
Abstract
Climate change mitigation policies lower greenhouse gas emissions and generally reduce fine particulate matter (PM2.5) concentrations, hereby bringing health co-benefits. Yet, the spatial and distributional air quality co-benefits in Europe of such policies are not fully understood. Here, We quantify premature mortality from air pollution in 1366 regions of Europe for different scenarios obtained from the Coupled Model Intercomparison Project Phase 6. We model PM2.5 concentrations at high spatial resolution and then combine it with population data and regional age structure and total mortality, to calculate attributable deaths. We find that the share of the European population meeting WHO (World Health Organization) guideline value for PM2.5 could exceed 90% by 2100 under the most ambitious scenario, while less than 10% under the least ambitious one. Corresponding premature deaths in Europe would total 67,000 (95% CI: 13,000–141,000) per year by the end of the century compared to 282,000 (95% CI: 202,000–364,000).
Similar content being viewed by others

Introduction
Despite improvements in air quality in recent decades, thanks to implemented emission reduction policies, air pollution still remains a major health concern for European citizens. In 2022, in the European Union, 96% of the urban population was still exposed to levels of fine particulate matter above the health guideline level of 5 μg per m3 for yearly average PM2.5 (particulate matter with diameter less than 2.5 micrometers) set by the World Health Organization (WHO)1. To tackle this issue, among other policies, the Zero Pollution action plan has set a target to reduce premature deaths due to exposure to fine particulate matter by 55% by 2030, compared to 2005.
Exposure to fine particulate matter, in particular PM2.5, is associated with the strongest health impacts among atmospheric pollutants2. They originate from air pollutant emissions, which to a large extent are linked to fossil fuel combustion3,4. Thus, there is a clear connection between climate and air quality policies. Decarbonization by transitioning away from fossil fuels, increasing energy efficiency, and promoting cleaner transportation options, generally contribute to decreased emissions of primary PM and secondary PM precursors such as nitrogen oxides, sulfur dioxide, and volatile organic compounds. So, climate mitigation, through decarbonization, ultimately has the important co-benefit5,6 of reducing the concentration of small particulate matters in the atmosphere7,8. In fact, it has been shown that stringent climate mitigation to meet the Paris agreement would bring co-benefits for human health globally, in different regions of the world9,10,11; while less ambitious scenarios could have detrimental air quality impacts12. Although reducing air pollutant emissions may have limited climate benefits (aerosols produce net cooling13) under specific circumstances) We focus in this paper on the health co-benefits of air quality due to climate mitigation actions14, with a particular focus on PM2.5, as this is the pollutant linked to the majority of human health impacts.
Large scale assessments of the co-benefits of climate mitigation on air quality have typically focused on averaged impacts across countries and regions of the world10,15,16. For instance, the co-benefits of tackling air pollution and climate change together have been studied over Europe (at coarse scale), showing how ambitious climate policies can be beneficial for air quality (and also including estimates of cost and monetized benefits on health). Air pollutant concentrations, however, can vary greatly across locations depending on pollution sources, degree of urbanization, climate, and geophysical conditions17,18,19, and their human impacts depend on the vulnerability of exposed population20. Understanding the spatial details and demographic distributional (in terms of age) impacts of air pollution in relation to greenhouse gas emissions is important (a) to target actions also at the local level, considering territorial; specificities, and (b) for further improving air quality in the most exposed and vulnerable regions in Europe.
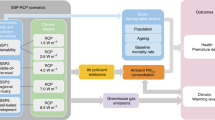
The aim of this study is to describe the spatial heterogeneity of health impacts (due to PM2.5 concentrations) of cutting greenhouse gas emissions across Europe (considering EU27 countries, Norway, Switzerland, and UK, from now on defined as the “study area”). To perform this study, we analyzed the recent population mortality associated with long-term exposure to outdoor air pollution2 across the study area and how it is projected to evolve under a range of different socioeconomic and emissions scenarios. We use a combination of the TM5-FAst Scenario Screening Tool (TM5-FASST)21 and Screening for High Emission Reduction Potential on Air (SHERPA)22 models to translate air pollutant emissions projections into air quality concentrations, and the Concentrations Response Function approach23 with spatial population projections from EUROSTAT “Ageing 2021 projections”24 to convert PM2.5 concentrations into population mortality at high spatial detail. We also analyse how PM2.5 related health impacts are distributed spatially and in terms of age class25. Results are presented using central estimates and 5th–95th percentile confidence intervals, derived through Monte Carlo analysis, to account for uncertainty in the health impact assessment (more details can be found in Methods, and Supplementary Note 3 and Supplementary Fig. 10). The contributions to the output uncertainty of key input variables is also quantified through sensitivity analysis. Finally, we mainly focus on the results of a dynamic demographic scenario, in which population, age structure, and age-specific all-cause mortality at regional level change in time. As additional analysis, we also assess how results would change under a static demographic scenario, which allows isolating the effects of population dynamics.
Results
Current air quality mortality in Europe
Figure 1 shows the all-cause death rate per 100,000 inhabitants attributable to air quality (AQDR) detailed by NUTS3 for the year 2015. AQDR can vary by more than 10 times across European regions and ranges from 4 to up to 212 deaths per 100,000 inhabitants.

Death rates (all-causes) per 100,000 inhabitants attributable to air quality (AQDR) across regions (NUTS3) in the study area. Year 2015. Countries and NUTS3 boundaries come from Eurostat/GISCO.
In 2015 we estimate that 315,000 (95% Confidence Interval: 227,000–403,000) premature deaths (AQD) can be attributed to poor air quality in the 30 European countries covered in this study. This is consistent with numbers reported by the European Environment Agency in their annual air quality reports26, where around 390,000 premature deaths were estimated for the same year. The largest share of deaths at the national level are found in Germany and Italy (around 56,000 per year), followed by France and Poland (nearly 30,000 per year), and Spain and UK (around 20,000 per year).
There is a considerable spatial variability at the regional level (NUTS3) in AQDR across Europe. The lowest AQDRs are observed for regions in Ireland, western and northern UK, Norway, Sweden, Finland, and the Alps, as well as for some isolated regions in southern France and central parts of the Iberian Peninsula. In Ireland and UK, prevailing winds are from the southwest and bring clear maritime air diluting air pollution concentrations27. Other regions with low mortality rates are typically sparsely populated and hence show lower emissions. It should be noted, however, that large uncertainties exist in estimating the effects of low exposure levels28. Higher AQDRs are observed for many regions in Eastern Europe, especially in Hungary, Romania, and Bulgaria, as well as some regions in Poland, where air pollution is still partly influenced by the combustion of very polluting fuels (i.e., coal). High AQDRs are also estimated in the Po Valley in Northern Italy. Despite recent reductions in anthropogenic emissions, air quality is still characterized by high air pollutant concentrations that are trapped in this area by the frequent occurrence of stagnant weather conditions at the foot of the Alps29.
Projections of air quality mortality in Europe
Figure 2 shows dynamics in population-aggregated total (all-cause) death rate, population age structure, population weighted exposure (PWE) and percentage of deaths attributable to air quality (from now on attributable fraction, AF) for the study area in 2015, 2050, and 2100. Total population is projected to remain fairly constant, while the total death rate increases slightly by 2050 to decrease mildly again afterwards (Fig. 2a). This is due to the combined effects of an ageing population and lower total death rates across all age classes. The substantial increase in elderly people (aged 85 and above) can be seen in Fig. 2b. PWE decreases in all scenarios except for SSP5-8.5 (SSP stands for “Shared Socioeconomic Pathways”), with much stronger reductions for stringent mitigation scenarios (Fig. 2c). Similar time patterns and differences among scenarios are found for AF (Fig. 2d).

a Time evolution of total death rate (DR), b age structure, c population weighted exposure (PWE) and d attributable fraction (AF) in the study area under the dynamic demographic scenario.
Figure 3 shows air quality related deaths (AQD) aggregated over the study area in 2015, 2050, and 2100 for the different emission scenarios, both for the dynamic and static demographic scenario. The premature mortality in 2015 amounted to 315,000 (95% CI: 227,000–403,000) deaths per year in the study area. Considering the dynamic demographic scenario, AQD will be lower under all scenarios by 2050 and 2100 compared to 2015. This is related to the combined effects of changing air pollution concentrations (due to emissions and air pollution control), as well as demographic changes. The beneficial effect of the decrease in PM2.5 concentrations is mitigated by the population aging, in a context of death rates remaining relatively stable.

a Historical (2015) and b, c projected (2050 and 2100) premature deaths attributable to air quality (AQD) aggregated on the study area. Each bar includes its confidence interval of the estimate calculated as detailed in the sensitivity analysis section. Lighter (darker) shading of bars refers to dynamic (static) demographic approach.
The scenarios characterized by ambitious greehhouse gases and air pollutants emission reductions show a very sharp reduction in AQD compared to 2015. AQD in 2100 for SSP1-1.9 and SSP1-2.6 are estimated at 67,000 (95% CI: 13,000–141,000) and 69,000 (95% CI: 15,000–144,000), respectively. Higher AQD are estimated for SSP2-4.5 (167,000; 95% CI: 109,000–234,000), SSP3-7.0 (207,000; 95% CI: 144,000–273,000), and SSP5-8.5 (279,000; 95% CI: 200,000–359,000). In 2050, higher fossil fuel-related activities under SSP5-8.5 compared to SSP3-7.0 are dampened by stronger air pollution control in SSP5-8.5, resulting in slightly lower mortality for this scenario. Yet, by 2100 the effects of strong air pollution control cannot longer compensate the very high levels of anthropogenic activities in a fossil fuel intensive world. This would result in 220,000 premature deaths per year, or 150,000 more than with stringent mitigation.
The beneficial effect of the reduced PM2.5 concentrations alone is shown by the AQD resulting from the static demographic scenario. In this case we observe trends across time and scenarios similar to the dynamic scenario with a decrease in AQD from 2015, which ranges from 22% for SSP3-7.0 to 70% for SSP1-1.9 in 2050, and from 11% for SSP3-8.5 to 79% for SSP1-1.9 in 2100.
The impact of concentration changes (comparison of the 2015 with the 2050 and 2100 static scenarios) is therefore higher than the impact of the demographic changes. Notably, the small overall impact of the demographic changes is the result of the contribution of two opposite time trends of death rates and aging population. The higher percentage of elderly people in the dynamic scenario translates into a bit higher AQD by 2050. By 2100, the increase in elderly people for the dynamic scenario is almost completely balanced by the decrease in all-cause death rates (due to better health systems, etc.), resulting in nearly equal mortality between the two demographic scenarios. Taken individually, the contributions from these two demographic factors could have a relevant impact, but they compensate each other.
Spatial variability in projections of air quality mortality in Europe
There is a large variability in air quality and related mortality across regions of Europe. According to the WHO air quality guideline, the yearly average levels of PM2.5 should remain below 5 μg per m330. In 2015, only 109 regions out of 1366 met the WHO guideline, corresponding to 5.4% of Europe’s population (see Table 1). By 2050, under the SSP1.1.9 dynamic scenario, more than 1000 regions, corresponding to 74.7% of Europe’s population, would meet the WHO target. A further increase of this percentage to 90.5% is estimated by the end of the century. For the high emission scenarios (SP3-7.0 and SSP5-8.5, on the other hand, 11.4% and 9.1% of population, respectively, will not meet the WHO guideline by 2100. Also for SSP2-4.5, about 740 regions, corresponding to 73.8% of people, will remain exposed to concentrations exceeding the WHO threshold.
Figure 4 provides an overview of AQDR values by 2050 and 2100 under the dynamic approach. Only the extreme and median mitigation scenarios are displayed here (SSP1-1.9, SSP2-4.5, SSP5-8.5), but the maps for all scenarios are available in Supplementary Figs. 2 and 3 for both the dynamic and the static approach. The maps show how SSP1-1.9 would lead to low AQDR in the large majority of regions. Only few areas (in Italy, Spain, the Benelux area, Eastern Europe) still have AQDRs higher than 50, for that scenario. This is not the case for the less ambitious scenarios. Considering for example, the SSP5-8.5 scenario, about 78% of regions show AQDR higher than 50.

Death rates attributable to air quality (AQDR) per 100,000 inhabitants at regional (NUTS3) level. Estimates are based on the dynamic demographic approach. a–c present the 2050 case for, respectively the SSP1-1.9, SSP2-4.5, and SSP5-8.5; while (d–f) similar information but for 2100. Countries and NUTS3 boundaries come from Eurostat/GISCO.
There is a marked difference among regions in the temporal pattern of AQDR. Figure 5 (with Supplementary Figs. 4 and 5 for the static approach) shows the change (in 2050 and 2100 compared to 2015) of AQDRs for the same three selected scenarios shown in the previous figure. While under SSP1-1.9 and SSP1-2.6 scenarios, almost all regions show a decrease of AQDR in 2100 compared to 2015, 3.7%, 7.5%, and 34.3% of regions undergo an increase in AQDR under the scenarios SSP2-4.5, SSP3-7.0, and SSP5-8.5, respectively. These differences in temporal patterns are found also for regions belonging to the same country, i.e., also between regions sharing the same time trend in precursor emissions. Supplementary Fig. 6 exemplifies this situation for two regions in Spain. The reason for these differences are mainly due to the combined effect of DR and age structure time trends in the different population. Almost all regions showing an increase in AQDR in 2100, are characterized by a huge increase in the proportion of people aged 85 or more. In any case, a full attribution analysis would require dedicated sensitivity analysis, and it is out-of-the-scope of this paper.

Relative change in death rates attributable to air quality (AQDR) in 2050 and 2100 compared to 2015. Estimates are based on the dynamic demographic approach. a–c present the 2050 case for, respectively the SSP1-1.9, SSP2-4.5, and SSP5-8.5; while (d–f) similar information but for 2100. Countries and NUTS3 boundaries come from Eurostat/GISCO.
Age distribution in projections of air quality mortality in Europe
Our analysis shows that air pollution has a much larger impact on the elderly compared to the younger age groups (i.e., below 44 years old). Figure 6, Supplementary Figs. 7 and 9 provide a closer look to the age-distribution of mortality across scenarios in terms of AQD and AQDR. In particular, focusing on the AQD of the dynamic case (Fig. 6) and the more affected category (people above 85 years, 85+) the historical case shows around 122,000 AQD (out of a total of around 315,000). We see that the SSP1-1.9 scenario would drastically reduce this value to 64,000 (in 2050) and 53,000 (in 2100). The median SSP2-4.5 shows an increase of AQD compared to 2015 (144,000 and 136,000 by 2050 and 2100, respectively). A much larger increase in AQD is shown for the SSP3-7.0 and SSP5-8.5 scenarios. The scenario SSP5-8.5 is the only scenario showing an increase in AQD from 2050 (163,000) to 2100 (224,000).

Premature deaths attributable to air quality for different age groups for a 2015, in b 2050 and c 2100 for the different SSP (Shared Socioeconomic Pathways) scenarios. Results for the dynamic demographic approach.
Supplementary Figs. 8 and 9 show the AQDR (average and range values) by age group, computed considering all NUTS3. Results do not show clear differences below 64 years across scenarios. On the contrary, from the 64 age group onward, a trend is appearing, with reduced mortalities for the most ambitious scenarios. These values increase for older age groups, with average values going from 76.5 (SSP1-1.9), to 484.8 (SSP2-4.5) and 581 (SSP5-4.5) AQDR in 2050.
Discussion
The focus of this paper is on the analysis of the impacts of some climate scenarios on mortality attributable to air quality, with a particular view on how these impacts vary in space (with high resolution) and time.
To address this issue, we used a combined modelling approach based on the TM5-FASST model to develop emission scenarios, the SHERPA model to convert emissions to concentrations and the Concentration Response Function approach to compute mortality attributable to air pollution. The focus of the study is on mortality attributable to PM2.5 yearly average concentrations, looking both at historical data (2015) and future scenarios (from 2020 to 2100). The study analyzes five combinations of SSP_RCP scenarios with different levels of ambition.
The high spatial resolution of the analysis both in terms of air quality and demographic detail is the main feature of the study. Varying time trends in PM2.5 exposure at 6 km resolution and in population age structure and mortality rates at NUTS3 level cause remarkable differences in the projected AQDR. Our results provide evidence of the spatial variability in terms of air quality impact of climate mitigation and indicates which regions would still require stronger and more focused air quality control.
To our knowledge this is one of the few available studies addressing the spatial variability of AQD associated to climate scenarios at high resolution and thus a direct comparison of our results with literature is not always possible considering our results at high spatial detail. For instance, the impact at 2050 of a combination of five SSP and two RCPs (RCP 2.6 and RCP 8.5) was analyzed for Barcelona12. For the AQD, and considering a cut-off at 2.4 μg per m3, they estimated under dynamic mortality approach a decrease of about 21% and an increase of about 9% associated to the scenarios SSP1-2.6 and SSP5-8.5, respectively. Our results show a very similar increase in AQD for the SSP5-8.5 scenario (8%) but a bigger decrease of AQD for the SSP1-2.6 scenario (38%).
A more direct comparison of our results with literature is possible considering AQD at the continental scale. Several studies2,31,32 estimated the health impact due to PM2.5 considering both the global scale and large spatial aggregations (usually continental). In the whole study area we showed that total historical (2015) AQD (300.000 premature deaths) could reach values lower than 50.000 or larger than 600.000 in 2050, depending on the ambition of the considered climate scenario. Our results are in line with previous studies, showing a reduced health impacts due to PM2.5 for the more ambitious scenarios and thus important co-benefits of mitigation scenarios. Yue et al.33 using a dynamic mortality approach (and considering a cut-off at 2.4 μg per m3) estimated a decrease of 21% and 67% from 2015 to 2050 associated to SSP1-2.6 scenario in the OECD and REF area (Eastern Europe countries + Russia), respectively. The same trend is therefore shown even though with a smaller decrease in AQD. More similar to the present study are the estimates found by these authors for the less ambitious scenarios with an increase of 8% and a decrease of 61% considering the SSP5-8.5 scenario in the OECD and REF areas, respectively. Another study was conducted by Silva et al.34 who analyzed (using a cut-off value between 5.9 μg per m3 and 8.7 μg per m3) three mitigation scenarios (RCP-2.6, RCP-4.5, and RCP-8.5) associated with ad hoc socio-economic projections. They found for Europe a decrease of about 200.000 AQD in 2050 (compared to year 2000) and about 100,000 in 2100, with minor differences between scenarios. A similar temporal trend in the health impact was also found by West at al.35 who analysed the AQD under RCP 4.5 estimating a decrease of about 300.000 deaths in 2050, followed by a slight increase in AQD in 2100.
Demographic factors play a key role in our AQD projections. While the total European population is not projected to change strongly in time, large differences are expected in its age structure. We have observed that the evolution of the 85+ population share is estimated to rise from about 3% in 2015 to 8% in 2050 and to 12% in 2100. And this has a considerable impact on AQD projections. Considering for example the SSP3-7.0, we estimated an increase of AQD for the 85+ age group from 122.000 in 2015 to about 220.000 in 2100 under the dynamic mortality approach (accounting for about 67% of AQD in 2100 compared to a quota of about 40% in 2015). To be noted, this increase in AQD in older ages is almost completely balanced by the decrease in AQD in the younger age groups (i.e., below 44 years old), in a context of overall stability of total death rates. Age structure and total death rates are therefore key factors in driving AQD projections and spatial variability. The importance of demographic changes has been underlined also by ref. 36 and should be carefully considered also to inform health prevention policies in the coming decades.
We estimated the robustness of our approach by performing an uncertainty and sensitivity analysis. In particular, we evaluated how the results of our modelling approach varied across 1000 Monte Carlo runs that sample uncertainty in the baseline mortality, relative risks, and cut-off value. Moreover, using Sensitivity Analysis indicators37 we further attributed the variability of the results to these uncertainty factors. We found that the baseline mortality uncertainty has a limited impact on the results. The uncertainty in the cut-off value strongly affects results for ambitious climate scenarios whereas the relative risk uncertainty is more important for low ambitious scenarios.
There are some limitations in the study. The first limitation is related to uncertainties associated with the definition of the scenarios, in particular in relation to the socio-demographic factors. However, in this study, we choose scenarios that are widely used in the climate change research community to facilitate the comparison with other studies and to provide insights on the range of possible impacts of different policies. A second limitation of the study is the use of a single model to simulate PM2.5 concentrations and population exposures. Several studies33,34 provided evidence of the large differences that may arise using different simulation models. However, our main objective was to identify the spatial differences in the health impact of future air quality using a high-resolution model (a spatial resolution roughly one order of magnitude higher than previous studies) and this prevented us from using more than one model. A third limitation concerns the epidemiological model and in particular its lacking interactions between PM2.5 exposure and other environmental risks closely related to climate change (e.g., bio-climatic discomfort, heat waves, ozone). We considered the results of current epidemiological studies not sufficiently robust to adopt concentration-response functions including those multiple interactions between risk factors. Considering these effects is however needed in future studies. A fourth limitation is that gender or pre-existing medical conditions are not considered in our health impact assessment. These factors can affect vulnerability to poor air quality. At present, however, differentiation based on gender and pre-existing medical conditions is not feasible at the scale of this application due to a lack of data. These additional distributional aspects are especially important when analysing different “type of deaths” due to air pollution (e.g., lung cancer, respiratory issues, ...) and are probably best investigated in a more local study with access to more detailed information on pre-existing medical conditions of people. A final limitation of the study is also related to the epidemiological approach. Following most studies available in literature we estimated the mortality burden attributable to PM2.5 as the result of the application of a concentration-response function using the population weighted exposure of a specific year. We used a concentration-response function referred to long term effects, justified by a number of studies showing much higher mortality burden associated to long-term compared to short-term effects38.
In conclusion, this study enabled to provide high resolution insight on the AQD associated to different climate mitigation and socio-demographic scenarios. The marked differences in AQD spatial and temporal patterns highlight the importance of more integrated air quality and climate policies, in which local level measures are combined with policies at the national and international levels.
Methods
A schematic view of the data and modeling framework applied in this study is presented in Supplementary Note 1. In the following sections, we describe each of the components in more detail.
Scenarios
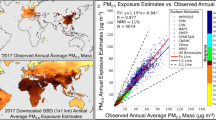
The year 2015 is selected as reference year to be consistent with previous studies33,39. High spatial resolution (roughly 6 × 6 km2) emissions detailed by sector and pollutant for 2015 are obtained from the Copernicus Atmosphere Monitoring Service (CAMS) v4.2 inventory40. The inventory primarily relies on the data officially reported to the Convention on Long-Range Transboundary Air Pollution for air pollutants. The inventory is also used in the global mosaic of best air pollutant emission databases by the Task Force on Hemispreric Transport of Air Pollution (TF HTAP) of the Air Convention41.
Air pollution emission scenarios at country level are defined by the so-called Shared Socioeconomic Pathway (SSP)—Representative Concentration Pathway (RCP) framework42. The selected scenarios are therefore indicated as SSP x-y where x indicates the societal evolution pathway and y the associated degree of climate forcing. The selected scenarios are SSP1-1.9, SSP-2.6, SSP2-4.5, SSP3-7.0, SSP5-8.5 and are characterized by a range of emissions, from very high (representative of fossil fuel intensive development in the absence of climate policies) to very low (including a sustainable and inclusive development trajectory). Air quality policies are linked to these climate scenarios, as explained in ref. 15. More information about SSP and RCP codes are provided in the Supplementary Table 1 and Supplementary Notes 1 and 2) while further details can be found in refs. 33,42.
The TM5-FASST model
The TM5-FASST is a global reduced-form air quality source-receptor model, used to compute ambient air pollutant concentrations as well as a broad range of pollutant-related impacts on human health, agricultural crop production, and short-lived pollutant climate metrics, taking as input annual pollutant emission data. For the European domain, it is applied at 0.1 degree resolution. In this work, TM5-FASST has been used to aggregate (at sectoral and country level) the SSP scenarios emissions, in a format compatible with the SHERPA air quality model.
The SHERPA model
The SHERPA model43,44 is a reduced-form air quality model that simulates pollutant concentrations in Europe.
SHERPA simulates PM2.5 yearly average concentrations using the “European Monitoring and Evalution Programme”45 as underlying Chemical Transport Model, with meteorology from the “Integrated Forecasting System”, “European Centre For Medium Weather Forercast” model46, and baseline emissions (including condensables for primary particulate matter residential emissions) from the CAMS v4.2 inventory40. In terms of input, the SHERPA model is fed by emissions of NOx, VOC, NH3, PPM, and SOx.
For the scenarios, emission changes by country-pollutant-year (as provided by TM5-FASST) are applied to the 2015 emission levels, assuming that relative emission changes are uniform within countries. In this way, the SHERPA model is run for the 5 considered scenarios from 2020 to 2100, with a 10-year interval to produce corresponding yearly average PM2.5 concentrations (in this paper, for sake of space, we focus on results in 2015, 2050, and 2100) at 6 km spatial resolution. Note that meteorology is unchanged for all scenarios, meaning that we do not evaluate the impact of meteorological changes on concentrations. In this way, we isolate the effect of emission changes on air quality and related health impacts21. It is worth noting that many studies have shown that the impact on PM2.5 concentrations of changes of meteorological variables due to climate change are expected to be relatively small compared to projected changes in emissions47,48. A validation of the concentrations in 2015, comparing model results and the estimation from the European Environmental Agency, is shown in Supplementary Fig. 11a.
Air quality mortality assessment
Gridded PM2.5 concentrations simulated by SHERPA for 2015 and for 10-year time steps for the scenarios are translated into population mortality by applying concentration-response functions23, in combination with spatial information on population counts, age structure, and age-specific all-cause mortality (for 5-year age classes above 20 years old). We use gridded (100 m) population counts for 2015 from the Global Human Settlement Layer49, which are aggregated to the grid of the air quality model (6 km). The population counts in the 6 km grids are combined with their corresponding PM2.5 concentrations to obtain population-weighted average PM2.5 concentrations for each administrative region at NUTS3 level (NUTS = Nomenclature of territorial units for statistics). In the study area there are 1366 NUTS3 regions. Information on the age structure (in 5-year classes) and age-specific total (all-cause) mortality is available only at NUTS3 scale (both for the historical period and projections), rather than at grid scale. The premature deaths are then estimated at NUTS3 level by combining the population-weighted average concentrations, population counts for different age classes, and the corresponding age-specific all-cause mortality using concentration response functions. Mortality for the 5-year classes is aggregated to obtain total mortality.
Total baseline death rates (DR) are obtained from the “Institute for Health Metrics Evaluation, Global Burden of Disease” IHME-GBD-2019 database50. These baseline mortalities are available at country level for 5-year age classes, which we then spatially allocate to the SHERPA grid.
For each 5-year age class i, mortality rates attributable to air quality (AQDR) are calculated as a fraction of the TDR for that age class (with both AQDR and TDR expressed per 100,000 inhabitants), using Eq. (1).
where AFi represents the fraction of total mortality attributable to air quality in the age class i. Following most epidemiological studies we considered AF independent from the age class and calculated it using Eq. (2).
where RR represents the relative risk. While the relative risk can be quantified based on a non-linear exposure-response function with higher increase at lower PM2.5 concentrations and lower increase at higher concentrations31, WHO still recommends assuming a linear relationship between the increase in PM2.5 concentrations and the % increase in the risk of mortality1. This has been shown to be appropriate at the concentration range typical of European cities and has been adopted by most European studies51. In particular, the relative risk is calculated as in ref. 23 using Eq. (3).
where PM represents the PM2.5 exposure difference between yearly average concentrations and 5 μg per m3, which is the reference concentration to which WHO recommends reducing air pollution levels to protect human health (however, in this study we also considered a cut-off to 0, to perform uncertainty and sensitivity analysis of the results).
AQDRs are then converted into premature deaths attributable to air pollution (AQD), by combining them with population counts and age structure information for the baseline (2015) and the projections. For this, we used demographic data available at NUTS3 level, as derived from EUROPOP2019 projections52.
We considered two scenarios of total mortality, referred to as ‘Static’ and ‘Dynamic’ approach. In the Static case, total population and TDRs were kept fixed in time (using the most recent available year). This implies that static human vulnerability to air quality, i.e., the AQDR for a given concentration of PM2.5, remains constant in time; this can be considered as the most conservative (pessimistic) case. In the Dynamic case, total population and baseline mortality change in time. In particular, baseline mortality gradually reduces in time as a result of better health systems, improved hygiene and living standards and better welfare policies. In this case, it is implicitly assumed that human vulnerability to air quality drops at the same rate as total mortality. Both cases (Static and Dynamic) are considered when presenting the results.
Results are computed for 5-years age classes aggregated to the following 5 age groups: 20–44 years, 45–64 years, 65–74 years, 75–84 years, and 84+ years. Spatially, all results are analyzed based on the NUTS3 classification. A validation of the Air Quality Deaths (AQD) in 2015, comparing model results and the estimation from the European Environmental Agency, is shown in Supplementary Fig. 11b.
Sensitivity analysis
When using complex modelling frameworks as the one applied in this study, it is important to analyze how the results are affected by input and model uncertainty. To explore this, we carried out an uncertainty and sensitivity analysis in which we perform multiple runs using different combinations of parameter values and modeling assumptions. Sources of uncertainty in this study mainly arise from the air quality modeling part and the health impact assessment part. While the uncertainty of the air quality modeling has been treated elsewhere (please refer to ref. 21 for the FASST model, and to ref. 53 for SHERPA), this is not the case of the health impact assessment part. We consider uncertainty stemming from 3 key aspects: baseline mortality, relative risks, and cut-off value of PM2.5 concentration below which no health impact is assumed. We perform a Monte Carlo analysis with sample size of 1000 in order to explore how the uncertainty related to these variables propagates to and affect the modeled mortality. A complete description of the proposed approach is provided in Supplementary Note 3 and Supplementary Fig. 10. In terms of emissions, we used the CAMS emission inventory, state-of-the-art for EU level emissions, as shown by previous studies40.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data used in this study have been deposited in the database accessible at https://zenodo.org/records/14851594. Shapefiles of country and NUTS3 boundaries were downloaded from the Geographic Information System of the European Commission (GISCO) (https://ec.europa.eu/eurostat/web/gisco).
Code availability
The code generated in this study have been deposited in the database accessible at https://zenodo.org/records/14851594.
References
WHO. WHO Global Air Quality Guidelines: Particulate Matter (PM2. 5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide (WHO, 2021).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet 403, 2162–2203 (2024).
Hopke, P. K., Dai, Q., Li, L. & Feng, Y. Global review of recent source apportionments for airborne particulate matter. Sci. Total Environ. 740, 140091 (2020).
Karagulian, F. et al. Contributions to cities’ ambient particulate matter (pm): a systematic review of local source contributions at global level. Atmos. Environ. 120, 475–483 (2015).
Markandya, A. et al. Health co-benefits from air pollution and mitigation costs of the paris agreement: a modelling study. Lancet Planet. Health 2, e126–e133 (2018).
Sampedro, J. et al. Health co-benefits and mitigation costs as per the paris agreement under different technological pathways for energy supply. Environ. Int. 136, 105513 (2020).
Braspenning Radu, O. et al. Exploring synergies between climate and air quality policies using long-term global and regional emission scenarios. Atmos. Environ. 140, 577–591 (2016).
Fujimori, S., Kainuma, M., Masui, T., Hasegawa, T. & Dai, H. The effectiveness of energy service demand reduction: a scenario analysis of global climate change mitigation. Energy Policy 75, 379–391 (2014).
Vandyck, T. et al. Air quality co-benefits for human health and agriculture counterbalance costs to meet Paris agreement pledges. Nat. Commun. 9, 4939 (2018).
Hamilton, I. et al. The public health implications of the Paris agreement: a modelling study. Lancet Planet. Health 5, e74–e83 (2021).
Belis, C. A., Van Dingenen, R., Klimont, Z. & Dentener, F. Scenario analysis of PM2.5 and ozone impacts on health, crops and climate with TM5-FASST: a case study in the Western Balkans. J. Environ. Manag. 319, 115738 (2022).
Ingole, V. et al. Local mortality impacts due to future air pollution under climate change scenarios. Sci. Total Environ. 823, 153832 (2022).
Scovronick, N. et al. The impact of human health co-benefits on evaluations of global climate policy. Nat. Commun. 10, 2095 (2019).
Dimitrova, A. et al. Health impacts of fine particles under climate change mitigation, air quality control, and demographic change in India. Environ. Res. Lett. 16, 054025 (2021).
Rao, S. et al. Future air pollution in the shared socio-economic pathways. Glob. Environ. Change 42, 346–358 (2017).
Reis, L. A., Drouet, L. & Tavoni, M. Internalising health-economic impacts of air pollution into climate policy: a global modelling study. Lancet Planet. Health 6, e40–e48 (2022).
Colmer, J., Hardman, I., Shimshack, J. & Voorheis, J. Air pollution disparities in PM2.5 air pollution in the United States. Science 575–578. https://www.science.org.
Shetty, S. et al. Daily high-resolution surface PM2.5 estimation over Europe by ML-based downscaling of the CAMS regional forecast. Environ. Res. 264, 120363 (2025).
Degraeuwe, B., Pisoni, E., Christidis, P., Christodoulou, A. & Thunis, P. Sherpa-city: a web application to assess the impact of traffic measures on NO2 pollution in cities. Environ. Model. Softw. 135, 104904 (2021).
Grekousis, G., Sunarta, I. N. & Stratoulias, D. Tracing vulnerable communities to ambient air pollution exposure: a geodemographic and remote sensing approach. Environ. Res. 258, 119491 (2024).
Dingenen, R. V. et al. Tm5-fasst: a global atmospheric source-receptor model for rapid impact analysis of emission changes on air quality and short-lived climate pollutants. Atmos. Chem. Phys. 18, 16173–16211 (2018).
Pisoni, E. et al. Sherpa-cloud: an open-source online model to simulate air quality management policies in Europe. Environ. Model. Softw. 176, 106031 (2024).
Héroux, M. E. et al. Quantifying the health impacts of ambient air pollutants: recommendations of a WHO/Europe project. Int. J. Public Health 60, 619–627 (2015).
The 2021 ageing report: Economic and budgetary projections for the EU member states (2019-2070). Institutional Paper 148, European Commission, Directorate-General for Economic and Financial Affairs, Brussels https://economy-finance.ec.europa.eu/publications/2021-ageing-report-economic-and-budgetary-projections-eu-member-states-2019-2070_en (2021).
Pisoni, E., Dominguez-Torreiro, M. & Thunis, P. Inequality in exposure to air pollutants: a new perspective. Environ. Res. 212, 113358 (2022).
Guerreiro, C. et al. European Environment Agency, European Topic Centre on Air Pollution and Climate Change Mitigation (ETC/ACM). Air quality in Europe – 2018 report, (Publications Office, 2018).
Graham, A. M. et al. Impact of weather types on uk ambient particulate matter concentrations. Atmos. Environ.: X 5, 100061 (2020).
Lehtomäki, H. et al. Deaths attributable to air pollution in Nordic countries: disparities in the estimates. Atmosphere 11 https://www.mdpi.com/2073-4433/11/5/467 (2020).
Robotto, A. et al. Improving air quality standards in Europe: comparative analysis of regional differences, with a focus on northern Italy. Atmosphere 13 https://www.mdpi.com/2073-4433/13/5/642 (2022).
Organization, W. H. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide https://apps.who.int/iris/handle/10665/345329 License: CC BY-NC-SA 3.0 IGO (World Health Organization, Geneva, 2021).
Murray, C. et al. Gbd 2019 risk factors collaborators: global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396, 1223–1249 (2020).
Burnett, R. et al. Global estimates of mortality associated with longterm exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 115, 9592–9597 (2018).
Yue, H. et al. Substantially reducing global PM2.5-related deaths under SDG3. 9 requires better air pollution control and healthcare. Nat. Commun. 15, 2729 (2024).
Silva, R. A. et al. The effect of future ambient air pollution on human premature mortality to 2100 using output from the ACCMIP model ensemble. Atmos. Chem. Phys. 16, 9847–9862 (2016).
West, J. J. et al. Co-benefits of mitigating global greenhouse gas emissions for future air quality and human health. Nat. Clim. change 3, 885–889 (2013).
Yang, H., Huang, X., Westervelt, D. M., Horowitz, L. & Peng, W. Socio-demographic factors shaping the future global health burden from air pollution. Nat. Sustainability 6, 58–68 (2023).
Mara, T. A. & Becker, W. E. Polynomial chaos expansion for sensitivity analysis of model output with dependent inputs. Reliab. Eng. Syst. Saf. 214, 107795 (2021).
Izah, S., Ogwu, M., Etim, N., Shahsavani, A. & Namvar, Z. Short-term health effects of air pollution. In Air Pollutants in the Context of One Health: Fundamentals, Sources and Impacts, (Izah, S. C., Ogwu, M. C., Shahsavani, A eds.). vol. 134, 249–278 (Hdb Env Chem Cham, 2024).
Pisoni, E., Thunis, P. & Clappier, A. Application of the Sherpa source-receptor relationships, based on the EMEP MSC-W model, for the assessment of air quality policy scenarios. Atmos. Environ.: X 4, 100047 (2019).
Kuenen, J. et al. Cams-reg-v4: a state-of-the-art high-resolution European emission inventory for air quality modelling. Earth Syst. Sci. Data 14, 491–515 (2022).
Crippa, M. et al. The htap_v3 emission mosaic: merging regional and global monthly emissions (2000–2018) to support air quality modelling and policies. Earth Syst. Sci. Data 15, 2667–2694 (2023).
O’Neill, B. C. et al. Achievements and needs for the climate change scenario framework. Nat. Clim. change 10, 1074–1084 (2020).
Thunis, P. et al. PM2.5 source allocation in European cities: a SHERPA modelling study. Atmos. Environ. 187, 93–106 (2018).
Thunis, P., Degraeuwe, B., Pisoni, E., Ferrari, F. & Clappier, A. On the design and assessment of regional air quality plans: the SHERPA approach. J. Environ. Manag. 183, 952–958 (2016).
Simpson, D. et al. The EMEP MSC-W chemical transport model–technical description. Atmos. Chem. Phys. 12, 7825–7865 (2012).
Hersbach, H. et al. The ERA5 global reanalysis. Q. J. R. Meteorological Soc. 146, 1999 - 2049 (2020).
Westervelt, D. et al. Quantifying PM2.5-meteorology sensitivities in a global climate model. Atmos. Environ. 142, 43–56 (2016).
He, H., Liang, X.-Z. & Wuebbles, D. J. Effects of emissions change, climate change and long-range transport on regional modeling of future us particulate matter pollution and speciation. Atmos. Environ. 179, 166–176 (2018).
Pesaresi, M. et al. Advances on the global human settlement layer by joint assessment of Earth observation and population survey data. Int. J. Digital Earth 17 https://www.scopus.com/inward/record.uri?eid=2-s2.0-85202789083&doi=10.1080%2f17538947.2024.2390454&partnerID=40&md5=6a062a90c332124dee9a89404d51a8db. Cited by: 0; All Open Access, Gold Open Access. (2024).
Rafael, L. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2095–2128 (2012).
Soares, J. et al. Health risk assessment of air pollution and the impact of the new WHO guidelines (Eionet Report – ETC HE 2022/10). European Topic Centre on Human Health and the Environment (2022).
Eurostat. Population on 1st January by age, sex and type of projection https://ec.europa.eu/eurostat/databrowser/view/proj_19np/default/table?lang=en (2023).
Pisoni, E. et al. Application of uncertainty and sensitivity analysis to the air quality SHERPA modelling tool. Atmos. Environ. 183, 84–93 (2018).
Acknowledgements
We acknowledge the GHSL (Global Human Settlement Layer, https://human-settlement.emergency.copernicus.eu/) team, for providing population data used in this study. This study received funding from DG REGIO of the European Commission as part of the ‘Territorial Risk Assessment of Climate in Europe’ (TRACE) project (Administrative Agreement Nr JRC 36206-2022 // DG REGIO 2022CE160AT126). We also acknowledge Rossana Rosati and Elena Bastianon (JRC) for their help in the uncertainty and sensitivity analysis evaluation.
Author information
Authors and Affiliations
Contributions
E.P., C.B., L.F., and R.V.D. worked on the design of methodology, analysis, interpretation of results and the writing of the manuscript; C.M. and S.Z.S. contributed to the analysis and production of the data; S.K., F.M.F., B.B., J.M., and P.T. on the review and editing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Shaojie Song, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pisoni, E., Zauli-Sajani, S., Belis, C.A. et al. High resolution assessment of air quality and health in Europe under different climate mitigation scenarios. Nat Commun 16, 5134 (2025). https://doi.org/10.1038/s41467-025-60449-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-60449-2
This article is cited by
-
Assessing the health impact of the national air pollution control programme at city level: the case of Madrid
Clean Technologies and Environmental Policy (2026)
-
Climate action and clean cooking are vital for sustaining air pollution-related health benefits
Nature Sustainability (2025)
