
Abstract
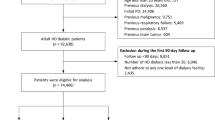
The objective of this completed, randomized, open-label trial across 11 hemodialysis centers in Shanghai, China, was to evaluate whether hemoadsorption combined with hemodialysis (HAHD) reduces mortality compared to hemodialysis (HD) alone in end-stage kidney disease patients (maintenance HD ≥ 3 months, Kt/V ≥ 1.2). We randomized 1362 patients 1:1 to receive HAHD (n = 683) or HD alone (n = 679; mainly low-flux HD plus intermittent HDF). All 1362 randomized patients were analyzed. The primary outcome was all-cause mortality, while secondary outcomes included cardiovascular mortality and major cardiovascular events. Over a median follow-up of 39.5 months, all-cause mortality occurred in 117 (17.1%) of HAHD patients compared to 144 (21.2%) of HD patients (hazard ratio [HR]: 0.778, 95% confidence interval [CI]: 0.609–0.994; P = 0.045). HAHD also significantly reduced cardiovascular mortality (HR: 0.659, 95% CI: 0.481–0.901; P = 0.009) and major cardiovascular events (HR: 0.772, 95% CI: 0.621–0.959; P = 0.019). Important adverse events, primarily infections and abnormal blood pressure, were comparable between the two groups. Adding hemoadsorption significantly reduced all-cause mortality, cardiovascular mortality, and major cardiovascular events compared to HD alone (mainly low-flux HD plus intermittent HDF). Trial Registration: ClinicalTrials.gov NCT03227770.
Similar content being viewed by others
Data availability
The study protocol, including a statistical analysis plan, is available as Supplementary Note in the Supplementary Information. The datasets generated and analyzed during the current study are not publicly available due to institutional and patient privacy regulations but are available from the corresponding author (jianggengru01@xinhuamed.com.cn) for academic research purposes one year after publication. Access is subject to approval by the Ethics Committee of Xinhua Hospital. Requests will be responded to within 20 working days. Requests for access to de-identified data will be reviewed for compliance with data sharing policies and ethical considerations, and approved data will be shared via secure transfer mechanisms. Source data containing the numerical values underlying the survival curves and forest plot are provided with this paper. Source data are provided with this paper.
References
Xie, F. et al. Design and implementation of the first nationwide, web-based Chinese Renal Data System (CNRDS). BMC Med Inf. Decis. Mak. 12, 11 (2012).
Golestaneh, L. et al. Community racial composition and hospitalization among patients receiving in-center hemodialysis. Am. J. Kidney Dis. 76, 754–764 (2020).
Stenvinkel, P., Lindholm, B., Heimburger, M. & Heimburger, O. Elevated serum levels of soluble adhesion molecules predict death in pre-dialysis patients: association with malnutrition, inflammation, and cardiovascular disease. Nephrol. Dial. Transpl. 15, 1624–1630 (2000).
Himmelfarb, J., Vanholder, R., Mehrotra, R. & Tonelli, M. The current and future landscape of dialysis. Nat. Rev. Nephrol. 16, 573–585 (2020).
Krieter, D. H., Kerwagen, S., Ruth, M., Lemke, H. D. & Wanner, C. Differences in dialysis efficacy have limited effects on protein-bound uremic toxins plasma levels over time. Toxins (Basel) 11, 47 (2019).
Ronco, C. & Clark, W. R. Haemodialysis membranes. Nat. Rev. Nephrol. 14, 394–410 (2018).
Bello, A. K. et al. Epidemiology of haemodialysis outcomes. Nat. Rev. Nephrol. 18, 378–395 (2022).
Flythe, J. E. & Watnick, S. Dialysis for chronic kidney failure: a review. JAMA 332, 1559–1573 (2024).
Ronco, C. Combined hemoperfusion-hemodialysis in end-stage renal disease patients. Contrib. Nephrol. 200, 118–122 (2023).
Bellomo, R. et al. Hemoadsorption: consensus report of the 30th Acute Disease Quality Initiative workgroup. Nephrol. Dial. Transplant. 39, 1945–1964 (2024).
Zhao, D. et al. Randomized control study on hemoperfusion combined with hemodialysis versus standard hemodialysis: effects on middle-molecular-weight toxins and uremic pruritus. Blood Purif. 51, 812–822 (2022).
Gu, Y. H. et al. Additional hemoperfusion is associated with improved overall survival and self-reported sleep disturbance in patients on hemodialysis. Int J. Artif. Organs 42, 347–353 (2019).
Li, J. et al. The effect of combination use of hemodialysis and hemoperfusion on microinflammation in elderly patients with maintenance hemodialysis. Blood Purif. 51, 739–746 (2022).
Yamamoto, Y. et al. Long-term efficacy and safety of the small-sized beta2-microglobulin adsorption column for dialysis-related amyloidosis. Ther. Apher. Dial. 15, 466–474 (2011).
Nguyen Huu, D. et al. A combination of hemodialysis with hemoperfusion helped to reduce the cardiovascular-related mortality rate after a 3-year follow-up: a pilot study in vietnam. Blood Purif. 50, 65–72 (2021).
Wang, X. F., Zhang, B. H., Lu, X. Q. & Wang, P. Efficacy of different hemodialysis methods on dendritic cell marker CD40 and CD80 and platelet activation marker CD62P and P10 in patients with chronic renal failure. J. Clin. Lab Anal. 33, e22713 (2019).
Chen, S. J. et al. Combination of maintenance hemodialysis with hemoperfusion: a safe and effective model of artificial kidney. Int J. Artif. Organs 34, 339–347 (2011).
Cheng, W. et al. Survival outcomes of hemoperfusion and hemodialysis versus hemodialysis in patients with end-stage renal disease: a systematic review and meta-analysis. Blood Purif. 51, 213–225 (2022).
Da, J. J. et al. Effect of hemoperfusion on protein energy wasting and long-term prognosis in patients on maintenance hemodialysis. Zhonghua yi xue za zhi 103, 559–565 (2023).
Sun, L., Hua, R. X., Wu, Y. & Zou, L. X. Effect of different hemodialysis modalities on hepcidin clearance in patients undergoing maintenance hemodialysis. Semin. Dial. 36, 240–246 (2023).
Zhao, D. & Shao, H. Effect of blood purification on serum miR-126 and VEGF levels in the process of atherosclerosis in uremic patients under maintenance hemodialysis. Kaohsiung J. Med. Sci. 34, 447–455 (2018).
Ramírez-Guerrero, G. et al. Efficacy of HA130 hemoadsorption in removing advanced glycation end products in maintenance hemodialysis patients. Artif. Organs 49, 900–906 (2025).
Ronco, C. & John, A. Which patient phenotype is the ideal candidate for hemoadsorption in acute and chronic kidney disease?.Integr. Med. Nephrol. Androl. 11, e00001 (2024).
Locatelli, F. et al. Effect of membrane permeability on survival of hemodialysis patients. J. Am. Soc. Nephrol. 20, 645–654 (2009).
Eknoyan, G. et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N. Engl. J. Med 347, 2010–2019 (2002).
Wang, A. Y.-M. et al. Nephrology in China. in Nephrology Worldwide (eds. Moura-Neto, J. A., Divino-Filho, J. C. & Ronco, C.) 251–290 (Springer, 2021).
Vernooij, R. W. M. et al. Haemodiafiltration versus haemodialysis for kidney failure: an individual patient data meta-analysis of randomised controlled trials. Lancet 404, 1742–1749 (2024).
Tattersall, J. E. & Ward, R. A. & group, E. Online haemodiafiltration: definition, dose quantification and safety revisited. Nephrol. Dial. Transpl. 28, 542–550 (2013).
Wang, H. et al. Cost-effectiveness analysis of hemodialysis plus hemoperfusion versus hemodialysis alone in adult patients with end-stage renal disease in China. Ann. Transl. Med. 9, 1133 (2021).
Puspitasari, M. H., Wijaya, A. R. P., Wardhani, W., Sattwika, Y. & Puspitawati, P. D. J. I. Effectiveness of combined hemodialysis-hemadsorption therapy in improving uremic toxin clearance, inflammatory markers, and symptoms in maintenance hemodialysis patients. Blood Purif. 53, 732–742 (2024).
Brendolan, A. L. et al. Hemoadsorption combined with hemodialysis and the "inflammation mitigation hypothesis". Integr. Med. Nephrol. Androl. 11, e00006 (2024).
Lu, W. & Jiang, G.-R. Randomised, open-label, multicentre trial comparing haemodialysis plus haemoperfusion versus haemodialysis alone in adult patients with end-stage renal disease (HD/HP vs HD): study protocol. BMJ Open 8, e022169 (2018).
Chen, X. M. Standard Operating Procedures for Blood Purification 78–82 (People’s Military Medical Press, Beijing, 2010).
Acknowledgements
The authors thank the study participants, trial staff, and investigators for their participation. Principal investigators at the clinical sites are listed below according to the number of patients in each site: Jianzhou Zou, Bo Shen, Zhen Zhang from Zhongshan Hospital, Fudan University; Weiming Zhang, Renhua Lu from Renji Hospital affiliated to Shanghai Jiao Tong University School of Medicine; Xiaohua Sheng from Shanghai Sixth People’s Hospital Affiliated to Shanghai JiaoTong University School of Medicine; Haiyang Wu from Shanghai Changhai Hospital; Rong Zhu from Longhua Hospital, Shanghai University of Traditional Chinese Medicine; Jiangtao Li from Tongji Hospital, School of medicine, Tongji University; Xi Chen from Yangpu Hospital, School of Medicine, Tongji University. The HAHD vs HD study was funded by a grant of Shanghai Hospital Development Center (grant No. 16CR1021A).
Author information
Authors and Affiliations
Contributions
W.L. and G.J. conceived and designed the study. W.L. and X.Z. accessed and verified the data, performed statistical analyses, and drafted the initial manuscript. H.H., G.J., Z.G., Y.D., Z.N., R.Z., N.W., C.Y., X.D., Q.Y., Y.W., and X.C. represented the coordinating centers and were responsible for patient recruitment, clinical management, and data collection. The corresponding author (G.J.) had full access to all study data and assumed final responsibility for the decision to submit the manuscript for publication. All authors critically reviewed the manuscript and approved the final version for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Gonzalo Ramírez-Guerrero, Brendan Smyth, Tom Greene, Haojin Zhou and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lu, W., Zhang, X., Guo, Z. et al. Hemoadsorption combined with hemodialysis versus hemodialysis alone on mortality in end-stage kidney disease: a randomized, open-label, multicenter trial. Nat Commun (2026). https://doi.org/10.1038/s41467-026-71079-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-026-71079-7
