
Abstract
Prenatal Zika virus (ZIKV) exposure can result in outcomes ranging from severe birth defects to subtle developmental delays, yet the underlying mechanisms remain unclear. Using a translational rhesus macaque model, we assess visual, auditory, and neurodevelopmental outcomes through 12 months of age following first-trimester ZIKV inoculation. Pregnant macaques, either flavivirus-naive or with prior dengue virus (DENV) exposure, are inoculated with Asian or African ZIKV lineages. Maternal viremia duration, placental viral burden, and neutralizing antibody titers vary but are not associated with developmental outcomes. At 12 months, ZIKV-exposed infants exhibit altered maternal attachment behaviors and reduced inhibition toward novel sensory stimuli. Visual evoked potentials are impaired at 3 months but normalize by 12 months; hearing loss is more frequent but not statistically significant. These outcomes are driven by ZIKV exposure itself, independent of maternal infection characteristics. Our findings highlight the limitations of maternal biomarkers in risk prediction and support incorporating infant-focused developmental outcomes in studies of maternal interventions.
Similar content being viewed by others

Introduction
Prenatal Zika virus (ZIKV) exposure produces a broad range of infant outcomes, including birth defects, neurodevelopmental delays, hearing loss, and visual impairment. ZIKV continues to cause periodic outbreaks in endemic regions, while emerging transmission is being detected in previously unaffected areas1,2. Notably, nearly 30% of affected human infants are asymptomatic at birth but develop neurodevelopmental deficits during early childhood3,4. These deficits span language, cognitive, motor, hearing, and visual domains4,5,6,7,8, alongside impairments in mobility, communication, and social cognition3,5. A smaller proportion (~6%) present at birth with congenital Zika syndrome, a constellation of findings including microcephaly, brain and ocular anomalies, congenital joint contractures, and neurologic sequelae such as sensorineural hearing loss9,10. Prenatal ZIKV infection also impacts vision11 and may impact hearing12,13, and early disruptions in vision and hearing are well recognized to profoundly influence language acquisition, cognition, and socio-emotional development14,15. Yet, critical gaps remain in understanding how maternal ZIKV infection conditions—including viral dynamics and immune responses—shape these developmental trajectories. Elucidating these relationships could enable earlier risk stratification and inform targeted intervention strategies.
Translational rhesus macaque models provide a uniquely powerful system for understanding how maternal ZIKV infection conditions shape developmental outcomes. Compared with murine models, macaques exhibit closer parallels to human placentation, gestational timelines, and fetal neurodevelopmental maturation16,17. Rhesus macaques have been firmly established as models for congenital ZIKV infection16,17,18,19,20 and have a longstanding role in modeling human neurodevelopment21. Our preclinical macaque model bridges critical gaps in clinical research by directly assessing ocular and auditory outcomes22 and by demonstrating visual orientation deficits in offspring with prenatal ZIKV exposure and maternal dengue virus (DENV) immunity23. The convergence of neurodevelopmental similarity and an established infection model uniquely positions rhesus macaques to unravel predictors of childhood developmental impairments.
Maternal viral dynamics and humoral immune responses may influence congenital infection outcomes; however, the relationship between these factors and the most common outcomes, namely developmental deficits, remains unclear. Although the hypothesis that prolonged maternal viremia increases the risk of adverse pregnancy and neonatal outcomes is biologically plausible, supporting data are limited. To date, only one cohort study from French Guiana has directly compared outcomes based on maternal viremia duration, demonstrating that maternal plasma viremia persisting for more than 30 days was associated with an increased risk of fetal loss and structural brain abnormalities24. Additional support for this hypothesis is suggested by multiple human case reports25,26,27. Maternal neutralizing antibody (nAb) responses may also modulate outcomes, as higher nAb titers measured 36–60 days after acute infection were associated with a reduced risk of microcephaly and structural brain abnormalities in one human study28, although neurodevelopmental outcomes were not assessed. Better characterization of maternal viro-immunologic parameters associated with neurodevelopmental deficits could identify potential targets for future early intervention strategies.
Maternal pre-existing immunity to dengue virus (DENV), resulting from infection prior to pregnancy, may influence offspring outcomes following prenatal Zika virus (ZIKV) exposure. In human pediatric cohorts, prior DENV infection has been associated with reduced risk of symptomatic ZIKV disease, suggesting potential cross-protection29. However, experimental data from in vitro systems, ex vivo placental models, and murine studies raise concerns that DENV-specific IgG could enhance ZIKV infection via antibody-dependent enhancement mechanisms30,31. In contrast, translational studies in nonpregnant macaques have shown no evidence that pre-existing DENV immunity increases ZIKV titers or disease severity32,33. We previously demonstrated that maternal DENV immunity can worsen early neurodevelopmental outcomes in neonatal macaques exposed to ZIKV in utero23; however, its impact on later developmental outcomes has not been evaluated. This knowledge gap is increasingly important as DENV incidence rises in parts of South America34, and human studies remain inconclusive—some reporting no association between maternal DENV immunity and adverse pregnancy outcomes35,36,37, while others suggest a protective effect against congenital Zika syndrome38. Defining how prior maternal DENV immunity modulates the effects of prenatal ZIKV exposure on long-term development is essential to optimize early intervention strategies and inform maternal risk assessment.
The timing of maternal Zika virus (ZIKV) infection during pregnancy critically influences offspring outcomes. First-trimester infections are well established to confer a higher risk of birth defects and microcephaly compared to infections occurring later in pregnancy9,39,40,41. However, the impact of gestational age at exposure on longer-term developmental outcomes is less well-studied. A recent study reported that children with prenatal ZIKV exposure exhibited motor and cognitive delays, with first-trimester exposure associated with an 11.2-fold greater odds of adverse developmental outcomes compared to third-trimester exposure7. Nonetheless, the first trimester encompasses a broad period of early development, and it remains unclear whether the timing within the first trimester further modifies the risk of developmental deficits.
Finally, infection with different ZIKV lineages may impact developmental outcomes. Two primary lineages exist—Asian-American and African. While African-lineage ZIKV has circulated since its initial detection in 1947, its role in congenital infection and subsequent developmental impairments remains poorly characterized in humans. In pregnant immunocompromised mouse models, African-lineage strains have demonstrated greater fetal harm and mortality than Asian-lineage strains42. Similarly, nonhuman primate studies report higher burden of ZIKV RNA within the maternal-fetal interface43 and high rates of fetal demise following African-lineage ZIKV infection during early gestation44 compared to Asian-lineage ZIKV. However, whether these findings extrapolate to humans remains unclear. Defining the impact of African-lineage ZIKV on early childhood development is critical to capturing the full clinical spectrum of congenital ZIKV disease.
To address these gaps, we conducted longitudinal assessments of visual and auditory development during the first year of life and characterized neurodevelopmental outcomes at 12 months in a translational rhesus macaque model of prenatal ZIKV exposure. Using the largest cohort of prenatally ZIKV-exposed infant macaques to date (n = 41), we investigated how maternal ZIKV inoculation, viremia duration, and antibody responses influence infant developmental trajectories. These data offer critical insight into the lasting impact of prenatal ZIKV exposure and the limitations of maternal biomarkers in predicting neurodevelopmental outcomes.
Results
Virologic outcomes
Pregnant ZIKV-inoculated animals developed positive plasma ZIKV viral RNA (vRNA) loads in the first few days after inoculation (Fig. 1a). The duration of positive plasma vRNA loads varied among animals, ranging from 2 to 70 days, but did not differ significantly among dams with different maternal ZIKV inoculation conditions, including inoculation of ZIKV-PR at ~30 or ~45 gestational days (gd), history of infection with DENV, or with ZIKV-DAK (Fig. 1b and Table S1). Area under the plasma vRNA load curve (AUC) also did not differ between dams in the different maternal ZIKV inoculation conditions (Fig. 1c). We also examined the vRNA loads in the maternal interface tissues following Cesarean delivery, specifically examining viral loads separately in the placenta, decidua, and chorionic membrane in biopsies from all the cotyledons in both placentas and found no differences between groups (Fig. 1d). When biopsies from the placenta, decidua, and chorionic membrane were combined as a single parameter (% of total biopsies), there was also no difference between dams in the inoculation groups (Table S1). Amniotic fluid vRNA loads measured at the time of Cesarean delivery for the ZIKV-exposed dams were negative (Table S2). There were also no differences in the ZIKV-specific neutralizing antibody titers (plaque reduction neutralization test, PRNT90) 1 month post-inoculation between the different maternal inoculation groups (Fig. 1e). We also assessed infants for ZIKV vRNA in plasma and urine, and for ZIKV-specific IgM, as direct markers of fetal infection. None of the infants had detectable ZIKV RNA in plasma (measured longitudinally from birth to 12 months of age) or in urine (measured at birth) (Table S3). None of the infants had detectable ZIKV-specific IgM measured at 0–8 days of age (Table S4). Because we detected neither ZIKV RNA nor virus-specific IgM, we refer to these infants as ZIKV-exposed for future discussion, although it is possible that vRNA and/or IgM were present at one time but cleared after the first trimester infection more than 110 days before delivery.

a ZIKV vRNA loads in plasma following inoculation in the ZIKV-PR 30gd, ZIKV-PR-45gd, DENV/ZIKV, and ZIKV-DAK groups. b Duration of plasma viremia, defined as the last day of a vRNA load above the limit of detection (150 copies/ml). c Area under the plasma viremia curve. d The proportion of biopsies from the placenta, decidua, chorionic plate, and all three combined (total) that were vRNA-positive (above the limit of detection of 3 copies/mg of tissue) at delivery. e PRNT90 titers 1 month post-infection. Box plots show the interquartile range within the box, the median as a dark horizontal line, and the minimum and maximum values excluding the outliers are shown as whiskers.
Infant demographics and growth
A total of 41 pregnancies and their offspring were included in this study. Because there were no significant virologic differences among the maternal infection conditions, the ZIKV-exposed offspring are grouped together for subsequent analyses and compared to the control infants and then split into inoculation groups if differences were observed between control and ZIKV-exposed offspring. The control offspring were exposed to the same prenatal and postnatal stressors (maternal sedation events, infant exams, blood draws) as the ZIKV-exposed offspring. The ZIKV-exposed and control infants had similar gestational ages at inoculation, 39.8 and 40.2 days, respectively (t = 0.29, p = 0.7683) (Table S5). Half of the ZIKV-exposed infants were male (51.7%) and none of the control infants were male (χ² = 12.03, p = 0.0014) (Table S5). The proportion of male and female infants in each group was random because dams were divided into inoculation groups before fetal sex was known. Nearly all infants were delivered by Cesarean section in both the ZIKV-exposed (89%) and control (92%) groups (χ² = 0.02, p = 0.9999) (Table S5). There was no significant difference in proportion of infants that were housed with a dam (either biological or surrogate) compared to infants housed in the nursery then peer group reared throughout the first year of life (χ² = 0.93, p = 0.3344) or infant ages at hearing, eye, or developmental examinations (Table S5). ZIKV-exposed infants have similar weights at birth (within 10 days of birth) as control infants, but have a significantly greater weight gain trajectory from birth to 12 months of age (Slope of 146 g/month vs. 137.3 g/month, p value 0.0317), and are heavier at 12 months of age (2.2 kg vs. 2.1 kg, p value 0.0121) (Fig. 2 and Table S6). There was no association between ZIKV-exposed infants’ weight at 12 months and maternal viral or immunologic parameters (Fig. S1). Head circumferences were similar between ZIKV-exposed and control infants at birth and 12 months of age, and the trajectories were similar as well (Table S6).

Infant weight and head circumference was measured longitudinally (ZIKV n = 29, control n = 12). a Birth weights. b Weight gain trajectory from birth to 12 months. The mean weight is shown by the solid line and the 95% confidence interval by the shaded area. ZIKV-exposed infants had a significantly greater weight gain trajectory (slope 146.1 g/month vs. 137.3 g/month; t(39) = 2.19, p = 0.0317, d = 0.74, 95% CI [0.05, 1.43]). c Weights at 12 months. ZIKV-exposed infants had significantly greater weights at 12 months (2.2 kg vs. 2.1 kg; t(39) = 2.67, p = 0.0121, d = 0.90, 95% CI [0.20, 1.60]). d Head circumferences at birth. e Head circumferences from birth to 12 months. The mean head circumference is shown by the solid line and the 95% confidence interval by the shaded area. f Head circumferences at 12 months. Complete statistical comparisons are provided in Table S6. Weight comparisons were analyzed using linear mixed-effects models; all tests were two-sided. No adjustments were made for multiple comparisons as these were pre-specified primary outcomes. For box plots (a, c, d, f), the center line represents the median, box bounds represent the 25th and 75th percentiles (interquartile range), and whiskers extend to the minimum and maximum values excluding outliers (values beyond 1.5× IQR).
Infant development
We compared infant development at 12 months of age between ZIKV-exposed infants and controls within the domains of social-emotional development, sensory responsiveness, visual motor, fine motor, and cognitive skills. Behavioral assessments included ZIKV (n = 26) and control (n = 9) infants raised in dyads. Due to factors such as COVID-19 research restrictions, there is missing data in some behavioral assessments. Infants raised in peer-groups were excluded from the behavioral analysis.
Social-emotional development was assessed in dam-reared infants by analyzing video recordings of maternal-infant interactions in their home enclosure. ZIKV-exposed infants spent significantly more time in mutual ventral contact (36.3% vs. 0.0%, Z = 2.49, p = 0.0127), close proximity with their mothers (74.8% vs. 50.4%, Z = 2.43, p = 0.0149), and nipple contact (33.3% vs. 0.0%, Z = 2.60, p = 0.0093), compared to control infants (Fig. 3 and Table S7), suggesting that ZIKV exposure impacts social attachment. These behaviors were not mutually exclusive—infants could be in nipple contact and mutual ventral contact simultaneously—but they were not entirely co-dependent, as nipple contact sometimes occurred independently. To determine whether increased maternal contact in ZIKV-exposed infants resulted from infant impaired motor function, we compared the duration of time spent moving around the enclosure (i.e., in locomotion). There was no significant difference in the time spent moving through the enclosure between ZIKV-exposed and control groups (Z = −0.894, p = 0.3751) (Fig. 3), indicating that reduced locomotion was not responsible for increased maternal attachment. Next, we examined whether the inoculation group influenced the mutual ventral contact phenotype, a well-recognized measure of attachment from video recordings. Infants in the ZIKV-PR 45gd group spent significantly more time in mutual ventral contact than controls (48.8% vs. 9.7%, Z = 2.43, p = 0.0104), with no other significant pairwise differences (Table S7). We also assessed if maternal virologic and antibody variables predicted mutual ventral contact duration using linear regression. Maternal viremia duration, area under the viral load curve, percentage of maternal-fetal interface biopsies positive for vRNA, and PRNT90 titer were not significantly associated with mutual ventral contact duration (Fig. 3). These findings suggest that prenatal ZIKV exposure alone influences social attachment development at 12 months of age, but specific maternal virologic and antibody measurements did not.

Mother-infant dyads (ZIKV n = 26, control n = 9) were videotaped in their home enclosure, and the durations spent in nipple contact, togetherness, ventral contact, and locomotion were recorded as a percentage of the total observation time (a). Significant differences between ZIKV-exposed and control groups were assessed using two-sided Wilcoxon rank-sum tests: mutual ventral contact (Z = 2.49, p = 0.0127, ZIKV median = 36.3%, control median = 0.0%), togetherness (Z = 2.43, p = 0.0149, ZIKV median = 74.8%, control median = 50.4%), and nipple contact (Z = 2.60, p = 0.0093, ZIKV median = 33.3%, control median = 0.0%). b Mutual ventral contact duration by inoculation group. A significant difference between ZIKV-PR 45gd and control groups was observed (49.4% vs 0.0%; two-sided Wilcoxon rank-sum test, Z = 2.43, p = 0.0104). The association between mutual ventral contact duration and maternal infection variables were assessed using linear regression, including plasma viremia duration (c), area under the curve plasma viral load (d), maternal-fetal interface biopsies that were vRNA positive (e) and PRNT90 titer (f). For box plots (a, b), the center line represents the median, box bounds represent the 25th and 75th percentiles (interquartile range), and whiskers extend to the minimum and maximum values excluding outliers (values beyond 1.5× IQR), with individual data points overlaid. For scatter plots (c–f), data are presented as individual values with linear regression lines; shaded areas represent the 95% confidence interval of the regression. Linear regression statistics (R2, t-statistic, and p value) are displayed on each graph.
Infant fine motor, visual motor, and cognitive skills were assessed in dam-reared infants through manipulation of the puzzle feeder over 3 days. The maximum puzzle feeder level completed by either group was 4 out of 8. The ZIKV-exposed infants performed similarly as the control infants for the number of levels completed (Fig. 4 and Table S7). Although they ended up completing a similar number of levels, some ZIKV-exposed infants took longer to complete level 1, even though there was no significant difference in the time to complete level 1 overall (Fig. 4). ZIKV-exposed infants had a similar number of attempts to complete level 1 and level 2 as the control infants (Fig. 4). To assess the role of motor deficits, digit isolation and overall motor coordination were assessed, but no significant differences were identified (Table S7). These findings indicate that prenatal ZIKV exposure does not impair motor, visuomotor, or cognitive performance on a puzzle feeder task at 12 months of age in this study.

a The number of levels completed by ZIKV-exposed and control infants did not differ. b The time to complete level 1 did not differ significantly between groups, but some ZIKV-exposed infants had much higher times to complete level 1. c The groups displayed a similar number of attempts to complete level 1 and 2.
Infant fine motor skills and sensory responsiveness were assessed in dam-reared infants using the PVC Pipe Test that included manipulating a PVC pipe that was filled with raisins and frosting. The ZIKV-exposed infants did not differ in the percentage of time that they orally explored the materials or manipulated the frosting with their fingers. In addition, they did not differ on whether they were isolating their fingers to explore the pipe and raisins (Fig. S2 and Table S7).
We also defined infant sensory processing response in dam-reared infants by assessing their approach to three sensory stimuli (1. feather, 2. cotton ball, 3. brush) in the same order over three consecutive days of testing. The duration of time that it took each infant to approach the sensory stimuli was categorized into no approach, >2 min, 1–2 min, or <1 min. On the first day of testing, most of the ZIKV-exposed infants approached the sensory stimuli, whereas only about half of the control infants approached each stimulus (brush 88% vs. 50%, p = 0.0374; cotton ball 92% vs. 38%, p = 0.0035; feather 88% vs. 38%, p = 0.0085; Fisher’s exact test). Of the ZIKV-exposed infants that approached the stimulus on day 1, most approached quickly within 1 min, with fewer infants taking 1–2 or >2 min to approach (Fig. 5a). After becoming familiarized with the stimuli on days 2 and 3 of testing, ZIKV-exposed infants had an approach pattern that became more similar to the control infants, with most approaching the stimuli quickly. To explore possible contributions of maternal viral and antibody variables to the abnormal day 1 approach phenotype for ZIKV-exposed infants, we selected the feather stimulus as the representative variable because it was most different from all normal stimuli in the enclosure. The proportion of infants that approached the feather stimuli differed by inoculation group, with 100% of DENV/ZIKV and ZIKV-DAK infants approaching the stimuli, compared to between 75–90% of ZIKV-PR 45gd and ZIKV-PR 30gd approaching the stimuli (Fig. 5b). The percent of control infants that approached the feather stimulus was <50%. Maternal viremia duration, area under the viral load curve, percentage of maternal-fetal interface biopsies positive for vRNA, and PRNT90 titer were not significantly different between ZIKV-exposed infants that did and did not approach the feather on day 1 (Fig. 5c–f). Altogether, this indicates that ZIKV-exposed infants initially had decreased inhibition when approaching sensory stimuli in their enclosure.

Infant macaques were exposed to sensory stimuli for 3 consecutive days and their time to approach time was measured (ZIKV n = 28, control n = 8). a More ZIKV-exposed infants approached the three sensory stimuli on day 1 compared to control infants (brush 88% vs. 50%, p = 0.0374, OR = 7.10, 95% CI [1.22, 48.05]; cotton ball 92% vs. 38%, p = 0.0035, OR = 17.25, 95% CI [2.62, 152.61]; feather 88% vs. 38%, p = 0.0085, OR = 11.41, 95% CI [1.97, 82.89]; two-sided Fisher's exact test), and these differences resolved by day 2 (feather p = 0.1648, cotton ball p = 0.3551, brush p = 0.1949) and 3 (all stimuli p = 1.0). Stimuli were presented in the same order each day (feather, cotton ball, brush) for 5 min, and their approach time was reported as no approach, >2 min to approach, 1–2 min to approach, and <1 min to approach. The approach to feather on day 1 was selected as a representative sensory stimulus for day 1 and used in (b–f), to show how the binary response of approach or no approach did not differ based on inoculation group (b), plasma viremia duration (c), area under the curve plasma viral load (d), maternal-fetal interface biopsies that were vRNA positive (e) and PRNT90 titer (f). Complete statistical comparisons are provided in Table S7.
Infant vision and hearing development
In a prior study using this macaque model of ZIKV infection, we identified structural ocular abnormalities in a ZIKV-exposed fetus45. In the present cohort of prenatally ZIKV-exposed infants, we did not observe structural eye abnormalities classically associated with congenital ZIKV infection during ophthalmic examinations. However, we identified two ocular findings not previously reported in human infants with congenital ZIKV infection—iris nodules and persistent fetal vasculature (Fig. S3 and Table S8). These findings may be incidental and are not expected to impact visual function. Retinal structure was assessed by measuring layer thickness using spectral-domain optical coherence tomography. Total retinal layer thickness at the center of the fovea did not differ between ZIKV-exposed and control infants. Of the eight retinal layers measured, only the outer plexiform layer showed a small, non-significant difference (Fig. S4 and Table S9). Together, these findings indicate that these prenatally ZIKV-exposed infants did not have structural ocular abnormalities detectable by ophthalmic examination or optical coherence tomography.
We evaluated retinal and cortical visual function using visual electrophysiology studies. Retinal function was assessed by electroretinography (ERG), and cortical visual pathway function was assessed by visual evoked potentials (VEPs). Retinal visual function, as measured by ERG, was comparable between ZIKV-exposed and control infants at both 3 and 12 months of age (Fig. 6). In contrast, VEP responses in ZIKV-exposed infants differed significantly from controls. At 3 months of age, ZIKV-exposed infants exhibited significantly lower VEP amplitudes, as measured by the root mean square amplitude across left and right lateralities (Fig. 6). These differences resolved by 12 months of age, with VEP amplitudes no longer significantly different from controls (Fig. 6), suggesting delayed maturation of the cortical visual pathway in ZIKV-exposed infants. No significant associations were identified between 3-month VEP amplitudes and maternal viro-immunologic parameters, including viremia duration, area under the viral load curve, percentage of maternal-fetal interface biopsies positive for vRNA, or PRNT90 titer (Fig. S5).

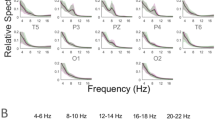
a Light-Adapted Electroretinogram (LA ERG) at 3 months. Waveforms shown are group averages (±SEM) of the left eye ERG recorded from a corneal electrode to monocularly-delivered 2.5 cd s m−2 white flashes on a 30 cd m−2 background following 10 min of light adaptation. b Flash visual evoked potential (FVEP) group averages (±SEM) at 3 months. FVEPs were recorded concurrently with the LA ERG. Waveforms shown are group averages of combined right and left occipital FVEPs following left eye stimulation. LA ERG and FVEP waveforms elicited by right eye stimulation are not shown as they were indistinguishable from those of the left eye. c Root mean square (RMS) amplitudes of the FVEP from left and right occipital sites. RMS amplitudes differed between groups at 3 months of age (Wilcoxon rank-sum test, p = 0.0023). d LA ERG group average waveforms (±SEM) at 12 months. e FVEP group average (±SEM) waveforms at 12 months. f FVEP RMS amplitudes for ZIKV-exposed became statistically indistinguishable from controls at 12 months (p = 0.52).
We observed a higher rate of hearing loss in ZIKV-exposed infants compared to control infants at 12 months of age, although this difference did not reach statistical significance. At 12 months, 5 of 29 (17.2%) ZIKV-exposed infants and 1 of 12 (8.3%) control infants demonstrated hearing loss (Fig. S6). Hearing loss was identified in the ZIKV-PR 45gd, ZIKV-PR 30gd, and DENV/ZIKV groups, but not in the ZIKV-DAK group, possibly due to the smaller sample size. Hearing loss was frequency specific, occurring with either the low pitch (i.e., low-frequency 500 Hz) or mid pitch (i.e., mid-frequency 1000 Hz) tone bursts, but not with the click stimulus, which assesses a broader frequency spectrum (Table S10). Auditory brainstem responses were absent at the lowest volume assessed (40 decibels) and not the higher volumes, suggesting mild to moderate loss. To evaluate whether the hearing loss were persistent, suggesting early-onset sensorineural hearing loss rather than transient conductive or late-onset sensorineural loss, we examined auditory brainstem responses at earlier time points for infants with hearing loss at 12 months. None of these affected infants had hearing loss immediately preceding evaluation; however, some had losses detected at earlier ages, precluding clear differentiation between transient conductive loss and late-onset sensorineural hearing loss (Table S10).
Maternal predictors and potential mediators of ZIKV-associated developmental deficits
To determine whether sensory impairments serve as mechanistic pathways through which ZIKV exposure affects neurodevelopmental outcomes, we conducted mediation analyses rather than standard regression. While regression can identify associations, mediation analysis allows us to formally test whether the effect of ZIKV exposure operates through (is mediated by) sensory deficits, or whether ZIKV has direct effects on behavior independent of sensory pathways. This distinction is critical for understanding biological mechanisms and identifying potential intervention targets. We assessed whether maternal infection characteristics—ZIKV exposure status, duration of plasma viremia, or neutralizing antibody titer—predicted two behavioral outcomes: mutual ventral contact duration and approach behavior to a novel stimulus. We selected two candidate mediators based on domains with significant group differences: visual function (visual evoked potential amplitude at 3 months) and hearing (hearing loss at 12 months). Because we have a relatively small sample size for this type of analysis, we used a p value of 0.1 to define significance. We could not evaluate the impact of ZIKV inoculation groups on the mediators and outcomes because of the much smaller sample size within each inoculation group. Given the exploratory nature of these analyses, we present the conceptual framework and key results in Fig. 7, with complete statistical details provided in Table S11.

a Conceptual framework testing whether prenatal ZIKV exposure affects behavioral outcomes (ventral contact duration and approach to novel stimuli) through sensory impairments (visual evoked potential deficits at 3 months, hearing loss at 12 months) or through direct brain effects. b Results showing ZIKV exposure significantly predicted visual evoked potential deficits (p = 0.020) but not hearing loss (p = 0.475). Neither visual nor auditory impairments predicted behavioral outcomes (all p > 0.1), while ZIKV exposure had significant direct effects on both outcomes (p = 0.012 and p = 0.003). Sobel tests confirmed no significant mediation through sensory pathways (p = 0.56, p = 0.86). Red solid lines, significant relationships (p < 0.05); gray lines, non-significant relationships; red dashed lines, significant direct effects. Light cyan, predictor; light blue, mediators; golden yellow, outcomes. See Table S11 for complete statistics.
ZIKV exposure significantly predicted both behavioral outcomes (Fig. 7 and Table S11). Although ZIKV exposure also predicted visual evoked potential deficits (p = 0.020), these visual deficits did not predict behavioral outcomes (p > 0.1 for both outcomes). ZIKV exposure did not predict hearing loss (p = 0.475), and hearing loss did not predict behavioral outcomes (p > 0.1 for both outcomes). Formal mediation analyses (Sobel test) confirmed no statistically significant indirect effects of ZIKV exposure on behavior through either visual (p = 0.56, p = 0.86) or auditory pathways. These findings indicate that ZIKV exposure affects social-emotional development and sensory approach behavior through direct brain pathways rather than through sensory impairments. We next tested whether two maternal infection characteristics—plasma viremia duration and neutralizing antibody titer—predicted behavioral outcomes through sensory pathways. We focused on these clinically feasible variables rather than AUC plasma viral loads or vRNA distribution within the maternal-fetal. Longer maternal viremia duration showed a trend toward increased ventral contact duration (p = 0.093) but was not associated with approach behavior (p = 0.367) (Table S11). Neutralizing antibody titers were not significantly associated with either behavioral outcome (Table S11). Neither visual function nor hearing status met criteria for statistically significant mediation between maternal infection characteristics and behavioral outcomes (Sobel tests p > 0.4). These results indicated that while prolonged maternal viremia may be linked to certain developmental deficits, the effect does not operate through visual or auditory impairments as intermediary mechanisms.
Discussion
We aimed to define how maternal ZIKV inoculation, viremia, and antibody responses influence infant developmental trajectories. Prenatal ZIKV exposure—regardless of maternal inoculation group—increased the risk of developmental deficits, delayed maturation of the cortical visual pathway, and hearing loss. At 12 months of age, ZIKV-exposed infant macaques exhibited abnormal development across multiple domains, including social-emotional delays and reduced inhibition to sensory stimuli, compared to procedure-matched controls. This constellation of findings mirrors the mild-to-moderate neurodevelopmental impairments most commonly reported in children with prenatal ZIKV exposure3,4,5,6,7,8. Importantly, these impairments were attributable to ZIKV exposure itself and were not mediated by maternal virologic or immunologic status, viral lineage, gestational timing of infection, or prior DENV immunity. Mediation analyses further supported a direct effect of ZIKV exposure on neurodevelopment, particularly in social attachment behaviors, independent of changes in visual or auditory function. These findings demonstrate that even in the absence of overt congenital anomalies, prenatal ZIKV exposure can disrupt early neurobehavioral development. They underscore the need for risk assessment protocols that account for subclinical outcomes and support early developmental screening and longitudinal neurodevelopmental monitoring in exposed infants.
At 12 months of age, ZIKV-exposed infant macaques exhibited significant differences in social-emotional behavior, while their cognitive, fine motor, and gross motor development remained comparable to controls. ZIKV-exposed infants spent more time in mutual ventral contact, close proximity, and nipple contact with their mothers—behaviors that typically decline as infants transition toward greater independence and peer-group engagement by the end of the first year of life46,47,48. This increased maternal attachment may reflect underlying disruptions in threat perception or self-regulation such that ZIKV-exposed infants rely more heavily on maternal social buffering49. This reliance could interfere with the normative transition toward independent regulation of stress and emotional reactivity, thereby constraining the development of typical peer-directed social behaviors. Notably, the increased duration of nipple contact may also contribute to the accelerated growth trajectory observed in ZIKV-exposed infants. Similar mother-infant interactions have previously been characterized in a macaque model of prenatal ZIKV infection at 1 month of age50, and we have now shown that this alteration still exists at 12 months of age. Our observation that prenatal ZIKV exposure is associated with prolonged mother-infant contact is particularly significant because, under typical conditions, rhesus macaque infants spend the majority of their early life in close physical proximity to their mothers, most often positioned ventrally against the mother’s chest in ventro-ventral contact, which is the primary mode of maternal-infant interaction and is critical for infant development and social bonding46,51,52. Additionally, emotional reactivity is disrupted in infant macaques infected postnatally with ZIKV53, suggesting that social-emotional alterations may be a shared outcome of both prenatal and postnatal ZIKV exposure. The amygdala may influence mother–infant interactions, as infant macaques with amygdala lesions show altered socioemotional behaviors54 and ZIKV-infected infant rhesus macaques exhibit smaller amygdala volumes with weaker connectivity compared to controls53,55. Together, these findings indicate that prenatal ZIKV exposure social-emotional development, increasing maternal dependence and potentially hindering peer engagement. Future studies should define how social-emotional outcomes evolve in early childhood and the contribution of amygdala structure and connectivity.
ZIKV-exposed infants also demonstrated a lack of inhibition, characterized by an accelerated approach to sensory stimuli introduced into their environment. This pattern may reflect inappropriate approach behaviors or impaired sensory processing and integration, leading to deficits in novelty detection or threat assessment. Similar exaggerated or unmodulated responses to environmental stimuli have been reported in macaques exposed to prenatal stress56, prenatal lead57, and maternal ZIKV infection58. These neurobehavioral features may serve as early indicators of neurodevelopmental risk for later-emerging deficits in social behavior, anxiety regulation, or cognitive flexibility59. A lack of inhibition may also suggest delayed or atypical emotional learning, resulting in diminished caution or blunted responsiveness to adverse cues. Collectively, these findings implicate potential disruption of brain regions critical to inhibitory control and emotional regulation—particularly the amygdala, hippocampus, rhinal cortex, and orbital frontal cortex—in the emergence of disinhibited behavior and reduced aversion to novelty following early brain injury60,61,62,63,64,65. Neonatal lesion studies in rhesus macaques demonstrate that damage to these regions impairs behavioral inhibition and emotional reactivity, resulting in persistent alterations in approach–avoidance behavior and novelty detection60,61,62,63,64,65. They further raise the possibility that behavioral phenotypes observed in ZIKV-exposed children—such as altered attachment or sensory processing disorders—may have neurobiological origins detectable in early infancy.
Human studies have shown that prolonged maternal viremia (>30 days) is associated with increased risk of fetal loss and structural brain abnormalities24, while higher maternal neutralizing antibody titers two months post-infection are linked to reduced risk of microcephaly and structural brain abnormalities28. In our macaque cohort, consistent with prior studies [reviewed in ref. 20], we did not observe microcephaly, limiting our ability to assess whether maternal viral or immunologic parameters are associated with these more severe outcomes, which represent the most severe end of the congenital ZIKV infection spectrum. Notably, we found that prenatal ZIKV exposure increased the risk of developmental deficits and cortical visual pathway delays regardless of maternal viremia duration or antibody responses. This challenges the prevailing assumption that longer maternal viremia necessarily leads to worse neurodevelopmental outcomes. Despite a wide range of viremia durations (2–70 days) in our cohort, no association was observed between viremia length and infant outcomes. These findings highlight the need for prospective human studies to determine whether longer maternal viremia is indeed predictive of later developmental deficits and, in turn, whether antiviral treatment can improve long-term neurodevelopment. Ultimately, prevention strategies—such as immunization or mosquito control—may prove more effective for improving outcomes than treatment after infection.
ZIKV-exposed infants in this study exhibited a higher weight gain trajectory from birth to 12 months and higher weight at 12 months compared to controls, despite no difference in birth weight. This finding differs from human congenital Zika virus infection, where growth impairment is primarily observed in children with congenital Zika syndrome or microcephaly, not in those without microcephaly. Most non-microcephalic Zika-exposed children maintain normal body mass index and weight-for-age, although a minority may show low growth velocity or subtle differences in body composition66,67. In another rhesus macaque model, prenatally Zika virus-exposed infants had lower weights than controls at birth, with male Zika-exposed infants gaining less weight and female Zika-exposed infants gaining more weight across the first month of life compared to their respective controls50. The differences between our study results and the other infant macaque study may stem from distinct measurement timepoints and the analysis of sex-specific differences. The present study did not compare weight gain by sex, as all control infants were female by random chance. Future studies are needed to determine whether the higher weight gain trajectory persists in these ZIKV-exposed infants and to assess the impact of housing separate from the mother on weight gain.
ZIKV-exposed infants in our study showed delayed maturation of the cortical visual pathway despite normal ocular structure and retinal signaling. While retinal abnormalities are a hallmark of congenital Zika syndrome, less is known about visual function in infants without structural eye defects. We found significantly reduced visual evoked potential (VEP) amplitudes in ZIKV-exposed infants, suggesting dysfunction in the post-retinal visual pathway to the occipital cortex. In contrast, electroretinography and retinal imaging were largely normal, and rare findings such as iris nodules and persistent fetal vasculature were unlikely to affect vision. Similar patterns have been observed in children with congenital ZIKV infection, where VEP abnormalities occur despite normal ophthalmic exams68, or alongside retinal changes with primarily latency shifts69. Cortical visual impairment, a leading cause of childhood visual dysfunction, can affect acuity and higher-order processes such as motion perception and face recognition70. Although early cortical visual deficits were detected at 3 months in our cohort, they resolved by 12 months, and we found no association between early visual function and later developmental outcomes. Ongoing analyses will examine how changes in cortical visual function across the first year of life relate to neurodevelopmental trajectories from birth to 12 months. These findings underscore the importance of comprehensive visual assessments in ZIKV-exposed children, even in the absence of structural abnormalities, and point to the need for further study of subtle or transient cortical visual impairments.
This study has several important limitations. First, although the sample size is large for a nonhuman primate model, it may have limited our power to detect subtle group differences or mediation effects, particularly for binary outcomes such as hearing loss. This is especially relevant given that approximately 30% of infants are expected to exhibit neurodevelopmental deficits, consistent with rates reported in human cohorts3,4. The limited sample size within each inoculation group also precluded mediation analyses examining how factors such as timing of maternal ZIKV exposure, prior DENV immunity, or viral lineage influence developmental outcomes through intermediate variables. We were unable to assess the role of sex differences in developmental outcomes, as all control infants were female by chance. Behavioral differences between biological dam– and surrogate dam–reared infants were not assessed, as further stratification would have limited our already small sample size. Second, although we evaluated a broad range of developmental domains, some behavioral or cognitive impairments may emerge later in life and would not have been detected at the 12-month time point. Despite these limitations, this remains the largest study of nonhuman primate development following prenatal ZIKV exposure20, and the only one to date to examine associations between maternal virologic and immunologic characteristics and infant developmental outcomes.
In summary, our findings demonstrate that prenatal ZIKV exposure results in measurable neurodevelopmental deficits—including altered social-emotional behavior, sensory processing abnormalities, hearing loss, and delayed cortical visual pathway maturation—even in the absence of structural birth defects. These outcomes were not predicted by maternal viremia duration, antibody titers, ZIKV lineage, or DENV immunity, challenging the assumption that maternal virologic or immunologic features alone can accurately stratify fetal risk. This highlights a critical limitation in current maternal-centric approaches to evaluating the effectiveness of prenatal interventions. Infant-focused outcome measures—particularly neurodevelopmental endpoints—must be incorporated into the design and evaluation of maternal treatment trials to capture the full spectrum of congenital ZIKV impact. The combination of behavioral, electrophysiologic, and structural assessments used in this translational model provides a framework for identifying early markers of atypical development and evaluating the downstream effects of maternal therapies. These findings also support the need to include all ZIKV-exposed infants—regardless of symptom status at birth—in pediatric developmental screening and follow-up, to enable early identification of delays and timely intervention during critical periods of early childhood development.
Methods
Study design, inoculation, and monitoring
Indian-origin rhesus macaques (Macaca mulatta) were inoculated with ZIKV or phosphate-buffered saline (PBS) during the first trimester, either early in the first trimester around 30 gestational days (gd) or closer to the second trimester around 45gd. All dams were housed at the Wisconsin National Primate Research Center (WNPRC) and were free of Macacine herpesvirus 1 (Herpes B virus), simian retrovirus type D (SRV), simian T-lymphotropic virus type 1 (STLV), and simian immunodeficiency virus (SIV). To generate pre-existing immunity to DENV, eight macaques were inoculated with 1 × 104 plaque forming units (PFU) DENV-2/US/BID-V594/2006 37–68 days prior to breeding, as previously described71. Macaques were bred, and once pregnant, were inoculated subcutaneously over the cranial dorsum with PBS, or 1 × 104 PFU Zika virus/H.sapiens-tc/PUR/2015/PRVABC59_v3c2 (PRVABC59, GenBank: KU501215), or 1 × 108 PFU Zika virus/A.africanus-tc/Senegal/1984/DAKAR 41524 (ZIKV-DAK; GenBank: KX601166) (Table S11). Preparation of the ZIKV-PR23 and ZIKV-DAK42 virus stocks have been described previously. The pregnancies of the seven DENV/ZIKV and four ZIKV-DAK pregnancies have been described earlier43,71. Post-inoculation, the animals were closely monitored by veterinary and animal care staff for adverse reactions or any signs of disease. Blood was drawn for ZIKV RT-qPCR (or neutralizing antibody titers) daily for 10 days following inoculation during pregnancy, then twice weekly until viremia cleared, then weekly until Cesarean delivery. Amniotic fluid vRNA loads were not measured during pregnancy until the time of delivery because of concern for adverse outcomes that could compromise fetal health45. Infants had blood drawn for ZIKV RT-qPCR immediately after delivery, or within the first week of life, if the infant was born naturally, and with other sedated exams (overview in Fig. 8; details in Table S12).

a Pregnant macaques were inoculated with ZIKV-PR, ZIKV-DAK or PBS at approximately 30 or 45 gestational days. Some females had a history of DENV infection 1–2 months prior to pregnancy. Specific inoculation virus and timeline are described in Table S12. Inoculation group colors are consistent throughout the manuscript. b After delivery, infants underwent a battery of tests, including ZIKV plasma viral loads, IgM testing, hearing tests, ocular exams, developmental testing and mother-infant observations at the time points indicated. Created in BioRender. Mohr, E. (2025) https://BioRender.com/i5ohpzl.
Cesarean delivery
Infants were delivered by Cesarean at approximately 160 gestational days (gd) (±5 days) (full details in Table S13), about 8 days earlier than the average gestational age of a natural birth72 to ensure that the placenta could be collected for virologic and histologic evaluation. Full thickness sections of each cotyledon in each placental disc were collected for vRNA isolation from the villous parenchyma, decidua basalis, and chorionic membranes. Amniotic fluid was collected immediately prior to infant delivery using a syringe and needle inserted through the fetal membranes. Three infants were delivered through spontaneous parturition (044-108, 044-109, 044-531) prior to their scheduled Cesarean section; placental tissues could not be collected from 044-109.
Ethics and study approval
All rhesus macaques are cared for by the staff at the WNPRC in accordance with the regulations and guidelines outlined in the Animal Welfare Act and the Guide for the Care and Use of Laboratory Animals, the recommendations of the Weatherall report73, and the principles described in the National Research Council’s Guide for the Care and Use of Laboratory Animals74. The University of Wisconsin-Madison Institutional Animal Care and Use Committee approved the nonhuman primate research covered under protocol numbers G006290 and G006108. The University of Wisconsin–Madison Institutional Biosafety Committee approved this work under protocol number B00000764.
Care & use of macaques
All animals were housed in enclosures with required floor space and fed using a nutritional plan based on recommendations published by the National Research Council74. Dams were fed a fixed formula, extruded dry diet with adequate carbohydrate, energy, fat, fiber, mineral, protein, and vitamin content. Macaque dry diets were supplemented with fruits, vegetables, and other edible objects (e.g., nuts, cereals, seed mixtures, yogurt, peanut butter, popcorn, marshmallows, etc.) to provide variety to the diet and to inspire species-specific behaviors such as foraging. When needed, infants were fed 5% dextrose for the first 24 h of life and liquid formula subsequently. To further promote psychological well-being, animals were provided with food enrichment, structural enrichment, and/or manipulanda. Environmental enrichment objects were selected to minimize chances of pathogen transmission from one animal to another and from animals to care staff. While on study, all animals were evaluated by trained animal care technicians at least twice each day for signs of pain, distress, and illness by observing appetite, stool quality, activity level, and physical condition. Animals exhibiting abnormal presentation for any of these clinical parameters were provided appropriate care by attending veterinarians. Prior to all minor/brief experimental procedures, macaques were sedated using ketamine anesthesia and monitored regularly until fully recovered from anesthesia.
For breeding, the female macaques were co-housed with a compatible male and observed daily for menses and breeding. Pregnancy was detected by ultrasound examination of the uterus at approximately 20–24 gestation days (gd) following the predicted day of ovulation. The gd was estimated (±2 days) based on the dam’s menstrual cycle, observation of copulation, and the greatest length of the fetus at initial ultrasound examination which was compared to normative growth data in this species75. For physical examinations, virus inoculations, ultrasound examinations, blood or swab collections, the dam was anesthetized with an intramuscular dose of ketamine (10 mg/kg). Blood samples from the femoral or saphenous vein were obtained using a vacutainer system or needle and syringe. Pregnant macaques were monitored daily prior to and after viral inoculation for any clinical signs of infection (e.g., diarrhea, inappetence, inactivity, fever and/or atypical behaviors).
vRNA isolation from blood and tissues and RT-qPCR
RNA was extracted from 300 µL of plasma using the Viral Total Nucleic Acid Purification kit (Promega, Madison, WI, USA) on a Maxwell 48 RSC instrument. RT-qPCR was performed as previously described76 using the primers and probe designed by Lanciotti et al.77. Fetal and maternal–fetal interface tissues (placenta, decidua, umbilical cord, chorionic plate, fetal membranes) were preserved with RNAlater® (Invitrogen, Carlsbad, CA, USA) at 4 °C for 24–72 h before the RNAlater was removed and the tissue was frozen at −80 °C. RNA was isolated from maternal and fetal tissues using a method described by Hansen et al.78 and previously described in detail22. The RT-qPCR limits of detection are 150 copies/mL from plasma and estimated to be 3 copies/mg from tissue. The duration of maternal plasma viremia was defined as the last RNA viral load equal to or greater than the RT-qPCR limit of detection of 150 copies/mL. The distribution of vRNA within the maternal-fetal interface was defined as the fraction of ZIKV vRNA-positive biopsies divided by the number of biopsies assessed for viral loads within the placenta, decidua and chorionic plate.
Plaque reduction neutralization test (PRNT)
Neutralizing antibody titers were measured in serum samples 1 month post-infection (range 24–38 days) using a plaque reduction neutralization test using a 90% cutoff (PRNT90). Endpoint titrations of reactive sera were performed against ZIKV-PR for dams inoculated with ZIKV-PR (ZIKV-PR 30gd, ZIKV-PR 45 gd, DENV/ZIKV), or against ZIKV-DAK for dams inoculated with ZIKV-DAK, as previously described44,71,79. These data were previously published for the ZIKV-PR 30gd and 45gd dams79, for the DENV/ZIKV dams71, and for the ZIKV-DAK dams44.
ZIKV IgM assay
Infant serum was tested for ZIKV-specific IgM antibodies using a commercial assay (Euroimmune, Germany, catalog #EI 2668-9601 M).
Infant care
After delivery, infants were dried, stimulated, and received respiratory support as clinically indicated. Birth weight was measured shortly after delivery. Infants were returned to their biological dam following her recovery from anesthesia. If the dam rejected the infant after multiple reintroduction attempts over the subsequent 2–3 days, the infant was placed with a surrogate dam from the colony when available or transferred to the nursery if no surrogate was available. Upon reaching 1 month of age, infants (n = 6) initially raised in the nursery were placed in an age-matched peer group and remained with this peer group until 12 months of age. Infants in peer-raised groups were not included in behavioral analysis. Infants (n = 35) initially placed with a dam remained with the same dam until 12 months of age. Infant weights were measured when dam and infant were separated for any reason. Head circumference was measured at each infant assessment using a head circumference tape measure. When multiple measurements (up to three) were obtained, the median value was recorded.
Mother-infant home enclosure observations
Mother-infant dyad behavior was assessed using a 25 to 30-min home-enclosure video recording at 12 months of age to evaluate the infant’s social-emotional, motor, feeding, self-care, and exploratory behaviors in a familiar environment. An observer known to the animals was present when recording the dyad to adjust the camera as needed. Behaviors were analyzed for two consistent time segments of 5 min each from near the beginning and end of the observation to capture the range of behaviors. Infants in peer groups were not included in this assessment as mother-infant dyad interactions could not be measured; this resulted in the exclusion of three ZIKV-exposed and three control infants. Mutual ventral contact, nipple contact, proximity to mother (together), and infant locomotion were coded (Table S13). Behaviors were not mutually exclusive and could be coded simultaneously as appropriate.
Puzzle feeder
Infants’ fine motor, visual motor, and cognitive skills were assessed through the macaques’ manipulation of a treat through a 9-level puzzle in their home enclosure at 12 months of age. The puzzle feeder, a clear Plexiglas puzzle that has 9 levels of increasing complexity, was attached to the side or front of the home enclosure (Fig. S7). A food treat was placed in the top compartment and the infant must move the treat laterally through multiple paths to reach the bottom of the puzzle feeder, where the treat can be removed from a larger opening in the feeder. Two puzzle feeders were attached to opposite sides of the enclosure, so that the mother and infant could be engaged in separate puzzle feeders simultaneously. The infant’s interaction with the puzzle feeder was recorded by a tester familiar to the dyad using two stationary cameras, each providing a full view of one of two puzzle feeders attached to the sides of the dyad’s home enclosure. The mother and infant had 30 min to engage in the task. Both puzzle feeders were set at the easiest level first and then advanced to more difficult levels as the previous level was successfully completed. Completion of levels, individual attempts, digit isolation, and motor coordination were coded (Table S14).
Fine motor PVC pipe test
Infants were observed in their home enclosure to define fine motor skills and sensory differences using a 10 min PVC pipe enrichment test at 12 months of age. The observation was recorded by a familiar tester, using both a handheld camera and a stationary camera. Three PVC pipes, approximately 0.5 inches in diameter and 4 inches in length, were prepared by filling both ends with frosting and layering in three raisins at each end to provoke the use of fine motor movements. One PVC was completely inserted into the enclosure to engage the mother while the second PVC was inserted into the enclosure frame, stabilized between the bars to more easily capture infant interactions. If the mother monopolized both PVCs, a third PVC was held next to the enclosure frame by the tester to capture infant interactions. The assessment was recorded for 10 min on three sequential days; the first day of testing was considered acclimation to task and wasn’t analyzed except to substitute for missing data on a subsequent test day for (n = 2, 1 ZIKV, 1 control) infants. Oral exploration, frosting exploration, and digit isolation were coded (Table S14). All pipes remained in the enclosure a minimum of 98% of the time during the task.
Sensory processing measure for monkeys
Infant responses to sensory materials were assessed in their home enclosure environment at 12 months of age using the Sensory Processing Measure for Monkeys56. Three sensory stimuli, feathers (black colored), cotton balls, or a brush, were attached to a metal rod and presented sequentially in the enclosure independently and in the same order each time, for a duration of five minutes per stimulus for a total of 15 min. Exposure to sensory stimuli was shortened if the infant or dam demonstrated excessive aggression towards stimuli such as destroying or eating materials. Infant approach, time to approach, and method of approach (visual or touch) were coded (Table S14).
Coding reliability and software
A video coding software program, Noldus Observer XT 14.0 was used to code infant behaviors for the mother-infant dyad interactions and Fine Motor PVC Pipe test. Qualtrics (Qualtrics, Provo, UT) was used to capture the coding for the Puzzle Feeder and Sensory Response tests. All videos for all behavior protocols were coded by two individuals and an inter-rater reliability of Cohen’s kappa = 0.9 was used. Any behaviors with a kappa below 0.9 were reviewed by the specific coding team until consensus was reached. All coders were blinded to the infant’s group.
Auditory brainstem response testing
Hearing, or auditory brainstem function, was assessed with auditory brainstem response audiometry, which measures brainstem evoked potentials generated by a brief click, as previously described. Examinations were performed by a human audiologist with pediatric training (A. Hartman) who was blinded to the infant’s inoculation group. Auditory brainstem response (ABR) thresholds were obtained for auditory (click) stimuli and tone bursts (500 and 1000 Hz), as described in ref. 80, using the Biologic Navigator Pro system. Ambient noise level was minimized. Needle electrodes were placed at the brow ridge (positive input) and behind the right pinna (negative input) for channel 1 and from the brow ridge (positive input) and behind the left pinna (negative input) for channel 2. An electrode was placed below the brow ridge on the forehead for the ground. Electrode impedances were below 10 kohm for all electrodes. Physiological filters were set to pass 100–3000 Hz. The stimuli were clicks with rarefaction, condensation, and alternating polarities and tone bursts with alternating polarity gated with a Blackman window with 2 ms rise-fall and 1 ms plateau times. Insert earphones (Etymotic ER-3A) were used for testing. Signal levels for click stimuli were presented at 70, 50, 30, and 20 dB nHL and wave IV was observed at each presentation level. Signal levels for tone burst stimuli were presented at 80, 60, and 40 dB nHL and wave IV was observed at each presentation level. Each response was recorded twice for reliability, with the noise floor being less than 10% of sweeps. To distinguish sensorineural hearing loss, which is typically persistent, from conductive hearing loss, which is often transient, infants with absent wave IV responses to one or more stimuli at 12 months of age were identified. Longitudinal wave IV responses from 1 to 12 months were then reviewed for these infants to assess for persistent patterns of hearing deficits.
Ophthalmic exam
Ophthalmic exams were performed by a human ophthalmologist with retinal fellowship training (M. Nork) who was blinded to the infant’s inoculation group. Slit-lamp biomicroscopy and indirect ophthalmoscopy were performed after pupillary dilation.
Optical coherence tomography
Spectral-domain optical coherence tomography is a noninvasive imaging method that uses reflected light to create images of the retinal layers. High resolution scans were collected through the center of the fovea and around the optic nerve. Scans of the retina were carried out in both eyes using a Heidelberg™ Spectralis HRA + OCT (Heidelberg™ Engineering, Heidelberg, Germany) instrument. Determination of retinal layer thickness was performed using combined manual and automatic segmentation algorithms from both Heidelberg and EXCELSIOR Preclinical (EdgeSelect™)81. After segmentation, EXCELSIOR Preclinical was used to calculate mean thicknesses for individual retinal layers.
Visual electrophysiology
To objectively evaluate visual function, ocular specialists under the auspices of a clinically trained visual electrophysiologist (J. Ver Hoeve) performed standard visual electrodiagnostic procedures including a full-field electroretinogram and the cortical-derived visual evoked potential82 and were blinded to the infant’s inoculation group. The electroretinogram is used clinically to assess generalized retinal function under light-adapted (focused on cone photoreceptors) conditions82. Visual evoked potentials reflect the function of the entire visual pathway from the retina via the optic nerve to the visual cortex of the brain82. The light-adapted full-field flash electroretinogram, recorded on a rod saturating background, measures the electrical activity generated predominantly by cone photoreceptor and bipolar cells, which are found in high density in the primate macula and are primarily responsible for light-adapted, high acuity and color vision.
Binocular photopic (light-adapted) electroretinography flashes (2.5 cd s m−2 and 30-Hz flicker) followed by monocularly stimulated (right eye, then left eye) visual evoked cortical potentials were recorded and collected. Measurements were recorded using an LKC UTAS visual electrodiagnostic test system configured with the BigShot Ganzfeld stimulator for electroretinogram and visual evoked potentials response collection (LKC Technologies™, Gaithersburg, MD). When isoflurane was used during an earlier procedure in the same sedation event, a washout period was allowed before visual electrophysiology studies to minimize isoflurane suppression of cortical activity83. For the electroretinogram, corneas were anesthetized with topical 0.5% proparacaine prior to application of ERG-Jet™ (Universo™, Switzerland) contact lens electrodes and a conductive wetting solution. Four-channel (channel 1: right eye, channel 2: left eye, channel 3: right occipital cortex, channel 4: left occipital cortex) recordings were carried out with the use of the UBA patient amplifier interfaced to the system computer. The UBA amplifier response was calibrated at the initiation of the study. Reference electrodes were subdermal stainless-steel needle electrodes inserted near the ipsilateral outer canthus of each eye. To measure visual evoked potentials, a light stimulus was applied to either the left or right eyes (the non-tested eye was covered with an opaque occluder), and electrical potentials were recorded near the occipital cortex from two active subdermal electrodes situated approximately 1 cm superior to the occipital ridge and 1 cm lateral to the midline; reference electrodes were situated along the midline at the vertex. ERG-Jet™ and subdermal needle electrode impedances were <5 kΩ (Grass Electrode Impedance Meter Model F-EZM5, Astro-Med, Inc., Grass Instrument Division, West Warwick, RI) and equivalent. The band pass for electroretinogram signals was 0.3 Hz (high pass) and 500 Hz (low pass) and the band pass for visual evoked potentials was 1 Hz (high pass) and 100 Hz (low pass). Each of the two electroretinogram flash stimulations were repeated for replicability. Replicates (2–4) of 80 flash stimulations each were performed on each macaque for visual evoked potentials. Response waveforms were digitized at 0.5 ms intervals. All response waveforms were processed off-line. The root mean square of the visual evoked potential amplitude from 50–200 ms post flash was machine-scored using software written in MATLAB™ (Natick, MA).
Statistical analyses
All frequentist inferential statistics are reported with test statistics, degrees of freedom (where applicable), p values, effect sizes, and 95% confidence intervals in the Supplementary tables.
In order to better understand the infants included in this study, several statistical analyses were performed to obtain the demographic features of exposure groups. Descriptive statistics including means, confidence intervals, and missing data were determined for each exposure group for demographic features measured on a quantitative scale. Categorical features were summarized in terms of frequencies and percentages. Comparisons of demographic features between exposure groups were conducted using a two-sample t-test for quantitative variables and chi-square/Fisher’s exact test for categorical variables. A two-sided 0.05 significance level was used to determine statistical significance for all comparisons.
Developmental outcomes were reported in the form of continuous quantitative data, discrete quantitative data, and ordinal and nominal qualitative data, as ratio/percentage, frequency, or categorical values respectively. Group-level summaries were generated separately for ZIKV-exposed and control animals. Categorical data for the sensory processing task were summarized in terms of frequencies and percentages (n (%)).
For continuous behavioral outcomes measured on a quantitative scale, including puzzle feeder metrics and sensory processing measures as well as all variables for the PVC and home enclosure observation coding schemes, we reported number of observations, medians, and interquartile ranges (IQRs). Comparisons between exposure groups between those outcomes were conducted using analysis of variance (ANOVA), followed by pairwise post hoc comparisons. Distributions of outcome variables and heteroskedasticity between groups was evaluated visually using box and whisker plots. Chi-square or Fisher’s exact test was used to compare binary development outcomes between groups. Statistical inference was conducted using SAS software (SAS Institute, Cary NC), version 9.4.
Linear regression models were used to assess associations between infant weight at 12 months and key maternal or placental virologic parameters, including maternal plasma viremia duration, area under the curve of plasma viral loads, proportion of maternal-fetal interface biopsies positive for viral RNA, and PRNT90 neutralizing antibody titers. Data were analyzed in R (version 4.3.1) using the lm() function. Data visualization was performed using ggplot2 (v3.5.1), ggpubr (v0.6.0), and ggsignif (v0.6.4). Each parameter was evaluated in a separate univariate model with infant weight as the outcome. Prior to modeling, variables were explicitly converted to numeric type, and records with missing values for either the predictor or outcome variable were excluded. Model fit was visualized using ggplot2, with scatter plots displaying individual data points and fitted regression lines. R² and p values were reported for each model to quantify the strength and significance of the associations.
We conducted causal mediation analyses to evaluate whether the relationship between prenatal ZIKV exposure and 12-month behavioral outcomes was mediated by hearing loss or visual pathway function. Behavioral outcomes included ventral contact duration and feather approach behavior, which was assessed both as a 4-level ordinal variable and as a binary outcome (approached vs. did not approach). Predictor variables included plasma viremia duration, maternal PRNT90 neutralizing antibody titer at 1 month, ZIKV inoculation group, and binary exposure classification (ZIKV-exposed vs. control). For each predictor–mediator–outcome combination, we fitted two linear models: a mediator model (mediator ~ predictor) and an outcome model (outcome ~ predictor + mediator). Mediation analysis was performed using the mediate() function from the R mediation package (version 2024.12.0), with 1000 simulations and quasi-Bayesian approximation for inference. All continuous outcomes and mediators were modeled using linear regression. Binary outcomes (feather approach) and binary mediators (hearing loss) were treated as numeric (0/1) and analyzed using linear models given the small sample size and model convergence considerations. Mediation significance was evaluated by examining the average causal mediation effect (ACME), average direct effect (ADE), total effect, and proportion mediated. All analyses were conducted using R version 2024.12.0.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Source data are provided with this paper.
Change history
13 April 2026
A Correction to this paper has been published: https://doi.org/10.1038/s41467-026-72056-w
References
Deshpande, G. R. et al. An outbreak of Zika virus in western India in the metropolis of Pune in the monsoon of 2024. J. Infect. Public Health 18, 102720 (2025).
Pezzi, L. et al. Zika virus infection in a traveller returning to France from Seychelles, 2024. J. Travel Med. https://doi.org/10.1093/jtm/taaf048 (2025).
Mulkey, S. B. et al. Neurodevelopmental abnormalities in children with in utero Zika virus exposure without congenital Zika syndrome. JAMA Pediatr. 174, 269–276 (2020).
Nielsen-Saines, K. et al. Delayed childhood neurodevelopment and neurosensory alterations in the second year of life in a prospective cohort of ZIKV-exposed children. Nat. Med. 25, 1213–1217 (2019).
Peçanha, P. M. et al. Neurodevelopment of children exposed intra-uterus by Zika virus: a case series. PLoS ONE 15, e0229434 (2020).
Vianna, R. A. et al. Children born to mothers with rash during Zika virus epidemic in Brazil: first 18 months of life. J. Trop. Pediatr. 65, 592–602 (2019).
Venancio, F. A. et al. Early and long-term adverse outcomes of in utero Zika exposure. Pediatrics 155, e2024067552 (2025).
Mulkey, S. B. et al. School-age child neurodevelopment following antenatal Zika virus exposure. Pediatr. Res. https://doi.org/10.1038/s41390-025-03981-7 (2025).
Moore, C. A. et al. Characterizing the pattern of anomalies in congenital Zika syndrome for pediatric clinicians. JAMA Pediatr. 171, 288–295 (2017).
Roth, N. M. et al. Zika-associated birth defects reported in pregnancies with laboratory evidence of confirmed or possible Zika virus infection—U.S. Zika Pregnancy and Infant Registry, December 1, 2015-March 31, 2018. Morb. Mortal. Wkly. Rep. 71, 73–79 (2022).
Mahmoud, A., Pomar, L., Lambert, V., Picone, O. & Hcini, N. Prenatal and postnatal ocular abnormalities following congenital Zika virus infections: a systematic review. Ocul. Immunol. Inflamm. 1, 11 (2024).
Almeida, L. C. et al. Hearing and communicative skills in the first years of life in children with congenital Zika syndrome. Braz. J. Otorhinolaryngol. 88, 112–117 (2022).
Barbosa, M. H. et al. Auditory findings associated with Zika virus infection: an integrative review. Braz. J. Otorhinolaryngol. 85, 642–663 (2019).
Veldhorst, C., Vervloed, M., Kef, S. & Steenbergen, B. A scoping review of longitudinal studies of children with vision impairment. Br. J. Vis. Impair. 41, 587–609 (2023).
Lieu, J. E. C., Kenna, M., Anne, S. & Davidson, L. Hearing loss in children: a review. JAMA 324, 2195–2205 (2020).
Mohr, E. L. Modeling Zika virus-associated birth defects in nonhuman primates. J. Pediatric Infect. Dis. Soc. 7, S60–S66 (2018).
Dudley, D. M. et al. Using macaques to address critical questions in Zika virus research. Annu. Rev. Virol. 6, 481–500 (2019).
Narasimhan, H., Chudnovets, A., Burd, I., Pekosz, A. & Klein, S. L. Animal models of congenital zika syndrome provide mechanistic insight into viral pathogenesis during pregnancy. PLoS Negl. Trop. Dis. 14, e0008707 (2020).
Morrison, T. E. & Diamond, M. S. Animal models of Zika virus infection, pathogenesis, and immunity. J. Virol. 91, e00009-17 (2017).
Gutkes, J., Krabbe, N. P., Ausderau, K. & Mohr, E. L. Macaque models of prenatal and postnatal Zika virus exposure and developmental outcomes. J. Pediatric Infect. Dis. Soc. https://doi.org/10.1093/jpids/piaf024 (2025).
Sackett, G. P. Chapter 1—Developmental disabilities and primate models defined. in Primate Models of Children’s Health and Developmental Disabilities (eds Burbacher, T. M., Sackett, G. P. & Grant, K. S.) 1–10 (Academic Press, 2008).
Koenig, M. R. et al. Quantitative definition of neurobehavior, vision, hearing and brain volumes in macaques congenitally exposed to Zika virus. PLoS ONE 15, e0235877 (2020).
Ausderau, K. et al. Neonatal development in prenatally Zika virus-exposed infant macaques with dengue immunity. Viruses 13, 1878 (2021).
Pomar, L. et al. Prolonged maternal Zika viremia as a marker of adverse perinatal outcomes. Emerg. Infect. Dis. 27, 490–498 (2021).
Driggers, R. W. et al. Zika virus infection with prolonged maternal viremia and fetal brain abnormalities. N. Engl. J. Med. 374, 2142–2151 (2016).
Suy, A. et al. Prolonged Zika virus viremia during pregnancy. N. Engl. J. Med. 375, 2611–2613 (2016).
Schwartz, K. L. et al. Zika virus infection in a pregnant Canadian traveler with congenital fetal malformations noted by ultrasonography at 14-weeks gestation. Trop. Dis. Travel Med. Vaccines 4, 2 (2018).
Nielsen-Saines, K. et al. Development of maternal antibodies post ZIKV in pregnancy is associated with lower risk of microcephaly and structural brain abnormalities in exposed infants. J. Infect. Dis. https://doi.org/10.1093/infdis/jiaf146 (2025).
Gordon, A. et al. Prior dengue virus infection and risk of Zika: a pediatric cohort in Nicaragua. PLoS Med. 16, e1002726 (2019).
Bardina, S. V. et al. Enhancement of Zika virus pathogenesis by preexisting antiflavivirus immunity. Science 356, 175–180 (2017).
Langerak, T. et al. Transplacental Zika virus transmission in ex vivo perfused human placentas. PLoS Negl. Trop. Dis. 16, e0010359 (2022).
McCracken, M. K. et al. Impact of prior flavivirus immunity on Zika virus infection in rhesus macaques. PLoS Pathog. 13, e1006487 (2017).
Pantoja, P. et al. Zika virus pathogenesis in rhesus macaques is unaffected by pre-existing immunity to dengue virus. Nat. Commun. 8, 15674 (2017).
Sansone, N. M. S., Boschiero, M. N. & Marson, F. A. L. Dengue outbreaks in Brazil and Latin America: the new and continuing challenges. Int. J. Infect. Dis. 147, 107192 (2024).
Halai, U.-A. et al. Maternal Zika virus disease severity, virus load, prior dengue antibodies, and their relationship to birth outcomes. Clin. Infect. Dis. 65, 877–883 (2017).
Brasil, P. et al. Zika virus infection in pregnant women in Rio de Janeiro. N. Engl. J. Med. 375, 2321–2334 (2016).
Moreira-Soto, A. et al. Exhaustive TORCH pathogen diagnostics corroborate Zika virus etiology of congenital malformations in Northeastern Brazil. mSphere 3, e00278-18 (2018).
Pedroso, C. et al. Cross-protection of dengue virus infection against congenital Zika syndrome, northeastern Brazil. Emerg. Infect. Dis. 25, 1485–1493 (2019).
de Paula Freitas, B. et al. Ocular findings in infants with microcephaly associated with presumed Zika virus congenital infection in Salvador, Brazil. JAMA Ophthalmol. 134, 529–535 (2016).
Pimentel, R. et al. Birth defects and long-term neurodevelopmental abnormalities in infants born during the Zika virus epidemic in the Dominican Republic. Ann. Glob. Health 87, 4 (2021).
Honein, M. A. et al. Birth defects among fetuses and infants of US women with evidence of possible Zika virus infection during pregnancy. JAMA 317, 59–68 (2017).
Jaeger, A. S. et al. Zika viruses of African and Asian lineages cause fetal harm in a mouse model of vertical transmission. PLoS Negl. Trop. Dis. 13, e0007343 (2019).
Crooks, C. M. et al. African-lineage Zika virus replication dynamics and maternal-fetal interface infection in pregnant rhesus macaques. J. Virol. 95, e0222020 (2021).
Raasch, L. E. et al. Fetal loss in pregnant rhesus macaques infected with high-dose African-lineage Zika virus. PLoS Negl. Trop. Dis. 16, e0010623 (2022).
Mohr, E. L. et al. Ocular and uteroplacental pathology in a macaque pregnancy with congenital Zika virus infection. PLoS ONE 13, e0190617 (2018).
Hinde, R. A. & White, L. E. Dynamics of a relationship: rhesus mother-infant ventro-ventral contact. J. Comp. Physiol. Psychol. 86, 8–23 (1974).
Hinde, R. A. & Spencer-Booth, Y. The behaviour of socially living rhesus monkeys in their first two and a half years. Anim. Behav. 15, 169–196 (1967).
Hinde, R., Rowell, T. E. & Spencer-Booth, Y. Behavior socially living rhesus monkey first six months. Proc. Zool. Soc. Lond. 143, 609–649 (1964).
Sanchez, M. M., McCormack, K. M. & Howell, B. R. Social buffering of stress responses in nonhuman primates: maternal regulation of the development of emotional regulatory brain circuits. Soc. Neurosci. 10, 512–526 (2015).
Moadab, G. et al. Prenatal Zika virus infection has sex-specific effects on infant physical development and mother-infant social interactions. Sci. Transl. Med. 15, eadh0043 (2023).
Bliss-Moreau, E., Moadab, G. & Amaral, D. G. Living Without Amygdala 149–185 (The Guilford Press, 2016).
Machado, C. J. Building Babies: Primate Development Proximate Ultimate Perspective, Developments Primatology: Progress Prospects 259–279 (Springer, 2013).
Raper, J. et al. Long-term alterations in brain and behavior after postnatal Zika virus infection in infant macaques. Nat. Commun. 11, 2534 (2020).
Raper, J., Stephens, S. B. Z., Sanchez, M., Bachevalier, J. & Wallen, K. Neonatal amygdala lesions alter mother-infant interactions in rhesus monkeys living in a species-typical social environment. Dev. Psychobiol. 56, 1711–1722 (2014).
Medina, A. et al. Treatment with sofosbuvir attenuates the adverse neurodevelopmental consequences of Zika virus infection in infant rhesus macaques. J. Neuroimmunol. 381, 578148 (2023).
Schneider, M. L. et al. Sensory processing disorder in a primate model: evidence from a longitudinal study of prenatal alcohol and prenatal stress effects. Child Dev. 79, 100–113 (2008).
Moore, C. F. et al. Developmental lead exposure induces tactile defensiveness in rhesus monkeys (Macaca mulatta). Environ. Health Perspect. 116, 1322–1326 (2008).
Cogo, P. R., Moadab, G., Bliss-Moreau, E. & Pittet, F. Prenatal Zika virus exposure alters the interaction between affective processing and decision-making in juvenile rhesus macaques (Macaca mulatta). Dev. Psychobiol. 66, e70002 (2024).
White, L. K., McDermott, J. M., Degnan, K. A., Henderson, H. A. & Fox, N. A. Behavioral inhibition and anxiety: the moderating roles of inhibitory control and attention shifting. J. Abnorm. Child Psychol. 39, 735–747 (2011).
Bliss-Moreau, E., Toscano, J. E., Bauman, M. D., Mason, W. A. & Amaral, D. G. Neonatal amygdala or hippocampus lesions influence responsiveness to objects. Dev. Psychobiol. 52, 487–503 (2010).
Bliss-Moreau, E., Toscano, J. E., Bauman, M. D., Mason, W. A. & Amaral, D. G. Neonatal amygdala lesions alter responsiveness to objects in juvenile macaques. Neuroscience 178, 123–132 (2011).
Meunier, M. & Bachevalier, J. Comparison of emotional responses in monkeys with rhinal cortex or amygdala lesions. Emotion 2, 147–161 (2002).
Meunier, M., Nalwa, V. & Bachevalier, J. Reactions to familiar and novel objects in infant monkeys with neonatal temporal lesions. Hippocampus 13, 489–493 (2003).
Malkova, L., Mishkin, M., Suomi, S. J. & Bachevalier, J. Long-term effects of neonatal medial temporal ablations on socioemotional behavior in monkeys (Macaca mulatta). Behav. Neurosci. 124, 742–760 (2010).
Medina, A., Torres, J., Kazama, A. M., Bachevalier, J. & Raper, J. Emotional responses in monkeys differ depending on the stimulus type, sex, and neonatal amygdala lesion status. Behav. Neurosci. 134, 153–165 (2020).
de Aguiar, E. B. et al. Anthropometric parameters of children with congenital Zika virus exposure in the first three years of life. Viruses 14, 876 (2022).
Peixoto, L. et al. Growth velocity and nutritional status in children exposed to Zika virus during pregnancy from Amazonas Cohort, Brazil. Viruses 15, 662 (2023).
Almeida, L. F. B. et al. Pattern-reversal visual evoked potential in children with congenital Zika syndrome. J. Pediatr. Ophthalmol. Strabismus 58, 78–83 (2021).
García-Boyano, M. et al. Long-term outcomes of infants with congenital Zika virus infection in Ecuador: a retrospective longitudinal study. J. Trop. Pediatr. 67, fmaa066 (2021).
Gordon, S., Kerr, A., Wiggs, C. & Chiang, M. F. What is cerebral/cortical visual impairment and why do we need a new definition? Ophthalmology 131, 1357–1358 (2024).
Crooks, C. M. et al. Previous exposure to dengue virus is associated with increased Zika virus burden at the maternal-fetal interface in rhesus macaques. PLoS Negl. Trop. Dis. 15, e0009641 (2021).
Coe, C. L. & Lubach, G. R. Maternal determinants of gestation length in the rhesus monkey. Trends Dev. Biol. 14, 63–72 (2021).
Weatherall, D. The Use of Non-Human Primates in Research (Academy of Medical Sciences, Medical Research Council, Royal Society, Wellcome Trust, London, 2006).
National Research Council, Division on Earth and Life Studies, Institute for Laboratory Animal Research & Committee on Guidelines for the Use of Animals in Neuroscience and Behavioral Research. Guidelines for the Care and Use of Mammals in Neuroscience and Behavioral Research (National Academies Press, 2003).
Tarantal, A. F. Ultrasound imaging in rhesus (Macaca mulatta) and long-tailed (Macaca fascicularis) macaques: reproductive and research applications. In The Laboratory Primate. (ed. Wolfe-Coote, S.) 317–352 (Elsevier, 2005).
Dudley, D. M. et al. A rhesus macaque model of Asian-lineage Zika virus infection. Nat. Commun. 7, 12204 (2016).
Lanciotti, R. S. et al. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 14, 1232–1239 (2008).
Hansen, S. G. et al. Immune clearance of highly pathogenic SIV infection. Nature 502, 100–104 (2013).
Krabbe, N. P. et al. Control of maternal Zika virus infection during pregnancy is associated with lower antibody titers in a macaque model. Front. Immunol. 14, 1267638 (2023).
Hall, J. W. New Handbook of Auditory Evoked Responses (Pearson, 2007).
Huang, Y. et al. Development of a semi-automatic segmentation method for retinal OCT images tested in patients with diabetic macular edema. PLoS ONE 8, e82922 (2013).
Robson, A. G. et al. ISCEV guide to visual electrodiagnostic procedures. Doc. Ophthalmol. 136, 1–26 (2018).
Sitdikova, G. et al. Isoflurane suppresses early cortical activity. Ann. Clin. Transl. Neurol. 1, 15–26 (2014).
Acknowledgements
We thank the Wisconsin National Primate Research Center, specifically Behavioral Management Services, Scientific Protocol Implementation Services, Pathology Services, and Veterinary Services for their assistance with this project. We thank David O’Connor for insightful discussions on experimental design. This project was supported in part by NIH P01AI132132. We used ChatGPT 4o to assist with improving readability. We thank Saswati Bhattacharya, Taylor Treadway, and Nikunj Makwana for their contributions. This work was supported by the National Institutes of Health grants R01 AI153130 (to K.K.A. and E.L.M.), P01AI132132 (David O’Connor), and P30EY016665 (Vision Research Core), and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development grant P50HD105353 (Waisman Center).
Author information
Authors and Affiliations
Contributions
Conceptualization: K.K.A. and E.L.M. Methodology: K.K.A., A.H., A.M.W., C.R., M.N., H.A.S., J.V.H., T.C.F., M.T.A., and E.L.M. Investigation: K.K.A., B.B., E.R.R., J.K., N.P.K., A.M.M., S.W., V.M., J.R.D., S.K., F.E., R.V.S., A. Shah, A. Sun, J.G., A.K., C.K., A.H., A.M.W., C.R., M.N., P.B., H.A.S., J.V.H., M.T.A., and E.L.M. Visualization: E.R.R., A. Shah, A. Sun, J.V.H., and E.L.M. Funding acquisition: K.K.A. and E.L.M. Project administration: K.K.A. and E.L.M. Supervision: K.K.A., A.H., M.N., H.A.S., S.C., and T.C.F. Writing—original draft: K.K.A., B.B., E.R.R., and J.K. Writing—review & editing: K.K.A., B.B., E.R.R., J.K., N.P.K., A.M.M., S.W., V.M., J.R.D., S.K., F.E., R.V.S., A. Shah, A. Sun, J.G., A.K., C.K., A.H., A.M.W., C.R., M.N., P.B., S.C., H.A.S., J.V.H., M.T.A., T.C.F., and E.L.M.
Corresponding author
Ethics declarations
Competing interests
J.V.H. is a consultant for a company called OSOD, A Merit Company, which provides consulting services to the pharmaceutical industry. The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks the anonymous reviewers for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ausderau, K.K., Boerigter, B., Razo, E.R. et al. Prenatal Zika virus exposure disrupts social-emotional development and cortical visual function in infant macaques. Nat Commun 17, 1803 (2026). https://doi.org/10.1038/s41467-026-68517-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-68517-x
