72–12.02) months (Fig. 3B).
Based on immune-modified RECIST (imRECIST), the ORR was 45.5% (95% CI, 31.97–59.45), the DCR was 90.9% (95% CI, 80.05–96.98), the median TTR was 2.6 (95% CI, 1.31–2.69) months, and the median DOR was NR (95% CI, 9.33-NR) months (Table 3). A total of 28 (50.9%) PFS events occurred, and the median PFS based on imRECIST was 11.0 (95% CI, 8.21–15.24) months. The median OS was 16.4 (95% CI, 11.20-not estimable) months, and the 12-month OS rate was 60.0% (95% CI, 45.87–71.55) (Fig. 3C).
Biomarker analysis for efficacy of KN046 and lenvatinib
The NGS was performed on baseline tumor tissue samples from 44 participants available for further exploration of potential biomarkers to predict response (Fig. 4A). TP53 (59.1%), TERT (47.7%), and LRP1B (27.3%) were the most frequently mutated genes in these patients at baseline. Cytokines pathway, cell cycle pathway, Wnt pathway, and SWI/SNF pathway were the most common mutated pathways. CCND1 and FGF19 copy-number variations (CNVs) were significantly more frequent in non-responders (patients with stable disease [SD] + disease progression [PD]) than in responders (patients with CR + PR), and no other significant differences in gene mutations were found between these two subgroups (Fig. 4B). Patients harboring CCND1 and FGF19 CNVs also showed unfavorable PFS and OS (Supplementary Fig. 1B, C). Additionally, there was no difference in tumor mutation burden (TMB) between responders and non-responders (P = 0.921, Supplementary Fig. 1A).

A Genetic profiling of the baseline tumor tissue from 44 patients. The clincopathological features including treatment, age, sex, alpha-fetoprotein (AFP) level, and best-of-response (BOR) status were indicated by the bar on the top. The types of alterations were indicated by different colors. Each column represented one patient. B The comparison of gene alterations between the patients with complete response (CR) + partial response (PR) and stable disease (SD) + progressive disease (PD). C The comparison of circulating tumor DNA (ctDNA)-positive rate between the patients with CR + PR and SD + PD at different time points. D–F Kaplan–Meier analysis of progression-free survival stratified by ctDNA status at P1 (D), serial plasma (E), and P0 + P1 (F). The Kaplan–Meier survival curve was utilized to analyze progression-free survival (PFS). Hazard ratio (HR) with 95% CIs were estimated by the Cox proportional hazards regression analysis, and a two-sided P < 0.05 was considered to be statistically significant. Adjustments were not made for multiple comparisons. Source data are provided as a Source Data file.
A comparison of genetic variations between tumor tissue and baseline plasma (P0) was depicted in Supplementary Fig. 3A. A high detection consistency was observed between the two sample types, with TP53 being the most frequently mutated gene. Unlike the findings in baseline tumor tissues, TP53, TERT and CTNNB1 mutations were significantly more frequent in non-responders (patients with SD + PD) than in responders (patients with complete response [CR] + partial response [PR]) concerning baseline plasma (P0) (Supplementary Fig. 2A). Patients harboring CCND1 CNV or TP53 mutation showed unfavorable PFS and OS (Supplementary Fig. 2B, C, F, G); while those harboring FGF19 CNV or TERT mutation showed unfavorable OS (Supplementary Fig. 2E, I), but not PFS (Supplementary Fig. 2D, H).
Furthermore, we compared ctDNA dynamic changes at different time points: pre-treatment (P0, n = 49), at the first time point (P1, n = 48) and the second time point (P2, n = 30) of tumor assessment, between responders and non-responders. The percentage of ctDNA-positive patients dramatically decreased during treatment (Supplementary Fig. 3B). Among P0, P1, P2, and serial plasma, the positive rate of ctDNA showed significant differences at P1 (P < 0.001), P2 (P = 0.002) and serial plasma (P < 0.001) in the two subgroups (Fig. 4C). Additionally, 14 patients with ctDNA-negative status at P1, and 13 patients with ctDNA-negative status in serial plasma exhibited improved PFS (Fig. 4D, E) and OS (Supplementary Fig. 3D, E) compared to ctDNA-positive. The analysis of hazard ratio (HR) values also supported the prognostic significance of P1 and serial plasma status (Supplementary Fig. 3C). Concerning P0 and P1 ctDNA status, patients with persistently negative ctDNA had the best PFS (Fig. 4F) and OS (Supplementary Fig. 3F), followed by those who converted from positive to negative, and finally, those with persistently positive ctDNA. Further randomized studies are needed to determine whether this dynamic biomarker serves as a prognostic or predictive factor.
Discussion
To our knowledge, this is the first exploratory study assessing a bispecific antibody, as well as a combination of a bispecific antibody plus a small-molecule tyrosine kinase inhibitor (TKI) in HCC treatment. This open-label phase II clinical trial showed that KN046, a bispecific antibody against PD-L1 and CTLA-4, combined with lenvatinib achieved an ORR of over 40% and median PFS of 11.0 months, indicating promising efficacy as first-line treatment for advanced unresectable or metastatic HCC. However, safety concerns have been raised due to the incidence of grade ≥3 TRAEs being 47.3%, underscoring the necessity for appropriate management of AEs.
Most patients with HCC are in the intermediate or advanced stages at diagnosis, and BCLC stage B-C accounts for 60%2. In recent years, with the advances of immunotherapy, many patients can achieve tumor regression and reduced adverse oncological factors, thereby prolonging survival to the greatest extent and even gaining opportunities for surgery9,10,14. The main issue with single-agent immunotherapy is incomplete immunosuppression mediated by a single blocking site, which is prone to drug resistance27. Hence, new treatment regimens combining targeted therapy with immunotherapy receive more attention. Previous studies found that the efficacy of targeted therapy plus immunotherapy and interventional therapy was significantly improved in HCC patients with large intrahepatic tumor burden, achieving an ORR of about 50% but with serious side effects28,29,30. Therefore, patients with adequate liver function and tumors confined to the liver who are more tolerant to the combination therapy are the potential beneficiaries, and their long-term survival remains to be explored.
Another way to circumvent immunotherapy resistance is to target the two main immune tolerance pathways, but the reported ORR of such regimens is still comparatively low and toxicity is high14. In particular, nivolumab plus ipilimumab in advanced melanoma, recurrent small cell lung cancer, and metastatic renal cell carcinoma showed an improved response and OS with higher ipilimumab doses31,32. In HCC, tremelimumab plus durvalumab achieved a median PFS of 3.78 months, a median OS of 14.63 months, and an ORR of 20.1%. In the CheckMate 040 trial, the investigator-assessed ORR was over 30% across treatment arms with nivolumab plus ipilimumab33. At the same time, high incidence rates of AEs with dual immunotherapy limit its use and prevent the addition of a TKI. The present study innovatively used a bispecific antibody plus lenvatinib; the ORR reached about 50%, and the median PFS reached 11 months, supporting the use of bispecific immunotherapy as a potential treatment option for HCC.
Previous research indicated that combining anti-VEGF therapy with ICIs could provide a synergistic effect, due to the immunomodulatory role of VEGF-A, which stimulates the activity of immune suppressor cells, including tumor-associated macrophages, Treg cells, and myeloid-derived suppressor cells34. As a result, combining antiangiogenic therapy with ICIs may potentiate the counteraction against tumor immunity suppression. The results of the present study, consistent with previous findings, suggest that the synergistic combination may lead to higher, more durable response and improve survival in patients with advanced HCC. Moreover, the duration of treatment in this study was longer than in previous studies33, and the proportion of patients who achieved durable clinical response was also higher than when using two separate antibodies against de PD-1/L1 and CTLA-4/B7 axes33. The ORR in the present study (46%) was higher than 13%–30% in previous clinical trials12,15,35,36. These results highlight the good prospects of bispecific antibodies for immunotherapy in HCC.
In addition, our biomarker analysis of the efficacy of KN046 combined with lenvatinib suggested that ctDNA status was closely linked to therapeutic efficacy, and patients achieving ctDNA clearance in the early treatment period are more likely to have a better survival benefit. This finding is in line with previous studies, where concentration and presence of ctDNA were associated with the prognosis in advanced liver cancer37,38, and high levels of ctDNA were generally associated with a worse prognosis37. Moreover, previous studies in patients with other advanced solid tumors had also suggested that patients with ctDNA clearance after treatment had longer OS39,40,41. Therefore, the presence of ctDNA may be potentially used as a prognostic indicator for patients with advanced HCC who undergo immunotherapy. Additionally, the HR analysis has demonstrated significant differences in both PFS and OS based on ctDNA status at P1 (the first tumor assessment). However, the HR value decreased at P2 (the second tumor assessment), indicating a reduction in predictive value for subsequent assessments. In addition, an increasing number of patients had evidence of disease progression at later time points, rendering further ctDNA testing. This highlights the value of early dynamic monitoring.
The incidences of grade ≥3 TEAEs and grade ≥3 TRAEs with KN046 plus lenvatinib were 58.2% and 47.3%, respectively. In previous trials of single-agent immunotherapy plus antiangiogenic therapy, the incidence of grade ≥3 TRAEs ranged from 55% to 80.9%, which may potentially lead to early discontinuation of treatment15,35,36,42. The incidence of grade ≥3 TRAEs in this study was numerically lower than those previously reported. Despite differences in safety profiles between different treatment combinations, this discrepancy could also stem from variations in the patient populations included in the studies. For example, our study included 50.9% of participants with extrahepatic disease, while the LEAP-002 and REFLECT trials had higher proportions of 63% and 60.9%, respectively15,42, which may potentially influence the safety results.
In addition to the above, KN046 is a fully human wild-type IgG1 Fc, which was designed in tandem with domain antibodies (dAbs) to form a bispecific antibody that simultaneously recognizes PD-L1 and CTLA-4 and activates the immune response25,43. Along with releasing PD-L1-mediated immunosuppression, enhancing CTL immune function, and releasing CTLA4-mediated Treg immunosuppression, bispecific antibodies may cause fewer side effects than two separate PD-1/L1 and CTLA-4 antibodies. Furthermore, a bispecific antibody requires only one infusion, compared with dual immunotherapy, which requires two separate infusions, resulting in longer treatment times and sometimes more premedication44. However, it is worth noting that the inclusion of an antiangiogenic agent may result in a higher incidence of adverse events, which necessitates close monitoring for potential side effects in clinical settings45.
This trial had several limitations. First, it was a phase II trial with a limited sample size. In addition, there was no control group, preventing the direct evaluation of efficacy compared with standard treatment. Second, the enrolled population consisted of only participants from China, with a relatively high prevalence of viral hepatitis. The impact of HBV on the response to immunotherapy remains a critical factor; hence, the findings may not be generalizable to other populations with different epidemiological characteristics. Moreover, the follow-up was relatively short. Large-scale, randomized controlled trials with a longer follow-up are needed to confirm the results. Finally, the incorporation of RNA sequencing data could further increase the utility of the biomarker analysis46. However, this was not conducted due to the unavailability of additional biological samples. Future studies should consider incorporating RNA sequencing to provide a more comprehensive evaluation.
In conclusion, KN046 combined with lenvatinib shows promising efficacy as a first-line treatment for advanced unresectable or metastatic HCC. These results support the KN046 plus lenvatinib combination as a potential treatment option for this population. The results also support conducting a phase III trial.
Methods
Study design and participants
This study was approved by the Institutional Ethical Review Board Committee of Beijing Cancer Hospital and Institute (Beijing, China; approval number 2020YJZ37 and clinical trial number NCT04542837; date of registration: September 2, 2020). Informed consent was obtained from all patients before being included in the study. This trial was conducted in accordance with the Declaration of Helsinki and Good Clinical Practices.
This multi-center open-label phase II clinical trial enrolled patients with advanced HCC from September 29, 2020, to September 30, 2021, at Beijing Cancer Hospital and Harbin Medical University Cancer Hospital in China. The key inclusion criteria were (1) age of 18–75 years, (2) diagnosis of unresectable advanced HCC confirmed by histology or cytology, with BCLC stage B or C, (3) Eastern Cooperative Oncology Group performance status (ECOG PS): 0–1, (4) Child-Pugh score ≤7, (5) adequate functions of the major organs, (6) ≥1 measurable lesion(s) based on RECIST v1.1 at baseline. Both male and female patients were included in the study, and sex was self-reported. The key exclusion criteria were (1) fibrolamellar HCC, sarcomatoid HCC, cholangiocarcinoma, mixed type HCC, (2) tumor thrombus invading the main portal vein (Vp4), inferior vena cava, or heart involvement, (3) previously received systemic therapy, immune checkpoint inhibitors (such as anti-PD-1/L1 or CTLA-4 antibodies), (4) local treatment received within 4 weeks before enrollment, and (5) history of autoimmune diseases, hepatic encephalopathy or liver transplantation. Complete inclusion and exclusion criteria are provided in the Supplementary Methods.
Intervention
The first six participants entered the 28-day safety run-in period (i.e., the first treatment cycle) for observation of DLT. Hematological or non-hematological toxicity that occurred in ≥2/6 participants was considered a DLT unless the investigators judged that it was definitely related to disease progression or caused by other external causes. DLT also included any-grade toxicity leading to the withdrawal of the study judged by the investigators. Intravenous KN046 5 mg/kg d1 and oral lenvatinib 12 mg once daily (QD) (body weight ≥60 kg) or 8 mg QD (body weight <60 kg) were administered. If ≥2 DLTs occurred, the dose of lenvatinib was reduced to 8 mg QD (body weight ≥60 kg) or 4 mg QD (body weight <60 kg). Each subsequent cycle was 21 days. KN046 was administered until disease progression, intolerable toxicity, or the completion of the planned 27-month treatment. Lenvatinib was administered until disease progression or intolerable toxicity.
Dose adjustment for KN046 was not allowed. When participants had grade ≥3 KN046-related AEs specified in the protocol, KN046 was suspended until the AEs recovered to grade ≤1 or the baseline. If the same type of KN046-related toxicity recurred and required dose suspension, KN046 was permanently discontinued. Guidelines for treatment interruption and discontinuation are detailed in the Supplementary Methods.
Endpoints
The primary endpoints were safety, tolerability, DLT, and ORR as judged by the investigators according to RECIST v1.1. The secondary endpoints were ORR assessed by the investigators based on mRECIST and imRECIST, DOR, DCR, TTR, PFS, OS, and 12-month OS rate, assessed by the investigators based on RECIST v1.1, mRECIST, and imRECIST, with specific definitions provided in the Supplementary Methods.
Hematological or non-hematological toxicity was considered a DLT unless the investigators judged that it was definitely related to disease progression or caused by other external causes. DLT also included any-grade toxicity leading to the withdrawal of the study judged by the investigators.
Clinical assessment
Tumor assessment at baseline and follow-up based on computed tomography (CT) or magnetic resonance imaging (MRI) was conducted once every 6 (±1) weeks in the first year and then once every 12 (±1) weeks thereafter. Tumor response was assessed by the investigators based on the RECIST v1.1, mRECIST, and imRECIST criteria.
For participants in the safety run-in period, safety was assessed once every week. DLT was recorded and graded based on Common Terminology Criteria for Adverse Events (CTCAE 5.0). During the subsequent treatment period, a follow-up visit was conducted before each administration of KN046. The safety assessment included vital signs, height, weight, physical examination, ECOG PS score, laboratory tests (blood routine, blood biochemistry, coagulation function, urine routine, stool routine, thyroid function, and blood/urine pregnancy test), and 12-lead electrocardiogram. AEs were followed until 30 days after the last administration of the study drug or initiation of a new antitumor therapy. SAEs and TRAEs were followed up to 90 days after the last administration. SAEs suspected to be related to KN046 were recorded regardless of the time of occurrence and time interval from discontinuing KN046 treatment.
Next-generation sequencing and data analysis
Baseline tissue samples were available in 44 patients. Plasma cell-free DNA (cfDNA) samples were collected before treatment (P0, n = 49), before the third cycle of treatment (P1, n = 48), before the fifth cycle of treatment (P2, n = 30), and at the time of PD (P3, n = 7). Serial plasma was defined as plasma from patients with any of the points P1/P2, which was available in 49 patients. Serial plasma positive was defined as at least one positive result in either P1 or P2. Due to the limited sample size of P3, it was excluded from the data analysis in this study.
The DNA was extracted from the formalin-fixed, paraffin-embedded (FFPE) samples using the QIAamp DNA FFPE Kit (QIAGEN, Valencia, CA), and ctDNA-MRD DNA (ctDNA) was extracted from plasma samples using the QIAamp Circulating Nucleic Acid Kit (QIAGEN, Valencia, CA), following the manufacturer’s instructions. The VarScan2 was used for the detection of candidate somatic mutations47. Single-nucleotide variants (SNVs) or indels were annotated with DELLY and manually checked with the Integrative Genomics Viewer (IGV)48. Detailed filter criteria for tumor samples were as follows: (1) for hotspot SNV or indel: variant allele frequency (VAF) ≥0.5%, supporting reads ≥3, depth ≥30×, (2) for non-hotspot SNV or indel: VAF ≥ 1%, supporting reads ≥6, depth ≥30×, (3) for structural variant (SV), reads ≥3. CNVs were detected using a freely available software package CNVkit with default parameters49. Somatic CNVs were identified using paired normal/tumor samples for each exon with a cut-off of 0.6 for copy-number loss and 2.0 for copy-number gain. TMB was defined as the total number of missense mutations, as previously reported50.
To sensitively and specifically detect low-abundance mutations in cfDNA, a customized library preparation with a bi-barcoding system called Automated Triple Groom Sequencing (ATG-Seq) was applied to cfDNA samples51. To assemble a position- and base substitution-specific background error database based on allele frequency and distinct supporting reads throughout the panel, we constructed a bioinformatics polishing pipeline by sequencing a pool of plasma samples collected from over 500 healthy donors. An alternation was considered as sequencing noise if its allele frequency and distinct supporting reads were not significantly higher than the corresponding background errors in the database. To minimize the errors from polymerase chain reaction (PCR), hybridization, damaging, sequencing, and contamination, and avoid mutations from nontumor sources in cfDNA, we conducted the following procedures: (a) cfDNA fragment was sequenced at a depth of ~5000, which produced redundant DNA molecules; (b) mapping positions and a bi-barcode system were used to maximize the representative power of unique DNA molecules; (c) a duplex assisted decoder system was used to filter mapping and sequencing artifacts. Genomic DNA from the white blood cells of the buffy coat after plasma separation was also analyzed as the normal control sample for germline and clonal hematopoiesis mutation filtering. Detection threshold requirements of plasma ctDNA for the mutations detected in tissues: (1) for hotspot SNV or indel: alter reads ≥3, depth ≥100×; (2) for non-hotspot SNV or indel: alter reads ≥6, depth ≥100×. Detection threshold requirements of plasma ctDNA for the mutations undetected in tissues: for all SNV or indel, VAF ≥ 1%, alter reads ≥6, depth ≥100×. Plasma ctDNA was considered positive if any true mutation had been detected in the sample.
Statistical analysis
With the ORR in this study estimated to be 40% and considering a one-sided α of 0.025 and β of 0.15, 53 participants were required (six of them in the safety run-in period).
The safety set (SS) included all participants who received the study drugs at least once and had at least one safety assessment. The efficacy analysis set (EAS) included all participants who received the study drugs at least once and had at least one follow-up tumor assessment. The ORR, DCR, and TTR were reported, and the corresponding 95% CIs were calculated using the Clopper–Pearson method in the total population. The medians and 95% CIs of DOR, PFS, and OS were estimated using the Kaplan–Meier method. The Kaplan–Meier survival curve was utilized to analyze PFS and OS among different patient groups, with statistical differences assessed using the log-rank test. The censoring rules are listed in Supplementary Tables 3 and 4. Reverse Kaplan–Meier method was used for calculating the median follow-up time. For categorical variables, Fisher’s exact test was used. For continuous variables, the Wilcoxon rank-sum test was used. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) or R software version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria), HR with 95% CIs were estimated by the Cox proportional hazards regression analysis, and a two-sided P < 0.05 was considered to be statistically significant.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The raw sequence data used in this study are available in the Genome Sequence Archive (Genomics, Proteomics & Bioinformatics 2021) in the National Genomics Data Center (Nucleic Acids Res 2022), China National Center for Bioinformation/Beijing Institute of Genomics, Chinese Academy of Sciences database under accession code HRA009542 (https://ngdc.cncb.ac.cn/gsa-human/s/Sg33BdDh). To respect participant confidentiality, the study clinical data are not publicly available. Individual de-identified clinical data can be made available for academic purposes upon request and approval by the study management committee and subject to appropriate data transfer agreements. Request should be directed to the corresponding authors Kun Wang (wang-kun@vip.sina.com) and Baocai Xing (xingbaocai88@sina.com). Requests for data access will be processed within 4 weeks, and access will be granted for a month. The remaining data are available within the Article, Supplementary Information, or Source Data file. Source data are provided with this paper.
Code availability
The VarScan2 code is available at https://github.com/Jeltje/varscan2, the DELLY code can be accessed at https://github.com/dellytools/delly, and CNVkit is available at https://github.com/etal/cnvkit. The “ComplexHeatmap” package was used in R (Version 4.1.0) for heatmap visualization. The ‘survival’ package was used to plot KM curves. The ‘forest plot’ package was used to generate a forest plot. The ‘ggplot2’ package was used to create a box plot. The code is accessible at https://github.com/jiaohuipang/R_code.
References
Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 380, 1450–1462 (2019).
Allemani, C. et al. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 385, 977–1010 (2015).
Brown, Z. J. et al. Management of hepatocellular carcinoma: a review. JAMA Surg. 158, 410–420 (2023).
Rimassa, L., Finn, R. S. & Sangro, B. Combination immunotherapy for hepatocellular carcinoma. J. Hepatol. 79, 506–515 (2023).
Han, Y., Liu, D. & Li, L. PD-1/PD-L1 pathway: current researches in cancer. Am. J. Cancer Res. 10, 727–742 (2020).
Darvin, P., Toor, S. M., Sasidharan Nair, V. & Elkord, E. Immune checkpoint inhibitors: recent progress and potential biomarkers. Exp. Mol. Med. 50, 1–11 (2018).
Buchbinder, E. I. & Desai, A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Am. J. Clin. Oncol. 39, 98–106 (2016).
Zhang, H. et al. Regulatory mechanisms of immune checkpoints PD-L1 and CTLA-4 in cancer. J. Exp. Clin. Cancer Res. 40, 184 (2021).
Qin, S. et al. LBA36 Final analysis of RATIONALE-301: Randomized, phase III study of tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Ann. Oncol. 33, S1402–S1403 (2022).
Ren, Z. et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2-3 study. Lancet Oncol. 22, 977–990 (2021).
Chen, Y., Hu, H., Yuan, X., Fan, X. & Zhang, C. Advances in immune checkpoint inhibitors for advanced hepatocellular carcinoma. Front. Immunol. 13, 896752 (2022).
Cheng, A.-L. et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 76, 862–873 (2022).
Galle, P. R. et al. Nivolumab (NIVO) plus ipilimumab (IPI) vs lenvatinib (LEN) or sorafenib (SOR) as first-line treatment for unresectable hepatocellular carcinoma (uHCC): first results from CheckMate 9DW. J. Clin. Oncol. 42, LBA4008 (2024).
Abou-Alfa, G. K. et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 1, EVIDoa2100070 (2022).
Llovet, J. M. et al. Lenvatinib plus pembrolizumab versus lenvatinib plus placebo for advanced hepatocellular carcinoma (LEAP-002): a randomised, double-blind, phase 3 trial. Lancet Oncol. 24, 1399–1410 (2023).
Sangro, B. et al. Four-year overall survival update from the phase III HIMALAYA study of tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 35, 448–457 (2024).
Song, Y. et al. Anti-angiogenic agents in combination with immune checkpoint inhibitors: a promising strategy for cancer treatment. Front. Immunol. 11, 1956 (2020).
Raybould, A. L. & Sanoff, H. Combination antiangiogenic and immunotherapy for advanced hepatocellular carcinoma: evidence to date. J. Hepatocell. Carcinoma 7, 133–142 (2020).
Far, B. F. et al. Unresectable hepatocellular carcinoma: a review of new advances with focus on targeted therapy and immunotherapy. Livers 3, 121–160 (2023).
Jiang, C. et al. Engineering a smart agent for enhanced immunotherapy effect by simultaneously blocking PD-L1 and CTLA-4. Adv. Sci. 8, e2102500 (2021).
Ma, Y. et al. Phase I trial of KN046, a novel bispecific antibody targeting PD-L1 and CTLA-4 in patients with advanced solid tumors. J. Immunother. Cancer 11, e006654 (2023).
Li, Q. et al. The anti-PD-L1/CTLA-4 bispecific antibody KN046 in combination with nab-paclitaxel in first-line treatment of metastatic triple-negative breast cancer: a multicenter phase II trial. Nat. Commun. 15, 1015 (2024).
Lee, M. M. P., Chan, L. L. & Chan, S. L. The role of lenvatinib in the era of immunotherapy of hepatocellular carcinoma. J. Liver Cancer 23, 262–271 (2023).
Gao, X. et al. Cadonilimab with chemotherapy in HER2-negative gastric or gastroesophageal junction adenocarcinoma: the phase 1b/2 COMPASSION-04 trial. Nat. Med. 30, 1943–1951 (2024).
Xing, B. 938P KN046 (an anti-PD-L1/CTLA-4 bispecific antibody) in combination with lenvatinib in the treatment for advanced unresectable or metastatic hepatocellular carcinoma (HCC): preliminary efficacy and safety results of a prospective phase II trial. Ann. Oncol. 32, S822 (2021).
Kopystecka, A., Patryn, R., Leśniewska, M., Budzyńska, J. & Kozioł, I. The use of ctDNA in the diagnosis and monitoring of hepatocellular carcinoma-literature review. Int. J. Mol. Sci. 24, 9342 (2023).
Bai, R. et al. Mechanisms of cancer resistance to immunotherapy. Front. Oncol. 10, 1290 (2020).
Tibballs, J. & Clements, W. Immunotherapy and Transarterial therapy of HCC: what the interventional radiologist needs to know about the changing landscape of HCC treatment? J. Med. Imaging Radiat. Oncol. 66, 478–482 (2022).
Fang, T. et al. Combined with interventional therapy, immunotherapy can create a new outlook for tumor treatment. Quant. Imaging Med. Surg. 11, 2837–2860 (2021).
Kim, D. H. Combination of interventional oncology local therapies and immunotherapy for the treatment of hepatocellular carcinoma. J. Liver Cancer 22, 93–102 (2022).
Paz-Ares, L. et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 22, 198–211 (2021).
Larkin, J. et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 381, 1535–1546 (2019).
Yau, T. et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the CheckMate 040 randomized clinical trial. JAMA Oncol. 6, e204564 (2020).
Kudo, M. Combination cancer immunotherapy with molecular targeted agents/anti-CTLA-4 antibody for hepatocellular carcinoma. Liver Cancer 8, 1–11 (2019).
Kelley, R. K. et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. The Lancet. Oncology 23, 995–1008 (2022).
Qin, S. et al. LBA35 Camrelizumab (C) plus rivoceranib (R) vs. sorafenib (S) as first-line therapy for unresectable hepatocellular carcinoma (uHCC): a randomized, phase III trial. Ann. Oncol. 33, S1401–S1402 (2022).
Piciocchi, M. et al. Circulating free DNA in the progression of liver damage to hepatocellular carcinoma. Hepatol. Int. 7, 1050–1057 (2013).
Xu, R. H. et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 16, 1155–1161 (2017).
Zhang, Q. et al. Prognostic and predictive impact of circulating tumor DNA in patients with advanced cancers treated with immune checkpoint blockade. Cancer Discov. 10, 1842–1853 (2020).
Goodall, J. et al. Circulating cell-free DNA to guide prostate cancer treatment with PARP inhibition. Cancer Discov. 7, 1006–1017 (2017).
Yang, Y. et al. The clinical utility of dynamic ctDNA monitoring in inoperable localized NSCLC patients. Mol. Cancer 21, 117 (2022).
Kudo, M. et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 391, 1163–1173 (2018).
Xing, B. et al. A phase II study combining KN046 (an anti-PD-L1/CTLA-4 bispecific antibody) and lenvatinib in the treatment for advanced unresectable or metastatic hepatocellular carcinoma (HCC): Updated efficacy and safety results. J. Clin. Oncol. 40, 4115 (2022).
Thakur, A., Huang, M. & Lum, L. G. Bispecific antibody based therapeutics: strengths and challenges. Blood Rev. 32, 339–347 (2018).
Yang, W. et al. Efficacy and safety of immune checkpoint inhibitors combined with anti-VEGF therapy in the treatment of unresectable or advanced liver cancer: a systematic review. Immunopharmacol. Immunotoxicol. 45, 770–779 (2023).
Kurebayashi, Y. et al. Immunovascular classification of HCC reflects reciprocal interaction between immune and angiogenic tumor microenvironments. Hepatology 75, 1139–1153 (2022).
Koboldt, D. C. et al. VarScan 2: somatic mutation and copy number alteration discovery in cancer by exome sequencing. Genome Res. 22, 568–576 (2012).
Rausch, T. et al. DELLY: structural variant discovery by integrated paired-end and split-read analysis. Bioinformatics 28, i333–i339 (2012).
Talevich, E., Shain, A. H., Botton, T. & Bastian, B. C. CNVkit: genome-wide copy number detection and visualization from targeted DNA sequencing. PLoS Comput. Biol. 12, e1004873 (2016).
Fang, W. et al. Comprehensive genomic profiling identifies novel genetic predictors of response to anti-PD-(L)1 therapies in non-small cell lung cancer. Clin. Cancer Res. 25, 5015–5026 (2019).
Qiu, B. et al. Dynamic recurrence risk and adjuvant chemotherapy benefit prediction by ctDNA in resected NSCLC. Nat. Commun. 12, 6770 (2021).
Acknowledgements
We acknowledge Zhiqin Zhao and Baohong Guo for their support with manuscript revision. We thank Nanjing Geneseeq Technology Inc. (Nanjing, China), for their support in next-generation sequencing. Hybridization-based target enrichment was carried out with GENESEEQ PRIME” pan-cancer panel. We also thank the patients, their families, the investigators, and the teams who participated in this study. This work was funded by the National Key Research and Development Program of China (2023YFC3405100) (D.X.), as well as grants (No. 82303727) from The National Nature Science Foundation of China, Beijing Hospitals Authority Youth Programme (QML20231106) (D.X.), Clinical Medicine Plus X-Young Scholars Project of Peking University, the Fundamental Research Funds for the Central Universities (No. PKU2024LCXQ026) (D.X.), Beijing Physician Scientist Training Project (BJPSTP-2024-19) (D.X.), Science Foundation of Peking University Cancer Hospital (No. JC202404) (D.X.), and Beijing Capital’s Funds for Health Improvement and Research (CFH, No.2022-1-2151) (Baocai Xing) and the Primary Health Care Foundation of China - JINGRUI Liver Cancer Young Investigators Research and innovation capacity Building Public Welfare Project (D.X.).
Author information
Authors and Affiliations
Contributions
Da Xu and Baocai Xing had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Da Xu, Hongwei Wang, Kun Wang, and Baocai Xing were involved in the study concepts and design. All authors (Da Xu, Hongwei Wang, Quan Bao, Kemin Jin, Ming Liu, Wei Liu, Xiaoluan Yan, Lijun Wang, Yanqiao Zhang, Guangyu Wang, Yue Ma, Zhigang Ma, Chunhui Zhang, Jiebing Tang, Sha Wang, Jiaohui Pang, Ting Xu, Kun Wang and Baocai Xing) involved in the acquisition, analysis and interpretation of data. Kun Wang and Baocai Xing supervised the analysis. Da Xu and Hongwei Wang were involved in the draft of the manuscript. All authors read, critically revised, and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
S.W. and J.P. are employees of Nanjing Geneseeq Technology, Inc. T.X. is an employee of Jiangsu Alphamab Biopharmaceuticals Co., Ltd. The remaining authors declared that they have no competing interests.
Peer review
Peer review information
Nature Communications thanks Antonio D’Alessio, Dan Duda, Sze-Huey Tan, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, D., Wang, H., Bao, Q. et al. The anti-PD-L1/CTLA-4 bispecific antibody KN046 plus lenvatinib in advanced unresectable or metastatic hepatocellular carcinoma: a phase II trial. Nat Commun 16, 1443 (2025). https://doi.org/10.1038/s41467-025-56537-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-56537-y
This article is cited by
-
Remodeling the tumor dormancy ecosystem to prevent recurrence and metastasis
Signal Transduction and Targeted Therapy (2026)
-
Immune microenvironment in hepatocellular carcinoma: from pathogenesis to immunotherapy
Cellular & Molecular Immunology (2025)
-
Statins attenuate PD-L1 sorting to small extracellular vesicles dependent on ubiquitin-like 3 modification
Scientific Reports (2025)
-
Lokale und systemische Therapie beim hepatozellulären Karzinom
InFo Hämatologie + Onkologie (2025)
