
Abstract
This single-arm, phase Ib trial evaluated the antitumor activities and safety of afuresertib (a pan AKT inhibitor) plus fulvestrant for previously treated HR-positive, HER2-negative advanced breast cancer. Eligible patients received afuresertib at 125 mg/day and fulvestrant at 500 mg on days 1, 15, and 29, and every 28 days thereafter during safety run-in and, in the absence of serious toxicities, subsequent 4-week cycles. The trial enrolled 31 patients (median age 54 years; 30 women); 20 received prior CDK4/6 inhibitor therapy. The primary endpoint of investigators-assessed objective response rate was 25.8% (8/31; 90% CI 13.5-41.8). Nine patients (29.0%) had grade 3 or worse adverse events. No death due to adverse event occurred. In conclusion, afuresertib plus fulvestrant was well-tolerated and had promising antitumor activities against pretreated, advanced HR-positive, HER2-negative breast cancer, supporting further studies with randomized controlled trials. This trial is registered with ClinicalTrials.gov (NCT04851613).
Similar content being viewed by others

Introduction
Breast cancer is the most frequently diagnosed cancer in women, with an estimated 2.3 million new cases, and the fourth leading cause of cancer mortality, with 665,684 deaths in 2022 globally1. The disease poses a serious health concern in China as well, with 357,200 estimated new cases and 75,000 deaths in China in 20222. Hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative tumors account for approximately 70% of breast cancer cases1. The current standard of care for women with HR-positive, HER2-negative, locally advanced, recurrent or metastatic disease consists of endocrine therapy, often with an aromatase inhibitor, plus a cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor. Though pivotal clinical trials have established the efficacy of CDK4/6 inhibitors (ribociclib, abemaciclib, and others)3,4,5,6,7,8, acquired CDK4/6 inhibitor resistance eventually emerges and subsequent sequential single-agent chemotherapy is associated with decreasing response rates9,10, calling for a polypharmacology approach simultaneously targeting multiple kinases or an effective molecular therapy targeting critical signaling pathways that sustain endocrine resistance in breast cancer11,12.
The phosphatidylinositol 3-kinase (PI3K)–AKT–PTEN signaling pathway plays a pivotal role in cell proliferation and survival, and metabolism in breast cancer and alterations of this pathway, including PIK3CA and AKT1 and inactivating alterations in PTEN, occur in over 50% of patients with HR-positive13,14, HER2-negative tumors15,16,17. These genetic alterations lead to aberrant signaling that is not only of significance in tumor development but also in shaping responses to breast cancer treatment, including the emergence of endocrine therapy resistance through ligand-independent activation of the estrogen receptor (ER)18,19,20, rendering the pathway an attractive therapeutic target in breast cancer. Drugs that target the upstream effectors, such as PI3Kα-subunit-specific inhibitor alpelisib and downstream effectors like mTORC1 inhibitor everolimus, improved the progression-free survival (PFS) of patients with advanced breast cancer21,22,23.
Clinical CDK4/6 inhibitor resistance converges on CDK2, a key bypass kinase of CDK4/6 inhibition11,24,25. AKT phosphorylates its downstream substrates, including CDK2 and mTOR, and regulates cell growth and apoptosis18. Pivotal clinical trial showed that targeting AKT itself, mainly through its adenosine triphosphate (ATP) binding site of PI3K and phosphorylation sites, significantly extended the PFS of patients with HR-positive advanced breast cancer. In the CAPItello-291 trial (NCT04305496)26, capivasertib (AZD5363), an orally bioavailable, pan-AKT inhibitor, extended the median PFS by 3.6 months when added to fulvestrant, with a 40% reduction in the risk of progression or death (95% confidence interval [CI], 0.51 to 0.71). Consistent PFS benefit of capivasertib plus fulvestrant over placebo plus fulvestrant was observed in the cohorts of Asian patients27,28. Capivasertib was approved by the USA FDA for use in combination with fulvestrant for the treatment of adult patients with HR-positive, HER2-negative, locally advanced or metastatic breast cancer with PIK3CA/AKT1/PTEN alterations following progression on at least one endocrine-based regimen in the context of recurrent or metastatic setting or within 12 months of completing adjuvant therapy29. AKT inhibitors appear to exhibit varying efficacies. In the IPATunity130 trial (NCT03337724), the addition of pan-AKT inhibitor ipatasertib to paclitaxel did not lead to a significant PFS benefit compared to placebo plus paclitaxel in patients with PIK3CA/AKT1/PTEN-altered, HR-positive, HER2-negative advanced breast cancer30. In the open-label phase 1b portion of the IPATunity 150 trial (NCT04060862), ipatasertib plus palbociclib and fulvestrant achieved the best overall response in 11 of 20 patients (55%) and a median PFS of 11.5 months and, based on the phase 1b results, the authors decided not to open the randomized phase 3 portion of this study31. In the BEECH trial (NCT01625286), capivasertib added to weekly paclitaxel did not extend the median PFS in the subpopulation of HR-positive, HER2-negative advanced breast cancer patients with altered PIK3CA/AKT1/PTEN32. The results of these trials provide a rationale for co-targeting estrogen receptor (ER) and PI3K pathways, which are vital for AKT inhibitor activity.
Afuresertib (GSK2110183) is an orally selective, small-molecule pan inhibitor of AKT and has broad effects on the phosphoproteome in breast cancer cells, resulting in dephosphorylation of key downstream targets33,34. It exhibits distinct mechanistic features from other AKT inhibitors33,35. Similar to capivasertib, afuresertib is an ATP-competitive AKT inhibitor that competes with ATP for binding to the active site of AKT and induces AKT hyperphosphorylation via a membrane-dependent and kinase intrinsic mechanism36. Meanwhile, phosphatidylinositol 3,4,5-trisphosphate (PIP3) analogs bind to the PIP3-cavity within the pleckstrin homology (PH) domain of AKT but suffer from poor selectivity due to the presence of structurally-related PH domains in the cell, as PIP3, a product of PI3K activity and a key signaling molecule, functions by recruiting PH domain-containing proteins to cell membranes37,38,39. As AKT plays a critical role in glucose homeostasis, high kinase selectivity of an AKT inhibitor would lead to less perturbations in glucose metabolism and lower incidences of hyperglycemia and other adverse events (AEs). Despite the implementation of an intermittent administration schedule of capivasertib in the CAPItello-291 trial, grade 3 or worse hyperglycemia occurred in 2.3% of the patients on capivasertib and 13% of the patients discontinued treatment due to AEs3. Afuresertib has the highest potency with regard to AKT1 (IC50 0.08 nM; 2.0 and 2.6 nm for AKT2 and AKT3, respectively) and has weak activities on protein kinase C isoforms (IC50 430 to >1000 nm)35, suggesting that afuresertib would have fewer off-target effects and more favorable glucose homeostasis profiles than other AKT inhibitors40,41. In preclinical models, afuresertib had overall lower IC50 values than two other ATP-competitive AKT inhibitors (capivasertib; ipatasertib) and caused G1 arrest and promoted the apoptosis of cancer cells and inhibited the growth of tumor xenografts in rats34,42,43. Apart from the inhibition of the three isoforms of AKT, afuresertib inhibits the activity of AKT1 E17K mutant (IC50 0.2 nM)35. Afuresertib also had a favorable pharmacokinetics (PK) profile, with dose-proportional exposure characteristics at doses >75 mg/day, a time to peak plasma concentration of 1.5 to 2.5 h and a terminal half-life of 1.7 days41, allowing once daily (QD) dosing. The mechanistic properties and PK profile of afuresertib provide a rationale for investigating its clinical activities in PIK3CA/AKT1/PTEN altered tumors40,41.
Here, we report the results of the phase Ib trial in the phase Ib/III LAE205INT3101 study that assessed the efficacy and safety of afuresertib plus fulvestrant in pretreated patients with HR-positive, HER2-negative advanced breast cancer with PIK3CA/AKT1/PTEN alterations which progressed during or after endocrine therapy, with or without a CDK4/6 inhibitor, or chemotherapy.
Results
Patient characteristics
Between 15 April 2022 and 27 February 2024, 45 patients were screened; 14 did not meet the inclusion criteria (nine participants) or met the exclusion criteria (five patients) and were excluded from the trial. Of 31 eligible patients who were treated, 28 (90.3%) were Asian, and 30 (96.8%) were women. The median age was 54 years (range 36.0–77.0). Eighteen (58.1%) patients were postmenopausal. Twenty (64.5%) patients had received a CDK4/6 inhibitor, 22 (71.0%) received one prior line, and nine (29.0%) received two prior lines of systemic therapy. In addition, nine (29.0%) patients had received prior chemotherapy for advanced breast cancer and 29 (93.5%) had received prior endocrine therapy. Twenty-six (83.9%) patients had visceral metastases, including liver metastases in 15 (48.4%). Eighteen (58.1%) patients had PIK3CA/AKT1/PTEN alterations, and nine (29.0%) had mutated estrogen receptor 1 (ESR1). Two patients had unknown genetic status. Among patients with mutated ESR1, seven patients with mutated ESR1 had PIK3CA/AKT1/PTEN pathway-altered tumors. Compared to the non-PIK3CA/AKT1/PTEN altered group, more patients with PIK3CA/AKT1/PTEN alterations had received prior CDK4/6 inhibitor treatment (72.2 vs. 45.5%) or had received two lines of endocrine therapy (16.7 vs. 0%). Patient demographic and baseline characteristics are shown in Table 1.
Efficacy measures
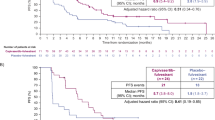
At the data cutoff (October 24, 2024), the median follow-up duration was 16.9 months (range 7.3–27.1). In the full-analysis set (FAS) that included all patients who met the eligibility criteria and enrolled in the trial, the objective response rate (ORR) assessed by investigators per response evaluation criteria in solid tumors (RECIST) version 1.1 was 25.8% (90% confidence interval CI 13.5–41.8) (Fig. 1). Eight patients had a partial response (PR), 17 patients had a stable disease (SD) and 6 had a progressive disease (PD) as their best overall response. The median duration of response was 9.1 months (95% CI 3.8-not assessable [NA]). The clinical benefit rate (CR, PR, or SD maintained ≥24 weeks) was 71.0% ([22/31]; 90% CI 54.8–83.9) (Table 2).

a Waterfall plots of the best percentage changes for the sum of target lesion diameters are shown for individual patients assessed by investigators per RECIST version 1.1. Each bar represents one patient. b Swimmer plots of time to tumor response (months) of individual patients as assessed by investigators. Each lane represents one patient. Source data are provided as a source data file.
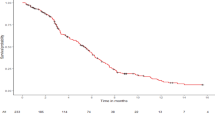
Twenty-one patients in the FAS had experienced disease progression as assessed by investigators per RECIST, version 1.1, and no patients died. The median PFS was 8.2 months (95% CI 5.6–13.6). The 6 and 12-month PFS rates were 60.8% (95% CI 43.4–78.1) and 35.8% (95% CI 16.0–55.5), respectively.
Archived or fresh biopsy tissue specimens, and/or peripheral blood samples were available from 29 patients. Eighteen patients were biomarker positive (i.e., with PIK3CA/AKT1/PTEN alterations) and 11 were biomarker negative, and the two groups were overall comparable in the baseline characteristics (Table 3). Among biomarker-positive patients, 6 (33.3% (90% CI 15.6–55.4)) had an investigator-assessed objective response. Among biomarker-negative patients, 1 (9.1% (90% CI 0.5–36.4)) had an investigator-assessed objective response. Eight patients who were biomarker positive and nine who were biomarker negative had a stable disease. The clinical benefit rate was 66.7% (90% CI 44.6–84.4) for biomarker-positive patients and 81.8% (90% CI 53.0–96.7) for biomarker-negative patients (Table 2 and Fig. 1).
At the data cutoff date, 13 and 7 PFS events had occurred in biomarker-positive and biomarker-negative patients, respectively. The median PFS was 7.3 months (95% CI 3.7–14.7) for biomarker-positive patients compared to 8.2 months (95% CI 5.4-NA) for biomarker-negative patients (Table 2). The 12-month PFS rates were 48.5% (95% CI 15.9, 81.0) for biomarker-negative patients and 25.9% (95% CI 0.3–51.5) for biomarker-positive patients, respectively. For 11 patients with PIK3CA alteration alone, the median PFS was 7.3 months (95% CI 1.9–14.7).
Current data are limited on how ESR1 mutations, which are partly responsible for endocrine resistance44, affect an AKT inhibitor added to endocrine therapy. Patients with mutated ESR1 had a numerically higher ORR compared with their wildtype counterparts (33.3% [3/9], 90% CI 9.8–65.5 vs. 20.0% [4/20], 90% CI 7.1–40.1). They also had a higher clinical benefit rate (77.8% [7/9], 90% CI 45.0–95.9 vs. 70.0% [14/20], 90% CI 49.2–86.0). Notably, three of seven patients with both mutated ESR1 and PIK3CA/AKT1/PTEN pathway alterations had an objective response (42.9%, 90% CI 12.9–77.5), and six of the patients had clinical benefit from the treatment (85.7%, 90% 47.9–99.3) (Table 4). Furthermore, they had a median PFS of 8.2 months (95% CI 5.6-NA).
Safety
The safety set included 31 patients. All patients experienced AEs of any grade, and nine (29.0%) developed AEs of grade 3 or higher. The most common AEs of any grade were hyperglycemia (51.6% [16/31]), diarrhea (45.2% [14/31]), and rash (41.9% [13/31]) (Table 5). The most frequently reported AEs of grade 3 or higher were diarrhea (9.7% [3/31]), alanine aminotransferase increased (6.5% [2/31]), aspartate aminotransferase increased (6.5% [2/31]), and gamma-glutamyl transferase increased (6.5% [2/31]). Grade 3 or higher rash occurred in one patient (3.2%) and no grade 3 or higher hyperglycemia occurred.
Serious AE (pneumonitis) occurred in one patient (3.2%). No death due to AEs occurred. AEs leading to a dose interruption occurred in 12 patients (38.7%). AEs leading to afuresertib dose reduction occurred in two patients (6.5%). No patients discontinued afuresertib or fulvestrant treatment due to AEs.
All patients experienced treatment-related AEs (TRAEs) of any grade, and 8 (25.8%) developed TRAEs of grade 3 or higher. TRAEs are described in Table 6.
Discussion
In this trial, pan-AKT inhibitor afuresertib plus fulvestrant demonstrated promising antitumor activities in patients with HR positive, HER2-negative advanced breast cancer. Approximately one quarter of the patients had an objective response to afuresertib plus fulvestrant; the response was durable, and 71.0% of the patients derived clinical benefit from the treatment (CR, PR or SD for ≥24 weeks). Afuresertib plus fulvestrant led to a median PFS of 8.2 months. Afuresertib had an overall manageable safety profile. These findings support further clinical development of afuresertib.
The CAPItello-291 trial demonstrated that the combination of capivasertib and fulvestrant significantly improved the PFS of patients with HR-positive, HER2-negative advanced breast cancer26. In this trial, the investigators-assessed ORR for afuresertib (25.8%) is comparable to that for capivasertib (22.9%). Moreover, 71.0% of our patients had clinical benefit compared to 51.3% of the patients in the CAPItello-291 trial. The median PFS for afuresertib was 8.2 months (95% CI 5.6–13.6) and is numerically higher than that for capivasertib in the overall population (7.2 months, 95% CI 5.5–7.4) and in the Chinese cohort (6.9 months, 95% 5.4–9.2)28.
Following progression on CDK4/6 inhibitor therapy, treatment choices are increasingly guided by genomic profiling. Delineation of biomarkers of activity of AKT inhibition in advanced breast cancer patients remains a research priority and allows molecular stratified treatment. This trial did not require PIK3CA/AKT1/PTEN pathway alterations as an inclusion criterion, thus allowing a population more in line with routine clinical practice and enabling assessment of afuresertib activities in patients with no pathway alterations. Biomarker-positive patients (i.e, with PIK3CA/AKT1/PTEN alterations) had a higher ORR than biomarker-negative patients (33.3 vs. 9.1%). Patients with PIK3CA/AKT1/PTEN pathway-altered tumors also had a higher ORR than the overall population in the CAPItello-291 trial26. Compared to patients with PIK3CA/AKT1/PTEN pathway-altered tumors, patients without PIK3CA/AKT1/PTEN alterations had a longer median PFS (8.2 months vs. 7.3 months). In addition, afuresertib may target beyond the PIK3CA/AKT1/PTEN pathway-altered patients. Consistent with our findings, in the Chinese cohort in the CAPItello-291 trial28, patients with PIK3CA/AKT1/PTEN pathway-altered tumors had a shorter median PFS than the patients with non-altered tumors (5.7 months, 95% CI 3.8–8.0 and 9.2 months, 95% 4.2–19.2). We tried to explore the clinical benefit of afuresertib by gene alterations and found that for 11 patients with PIK3CA alteration alone, the median PFS was 7.3 months. This data in CAPItello-291 is 5.6 months45. Both the CAPItello-291 trial and our study used next-generation sequencing for detecting PIK3CA/AKT1/PTEN alterations.
In the current study, PI3K/AKT/PTEN pathway alteration was determined only based on the alteration of PIK3CA/AKT1/PTEN genes. Elucidation of biomarkers for the activity of AKT inhibitors beyond PIK3CA/AKT1/PTEN gene alterations also helps molecularly stratified therapy of patients with advanced breast cancer. In the exploratory analysis of CAPItello-291 trial, PFS benefit was observed with capivasertib/fulvestrant treatment in patients with PTEN protein deficiency (demonstrated using PTEN immunohistochemistry), irrespectively of the PIK3CA/AKT1/PTEN gene status46. Thus, broader populations with PI3K/AKT/PTEN pathway alteration (as assessed by genetic alteration, protein level change or other biomarker status) could benefit from AKT inhibitor treatment.
In a preclinical study, ~3 μM of circulating GSK2110183 (afuresertib) (1500 ng/mL) corresponded with a 61% decrease in phospho-PRAS40, a downstream target of AKT, in tumor tissues35. However, in this trial, we did not explore whether the mechanism of action and clinical activities of afuresertib were consistent with its pharmacodynamic properties. Afuresertib, as a selective pan-AKT inhibitor, broadly affects the phosphoproteome in breast cancer cells33,35, with concentration-dependent effects on multiple AKT substrate phosphorylation levels. Pharmacodynamic analysis of afuresertib would provide insight into target engagement by afuresertib and help identify pharmacodynamic, proof-of-principle predictive biomarkers of altered PI3K/AKT pathway output following pan-AKT inhibition. Future trials should include secondary or exploratory endpoints of pharmacodynamic markers in blood and tumor tissue that may predict the outcome of pan-AKT inhibition in patients with PI3K/AKT pathway-altered tumors.
Though uncommon in untreated primary breast cancers, ESR1-mutated tumors occur in up to 40% of patients with advanced breast cancer following treatment with aromatase inhibitors44. ESR1 encodes ERα and ESR1 mutations are partly responsible for endocrine therapy resistance and may shape the response to an AKT inhibitor added to endocrine therapy44. In this phase 1b trial, patients with mutated ESR1 had a higher ORR than their wildtype counterparts (33.3 vs. 20.0%). Notably, 42.9% of the patients with both mutated ESR1 and AKT pathway alterations had an objective response, suggesting that afuresertib may also have a role in the treatment of ESR1-mutated tumors. However, given the limited size of patients with ESR1-mutated tumors, caution needs to be exercised in interpreting these results. Vepdegestrant, an oral proteolysis-targeting chimera (PROTAC) estrogen receptor (ER) degrader, and imlunestrant, a selective ER degrader, led to an ORR of 18.6 and 16.3% according to blinded independent central review in patients with ER-positive, HER2-negative, ESR1-mutated advanced breast cancer who had previously received endocrine therapy and a CDK4/6 inhibitor, respectively47,48. The PI3K-AKT-PTEN pathway is parallel to, and both downstream and upstream of ER, including through ligand-independent activation of ER49. Afuresertib could be effective in ESR1-mutated, AKT pathway-altered tumors, and a strategy may be explored for biomarker-ESR1 guided stratified therapy of advanced breast cancer.
Synergistic partnering of AKT inhibitors with targeted therapies and immune therapy may be explored as a second-line treatment of advanced disease. HR-positive, HER2-negative tumors are typically immunologically “cold” and are unresponsive to immunotherapy50. Besides, immune checkpoint inhibitors combined with CDK4/6 inhibitors led to excess toxicities51,52. Preclinical study showed that AKT inhibition resulted in a favorable immune profile in the tumor microenvironment in HR-positive, HER2-negative breast cancer tissues53. It remains to be investigated whether partnering pan-AKT inhibition with immune therapy is feasible and translates into clinical benefit. Preclinical studies showed that ESR1 mutations resulted in the generation of neoantigens in HR-positive breast cancers54, raising the intriguing possibility of targeting these antigens via immune therapy55,56. In this trial, afuresertib added to fulvestrant demonstrated antitumor activities in patients with ESR1 mutated tumors, including those with both mutated ESR1 and PIK3CA/AKT1/PTEN pathway-altered tumors. It would be of interest to explore whether afuresertib could be sequenced after or alongside drugs targeting ESR1 mutated tumors, or in the first line setting via dynamic monitoring of emerging ESR1 mutations57. Understanding resistance mechanisms by delineating specific molecular aberrations and tailoring treatment to individual patient profiles is crucial for optimizing treatment outcomes of patients with HR-positive, HER2-negative advanced breast cancer. CDK2 is a key bypass kinase of CDK4/6 inhibition and mediates clinical CDK4/6 inhibitor resistance11,24,25. In our study, 64.5% of the patients had previous exposure to a CDK4/6 inhibitor, and afuresertib demonstrated activities in this subgroup of patients, indicating progression on a CDK4/6 inhibitor does not abrogate the efficacy of afuresertib. CDK2 inhibitor development would pave the way for investigating the efficacy and safety of combined treatment.
The pattern of AEs observed with afuresertib is consistent with other PI3K/AKT pathway inhibitors and afuresertib tested in other cancer types. Hyperglycemia is a common AE with PI3K/AKT pathway inhibitors, given the prominent role of the pathway in regulating metabolism, and AKT inhibition perturbed insulin-mediated glucose homeostasis, which largely depends on PI3K signaling58. Any grade hyperglycemia occurred in 51.6% of our patients. This rate was higher than that with ipatasertib (14%) and capivasertib (16.3%) in the overall population but comparable to the Chinese cohort (57.7%)26,28,30. However, no grade 3 or higher hyperglycemia was reported with afuresertib compared to 2.3% with capivasertib (Chinese cohort 1.4%) and 2% with ipatasertib. Diarrhea was the most frequent AE with capivasertib (72.4%; grade 3 or higher 9.3%) and occurred in 45.2% of our patients (grade 3 or higher 9.7%)26. Dermatological toxicities are another consequence of PI3K/AKT pathway inhibition, as the pathway is implicated in keratinocyte differentiation and survival59. Rash occurred in 41.9% of our patients (capivasertib 38.0% in the overall population and 50.7% in the Chinese cohort), but grade 3 or higher rash was reported in only one patient (3.2%) compared to 12.0% with capivasertib (Chinese cohort 15.5%)26,28. Overall, afuresertib plus fulvestrant had a manageable toxicity profile. The rate of grade 3 or worse AEs was 29% and no treatment discontinuations occurred due to AEs, compared to 41.7% for grade 3 or worse AEs and 13.0% for AEs leading to discontinuation in patients receiving capivasertib plus fulvestrant26.
This phase 1b trial does not have a control group, limiting efficacy interpretation and generalizability. The phase 3 trial (AFFIRM-205) is ongoing. Though cross-trial comparison requires caution, afuresertib has shown promising efficacy that is comparable to capivasertib26. Patients with PI3K–AKT pathway-altered tumors may benefit from alpelisib plus fulvestrant23. Similar to capivasertib, afuresertib targets all three isoforms of AKT, downstream of PI3K, and may offer broader activities than alpelisib that targets only PIK3CA-mutated tumors. The ORR was 26.6% with alpelisib among patients with PIK3CA-mutated tumors and 24.5% with for ALK pathway-altered tumors23. Grade 3 or worse AEs occurred in 76% of the patients treated with alpelisib plus fulvestrant, including grade 3 or worse hyperglycemia in 36.6%. These results suggest that afuresertib might be preferable in patients with PIK3CA/AKT1/PTEN altered tumors or those intolerant to alpelisib. Furthermore, clinical development of afuresertib is especially relevant in regions where capivasertib access is limited or where broader and safer AKT inhibition is desired.
In conclusion, the combination of fulvestrant and afuresertib was overall tolerable and demonstrated promising antitumor activities in patients with advanced HR-positive, HER2-negative breast cancer who have previously progressed during or after endocrine therapy, with or without a CDK4/6 inhibitor, or chemotherapy. These data indicate that afuresertib is active when added to fulvestrant and support further studies in advanced clinical trials.
Methods
Trial design and patients
LAE205INT3101 is a phase Ib/III trial. The phase Ib trial, conducted at two participating centers in the USA and five participating centers in China, was a single-arm, open-label, proof-of-concept study aimed to evaluate the antitumor activities, safety, tolerability and PK of afuresertib plus fulvestrant for patients with pretreated advanced breast cancer. The PK data are to be reported separately. The phase III trial is a multicenter, randomized, double-blind, placebo-controlled study that aimed to investigate the efficacy and safety of afuresertib plus fulvestrant for patients with pretreated, HR-positive, HER2-negative, recurrent, locally advanced or metastatic breast cancer harboring gene mutations (PIK3CA, AKT1, or PTEN) in the PI3K–AKT–PTEN pathway. The phase III trial is ongoing, using the recommended dose and regimen from the phase Ib trial, and the results will be reported in a separate manuscript.
The phase Ib trial enrolled women, regardless of menopausal status, or men (≥18 years of age) with cytologically or histologically proven, HR-positive, HER2-negative recurrent, locally advanced or metastatic breast cancer. HR-positive status was defined as ER expression (≥1% based on immunohistochemical testing), with or without progesterone-receptor (PR) expression (≥1% based on immunohistochemical testing). HER2-negative status was defined as 0 or 1+ intensity on immunohistochemical testing, or 2+ intensity on immunohistochemical testing with no amplification on in situ hybridization, or in situ hybridization-negative in the absence of immunohistochemical testing according to China guidelines and the American Society of Clinical Oncology and College of American Pathologists recommendations60,61,62,63.
Patients must have received one or two prior lines of systemic therapy, including at least one line of endocrine therapy (per amended protocol, June 28, 2023), with or without a CDK4/6 inhibitor, or one line of chemotherapy and a second line of endocrine therapy for locally advanced or metastatic disease. If the disease recurred during or within 12 months following completion of adjuvant therapy, such treatment was deemed first-line therapy. Other key inclusion criteria were at least one measurable lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1), adequate bone marrow and organ function, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, fasting plasma glucose ≤167 mg/dL (≤9.3 mmol/L) and glycated hemoglobin level (HbA1c) ≤8%. Key exclusion criteria were active central nervous system metastasis or carcinomatous meningitis, prior treatment with fulvestrant, other selective ER degraders (SERDs), or any PI3K/AKT/mTOR inhibitor. Four weeks or five half-lives, whichever occurs earlier, should elapse between prior antitumor treatment and study enrollment. Men and pre- or perimenopausal women received a gonadotropin-releasing hormone agonist for continuous ovarian function suppression for the duration of the study.
The trial protocol and its subsequent amendments were approved by the ethics committee at all participating sites (listed in Supplementary Table 1) and complied with the International Ethical Guidelines for Biomedical Research Involving Human Subjects. The trial was conducted according to Good Clinical Practice guidelines and the Declaration of Helsinki. All patients provided written informed consent prior to any trial activities. The study protocol adhered to the SPIRIT statement, and the reporting of the study adhered to the CONSORT statement64,65. Trial protocol and Statistical Analysis Plan are available in the Supplementary Information file as Supplementary Notes. The trial is registered with ClinicalTrials.gov (NCT04851613).
Study intervention
The phase Ib trial used a dose non-escalation strategy for dose determination and had a safety run-in phase (cycle 1 of the first six enrolled patients) for assessing the safety of afuresertib plus fulvestrant and making necessary dose adjustments for serious treatment-related adverse events (TRAEs). During the safety run-in phase, six patients were to receive afuresertib 125 mg, given orally QD, and fulvestrant 500 mg, administered intramuscularly on days 1, 15, and 29, and every 28 days thereafter. Each cycle lasted for four weeks. In the absence of serious toxicities, the remaining patients started to receive afuresertib 125 mg QD and fulvestrant 500 mg (days 1, 15, and 29, and every 28 days thereafter). If any ≥ grade 3 TRAE occurred in one of the six patients and was not resolved within 7 days with active management per institutional standard of care, the dose of afuresertib for all patients participating in the safety run-in was reduced to 100 mg QD.
Treatment was continued until disease progression, the occurrence of intolerant toxicities, or at the discretion of the investigators. Dose reductions of afuresertib from 125 mg QD to 100 mg QD or interruptions for maximally continuous 28 days were allowed for ≥ grade 3 or higher AEs that were attributed to afuresertib or for lower grades of AEs as clinically appropriate. Reductions in the dose of fulvestrant were not allowed. Patients who discontinued fulvestrant were not allowed to continue to receive afuresertib.
Assessments
Tumors were measured by computed tomography or magnetic resonance imaging by investigators according to RECIST, version 1.1, within 28 days before study enrollment, on day 1 of cycles 3, 5, and 7, and then every three cycles from cycle 10, and within 30 days after the end of treatment and every 3 months thereafter. The initially documented CR and PR had to be confirmed at least 4 weeks apart. Hematologic and blood laboratory tests were performed within 28 days before study treatment and at day 1 of each cycle through the treatment period. HbA1c levels were assessed within 28 days before study treatment and on day 1 of the third cycle.
AEs were monitored throughout the treatment period and were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 5.0, and coded to a preferred term using the latest version of Medical Dictionary for Regulatory Activities (MedDRA). AEs, serious AEs and AEs of special interest were recorded.
Biomarker analysis
Archived tissue specimens, preferably within 18 months of study treatment, or fresh biopsy tissue specimens, and/or peripheral blood samples were acquired from patients regardless of PI3K pathway alteration status for retrospective testing of gene alterations. Activating mutations in PIK3CA, and AKT1 and inactivating alterations in PTEN genes and mutations in the ESR1 gene were determined by means of next-generation sequencing with the use of PredicineCARE assay (Predicine Inc. for samples in the USA; Huidu Shanghai Medical Sciences, Ltd for samples in China)66. PredicineCARE assay interrogates 152 key cancer genes and has an analytical sensitivity >99.99%, with a mutation detection rate of 98.0% at a limit of detection of 0.075% maximal allele frequency (MAF)67.
Endpoints
The primary endpoint of the trial was the ORR, defined as the proportion of patients who achieved CR or PR as the confirmed best overall response as assessed by investigators per RECIST, version 1.1. Secondary endpoints included duration of response, which was calculated from the first documented CR or PR to the first documented disease progression or death, whichever occurred earlier, the clinical benefit rate, which was the proportion of patients who achieved CR, PR, or SD for ≥24 weeks, PFS, which was calculated as the duration from the first dose of the study medication to radiographic disease progression or death, whichever occurred earlier, best overall response, defined as the best tumor response until disease progression or the final evaluation.
Statistical analysis
This study assumed an ORR of 25% for afuresertib plus fulvestrant, with a planned sample size of 20 participants26, which had a 91% probability of detecting ≥3 patients with an objective response. The ORR, along with its two-sided 90%CIs, was estimated using the Clopper-Pearson method. The median PFS and the corresponding 95%CI were estimated using the Kaplan–Meier method. The Center for Drug Evaluation of China National Medical Products Administration (NMPA) suggested a sample size of 30 patients for phase 1 trials in China. A final trial sample size of 30 patients was planned.
Efficacy analysis was based on the FAS that included all patients who met the eligibility criteria and enrolled in the trial. An exploratory retrospective analysis was conducted to assess the association between the antitumor activities of afuresertib plus fulvestrant and biomarkers.
The safety set included all patients who received at least one dose of afuresertib and/or fulvestrant. An independent safety review committee monitored and reviewed safety data and made decisions with regard to dose adjustment and determined whether the study could proceed to the next phase. Safety data were analyzed mainly using descriptive statistics.
Data were analyzed using SAS version 9.4 or higher (SAS Institute Inc., Cary, NC, USA).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Trial protocol and statistical analysis plan are available in the Supplementary Information file as Supplementary Notes. The de-identified participant data and targeted sequencing data are not publicly available due to data privacy laws and ethical restrictions, but will be available upon request for research purposes from the corresponding author 1 year after the publication of this article. The request should be accompanied by a research plan. A response to requests for data might be expected within 4 weeks, and the data will be available for 5 years. Source data are provided with this paper.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263 (2024).
Han, B. et al. Cancer incidence and mortality in China, 2022. J. Natl. Cancer Cent. 4, 47–53 (2024).
Turner, N. C. et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N. Engl. J. Med. 379, 926–1936 (2018).
Slamon, D. J. et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N. Engl. J. Med. 382, 514–524 (2020).
Sledge, G. W. Jr. et al. MONARCH 2: Abemaciclib in combination with fulvestrant in women with HR+/HER2-advanced breast cancer who had progressed while receiving endocrine therapy. J. Clin. Oncol. 35, 2875–2884 (2017).
Slamon, D. J. et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J. Clin. Oncol. 36, 2465–2472 (2018).
Cristofanilli, M. et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 17, 425–439 (2016).
Xu, B. et al. Dalpiciclib or placebo plus fulvestrant in hormone receptor-positive and HER2-negative advanced breast cancer: a randomized, phase 3 trial. Nat. Med. 27, 1904–1909 (2021).
Álvarez-Fernández, M. & Malumbres, M. Mechanisms of sensitivity and resistance to CDK4/6 inhibition. Cancer Cell 37, 514–529 (2020).
Lorusso, V., Latorre, A. & Giotta, F. Chemotherapy options beyond the first line in HER-negative metastatic breast cancer. J. Oncol. 2020, 9645294 (2020).
Freeman-Cook, K. et al. Expanding control of the tumor cell cycle with a CDK2/4/6 inhibitor. Cancer Cell 39, 1404–1421.e11 (2021).
Massarweh, S. & Schiff, R. Unraveling the mechanisms of endocrine resistance in breast cancer: new therapeutic opportunities. Clin. Cancer Res. 13, 1950–1954 (2007).
Manning, B. D. & Toker, A. AKT/PKB signaling: navigating the network. Cell 169, 381–405 (2017).
Lloyd, M. R., Jhaveri, K., Kalinsky, K., Bardia, A. & Wander, S. A. Precision therapeutics and emerging strategies for HR-positive metastatic breast cancer. Nat. Rev. Clin. Oncol. 21, 743–761 (2024).
Millis, S. Z., Ikeda, S., Reddy, S., Gatalica, Z. & Kurzrock, R. Landscape of phosphatidylinositol-3-kinase pathway alterations across 19784 diverse solid tumors. JAMA Oncol. 2, 1565–1573 (2016).
Cancer Genome Atlas Network Comprehensive molecular portraits of human breast tumours. Nature 490, 61–70 (2012).
Pereira, B. et al. The somatic mutation profiles of 2,433 breast cancers refines their genomic and transcriptomic landscapes. Nat. Commun. 7, 11479 (2016).
Browne, I. M., André, F., Chandarlapaty, S., Carey, L. A. & Turner, N. C. Optimal targeting of PI3K-AKT and mTOR in advanced oestrogen receptor-positive breast cancer. Lancet Oncol. 25, e139–e151 (2024).
deGraffenried, L. A. et al. Inhibition of mTOR activity restores tamoxifen response in breast cancer cells with aberrant Akt activity. Clin. Cancer Res. 10, 8059–8067 (2004).
Miller, T. W., Balko, J. M. & Arteaga, C. L. Phosphatidylinositol 3-kinase and antiestrogen resistance in breast cancer. J. Clin. Oncol. 29, 4452–4461 (2011).
Hortobagyi, G. N. et al. Correlative analysis of genetic alterations and everolimus benefit in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: Results from BOLERO-2. J. Clin. Oncol. 34, 419–426 (2016).
Baselga, J. et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 366, 520–529 (2012).
André, F. et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N. Engl. J. Med. 380, 1929–1940 (2019).
Morrison, L., Loibl, S. & Turner, N. C. The CDK4/6 inhibitor revolution - a game-changing era for breast cancer treatment. Nat. Rev. Clin. Oncol. 21, 89–105 (2024).
Gerosa, R. et al. Cyclin-dependent kinase 2 (CDK2) inhibitors and others novel CDK inhibitors (CDKi) in breast cancer: clinical trials, current impact, and future directions. Crit. Rev. Oncol. Hematol. 196, 104324 (2024).
Turner, N. C. et al. Capivasertib in hormone receptor-positive advanced breast cancer. N. Engl. J. Med. 388, 2058–2070 (2023).
Tokunaga, E. et al. Capivasertib and fulvestrant for patients with HR-positive/HER2-negative advanced breast cancer: analysis of the subgroup of patients from Japan in the phase 3 CAPItello-291 trial. Breast Cancer 32, 132–143 (2025).
Hu, X. et al. LBA5 Capivasertib (C) + fulvestrant (F) for patients (pts) with aromatase inhibitor (AI)-resistant HR+/HER2– advanced breast cancer (ABC): Phase III CAPItello-291 trial Chinese cohort. Ann. Oncol. 34, S1485–S1486 (2023).
Shirley, M. Capivasertib: first approval. Drugs 84, 337–346 (2024).
Turner, N. et al. Ipatasertib plus paclitaxel for PIK3CA/AKT1/PTEN-altered hormone receptor-positive HER2-negative advanced breast cancer: primary results from cohort B of the IPATunity130 randomized phase 3 trial. Breast Cancer Res. Treat. 191, 565–576 (2022).
Oliveira, M. et al. Abstract P5-16-11: Ipatasertib (ipat) in combination with palbociclib (palbo) and fulvestrant (fulv) in patients (pts) with hormone receptor-positive (HR+) HER2-negative advanced breast cancer (aBC). Cancer Res. 82, P5-16-11 (2022).
Turner, N. C. et al. BEECH: a dose-finding run-in followed by a randomised phase II study assessing the efficacy of AKT inhibitor capivasertib (AZD5363) combined with paclitaxel in patients with estrogen receptor-positive advanced or metastatic breast cancer, and in a PIK3CA mutant sub-population. Ann. Oncol. 30, 774–780 (2019).
Wiechmann, S. et al. Chemical phosphoproteomics sheds new light on the targets and modes of action of AKT inhibitors. ACS Chem. Biol. 16, 631–641 (2021).
Yamaji, M. et al. Novel ATP-competitive Akt inhibitor afuresertib suppresses the proliferation of malignant pleural mesothelioma cells. Cancer Med. 6, 2646–2659 (2017).
Dumble, M. et al. Discovery of novel AKT inhibitors with enhanced anti-tumor effects in combination with the MEK inhibitor. PLoS ONE 9, e100880 (2014).
Okuzumi, T. et al. Inhibitor hijacking of Akt activation. Nat. Chem. Biol. 5, 484493 (2009).
Mundi, P. S., Sachdev, J., McCourt, C. & Kalinsky, K. AKT in cancer: new molecular insights and advances in drug development. Br. J. Clin. Pharmacol. 82, 943–956 (2016).
Weisner, J. et al. Covalent-allosteric kinase inhibitors. Angew. Chem. Int. Ed. Engl. 54, 10313–10316 (2015).
Miao, B. et al. Small molecule inhibition of phosphatidylinositol-3,4,5-triphosphate (PIP3) binding to pleckstrin homology domains. Proc. Natl. Acad. Sci. USA 107, 20126–20131 (2010).
Blagden, S. P. et al. Phase IB dose escalation and expansion study of AKT inhibitor afuresertib with carboplatin and paclitaxel in recurrent platinum-resistant ovarian cancer. Clin. Cancer Res. 25, 1472–1478 (2019).
Spencer, A. et al. The novel AKT inhibitor afuresertib shows favorable safety, pharmacokinetics, and clinical activity in multiple myeloma. Blood 124, 2190–2195 (2014).
Min, B. et al. The protective mechanism of afuresertib against esophageal cancer. Dis. Markers 2022, 1832241 (2022).
Wu, J. H. et al. The novel AKT inhibitor afuresertib suppresses human Merkel cell carcinoma MKL-1 cell growth. Clin. Exp. Dermatol. 46, 1551–1554 (2021).
Brett, J. O., Spring, L. M., Bardia, A. & Wander, S. A. ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer. Breast Cancer Res. 23, 85 (2021).
Howell, S. et al. Capivasertib and fulvestrant for patients with aromatase inhibitor-resistant HR positive/HER2-negative advanced breast cancer: exploratory analysis of PFS by AKT pathway gene from the Phase 3 CAPItello-291 trial. Cancer Res. 84, PS17–03 (2024).
Jhaveri, K. et al. SABCS 2024 poster presentation: Capivasertib-fulvestrant for patients w/ HR-pos/HER2-negative advanced breast cancer who had relapsed or progressed during or after aromatase inhibitor treatment: exploratory analysis of PTEN deficiency by IHC from phase III CAPItello-291 trial.
Campone, M. et al. Vepdegestrant, a PROTAC estrogen receptor degrader, in advanced breast cancer. N. Engl. J. Med. 393, 556–568 (2025).
Jhaveri, K. L. et al. Imlunestrant with or without abemaciclib in advanced breast cancer. N. Engl. J. Med. 392, 1189–1202 (2025).
Vasan, N., Toska, E. & Scaltriti, M. Overview of the relevance of PI3K pathway in HR-positive breast cancer. Ann. Oncol. 30, x3–x11 (2019).
Harris, M. A. et al. Towards targeting the breast cancer immune microenvironment. Nat. Rev. Cancer 24, 554–577 (2024).
Masuda, J. et al. Abstract PS12-10: phase II study of nivolumab in combination with abemaciclib plus endocrine therapy in patients with HR+, HER2- metastatic breast cancer: WJOG11418B NEWFLAME trial. Cancer Res. 81, PS12–PS10 (2021).
Rugo, H. S. et al. A phase Ib study of abemaciclib in combination with pembrolizumab for patients with hormone receptor positive (HR+), human epidermal growth factor receptor 2 negative (HER2-) locally advanced or metastatic breast cancer (MBC) (NCT02779751): Interim result. J. Clin. Oncol. 38, 1051 (2020).
Andreopoulou, E. et al. Akt inhibition is associated with favorable immune profile changes within the tumor microenvironment of hormone receptor positive, HER2 negative breast cancer. Front. Oncol. 10, 968 (2020).
Lopez, M. et al. Exploring the role of ESR1 mutations in metastatic hormone receptor-positive breast cancer T cell immune surveillance disruption. Breast Cancer Res. 27, 19 (2025).
Ando, Y. et al. HLA class II-restricted T cell epitopes in public neoantigens of ESR1 and PIK3CA in breast cancer. BMC Cancer 25, 610 (2025).
Goldberg, J. et al. Estrogen receptor mutations as novel targets for immunotherapy in metastatic estrogen receptor-positive breast cancer. Cancer Res. Commun. 4, 496–504 (2024).
Bidard, F. C. et al. First-line camizestrant for emerging ESR1-mutated advanced breast cancer. N. Engl. J. Med. 393, 569–580 (2005).
Zhang, Y. et al. Molecular basis for class side effects associated with PI3K/AKT/mTOR pathway inhibitors. Expert Opin. Drug Metab. Toxicol. 15, 767–774 (2019).
Calautti, E., Li, J., Saoncella, S., Brissette, J. L. & Goetinck, P. F. Phosphoinositide 3-kinase signaling to Akt promotes keratinocyte differentiation versus death. J. Biol. Chem. 280, 32856–32865 (2005).
Yang, W. & Bu, H. Guideline for HER2 detection in breast cancer, the 2019 version. Chin. J. Pathol. 8, 169–175 (2015).
Guideline Recommendations for Immunohistochemistry Detection in Breast Cancer Group. Guideline for testing of estrogen and progesterone receptors in breast cancer. Zhonghua Bing Li Xue Za Zhi. 44, 237–239 (2015).
Wolff, A. C. et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 36, 2105–2122 (2018).
Allison, K. H. et al. Estrogen and progesterone receptor testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch. Pathol. Lab. Med. 144, 545–563 (2020).
Chan, A. W. et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann. Intern. Med. 158, 200–207 (2013).
Schulz, K. F., Altman, D. G. & Moher, D. CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 340, c332 (2010).
Predicine, Inc. PredicineCARE™ CLIA Validated Pan-cancer NGS Assay [PDF]. https://www.predicine.com/wp-content/uploads/2024/12/PredicineCARE-Flyer-APM-00001-Rev.5-13December2024.pdf (Predicine, Inc., San Carlos, 2024). Accessed August 12, 2025.
Zhang, T. et al. Development and application of an ultra-sensitive ctDNA mutation profiling assay in monitoring therapy response and drug resistance. J. Clin. Oncol. 42, 264–264 (2024).
Acknowledgements
This trial was sponsored by Laekna Therapeutics. The sponsor participated in the study design, data collection, data analysis, and results interpretation. We thank Dr. Bo Cui, MD, PHD, from the Ivy Medical Editing (Shanghai, China) for medical writing assistance.
Author information
Authors and Affiliations
Contributions
B.X., P.Z., W.M., and Y.Y. designed the study. P.Z., T.S., Y.W., W.L., Z.T., S.P., T.F., and B.X. contributed to patient enrollment and data acquisition. P.G. and M.Z. were responsible for data analysis. All authors are involved in data interpretation. The manuscript was drafted by P.Z., B.X., and W.M. and approved by all authors.
Corresponding author
Ethics declarations
Competing interests
B.X. discloses receiving advisory fees from Novartis and AstraZeneca. S.P. is a consultant and scientific advisory board member for Starling Biosciences. T.F. is a speaker for AstraZeneca, Sobi, and Sanofi and discloses receiving BeyondSpring’s support for travel. W.M., P.G., M.Z., and Y.Y. are employees of Laekna Therapeutics. The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Keyue Ding, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, P., Sun, T., Wang, Y. et al. Afuresertib plus fulvestrant for pretreated HR-positive, HER2-negative, advanced breast cancer: a phase Ib trial. Nat Commun 17, 2456 (2026). https://doi.org/10.1038/s41467-026-69225-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-69225-2
