
Abstract
Phage therapy is emerging as a promising alternative to antibiotics for treating various infections. However, there have been no prior studies on using bacteriophages for peritonitis in patients undergoing peritoneal dialysis. This report presents the successful treatment of refractory peritonitis in a 71-year-old male peritoneal dialysis patient using bacteriophages combined with antibiotics. The patient has a history of refractory and repeat peritonitis caused by Staphylococcus haemolyticus, which was resolved through simultaneous catheter replacement (SCR). Subsequently, the patient experiences another episode of refractory peritonitis due to Klebsiella pneumoniae. Although this strain is found to be susceptible to amikacin and imipenem, a 14-day course of treatment with these antibiotics in the abdominal cavity fails to resolve the peritonitis. Combined with antibiotic therapy, the patient is successfully treated with intraperitoneal phage therapy targeting his bacterial isolate. We monitor the longitudinal progression of phage loads, phage-neutralizing antibodies, interleukin-6 levels, and lipopolysaccharide concentrations in the dialysate effluent during the bacteriophage therapy. The combination of a phage cocktail and imipenem (IPM) demonstrates a greater effect in killing bacteria than either treatment alone, which indicates that a synergistic effect exists between the phage cocktail and IPM. Intraperitoneal IPM is discontinued after a 3-week course of treatment. At the same time, oral fluconazole is given to prevent fungal infections. The patient is discharged without any antibiotics. After this round of treatment, the patient remains healthy during the one-month follow-up. Our study suggests that personalized phage therapy combined with sensitive antibiotics can play a significant role in managing refractory peritonitis in patients undergoing peritoneal dialysis, showing promise for future applications.
Similar content being viewed by others

Introduction
Bacteriophages, or phages, are viruses that specially infect bacteria, leading to bacterial death through a process called lytic replication. The therapeutic potential of lytic phages is being increasingly explored for treating difficult-to-manage infections1. Peritonitis is a major cause of treatment failure in patients undergoing peritoneal dialysis (PD). Over the past few decades, the incidence of PD-related peritonitis has significantly decreased, largely due to improvements in connection techniques and protocols for decolonizing Staphylococcus. These advancements have primarily reduced the rate of Gram-positive peritonitis, resulting in an increased proportion of Gram-negative peritonitis. It has been reported that the incidence rate and proportion of Gram-negative bacterial peritonitis have increased gradually in recent decades, and the relapse and recurrence rate for Gram-negative bacterial peritonitis was higher than that for other pathogens, with severe clinical manifestations and poor prognosis2. Retrospective studies have indicated that Gram-negative peritonitis has higher risks of catheter loss and mortality when compared with Gram-positive episodes3,4,5,6,7. Among these bacteria involved, Klebsiella pneumoniae has been identified as the second most common Gram-negative pathogen responsible for monomicrobial PD-related peritonitis. This pathogen can lead to serious complications, including increased morbidity, a higher risk of PD catheter removal, and a greater mortality rate in PD-related peritonitis8.
Relapsing or repeat peritonitis caused by coagulase-negative Staphylococcus might indicate that the PD catheter is colonized with biofilm and catheter removal should be considered. If the PD effluent becomes clear with antibiotic therapy, many patients might benefit from the simultaneous re-insertion of a new catheter during the same procedure, provided they are on antibiotic coverage. This approach could help avoid the need for temporary hemodialysis9. However, the practice of simultaneous catheter replacement (SCR) remains controversial in cases of refractory peritonitis in PD patients. Current evidence suggests that refractory peritonitis may be caused by bacterial adherence along the intraperitoneal portion of the catheter. There has been a reported case where refractory peritonitis caused by Pseudomonas aeruginosa was successfully treated with SCR after a partial response to antibiotics10.
Local production of interleukin-6 (IL-6) serves as a marker of ongoing intraperitoneal inflammation in patients undergoing PD11,12. The concentrations of IL-6 in drained PD fluid (PDF) are significantly higher than in plasma under stable conditions. Moreover, levels of IL-6 in the dialysate increase shortly before the onset of, during peritonitis, and several months after clinically successful treatment for peritonitis, suggesting its local production and reflecting an intraperitoneal inflammatory state13,14,15. Lipopolysaccharide (LPS), also known as endotoxin, is a key component of the outer membrane of Gram-negative bacteria. It plays an essential role in maintaining cell wall integrity, acting as a barrier against harmful compounds and potential antibiotics in the environment16. LPS is released from the outer membrane during bacterial cell death or cell division and growth17. It has been reported that increased effluent LPS level was a prompt marker of Gram-negative peritonitis in PD patients18,19,20. It is necessary to measure the levels of both IL-6 and LPS in dialysate effluent during and after phage administration.
In this study, we reported the innovative use of personalized bacteriophage therapy in combination with antibiotics for treating refractory peritonitis caused by Klebsiella pneumoniae in a patient undergoing peritoneal dialysis.
Results
Patient history
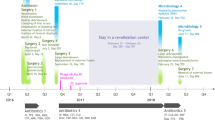
A 71-year-old male patient with end-stage renal disease due to membranous nephropathy began continuous ambulatory peritoneal dialysis (CAPD) in November 2015. The patient had a history of hypertension. Additionally, the patient experienced renal anemia, which was treated with erythropoietin. However, as the peritonitis progressed, the patient’s anemia worsened, leading to an increase in the dosing of erythropoietin. The patient also had secondary hyperparathyroidism, which was managed with cinacalcet. The parathyroid hormone level of this patient remained stable during that period. His medical history was significant for three episodes of peritonitis. In October 2023, the first case of peritonitis was reported, and the culture results were negative. In February 2024, a second episode of peritonitis occurred, which was identified as Staphylococcus epidermidis. By May 2024, a third episode of peritonitis took place, involving Staphylococcus haemolyticus. All three episodes of peritonitis were successfully treated with effective antibiotics. The patient received CAPD, which included four exchanges: three with 1.5% glucose and one overnight with 7.5% icodextrin, totaling a volume of 8 L. In early July 2024, the patient experienced another episode of peritonitis with cloudy peritoneal fluid and mild abdominal pain. Cultures from the PDF identified Staphylococcus haemolyticus, confirming a case of repeat peritonitis. Due to concerns about biofilm formation, an SCR was performed on July 17, 2024, once the PD effluent became clear. After the SCR, low-dose abdominal dialysis treatment began the next day while the patient remained in a supine position. We also continued administering intraperitoneal vancomycin for further treatment (Fig. 1).

(A) Bacteriologic cultures (▎dialysis effluent cultures: The dialysis effluent culture identified Staphylococcus haemolyticus on July 17, 2024. Subsequent cultures on July 26 and August 1, 2024, identified Klebsiella pneumoniae; Culture returned negative results on August 16 and August 18, 2024. ▎PD catheter tip culture identified Staphylococcus haemolyticus on July 18, 2024.). (B) Antibiotic regimens used: the patient was treated with vancomycin, tigecycline, teicoplanin, fluconazole, amikacin, and imipenem. (C) Bacteriophage treatment: Intraperitoneal bacteriophages were administered from August 13 to August 15, 2024. The cocktail of phage included ΦCP-p-KP-23240 and ΦCP-p-KP-21067. (D) the WBC counts in PD effluent and serum CRP levels were monitored. ▼SCR: simultaneous catheter replacement.
Refractory peritonitis caused by Klebsiella pneumoniae
The patient developed diarrhea three days after the SCR, and the PD effluent became cloudy again. We performed another bacterial culture of the effluent and adjusted the anti-infection regimen to include the systemic administration of tigecycline (50 mg q12h), combined with oral fluconazole (100 mg daily) and intraperitoneal teicoplanin (15 mg/kg per 5 days). On July 26, 2024, Klebsiella pneumoniae was identified in the PD effluent culture, with no growth of Staphylococcus haemolyticus. The antibiotic sensitivity of the patient’s isolate of Klebsiella pneumoniae was presented in Table 1, which did not change over all the cultures obtained. Based on the antibiogram, the antibiotic therapy was switched to intraperitoneal amikacin (200 mg daily) and imipenem (500 mg daily), along with oral fluconazole (100 mg daily) to reduce the risk of fungal peritonitis. After 14 days of standard treatment, the PD fluid remained cloudy, and the white blood cell (WBC) counts in the PD effluent fluctuated from 1370 cells/μL to 11885 cells/μL. On August 1, 2024, Klebsiella pneumoniae was still present in the PD effluent culture. We considered this episode of peritonitis caused by Klebsiella pneumoniae as refractory, and according to the International Society for Peritoneal Dialysis (ISPD) guidelines, catheter removal should be considered. Due to the significant difficulty of attending the hemodialysis center, the patient was reluctant to switch from peritoneal dialysis to hemodialysis. In this case of refractory peritonitis, phage therapy might be a potential treatment option. Due to the ototoxicity linked with amikacin, it was discontinued after 12 days of treatment. The antibiotic regimen was adjusted to intraperitoneal imipenem, combined with oral fluconazole only on August 7, 2024. Despite the prolonged use of sensitive antibiotics, the patient experienced a slow but steady improvement, with a minimum WBC count in the effluent of 528 cells/μL (Fig. 1).
Intraperitoneal administration of bacteriophage
The treatment regimen consisted of a combination of antibiotics and included a 3-day phage therapy using the cocktail I (including phages ΦCP-p-KP-23240 and ΦCP-p-KP-21067) from August 13 to August 15, 2024, as described in the methods. Although the WBC counts in the PD effluent fluctuated, reaching up to 6296 cells/μL during the first round of phage therapy, Klebsiella pneumoniae strains were not detected twice after the completion of the phage therapy. On August 18, 2024, the WBC counts in the PD effluent sharply decreased to 26 cells/μL. The dynamic changes of plasma C-reactive protein (CRP) levels are shown in Fig. 1. By the end of the phage therapy, the plasma CRP level had dropped to a near-normal level. Intraperitoneal IPM and oral fluconazole were discontinued after a 3-week treatment course. While using the bacteriophage, this patient did not have any adverse events. The patient was discharged without any medicine on August 21, 2024 (Fig. 1). During the long-term follow-up, there was no relapse of Klebsiella pneumoniae peritonitis.
Biological characteristics of bacteriophages
The biological characteristics of ΦCP-p-KP-23240 and ΦCP-p-KP-21067 used in the therapy case need to be defined. Therefore, the genomes of ΦCP-p-KP-23240 and ΦCP-p-KP-21067 were extracted and sequenced. The result showed their genome sizes were 39766 bp and 38762 bp, respectively, indicating that they both belonged to the Podoviridae. Both genomes were circular double-stranded DNA and did not contain any endogenous genes, which indicated they were lytic phages. Besides, the multiplicity of infection (MOI) of ΦCP-p-KP-23240 and ΦCP-p-KP-21067 were respectively detected. The results showed they were correspondingly 10-5 and 10-6 (Fig. 2A and Fig. 2B), which indicated that both of them had extremely high lysis efficiency for the target bacteria. The one-step growth curve was determined at the MOI of 0.1, which was widely used and recognized. The results showed that ΦCP-p-KP-23240 and ΦCP-p-KP-21067 had a short latent period (0 min) and burst period (25 mins and 30 mins) (Fig. 2C and Fig. 2D), which was very beneficial to clinical therapeutics.

(A) The MOI of ΦCP-p-KP-23240. (B) The MOI of ΦCP-p-KP-21067. (C) The one-step growth curve of ΦCP-p-KP-23240. (D) The one-step growth curve of ΦCP-p-KP-21067. Results are presented as mean values of biological replicates (n = 3) with error bars representing the standard deviations of the means. Source data are provided as a Source Data file.
Synergistic effect for bacteriophages and antibiotics on clinical strains
The sensitivity test and the synergistic effect for bacteriophages and antibiotics were detected by the kill curve test. The result indicated that the bacteria of the patient could be killed by ΦCP-p-KP-23240 within 4 hours, followed by the production of phage resistance. By contrast, ΦCP-p-KP-21067 could not inhibit the growth of bacteria. However, the cocktail could make the resistant time extend to 24 hours or even longer (Fig. 3A), which indicated the phage-resistant mutants could be effectively cleared out by the ΦCP-p-KP-21067. Furthermore, the bacteria were sensitive to the 0.25 and 0.5 μg/mL IPM, but not 0.125 μg/mL (Fig. 3B), which was in accordance with the antibiotic sensitivity test results (Table 1). Moreover, the effect of killing bacteria by combining the utilization of phage cocktail and IPM was superior to the phage cocktail and 0.5 μg/mL IPM, as well as the others (Fig. 3C), which indicated that the synergistic killing effect existed between the phage cocktail and IPM.

(A) The sensitivity test of the bacteria for ΦCP-p-KP-23240, ΦCP-p-KP-21067 and the cocktail. (B) The sensitivity test of the bacteria for IPM. (C) The synergistic effect of the phage cocktail and IPM. Results are presented as mean values of biological replicates (n = 3) with error bars representing the standard deviations of the means. Source data are provided as a Source Data file.
Changes in dialysate IL-6 and LPS levels during phage therapy
Before the bacteriophage treatment began, dialysate IL-6 levels were maintained at a relatively high level, ranging from 22022.05 pg/mL to 42457.05 pg/mL. The levels of IL-6 in the PD effluent rose to 62659.55 pg/mL on August 14, 2024, the second day of phage therapy. The intraperitoneal IL-6 levels gradually declined after that, aligning with the changes in WBC counts in the dialysate effluent. After August 18, 2024, the IL-6 levels in the PD effluent remained relatively low (Fig. 4).

The concentration of IL-6 in the overnight drained PDF was measured using ELISA both before and after phage treatment. Additionally, the LAL assay was used to measure LPS levels in the overnight drained PDF.
The levels of LPS in the PD effluent were monitored during the phage therapy. On August 3, 2024, a high concentration of LPS in the dialysate was recorded at 0.523 EU/mL before the initiation of phage therapy. Over the following days, the LPS levels gradually decreased, reaching a low of 0.007 EU/mL by August 7, 2024. During the phage treatment, there was a slight increase in the dialysate LPS levels, peaking at 0.123 EU/mL on August 16, 2024. This was followed by another decline, with levels dropping to 0.005 EU/mL by August 18, 2024. After this date, LPS in the PD effluent was no longer detectable (Fig. 4).
Neutralizing antibodies of phages in dialysate effluent before and after phage treatment
Phage treatment might fail due to the rapid production of neutralizing antibodies against phages by the host in response to the treatment. We collected dialysate effluent pre-phage day 7 and post-phage days 1, 3, 5, and 15, and tested it for neutralizing antibodies binding to both phages, with and without heating. Our findings indicated that complement inactivation in the dialysate effluent was not sufficient to impact phage activity. The analysis of dialysate effluent before and after treatment revealed no increase in dialysate-mediated neutralization of both ΦCP-p-KP-21067 and ΦCP-p-KP-23240 infections, suggesting that insufficient neutralizing antibodies were produced to affect phage activity (Fig. 5).

(1) The complement in PD effluent was inactivated at 56 °C for 30 min, which was not sufficient to affect phage activity. (2) No detectable levels of phage-neutralizing antibodies were produced intraperitoneally following phage administration, or the levels were too low to significantly impact phage activity. Panel A displays the results for strain ΦCP-p-KP-21067, while Panel B presents the results for strain ΦCP-p-KP-23240. Results are presented as mean values of biological replicates (n = 3) with error bars representing the standard deviations of the means. Source data are provided as a Source Data file.
Determination of phage titre in dialysate effluent
We collected dialysate effluent pre-phage day 7 and post-phage days 1, 3, 5, and 15, and tested it for the presence of phage in dialysate effluent, both with and without heating. Our findings revealed that the phage load decreased by ~10,000-fold within one day after treatment and could not be detected after 48 h for both ΦCP-p-KP-21067 and ΦCP-p-KP-23240 (Fig. 6). After the treatment, the patient was discharged with improved symptoms of infection. One month later, the patient was readmitted to the hospital for further evaluation and remained in good health.

Phage residues were identified in dialysate effluent following administration. On day 2, the concentrations exceeded 103 PFU/mL and reached over 104 PFU/mL by day 4. Panel A presents the results for strain ΦCP-p-KP-21067, while Panel B shows the results for strain ΦCP-p-KP-23240. The complement in dialysate effluent was either inactivated at 56 °C for 30 min or left untreated.
Review of published literature
After conducting extensive literature research, a total of 14 patients have received phage therapy for infections caused by Klebsiella pneumoniae. Out of these, 13 cases were successfully treated or showed clinical improvement, while 1 case did not respond to the treatment. The infection sites among these 14 patients included: 7 urinary tract infections, 2 post-fracture infections, 2 pulmonary infections, 2 post-joint replacement infections, and 1 case of purulent meningitis. Eleven patients received phage therapy in combination with antibiotics, while 3 patients received phage therapy alone. Throughout the phage therapy process for all 14 patients, no notable side effects were observed (Table 2).
Discussion
Phage therapy is a promising method for treating bacterial infections21. To our knowledge, this was the first report on the successful use of phage therapy for refractory peritonitis in PD patients. The patient in our study was suffering from refractory peritonitis caused by Klebsiella pneumoniae. Long-term antibiotic treatment significantly affected his quality of life and compromised the structural integrity of the peritoneal membrane. However, the patient was strongly opposed to the transition to hemodialysis. Given these circumstances, we proposed phage therapy as a compassionate use option while continuing standard-of-care antibiotics during the treatment, as previously reported22. In this instance, we applied a bacteriophage cocktail for the first time to treat refractory peritonitis induced by Klebsiella pneumoniae in a PD patient.
Phage therapy represents a promising strategy for treating infections caused by multidrug-resistant (MDR) bacteria23. Before administration, the first crucial step is to select the phage (or phages) efficiently targeting the bacteria to treat. Despite the significant biodiversity of phages, not all of them have the potential to be implemented in clinics, and they must be thoroughly characterized prior to their use24. In addition, the success of phage therapy might be limited by the development of phage resistance by bacteria25, much akin to the resistance developed toward antibiotics26. However, it can be prevented or delayed by different approaches. A common method is the combination of phages in a cocktail, allowing them to further reduce the bacterial burden and to increase the host range27. Indeed, this strategy has been widely employed as ready-to-use products for prevention or therapeutics28. In this context, we employed a phage cocktail therapy with a secondary phage to help reduce the risk of developing phage-resistant bacteria.
Another approach is combining phages with antibiotics, since it has been shown that phage-resistant mechanisms could re-sensitize bacteria to antibiotics, known as phage-antibiotic synergy (PAS effect). The relationship between the use of phage therapy and conventional antibiotics is complex and not completely understood. Under various conditions, in vitro studies of combined use of phage and antibiotics have identified additive, synergistic, antagonistic, or no effects29. Enhanced susceptibility to antibiotics by phage may occur via modification of cell wall permeability and anti-biofilm mechanisms30,31,32. In a recent study associated with phage treatment of Mycobacterium abscessus in advanced lung disease, it was confirmed that phage treatment did not promote antibiotic resistance33. Reports indicate that when Klebsiella pneumoniae is sensitive to certain antibiotics that do not cause complications, it is highly beneficial to combine this antibiotic with a phage cocktail34. This combined approach helps minimize the chances of regrowth of phage-resistant mutants. We presented a case report of a PD patient with refractory peritonitis caused by Klebsiella pneumoniae, successfully treated with a combination of an intraperitoneal bacteriophage cocktail and sensitive antibiotics. During the phage therapy, no adverse events were reported, and the patient was discharged one week after completing antibiotic treatment. At the one-month follow-up, no signs of peritonitis recurrence were observed.
A major concern with phage therapy is the eventual immune response against phages35. In some phage treatments, an immune response has been observed, whereas other studies have failed to demonstrate this, possibly due to the assumption that phages do not elicit a generalized immune response36,37. Nevertheless, it was found that synergy between bacteriophages and the immune system may be essential for the resolution of infections38. Indeed, given the natural interaction between humans and phages39,40, the relevance of immune response evaluation has often been overlooked, and the assessment of anti-phage antibody production following phage therapy has not been systematically examined. During the prolonged course of antibiotic and phage treatments, the emergence of neutralizing antibodies against phages poses a potential concern. It has been reported that the lack of anti-phage neutralizing antibodies was associated with the successful treatment of a patient with disseminated drug-resistant Mycobacterium abscessus41. Conversely, the rapid development of these antibodies was associated with treatment failure in a pulmonary Mycobacterium abscessus infection42. In our case, the phage cocktail was used in the peritoneal cavity, so we detected the neutralizing antibodies of the phage cocktail in the peritoneal cavity. The results showed that there were insufficient neutralizing antibodies produced in the peritoneal cavity to affect phage activity.
In previous overview of the first 100 consecutive real-world cases of personalized bacteriophage therapy treatment, it has been shown that when used in the treatment of 114 difficult-to-treat infections of various types and etiology, in combination with antibiotics 69.3% of cases, these preparations led to clinical improvements in 77.2% and eradication of the targeted bacteria in 61.3% of cases; seven non-serious suspected adverse drug reactions were reported37. In line with previous studies, a total of 14 patients who received phage therapy for refractory infections caused by Klebsiella pneumoniae were included in this study through an extensive literature review. Of the cases, 13 were successfully treated or showed clinical improvements, while only 1 case did not respond to treatment. 11 patients received phage therapy combined with antibiotics, and only 3 patients received phage therapy alone. The results indicated that phage therapy could be effective in treating refractory infections caused by Klebsiella pneumoniae, regardless of antibiotic use. The literature review identified several infection sites, including the urinary tract, post-fracture areas, lungs, locations following joint replacements, and one case of purulent meningitis. In this case report, we evaluated a PD patient who suffered from refractory peritonitis caused by Klebsiella pneumoniae and was successfully treated using a combination of an intraperitoneal bacteriophage cocktail along with sensitive antibiotics. This treatment represents the first application of bacteriophages in the management of refractory peritonitis. In a mouse model of severe septic peritonitis, a single injection of a bacteriophage cocktail completely reversed the trend of 100% mortality caused by Vancomycin-Resistant Enterococcus faecalis, leaving the microbiome unaffected43. This finding suggests that further research is necessary for patients experiencing refractory peritonitis related to peritoneal dialysis.
In Gram-negative sepsis, LPS is the primary trigger of the condition. It initiates a complex series of reactions that activate various cell types, including macrophages, neutrophils, endothelial cells, and resident tissue cells. Additionally, LPS stimulates fluid-phase plasma systems, such as the complement system and coagulation pathways44. Multiple studies have shown that the presence of LPS in dialysate effluent is indicative of Gram-negative bacteria causing PD-related peritonitis18,45,46. In our case report, we noted a high level of LPS in the dialysate, which gradually decreased before we started phage treatment. After completing the phage treatment, we observed a slight increase in LPS levels in the dialysate the day after treatment ended. However, this level subsequently declined and ultimately fell to an undetectable range. The temporary rise in LPS levels within the abdominal cavity might be associated with the phage infection and the subsequent lysis of Klebsiella pneumoniae. Local production of IL-6 serves as a marker for ongoing intraperitoneal inflammation in patients undergoing peritoneal dialysis11,47. PD patients with elevated IL-6 levels are at an increased risk of experiencing subsequent episodes of peritonitis during long-term follow-up12. In this case report, the levels of IL-6 in the dialysate were relatively high before bacteriophage treatment and peaked on the second day of treatment. The elevated levels of IL-6 might be associated with a temporary increase in LPS levels caused by the lysis of Klebsiella pneumoniae. After this peak, IL-6 levels gradually decreased, which aligned with changes in the WBC counts found in the dialysate effluent. Whereas, it has been reported that Lysis-deficient (LyD) phage therapy improved survival in murine peritonitis, which decreased LPS levels as well as cytokine release at the local site of infection48. This may minimize systemic cytokine responses and limit inflammation in bacterial sepsis. It warrants further investigation, particularly regarding refractory peritonitis.
The use of SCR in cases of mechanical complications of PD is well-established49, but its application for resolving peritonitis remains debated. Current evidence suggests that refractory peritonitis is often associated with bacterial adherence to the silicone catheter or the formation of biofilm along the tunnel or intraperitoneal section of the catheter50. This case report demonstrated the successful use of SCR as a treatment for refractory and repeat Staphylococcus haemolyticus peritonitis. The culture results from the tip of the removed catheter confirmed the presence of Staphylococcus haemolyticus, supporting our suspicion that biofilm formation by this bacterium on the inner surface of the catheter was responsible for the recurrent/repeat peritonitis.
Our study has several limitations. First, this study is a case report, and further research involving a larger sample size is necessary to confirm the value of phage therapy in treating refractory peritonitis. Second, while we conducted multiple bacterial culture tests on the peritoneal dialysis fluid during the treatment process, we did not perform metagenomic next-generation sequencing (mNGS). mNGS has been shown to improve the identification of pathogens in infectious diseases. Reports indicate that the pathogen detection rate of mNGS in the dialysis effluent of patients with peritonitis is significantly higher than that of traditional culture methods51. By continuously monitoring the WBC counts in the peritoneal dialysis effluent and correlating them with the dialysate culture results, we can effectively evaluate the therapeutic outcome of peritonitis. Finally, conducting a biofilm assay for Staphylococcus haemolyticus would have strengthened our findings by demonstrating the isolate’s biofilm-producing capability during the SCR process.
Our study demonstrated the safety and effectiveness of using personalized intraperitoneal bacteriophage treatment combined with antibiotics for refractory peritonitis caused by Klebsiella pneumoniae. Although our findings were based on a single observation, they clearly showed the successful application of phage therapy for refractory peritonitis related to PD. Additionally, the study also supported the use of specifically tailored phage therapies. We eagerly anticipate further clinical trials exploring the use of bacteriophages for PD-related peritonitis, especially in cases of refractory peritonitis.
Method
Klebsiella pneumoniae clinical isolates and antibiotic susceptibility assay (AST)
Before phage therapy, a clinical strain of Klebsiella pneumoniae was isolated from the patient’s peritonitis dialysate on July 26, 2024. The strain was cultured on MacConkey Agar plates and subsequently identified using mass spectrometry with Bruker MALDI (Matrix-assisted laser desorption/ionization) Biotyper Rapid Microbial Identification System (Bruker Daltonik GmbH). It was also cultured in Luria-Bertani medium at 37 °C52,53. To assess antibiotic sensitivity, the agar disk diffusion method was employed under the Clinical and Laboratory Standards Institute (CLSI) standard. The bacterial load was measured using Semi-Quantitative Clinical Cultures as previously described54. In brief, the culture plate was divided into four quadrants, and the peritonitis dialysate was streaked from the first quadrant to the last using an inoculation loop. After a 24-h incubation period, the number of quadrants exhibiting bacterial growth was evaluated. A result of ‘0’ was recorded if no growth of Klebsiella pneumoniae was observed on the plate; ‘1’ was noted if growth occurred only in the first quadrant; ‘2’ was reported if growth was observed in both the first and second quadrants.
Susceptibility testing of phage in the library by the phage spot test
Phages against the patient’s Klebsiella pneumoniae isolate, which was cultured on July 26, 2024, were screened from the Bacteriophage Library (CreatiPhage Biotechnology Co., Ltd, Shanghai, China.) using the method of spot test and the double agar overlay method55. The susceptibility of target bacteria to phages was measured by the efficiency of plating (EOP) assay as previously described56. Briefly, the bacteria were added to the 10 mL 0.5% LB medium. After mixing, the mixture was poured onto the 15 cm plate containing 1.5% LB medium, followed by waiting to solidify. 2 μL of each Klebsiella pneumoniae phage (a total of 250 different phages) was dropped onto the bacterial lawn, followed by waiting to dry. Finally, the plate was cultured at 37 °C overnight. The appearance of clear plaques means that the phages were sensitive to the bacteria. The experiment was performed three times. For the first round of phage therapy, two Klebsiella pneumoniae phages, ΦCP-p-KP-23240 and ΦCP-p-KP-21067, were selected to form the cocktail I. The titer of phage ΦCP-p-KP-23240 against the pathogenic bacteria from the patient was found to be 5 × 108 PFU/mL. Phage ΦCP-p-KP-21067 served as a second-line anti-tolerance phage but did not exhibit a lytic effect on the pathogenic bacteria57, and its titer against the expanded host was measured at 1 × 108 PFU/mL.
Genome sequencing and bioinformatics analysis of phages
The genomes of ΦCP-p-KP-23240 and ΦCP-p-KP-21067 were extracted using a viral genome extraction kit (QIAamp MinElute Viral Spin Kit, Qiagen, Hilden, Germany) following the instructions. The genomes were sequenced at Sangon Biotech, Shanghai, using the IlluminaHiSeq 2500 platform and assembled using SPAdes 3.15.5. Their genome sequences have been deposited in the GenBank in the National Center for Biotechnology Information (NCBI, Genbank NO. PX120905 and PX120903) (https://www.ncbi.nlm.nih.gov/).
Multiplicity of infection and one-step growth curve of phages
The host bacteria, Klebsiella pneumoniae, were cultured to the logarithmic growth phase (OD600 nm = 0.6) and adjusted to ~1 × 108 CFU/mL. Different amounts of ΦCP-p-KP-23240 were then added according to the multiplicity of infection (MOI) ratios of 1, 0.1, 0.01, 0.001, 0.0001, 0.00001, and 0.000001. For ΦCP-p-KP-21067, the MOI ratios used were 10, 1, 0.1, 0.01, 0.001, 0.0001, 0.00001, and 0.000001. The mixtures were cultured for 8 h at 37 °C while shaking at 180 rpm. After incubation, the cultures were centrifuged at 8000 × g for 5 min at 4 °C and subsequently filtered. Phage titers were detected using the double-layer plate method. This experiment was conducted in triplicate. For further analysis, phages (at an MOI of 0.1) were added to 0.1 mL of Klebsiella pneumoniae culture (1 × 108 CFU/mL) during the logarithmic growth phase and incubated for 5 min at 37 °C. The mixture was then centrifuged at 10,000 × g for 5 min at 4 °C. The pellet was resuspended in 10.0 mL of fresh LB liquid medium and incubated at 37 °C with shaking at 180 rpm. Samples of 200 µL were taken every 5 min during the first 30 min, and then every 10 min until reaching a total of 60 min, ultimately extending the time to 90 min. Two samples were collected at each time point. One sample was immediately filtered through a 0.22 μm filter and diluted for phage titer detection using the double-layer plate method. The other sample was treated with 1% (v/v) chloroform for 30 min at room temperature to determine the titer58. This experiment was also repeated in triplicate.
Sensitivity test and synergistic effect for bacteriophages and antibiotics
The sensitivity of the bacteria in the patient to the bacteriophages and antibiotics was detected by the kill curve test, as well as the synergistic effect of bacteriophages and antibiotics. Briefly, 190 μL of LB medium was added to one well of a 96-well plate, which was followed by adding 10 μL of the bacterial culture in the logarithmic growth phase. After mixing, 1 μL of bacteriophages or a specific concentration of imipenem (IPM, final concentration of 0.125, 0.25, or 0.5 μg/mL) was added to it. The well that only added the bacteria was the negative control. After all the above, the 96-well plate was placed in the BioTek 800 TS (America). The parameters were set as a total of 24 h of testing time at 37 °C, containing a 20-min interval as the reading period, which was performed at OD600 nm. The experiment was performed three times.
Bacteriophage propagation and administration
The preparation of the phage agent followed established protocols57. Phages were cultured on their original host, resulting in lysates with titers exceeding 1 × 109 PFU/mL. These lysates were then purified using a CIM® Anion Exchange Column QA (BIA Separations, Slovenia) according to the manufacturer’s instructions. The concentrate was dialyzed against a 0.9% sodium chloride physiological solution three times, with each dialysis lasting a minimum of three hours. Finally, the phage-containing solution was sterilized through a 0.22 μm filter, aliquoted, and packaged at the Good Manufacturing Practice (GMP) facility of Zhongshan Hospital of Fudan University, Shanghai, China. The phage cocktail I used (ΦCP-p-KP-23240 and ΦCP-p-KP-21067) was diluted in saline to a total volume of 10 mL, achieving concentrations of 5 × 108 PFU/mL for ΦCP-p-KP-23240 and 1 × 108 PFU/mL for ΦCP-p-KP-21067.This cocktail was diluted in peritoneal dialysate to a final volume of 1 L, achieving a concentration of 106 PFU/mL for each phage, which was administered through the PD catheter. The phage solution was retained in the intraperitoneal cavity for four hours and then drained out. The phage cocktail was injected twice a day for 3 consecutive days and two doses were administered successively. Simultaneously, the external exit of the PD catheter was moistened with a sterile gauze soaked in the phage solution for at least 20 min.
Phage neutralization assays
As previously described33, each PDF sample was diluted 1:10 in phage buffer, which consisted of 10 mM Tris-HCl (pH 7.5), 10 mM MgSO4, and 68 mM NaCl. The diluted samples were then incubated with either ΦCP-p-KP-23240 or ΦCP-p-KP-21067 at room temperature for 24 h. After incubation, 10-fold serial dilutions were performed, with 3 μL of each dilution placed onto top agar, followed by incubation at 37 °C for 24 h. Additionally, some PDF samples were inactivated by heating at 56 °C for 30 min to deactivate the complement. Each sample was tested in triplicate on each bacterial strain and the mean value and standard deviation were determined for each dialysate sample.
Determination of phage titre in dialysate effluent
Peritoneal dialysis effluent was collected from patients before and after phage treatment to determine the phage titre. The peritoneal dialysis fluid was then centrifuged at 8000 × g for 2 min. The phage titre was measured using the EOP, as described previously56. A volume of 5 µl from serial 10-fold dilutions of the phage was spotted on double-layer agar plates, onto which the host bacteria, Klebsiella pneumoniae, had been spread in the upper soft agar. The number of plaques was counted after overnight incubation. Additionally, some peritoneal dialysis fluid samples were inactivated by heating at 56 °C for 30 minutes to deactivate the complement.
Determination of interleukin-6 levels in dialysate effluent
The concentration of IL-6 in the overnight drained PDF was measured using an enzyme-linked immunosorbent assay (ELISA). All samples were analyzed simultaneously and in duplicate to minimize both intra- and inter-assay variations. The IL-6 concentration was determined using the Quantikine ® kit from R&D Systems Inc. (Minneapolis, MN, USA). The detectable range specified by the manufacturer was from 3.1 to 300 pg/mL. For samples that exceeded the detection level, we diluted them appropriately before conducting the test. The IL-6 value was reported as the mean of the parallel readings for each specimen. WBC counts in PD effluent and serum CRP levels were monitored, respectively.
Determination of lipopolysaccharide levels in dialysate effluent
A commercial photometric Limulus Amebocyte Lysate (LAL) assay kit (Charles River Laboratories International, Inc., Guangdong, China) was utilized to measure LPS levels in the overnight drained PDF. The detectable range specified by the manufacturer was 0.005–2.500 EU/mL, with an upper normal limit for plasma samples set at 0.053 EU/mL. Effluent specimens were stored in pyrogen-free tubes and processed within four hours. According to the manufacturer’s instructions, one serving of the LAL assay was dissolved in 250 mL of reagent water. One hundred microliters of each effluent were diluted tenfold and then subsequently heated in a 75 °C thermostat for ten minutes. After cooling to room temperature, 50 mL of specimen diluent was combined with 100 mL of the LAL solution in a reaction tube. Each specimen analysis included parallel measurements in two individual tubes, as well as two duplicate tubes containing 100 mL of reagent water as the negative controls, and two duplicate tubes containing 100 mL of quality control solution as the positive controls. All the tubes were incubated at 37 °C for 75 min and readings were taken using the LKM series Kinetic Tube reader (Lab Kinetics Ltd, UK). The LPS value was reported as the mean of the parallel readings for each specimen.
Literature search
To summarize the application of phage therapy in related infections caused by Klebsiella pneumoniae, we searched the PubMed database for related articles from 1985 to 2024. An electronic search was performed using the keywords “Klebsiella pneumoniae” and “phage” or “bacteriophage”.
Ethics approval statement
This study protocol was reviewed and approved by the Ethics Committee of Zhongshan Hospital, approval number [B2024-041R], and the participant gave written informed consent, according to CARE guidelines and in compliance with the Declaration of Helsinki Ethical Principles. Consent to publish clinical information potentially identifying individuals was also obtained.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The genome sequences of phages ΦCP-p-KP-23240 and ΦCP-p-KP-21067 have been deposited in GenBank at the National Center for Biotechnology Information (https://www.ncbi.nlm.nih.gov/), under accession codes PX120905 and PX120903, respectively. The authors declare that all other data supporting the findings of this study are available within the article. Source data are provided with this paper.
References
Hatfull, G. F., Dedrick, R. M. & Schooley, R. T. Phage Therapy for Antibiotic-Resistant Bacterial Infections. Annu. Rev. Med. 73, 197–211 (2022).
Feng, X. et al. Escherichia coli Peritonitis in peritoneal dialysis: the prevalence, antibiotic resistance and clinical outcomes in a South China dialysis center. Perit. Dial. Int. 34, 308–316 (2014).
Jarvis, E. M. et al. Predictors, treatment, and outcomes of non-Pseudomonas Gram-negative peritonitis. Kidney Int. 78, 408–414 (2010).
Valdés-Sotomayor, J. et al. Increased severity of Escherichia coli peritonitis in peritoneal dialysis patients independent of changes in in vitro antimicrobial susceptibility testing. Perit. Dial. Int. 23, 450–455 (2003).
Prasad, N. et al. Outcome of gram-positive and gram-negative peritonitis in patients on continuous ambulatory peritoneal dialysis: a single-center experience. Perit. Dial. Int. 23, S144–147 (2003).
Szeto, C. C. et al. Enterobacteriaceae peritonitis complicating peritoneal dialysis: a review of 210 consecutive cases. Kidney Int. 69, 1245–1252 (2006).
Zurowska, A. et al. Gram-negative peritonitis in children undergoing long-term peritoneal dialysis. Am. J. Kidney Dis. 51, 455–462 (2008).
Lin, W. H. et al. Clinical and microbiological characteristics of peritoneal dialysis-related peritonitis caused by Klebsiella pneumoniae in southern Taiwan. J. Microbiol. Immunol. Infect. 48, 276–283 (2015).
Cancarini, G. C. et al. Simultaneous catheter replacement-removal during infectious complications in peritoneal dialysis. Adv. Perit. Dial. 10, 210–213 (1994).
Nardelli, L. et al. Simultaneous removal and replacement of the peritoneal catheter in CAPD patient with refractory peritonitis sustained by P. aeruginosa: a case-report. J. Vasc. Access 25, 1341–1344 (2024).
Yang, X. et al. Intraperitoneal interleukin-6 levels predict peritoneal solute transport rate: a prospective cohort study. Am. J. Nephrol. 39, 459–465 (2014).
Yang, X. et al. High Intraperitoneal interleukin-6 levels predict peritonitis in peritoneal dialysis patients: a prospective cohort study. Am. J. Nephrol. 47, 317–324 (2018).
Zemel, D., Betjes, M. G., Dinkla, C., Struijk, D. G. & Krediet, R. T. Analysis of inflammatory mediators and peritoneal permeability to macromolecules shortly before the onset of overt peritonitis in patients treated with CAPD. Perit. Dial. Int. 15, 134–141 (1995).
Lai, K. N. et al. Changes of cytokine profiles during peritonitis in patients on continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis. 35, 644–652 (2000).
Zemel, D. et al. Relationship of TNF-alpha, interleukin-6, and prostaglandins to peritoneal permeability for macromolecules during longitudinal follow-up of peritonitis in continuous ambulatory peritoneal dialysis. J. Lab. Clin. Med. 122, 686–696 (1993).
Sutcliffe, I. C. A phylum level perspective on bacterial cell envelope architecture. Trends Microbiol. 18, 464–470 (2010).
Buttenschoen, K., Radermacher, P. & Bracht, H. Endotoxin elimination in sepsis: physiology and therapeutic application. Langenbecks Arch. Surg. 395, 597–605 (2010).
Muhammed, K. O., Ozener, Q. & Akoglu, E. Diagnostic value of effluent endotoxin level in gram-negative peritonitis in CAPD patients. Perit. Dial. Int. 21, 154–157 (2001).
Szeto, C. C. et al. Dialysate bacterial endotoxin as a prognostic indicator of peritoneal dialysis related peritonitis. Nephrology 21, 1069–1072 (2016).
Yan, H., Ma, D., Yang, S., Ni, Z. & Fang, W. Effluent lipopolysaccharide is a prompt marker of peritoneal dialysis-related gram-negative peritonitis. Perit. Dial. Int. 40, 455–461 (2020).
Uyttebroek, S. et al. Safety and efficacy of phage therapy in difficult-to-treat infections: a systematic review. Lancet Infect. Dis. 22, e208–e220 (2022).
Chan, B. K. et al. Personalized inhaled bacteriophage therapy for treatment of multidrug-resistant Pseudomonas aeruginosa in cystic fibrosis. Nat. Med. 31, 1494–1501 (2025).
Moelling, K., Broecker, F. & Willy, C. A wake-up call: we need phage therapy now. Viruses 10, 688 (2018).
Philipson, C. W. et al. Characterizing phage genomes for therapeutic applications. Viruses 10, 188 (2018).
Egido, J. E., Costa, A. R., Aparicio-Maldonado, C., Haas, P. J. & Brouns, S. J. J. Mechanisms and clinical importance of bacteriophage resistance. FEMS Microbiol. Rev. 46, fuab048 (2022).
Rohde, C. et al. Expert opinion on three phage therapy related topics: bacterial phage resistance, phage training and prophages in bacterial production strains. Viruses 10, 178 (2018).
Chadha, P., Katare, O. P. & Chhibber, S. In vivo efficacy of single phage versus phage cocktail in resolving burn wound infection in BALB/c mice. Micro. Pathog. 99, 68–77 (2016).
Huang, Y. et al. Phage products for fighting antimicrobial resistance. Microorganisms 10, 1324 (2022).
Gu Liu, C. et al. Phage-antibiotic synergy is driven by a unique combination of antibacterial mechanism of action and stoichiometry. mBio 11, e01462-20 (2020).
Chakraborty, P. & Kumar, A. The extracellular matrix of mycobacterial biofilms: could we shorten the treatment of mycobacterial infections? Micro. Cell 6, 105–122 (2019).
Li, Q. et al. Mycobacteriophage SWU1 gp39 can potentiate multiple antibiotics against Mycobacterium via altering the cell wall permeability. Sci. Rep. 6, 28701 (2016).
Senhaji-Kacha, A., Esteban, J. & Garcia-Quintanilla, M. Considerations for phage therapy against Mycobacterium abscessus. Front. Microbiol. 11, 609017 (2020).
Nick, J. A. et al. Host and pathogen response to bacteriophage engineered against Mycobacterium abscessus lung infection. Cell 185, 1860–1874.e1812 (2022).
Kuipers, S., Ruth, M. M., Mientjes, M., de Sévaux, R. G. L. & van Ingen, J. A Dutch case report of successful treatment of chronic relapsing urinary tract infection with bacteriophages in a renal transplant patient. Antimicrob. Agents Chemother. 64, e01281-19 (2019).
Champagne-Jorgensen, K., Luong, T., Darby, T. & Roach, D. R. Immunogenicity of bacteriophages. Trends Microbiol. 31, 1058–1071 (2023).
Dedrick, R. M. et al. Phage therapy of Mycobacterium infections: compassionate use of phages in 20 patients with drug-resistant mycobacterial disease. Clin. Infect. Dis. 76, 103–112 (2023).
Pirnay, J. P. et al. Personalized bacteriophage therapy outcomes for 100 consecutive cases: a multicentre, multinational, retrospective observational study. Nat. Microbiol. 9, 1434–1453 (2024).
Roach, D. R. et al. Synergy between the host immune system and bacteriophage is essential for successful phage therapy against an acute respiratory pathogen. Cell Host Microbe 22, 38–47.e34 (2017).
Clokie, M. R., Millard, A. D., Letarov, A. V. & Heaphy, S. Phages in nature. Bacteriophage 1, 31–45 (2011).
Navarro, F. & Muniesa, M. Phages in the human body. Front. Microbiol. 8, 566 (2017).
Dedrick, R. M. et al. Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus. Nat. Med. 25, 730–733 (2019).
Dedrick, R. M. et al. Potent antibody-mediated neutralization limits bacteriophage treatment of a pulmonary Mycobacterium abscessus infection. Nat. Med. 27, 1357–1361 (2021).
Gelman, D. et al. Combined bacteriophages and antibiotics as an efficient therapy against VRE Enterococcus faecalis in a mouse model. Res. Microbiol. 169, 531–539 (2018).
Tetta, C., Bellomo, R., Inguaggiato, P., Wratten, M. L. & Ronco, C. Endotoxin and cytokine removal in sepsis. Ther. Apher. 6, 109–115 (2002).
Clayman, M. D. et al. The Limulus amebocyte lysate assay. A rapid and sensitive method for diagnosing early gram-negative peritonitis in patients undergoing continuous ambulatory peritoneal dialysis. Arch. Intern. Med. 147, 337–340 (1987).
Peer, G., Serban, I., Blum, M., Cabili, S. & Iaina, A. Early diagnosis of gram-negative peritonitis in continuous ambulatory peritoneal dialysis patients with the Lymulus amebocyte lysate assay. Am. J. Nephrol. 12, 19–21 (1992).
Breborowicz, A. & Oreopoulos, D. G. Evidence for the presence of chronic inflammation during peritoneal dialysis: therapeutic implications. Perit. Dial. Int. 17, S37–41 (1997).
Matsuda, T. et al. Lysis-deficient bacteriophage therapy decreases endotoxin and inflammatory mediator release and improves survival in a murine peritonitis model. Surgery 137, 639–646 (2005).
Crabtree, J. H. & Siddiqi, R. A. Simultaneous catheter replacement for infectious and mechanical complications without interruption of peritoneal dialysis. Perit. Dial. Int. 36, 182–187 (2016).
Dasgupta, M. K. Biofilms and infection in dialysis patients. Semin. Dial. 15, 338–346 (2002).
Ye, P. et al. The application of metagenomic next-generation sequencing for detection of pathogens from dialysis effluent in peritoneal dialysis-associated peritonitis. Perit. Dial. Int. 42, 585–590 (2022).
Li, J. et al. A rapid MALDI-TOF mass spectrometry-based method for colistin susceptibility testing in Escherichia coli. Micro. Biotechnol. 15, 528–534 (2022).
Yo, C. H. et al. MALDI-TOF mass spectrometry rapid pathogen identification and outcomes of patients with bloodstream infection: a systematic review and meta-analysis. Micro. Biotechnol. 15, 2667–2682 (2022).
Serena, T. E., Bowler, P. G., Schultz, G. S., D’Souza, A. & Rennie, M. Y. Are semi-quantitative clinical cultures inadequate? Comparison to quantitative analysis of 1053 bacterial isolates from 350 wounds. Diagnostics 11, 1239 (2021).
Yang, L. et al. Temperature-dependent carrier state mediated by H-NS promotes the long-term coexistence of Y. pestis and a phage in soil. PLoS Pathog. 19, e1011470 (2023).
Yang, Y. et al. Development of a bacteriophage cocktail to constrain the emergence of phage-resistant Pseudomonas aeruginosa. Front. Microbiol. 11, 327 (2020).
Wu, N. et al. Pre-optimized phage therapy on secondary Acinetobacter baumannii infection in four critical COVID-19 patients. Emerg. Microbes Infect. 10, 612–618 (2021).
Cheng, M. et al. The characteristics and genome analysis of vB_ApiP_XC38, a novel phage infecting Acinetobacter pittii. Virus Genes 56, 498–507 (2020).
Strój, L., Weber-Dabrowska, B., Partyka, K., Mulczyk, M. & Wójcik, M. Successful treatment with bacteriophage in purulent cerebrospinal meningitis in a newborn. Neurol. Neurochir. Pol. 33, 693–698 (1999).
Zaldastanishvili, E. et al. Phage therapy experience at the Eliava phage therapy center: three cases of bacterial persistence. Viruses 13, 1901 (2021).
Qin, J. et al. Heterogeneous Klebsiella pneumoniae co-infections complicate personalized bacteriophage therapy. Front. Cell Infect. Microbiol. 10, 608402 (2020).
Nir-Paz, R. et al. Successful treatment of antibiotic-resistant, poly-microbial bone infection with bacteriophages and antibiotics combination. Clin. Infect. Dis. 69, 2015–2018 (2019).
Corbellino, M. et al. Eradication of a multidrug-resistant, carbapenemase-producing Klebsiella pneumoniae isolate following oral and intra-rectal therapy with a custom made, lytic bacteriophage preparation. Clin. Infect. Dis. 70, 1998–2001 (2020).
Rostkowska, O. M., Międzybrodzki, R., Miszewska-Szyszkowska, D., Górski, A. & Durlik, M. Treatment of recurrent urinary tract infections in a 60-year-old kidney transplant recipient. The use of phage therapy. Transpl. Infect. Dis. 23, e13391 (2021).
Rubalskii, E. et al. Bacteriophage therapy for critical infections related to cardiothoracic surgery. Antibiotics 9, 232 (2020).
Bao, J. et al. Non-active antibiotic and bacteriophage synergism to successfully treat recurrent urinary tract infection caused by extensively drug-resistant Klebsiella pneumoniae. Emerg. Microbes Infect. 9, 771–774 (2020).
Cano, E. J. et al. Phage therapy for limb-threatening prosthetic knee Klebsiella pneumoniae infection: case report and in vitro characterization of anti-biofilm activity. Clin. Infect. Dis. 73, e144–e151 (2021).
Doub, J. B. et al. Salphage: salvage bacteriophage therapy for a recalcitrant Klebsiella pneumoniae prosthetic shoulder infection - a case report. Acta Orthop. 93, 756–759 (2022).
Eskenazi, A. et al. Combination of pre-adapted bacteriophage therapy and antibiotics for treatment of fracture-related infection due to pandrug-resistant Klebsiella pneumoniae. Nat. Commun. 13, 302 (2022).
Le, T. et al. Therapeutic potential of intravenous phage as standalone therapy for recurrent drug-resistant urinary tract infections. Antimicrob. Agents Chemother. 67, e0003723 (2023).
Li, J. et al. Development of phage resistance in multidrug-resistant Klebsiella pneumoniae is associated with reduced virulence: a case report of a personalised phage therapy. Clin. Microbiol. Infect. 29, 1601.e1601–1601.e1607 (2023).
Acknowledgements
This study was supported by the National Natural Science Foundation of China (No. 82000726 to X.Yang), the Youth Fund of Zhongshan Hospital, Fudan University (No. 2020ZSQN48 to X.Yang), the Shanghai Municipal Key Clinical Specialty (shslczdzk02501 to X.X.), the Natural Science Foundation of Shanghai (23ZR1411200 to X.X.), and the Shanghai three-year action plan for preservation and innovative development of traditional Chinese medicine [ZY (2025-2027)-2-1-1 to X.X.].
Author information
Authors and Affiliations
Contributions
X.Yang analyzed the data and wrote the manuscript. N.W. and M.C. assisted with phage screening and synthesis. X.J., L.H., and N.L. provided support during the experiment. X.Yu participated in analyzing the data. Y.F. contributed to the clinical guidance of the patient. J.J., X.D., and X.X. designed and supervised all experiments and edited the manuscript. All authors read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Gregory German, Kārlis Rācenis, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, X., Wu, N., Jiang, X. et al. Combined bacteriophage and antibiotic therapy for refractory peritoneal dialysis-related peritonitis caused by Klebsiella pneumoniae. Nat Commun 17, 2468 (2026). https://doi.org/10.1038/s41467-026-69154-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-69154-0
