
Abstract
Public health guidelines recommend 7–9 hours of regular sleep and suggest weekend catch-up sleep after weekday sleep deficits. However, real-world sleep patterns are more complex than laboratory-studied models or simple weekday-weekend cycles. Epidemiological evidence on the necessity of acute rebound after restriction remains limited. In this prospective cohort study of 85,618 UK Biobank participants (mean [standard deviation] age 61.8 [7.8] years), we analyze accelerometer-derived sleep data and identify five day-to-day sleep restriction-rebound patterns: regular sleep, sleep restriction (SR) without rebound, SR with rebound, severe SR without rebound, and severe SR with rebound. Associations with all-cause mortality are examined over a median 8.0-year follow-up. Compared to regular sleep, severe SR without rebound is associated with higher mortality risks in the overall sample and across baseline sleep duration groups. SR without rebound is linked to higher mortality overall and in short sleepers. Conversely, neither SR with rebound nor severe SR with rebound is significantly associated with mortality. Results are replicated in an independent cohort from the National Health and Nutrition Examination Survey (N = 4,586). Our findings suggest that short-term SR might be detrimental, particularly for short sleepers, and highlight acute sleep rebound as a potential strategy to mitigate mortality risk.
Similar content being viewed by others

Introduction
Previous studies examining the association between sleep and mortality have primarily focused on average sleep duration as the exposure, revealing that both short and long sleep durations are associated with higher risk for all-cause mortality, when compared to normal sleep duration1,2. These studies have led to public health recommendations for adults to sleep 7–9 h on a regular basis to maintain optimal health3,4,5,6. Moreover, given that one in four adults habitually sleep less than 7 h7, particularly during weekdays, a recent consensus statement recommended an additional 1–2 h of weekend catch-up sleep to compensate for weekday sleep deficiency8. In addition to weekday-weekend differences, recent evidence further highlights that higher day-to-day variability in sleep duration is associated with higher risk of major chronic disease and mortality9,10,11,12,13, independent of average sleep duration and sleep quality. However, the day-to-day dynamics of sleep duration changes, such as the sleep restriction-rebound patterns, are far more complex in reality and cannot be fully captured by simple patterns of weekday sleep deficiency and weekend sleep extension or by intra-individual sleep variability measures (e.g., sleep duration standard deviation [SD], sleep regularity index).
Experimental studies have demonstrated that acute sleep restriction (SR) can harm health, leading to adverse outcomes, such as neurocognitive impairments14,15, reduced glucose tolerance16, elevated inflammatory markers17, and higher cardiometabolic risks18. On the other hand, the health effects associated with sleep rebound remain unclear. Some experimental studies have reported positive health effects, such as improvements in brain functions19,20 and insulin sensitivity21, while others have found no significant benefits22,23. Similarly, epidemiological studies on weekend catch-up sleep have yielded mixed findings. While most studies have shown that weekend catch-up sleep is associated with lower risks of inflammation, depression, and obesity24,25,26, and higher levels of brain activity27, one study has reported no associations between weekend sleep rebound and mortality or cardiovascular disease (CVD)28.
Several major gaps persist in our understanding of the associations between sleep restriction-rebound patterns and mortality. First, experimental SR studies, typically conducted on animals or humans in highly controlled laboratory settings, cannot account for the complex factors—individual sleep needs, environment, and social norms—that influence real-world day-to-day human sleep patterns29,30. Likely, epidemiologic studies examining weekday-weekend sleep differences or intra-individual sleep variability measures have not adequately captured real-world sleep changes28. Second, the health impacts of sleep restriction-rebound patterns may vary by an individual’s baseline sleep duration, which we defined as one’s typical sleep length during nights not affected by restriction or rebound. For example, the health risks of acute SR may differ between individuals with habitually short sleep and those who typically get sufficient sleep. Nevertheless, prior research has not addressed this heterogeneity9,11,12. Third, some previous studies have been constrained by small sample sizes and reliance on self-reported sleep data27. These limitations underscore the need for large-scale studies using objective sleep data to assess day-to-day sleep restriction-rebound patterns and their associations with important outcomes like all-cause mortality.
In this study, we characterized the day-to-day sleep restriction-rebound patterns using accelerometer-derived sleep data from 85,618 UK Biobank participants, and investigated their prospective associations with all-cause mortality. We examined whether these associations varied by age and sex and performed a series of sensitivity tests. We also examined the associations between sleep restriction-recovery period frequencies with mortality risk. Analyses were conducted in the overall sample and within subgroups stratified by short, medium, and long baseline sleep durations. Finally, we replicated the findings using accelerometer-derived sleep data from 4586 participants in the National Health and Nutrition Examination Survey (NHANES).
Results
Descriptive characteristics
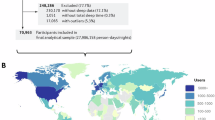
Our analyses included 574,230 person-nights of data from 85,618 UK Biobank participants with at least 3 days of valid accelerometer data collected between June 1, 2013 and December 23, 2015 (Supplementary Fig. 1). Sleep restriction-rebound patterns were identified based on notable deviations from individual sleep need, as detailed in the “Methods” and illustrated in Fig. 1. In brief, SR was defined as average cumulative sleep loss of 2.5–3.5 h across restriction periods relative to individual sleep need, while severe SR was defined as average cumulative sleep loss exceeding 3.5 h relative to individual sleep need. Sleep rebound referred to the average extra sleep more than 0 h across post-restriction periods relative to individual sleep need.

a The population of participants with valid accelerometer-derived sleep data. Icons designed by Shashank Singh on Freepik. b Illustration of one male participant with valid accelerometer-derived sleep data. Icons designed by Shashank Singh and Kanyanee Watanajitkasem on Freepik. c Definitions of sleep need and thresholds for SR and severe SR. Individual sleep need was estimated as the greater of two values: the participant’s own average sleep duration and the average sleep duration for their respective age and sex group. Thresholds for SR and severe SR were set at 2.5 and 3.5 h, respectively. d Classification of restriction, post-restriction, and baseline nights for the male participant. Restriction nights were defined as nights with sleep duration at least 2.5 h below individual sleep need. Post-restriction night was defined as the first night following each restriction period. Baseline nights were defined as nights, excluding restriction and post-restriction nights. e Calculation of average cumulative sleep loss across restriction periods. f Calculation of average extra sleep across post-restriction periods. Sleep recovery was defined as an extra sleep duration of more than 0 h relative to individual sleep need in each post-restriction period. g Calculation of average baseline sleep duration across baseline periods. h Definitions of sleep restriction-rebound patterns with corresponding real examples for each pattern. SR was defined as the average cumulative sleep loss of 2.5–3.5 h relative to individual sleep need across restriction periods. Severe SR was defined as average cumulative sleep loss exceeding 3.5 h. Sleep rebound was defined as the average extra sleep more than 0 h relative to individual sleep need across post-restriction periods. SR sleep restriction, h hours.
At the time of accelerometry, participants had a mean (SD) age of 61.8 (7.8) years, and 43.5% were male (Table 1). The mean (SD) sleep duration was 6.4 (1.0) hours across all participants. For sleep restriction-rebound patterns, participants were categorized into five groups: regular sleep (no restriction or post-restriction periods; n = 61,722; 72.1%), SR without rebound (n = 7734; 9.0%), SR with rebound (n = 7241; 8.5%), severe SR without rebound (n = 5110; 6.0%), and severe SR with rebound (n = 3811; 4.4%). Compared to those with rebound, severely sleep-restricted participants without rebound were older, more likely to be male and non-white. Socioeconomically, they were more often not employed, more deprived, and more educated. Regarding sleep patterns, they had more regular sleep and were less likely to be early chronotypes or night shift workers. In terms of other health behaviors, they were also less active, more likely to be individuals with obesity and current smokers, and less likely to drink daily. Sample characteristics stratified by sleep restriction-rebound patterns across short, medium, and long baseline sleep durations are detailed in Supplementary Tables 1–3.
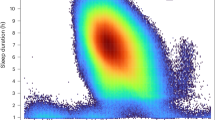
Fig. 2a–e shows the nightly sleep duration distributions in the five sleep restriction-rebound pattern groups. Compared to the regular sleep group, participants experiencing SR or severe SR (with or without rebound) showed shorter sleep durations during restriction nights. Those with sleep rebound patterns demonstrated markedly longer sleep durations during post-restriction nights compared to their baseline nights. In contrast, the regular sleep group maintained consistent sleep durations across nights. Fig. 2f shows the weekly distribution of restriction and post-restriction nights among participants experiencing SR or severe SR. Restriction nights occurred most often on weekdays only (60.9%), with fewer instances on weekends only (19.7%) and across both weekdays and weekends (19.5%). Post-restriction nights occurred most frequently on weekdays only (70.2%), followed by weekends only (20.8%), and least frequently across both weekdays and weekends (9.1%). Day-by-day analyses revealed that restriction nights were most common on Mondays (15.4%) and least common on Fridays (13.3%), whereas post-restriction nights peaked on Tuesdays (16.5%) and were least frequent on Saturdays (12.5%) (Supplementary Fig. 2).

a Regular sleepers. b Participants experiencing SR without rebound. c Participants experiencing SR with rebound. d Participants experiencing severe SR without rebound. e Participants experiencing severe SR with rebound. f Weekly distribution of restriction and post-restriction nights among participants experiencing SR or severe SR. Restriction nights were defined as nights with sleep duration at least 2.5 h below individual sleep need. Each restriction period comprised single or consecutive restriction nights. Post-restriction night was defined as the first night following each restriction period. Each post-restriction period comprised only one post-restriction night. Baseline nights were defined as nights, excluding restriction and post-restriction nights. Baseline periods included all baseline nights. SR was defined as average cumulative sleep loss of 2.5–3.5 h relative to individual sleep need across restriction periods. Severe SR was defined as average cumulative sleep loss exceeding 3.5 h. Sleep rebound was defined as average extra sleep more than 0 h relative to individual sleep need across post-restriction periods. Weekday nights included Sunday through Thursday nights, while weekend nights included Friday and Saturday nights. Source data are provided as a Source data file. SR sleep restriction.
Associations of sleep restriction-rebound patterns with mortality
Over a median follow-up of 8.0 years, 3549 deaths occurred (2240 in the regular sleep group, 415 in the SR without rebound group, 360 in the SR with rebound group, 341 in the severe SR without rebound group, and 193 in the severe SR with rebound group). Kaplan–Meier curves revealed different all-cause mortality risks for different sleep restriction-rebound patterns in the overall sample and in subsamples stratified by baseline sleep duration (Supplementary Fig. 3). In the overall sample, participants who experienced severe SR without rebound exhibited the highest cumulative risk of all-cause mortality, while those maintaining regular sleep patterns showed the lowest. Similar trends were observed in short, medium and long baseline sleep duration groups.
Cox proportional hazards regression models examined the associations of sleep restriction-rebound patterns with all-cause mortality risk in the overall sample and within baseline sleep duration subgroups, adjusting for sociodemographic and lifestyle factors (Fig. 3, Supplementary Tables 4 and 5). No significant violations of the proportional hazards assumption were observed in any of the models. In the fully adjusted Model 3, both SR without rebound and severe SR without rebound were significantly associated with higher mortality compared to regular sleep in the overall sample (hazard ratio [HR] = 1.15, 95% confidence interval [CI] = 1.01–1.31; HR = 1.42, 95% CI = 1.24–1.63, respectively). When sleep rebound occurred, neither SR nor severe SR showed significant associations with mortality, although the point estimates were above 1.0. The multivariable adjusted HRs for all-cause mortality were 1.12 (95% CI = 0.98–1.28) for participants experiencing SR with rebound and 1.13 (95% CI = 0.95–1.36) for those experiencing severe SR with rebound.

a Associations in the overall sample. Model 1 was adjusted for age, sex, and ethnicity. Model 2 additionally included employment status, education, BMI, smoking status, alcohol frequency, physical activity, night shift work, and early chronotype. Model 3 further accounted for baseline sleep duration (P values [vs. regular sleep] for SR without rebound, SR with rebound, severe SR without rebound, and severe SR with rebound, respectively: 0.030, 0.090, \(6.98\times {10}^{-7}\), and 0.169). b Associations stratified by baseline sleep duration. Models were adjusted for the same set of covariates as in Model 2 in (a). P values (vs. regular sleep) for SR without rebound, SR with rebound, severe SR without rebound, and severe SR with rebound, respectively: short (0.034, 0.628, \(1.36\times {10}^{-4}\), 0.639), medium (0.716, 0.226, 0.034, and 0.206), and long sleepers (0.564, 0.171, \(1.70\times {10}^{-3}\), 0.378). Cox proportional hazards regression models with two-sided Wald tests were used to estimate HRs for all-cause mortality. Data are presented as HRs with 95% CIs. SR was defined as average cumulative sleep loss of 2.5–3.5 h relative to individual sleep need across restriction periods. Severe SR was defined as average cumulative sleep loss exceeding 3.5 h. Sleep rebound was defined as average extra sleep more than 0 h relative to individual sleep need across post-restriction periods. Baseline sleep duration categories (short/medium/long) were defined based on the tertiles of average baseline sleep duration in 85,618 participants with sleep restriction-rebound patterns. Source data are provided as a Source data file. SR sleep restriction, HR hazard ratio, CI confidence interval, BMI body mass index, P uncorrected P value. *P < 0.05, **P < 0.01, and ***P < 0.001.
Among participants with short baseline sleep duration, both SR and severe SR without rebound were significantly associated with higher mortality risk compared to regular sleep (HR = 1.19, 95% CI = 1.01–1.40; HR = 1.38, 95% CI = 1.17–1.63, respectively). Among participants with medium and long baseline sleep durations, only the association between severe SR without rebound and mortality risk reached statistical significance (HR = 1.44, 95% CI = 1.03–2.01; HR = 1.81, 95% CI = 1.25–2.61), while all hazard ratios for SR (with and without rebound) and for severe SR with rebound were above 1.0 (Fig. 3 and Supplementary Table 5).
Age- and sex-stratified associations of sleep restriction-rebound patterns with mortality
The age- and sex-stratified results linking sleep restriction-rebound patterns to mortality are presented in Fig. 4 and Supplementary Tables 6, 7. In participants 65 years or younger from the overall sample, both SR and severe SR without rebound were associated with higher mortality risk (HR = 1.43, 95% CI = 1.13–1.79; HR = 1.35, 95% CI = 1.03–1.77), while no significant associations were found for SR or severe SR with rebound. In participants older than 65 years, severe SR without rebound was the only pattern associated with mortality risk (HR = 1.45, 95% CI = 1.24–1.71). Among short sleepers, SR without rebound was associated with higher mortality risk (HR = 1.68, 95% CI = 1.25–2.27) in those aged 65 years or younger, while severe SR without rebound was associated with higher mortality risk (HR = 1.38, 95% CI = 1.14–1.67) in those older than 65 years. Among medium duration sleepers, severe SR without rebound was associated with higher mortality risk in those older than 65 years (HR = 1.71, 95% CI = 1.15–2.54), but no associations were found in those aged 65 years or younger. Among long sleepers, severe SR without rebound was linked to mortality in both age groups, with a stronger association observed in those aged 65 years or younger (HR = 2.01, 95% CI = 1.09–3.72; HR = 1.66, 95% CI = 1.05–2.63). However, no statistically significant age interactions were observed in the overall sample or within short, medium, or long baseline sleep duration groups. These results suggest that the risk of all-cause mortality associated with sleep restriction-rebound patterns was generally similar across age groups.

a Mortality risk associations stratified by age (≤65 and >65 years). b Mortality risk associations stratified by sex (female and male). Cox proportional hazards regression models with two-sided Wald tests were adjusted for age (except age-stratified analyses), sex (except sex-stratified analyses), ethnicity, employment status, education, BMI, smoking status, alcohol frequency, physical activity, night shift work, early chronotype, and baseline sleep duration (overall sample analyses only). Data are presented as HRs with 95% CIs. SR was defined as the average cumulative sleep loss of 2.5–3.5 h relative to individual sleep need across restriction periods. Severe SR was defined as average cumulative sleep loss exceeding 3.5 h. Sleep rebound was defined as the average extra sleep more than 0 h relative to individual sleep need across post-restriction periods. Baseline sleep duration categories (short/medium/long) were defined based on the tertiles of average baseline sleep duration in 85,618 participants with sleep restriction-rebound patterns. Source data are provided as a Source data file. SR sleep restriction, HR hazard ratio, CI confidence interval, BMI body mass index.
In sex-stratified analyses (mean sleep duration: 6.5 h for women, 6.3 h for men), both women and men exhibited higher mortality risk only with severe SR without rebound, with a stronger association observed in men (HR = 1.38, 95% CI = 1.10–1.73; HR = 1.43, 95% CI = 1.21–1.71). Among short sleepers, women had elevated mortality risk with severe SR without rebound (HR = 1.36, 95% CI = 1.01–1.83), whereas men showed greater risk with both SR and severe SR without rebound (HR = 1.22, 95% CI = 1.004–1.47; HR = 1.39, 95% CI = 1.14–1.69). Among medium duration sleepers, women demonstrated higher mortality risk with SR both without and with rebound (HR = 1.48, 95% CI = 1.01–2.15; HR = 1.45, 95% CI = 1.03–2.02), and severe SR without rebound (HR = 1.81, 95% CI = 1.18–2.79), but no associations were observed in men. Among long sleepers, men showed higher mortality risk with SR with rebound and severe SR without rebound (HR = 1.42, 95% CI = 1.04–1.93; HR = 2.94, 95% CI = 1.88–4.59), while no associations were found in women. Statistically significant sex interactions were seen in the long (P for interaction = 0.015) and medium (P for interaction = 0.048) baseline sleep duration groups, though the latter showed only marginal significance. No significant interactions were observed in other groups. These findings indicate that the associations between sleep restriction-rebound patterns and mortality risk exhibited sex-specific differences, particularly among long sleepers.
Sensitivity analyses
The associations between sleep restriction-rebound patterns and mortality, using alternative thresholds to define SR, severe SR, and sleep rebound, are presented in Supplementary Figs. 4, 5, and Supplementary Tables 8–11. In the overall sample, severe SR without rebound was robustly associated with higher mortality risk across various thresholds for SR, severe SR, and sleep rebound. Similarly, SR without rebound was consistently linked to mortality risk across various thresholds for SR and sleep rebound. For example, at the 0.5-h threshold for sleep rebound (2.5 h for SR, 3.5 h for severe SR), the multivariable adjusted HRs for all-cause mortality were 1.20 (95% CI = 1.07–1.34) for SR without rebound and 1.36 (95% CI = 1.20–1.55) for severe SR without rebound. At this same threshold, the associations of both SR and severe SR with mortality were not statistically significant in the presence of sleep rebound, although point estimates were above 1.0. While minor exceptions were noted under certain thresholds for SR and severe SR, the primary findings remained consistent.
For those with short baseline sleep duration, severe SR without rebound showed an association with higher mortality risk across various thresholds for SR, severe SR, and sleep rebound. Similarly, SR without rebound was robustly linked to mortality risk across various thresholds for SR. Specifically, at the 1-h threshold for sleep rebound (2.5 h for SR, 3.5 h for severe SR), only severe SR without rebound was significantly associated with higher mortality risk compared to regular sleep (HR = 1.33, 95% CI = 1.14–1.55). For those with medium baseline sleep duration, significant associations between severe SR without rebound and mortality risk were consistently observed only at the 0.5-h and 1-h thresholds for sleep rebound (HR = 1.47, 95% CI = 1.10–1.97; HR = 1.35, 95% CI = 1.02–1.79). In participants with long baseline sleep duration, the relationship between severe SR without rebound and mortality risk remained stable across different thresholds for SR and severe SR and reached statistical significance at the 0.5-h threshold for sleep rebound (HR = 1.45, 95% CI = 1.03–2.03). Results remained robust to additional adjustments in separate models for the Townsend deprivation index (TDI), sleep duration SD, fruit and vegetable intake, history of CVD and cancer, history of depression and anxiety, and medication use. The findings also remained largely consistent when using CVD and cancer mortality as the outcomes, re-estimating sleep need based on age- and sex-specific group means, and excluding night shift workers and participants with baseline comorbidities or medication use (Supplementary Figs. 6–18 and Supplementary Tables 12–37).
Associations of sleep restriction-recovery period frequencies with mortality
Kaplan–Meier curves revealed different all-cause mortality risks for varying frequencies of sleep restriction-recovery periods in the overall sample and within subgroups stratified by baseline sleep duration (Supplementary Fig. 19). For SR periods not followed by recovery, participants who experienced two or more episodes exhibited the highest cumulative risk of all-cause mortality in the overall sample, while those with no such episodes had the lowest risk. Similar trends were observed across short, medium and long baseline sleep duration groups. For SR periods followed by recovery, participants with two or more episodes exhibited the highest cumulative risk of all-cause mortality in the overall sample, while those with no such episodes had the lowest risk. Similar trends were observed in the short baseline sleep duration group, except for the medium and long baseline sleep duration groups, where participants with one episode exhibited the highest risk, and those with none had the lowest.
Cox proportional hazards regression models were used to examine the associations between the sleep restriction-recovery period frequencies and all-cause mortality risk, both in the overall sample and within baseline sleep duration categories, adjusted for sociodemographic and lifestyle factors (Fig. 5, Supplementary Tables 38 and 39). No significant violations of the proportional hazards assumption were observed in any of the models. In the fully adjusted Model 3, both having one episode of SR without recovery (HR = 1.20, 95% CI = 1.08–1.33) and having two or more episodes (HR = 1.49, 95% CI = 1.21–1.83) were significantly associated with higher mortality risk compared to having none in the overall sample. The number of SR periods without recovery was positively associated with mortality risk (P for trend = 3.10 × 10−6). In contrast, the number of SR periods with recovery was not significantly associated with mortality (P for trend = 0.109), although the point estimates were above 1.0. The multivariable adjusted HRs for all-cause mortality were 1.10 (95% CI = 0.99–1.23) for participants with one episode and 1.02 (95% CI = 0.68–1.52) for those with two or more episodes. Among participants with short baseline sleep duration, both having one episode of SR without recovery (HR = 1.19, 95% CI = 1.04–1.36) and having two or more episodes (HR = 1.59, 95% CI = 1.27–1.99) were significantly associated with higher mortality risk compared to having none. In this group, the number of SR periods without recovery was positively associated with mortality risk (P for trend = 1.65 × 10−5), whereas the number of SR periods with recovery was not significantly related to mortality (P for trend = 0.522). Among participants with medium baseline sleep duration, no significant associations were observed. Among participants with long baseline sleep duration, only having one episode of SR without recovery (HR = 1.29, 95% CI = 1.01–1.64) showed a statistically significant association with mortality, but the linear trend was not significant (P for trend = 0.053).

These analyses quantified the number and type of restriction and post-restriction periods experienced by each participant and examined their associations with mortality risk. a Associations in the overall sample. Model 1 was adjusted for age, sex, ethnicity, and number of days of valid accelerometer wear. Model 2 additionally included employment status, education, BMI, smoking status, alcohol frequency, physical activity, night shift work, and early chronotype. Model 3 further accounted for baseline sleep duration (P values [1 and 2 vs. 0]: \(7.97\times {10}^{-4}\) and \(1.41\times {10}^{-4}\) for SR without recovery; 0.073 and 0.930 for SR with recovery). b Associations by baseline sleep duration. Models were adjusted for the same set of covariates as in Model 2 in (a). P values (1 and 2 vs. 0): for SR without recovery, short (\(9.34\times {10}^{-3}\), \(5.58\times {10}^{-5}\)), medium (0.175, 0.508), and long sleepers (0.040, 0.752); for SR with recovery, short (0.919, 0.243), medium (0.072, 0.628), and long sleepers (0.083, 0.308). Cox proportional hazards regression models with two-sided Wald tests were used to estimate HRs for all-cause mortality. Data are presented as HRs with 95% CIs. SR was defined as cumulative sleep loss of 2.5 h or more relative to individual sleep need in each restriction period, while sleep recovery was defined as an extra sleep duration of more than 0 h relative to individual sleep need in each post-restriction period. Baseline sleep duration categories (short/medium/long) were defined based on the tertiles of average baseline sleep duration in 85,618 participants with sleep restriction-rebound patterns. Source data are provided as a Source data file. SR sleep restriction, HR hazard ratio, CI confidence interval, BMI body mass index, P uncorrected P value. *P < 0.05, **P < 0.01, and ***P < 0.001.
Replication analyses in NHANES
To examine whether the associations between sleep restriction-rebound patterns and mortality were replicable in an independent cohort, we performed replication analyses using 32,260 person-nights of data from 4586 NHANES participants with at least 3 days of valid accelerometer data (Supplementary Fig. 20). Participants in NHANES had a mean (SD) age of 60.5 (10.4) years; 45.3% were male. The mean (SD) sleep duration was 7.9 (1.5) hours, notably longer than that of the UK Biobank (Supplementary Fig. 21 and Supplementary Table 40). We initially applied the same thresholds used in UK Biobank (2.5 h for SR, 3.5 h for severe SR, and 0 h for sleep rebound) to define sleep restriction-rebound patterns in NHANES. We also performed analyses using increased thresholds for both SR and severe SR (3 h for SR, 4 h for severe SR), given the differences in sleep duration distributions between NHANES and UK Biobank. In NHANES, using the same thresholds as those applied in UK Biobank, participants were categorized into five groups: regular sleep (no restriction or post-restriction periods; n = 2509; 54.7%), SR without rebound (n = 592; 12.9%), SR with rebound (n = 364; 7.9%), severe SR without rebound (n = 642; 14.0%), and severe SR with rebound (n = 479; 10.4%) (Supplementary Table 40).
Over a median follow-up of 6.8 years, 646 deaths occurred (355 in the regular sleep group, 74 in the SR without rebound group, 46 in the SR with rebound group, 105 in the severe SR without rebound group, and 66 in the severe SR with rebound group). Cox proportional hazards regression models in NHANES replicated mortality associations found in UK Biobank for sleep restriction-rebound patterns and sleep restriction-recovery period frequencies (Supplementary Figs. 22–24, Supplementary Tables 41 and 42). No significant violations of the proportional hazards assumption were observed in any of the models. Severe SR without rebound was significantly associated with higher mortality risk compared to regular sleep in the overall sample (HR = 1.41, 95% CI = 1.03–1.93) under the same thresholds used in UK Biobank. Under the second set of thresholds, both SR and severe SR without rebound (HR = 1.43, 95% CI = 1.01–2.02; HR = 1.43, 95% CI = 1.07–1.90) were significantly associated with higher mortality risk. For sleep restriction-recovery period frequencies, having one episode of SR without recovery (HR = 1.43, 95% CI = 1.08–1.89) was significantly associated with higher mortality risk only under the second set of thresholds, compared to having none. This association was supported by a significant linear trend with increasing number of SR periods without recovery (UK Biobank thresholds: P for trend = 0.037; alternative thresholds: P for trend = 0.039).
Discussion
In an era of widespread short and irregular sleep, understanding which real-world sleep patterns associate with adverse outcomes is critical. Analyzing accelerometer-derived sleep data from a large UK Biobank cohort of 85,618 adults, we found that 27.9% experienced short-term SR, with 46.3% of these participants demonstrating sleep rebound following SR. In contrast to traditional models of weekday sleep loss with weekend recovery, our findings revealed that SR and rebound occurred throughout the week. This intricacy underscores the need for a nuanced characterization of sleep restriction-rebound patterns, which our study has provided. In the overall sample, both SR and severe SR without rebound were linked to higher all-cause mortality risk. Sleep rebound appeared to attenuate these associations, suggesting that increased sleep duration following SR may buffer the adverse effects of prior sleep deprivation. Across all baseline sleep duration categories, severe SR without rebound remained broadly associated with mortality risk, whereas SR without rebound was linked to mortality risk only in short sleepers. Furthermore, the associations between sleep restriction-rebound patterns and mortality were similar across age groups but exhibited sex-specific differences. More episodes of SR without recovery were linked to higher mortality risk in the overall sample and among short and long sleepers, whereas the frequency of SR with recovery showed no association with mortality. These findings have suggested adverse health associations with SR and a potentially buffering role of acute sleep rebound. Mortality associations of sleep restriction-rebound patterns and sleep restriction-recovery period frequencies were replicated in NHANES.
Our findings that SR and its frequency were associated with higher mortality risk aligned with previous experimental studies showing detrimental health effects of SR, such as neurocognitive deficits31, reduced insulin sensitivity32, and elevated inflammatory markers17. We advance prior research by characterizing the day-to-day sleep restriction-rebound patterns and their frequencies, and uncovering more specific prospective associations with mortality risks in the overall sample and across different baseline sleep duration categories. Notably, these associations were most evident among short sleepers. The robustness of our findings was further supported by consistent results in replication analyses using data from NHANES.
The mechanisms linking SR to mortality are multifaceted and involve multiple biological pathways, including metabolic, immune, oxidative stress, and neurological processes. For instance, SR disrupts leptin and ghrelin balance, promotes food desire33, reduces insulin sensitivity, and decreases energy expenditure, leading to higher risks of diabetes and obesity34,35. In line with this pathway, we observed higher BMI levels among individuals who experienced SR or severe SR without rebound, compared to those who had rebound. Additionally, SR impairs immune function, as evidenced by weakened antibody responses to vaccines36, and increased inflammation, with higher levels of C-reactive protein17, cytokines37, and other inflammatory markers associated with cardiovascular risk18. Furthermore, in animal models, SR has been shown to contribute to premature mortality through the accumulation of reactive oxygen species in the gut38. Moreover, SR acts as a stressor that activates neuroendocrine systems and enhances their reactivity to subsequent stressors, leading to dysregulated serum glucocorticoid levels16. This dysregulation may promote chronic diseases, neuronal damage, and accelerated aging39. SR in animal models also exacerbates seizures and accelerates mortality, potentially through impaired GABAergic inhibition40, further emphasizing the neurological consequences of SR.
Prior studies have reported mixed findings regarding the health implications linked to sleep rebound. Some studies have reported positive outcomes, such as improvements in brain functions41 and insulin sensitivity21, inverse associations with depression, obesity, and cardiometabolic diseases25,26,42, whereas others have observed no significant benefits22,23. One recent study using objectively measured sleep data showed a 17% higher mortality risk among individuals with two or more hours of weekend catch-up sleep, although this association was not statistically significant28. These discrepancies may stem from two potential factors: competing mechanisms underlying sleep restriction-rebound patterns and inconsistent definitions of sleep rebound. The compensatory mechanism suggests that sleep rebound helps offset sleep loss, although it may not fully resolve accumulated sleep debt. By contrast, the circadian mechanism posits that sleep rebound could contribute to circadian disruption, since sleep restriction-rebound patterns alter the timing of the sleep-wake cycle between consecutive days. Moreover, the inconsistency in definitions of sleep rebound across studies may further complicate interpretations. Epidemiological studies have typically assessed weekend catch-up sleep (i.e., differences in sleep duration between weekdays and weekends), whereas laboratory studies have examined sleep extension following restriction. Moving beyond traditional weekday-weekend analyses, our results suggest that the compensatory pathway of sleep rebound may better account for the attenuation of SR-associated mortality risk than the circadian disruption pathway.
Sleep rebound may offer protective effects by buffering the negative health consequences of SR-induced sleep debt43. For example, sleep rebound has been shown to stabilize disruptions in carbohydrate metabolism and endocrine function caused by SR16, leading to improvements in glucose metabolism44. Additionally, it mitigates systemic inflammation primarily through the restoration of balance in the hypothalamic–pituitary–adrenal axis and sympathetic nervous system activity45, as evidenced by reductions in high-sensitivity plasma IL-646 and monocyte recruitment47.
Stratified analyses showed that the associations between sleep restriction-rebound patterns and mortality were generally similar across age groups. This finding aligned with previous studies, which have suggested no significant age-related differences in the association between short sleep duration and mortality48. As for sex-based differences, the most notable finding was that the associations between sleep restriction-rebound patterns and mortality were significantly stronger in men than in women among long sleepers. Specifically, both SR with rebound and severe SR without rebound were associated with elevated mortality risk only in men with long baseline sleep duration. This finding was consistent with some previous research showing stronger associations in men between insomnia and hypertension49, sleep disruption and cognitive decline50, as well as short sleep duration and mortality51,52. Nonetheless, given the wide confidence intervals and the issue of multiple comparisons, these subgroup findings should be considered exploratory and interpreted cautiously.
Current societal and clinical sleep-related efforts center primarily on average sleep duration, overlooking the dynamic patterns of SR and rebound in real-world settings. Our study is consistent with the hypothesis that acute sleep rebound may mitigate SR-associated mortality risks, particularly among individuals with short baseline sleep duration. In reality, some people may have to wait until weekends (or “free days”) for having the opportunity to extend their sleep; however, prior evidence indicates that weekend sleep extension does not necessarily confer health benefits, and may even be associated with adverse effects28. Collectively, these findings highlight that different patterns of catch-up sleep may have different associations with health outcomes. It is possible that extending sleep in the subsequent night(s) following SR may be preferable to deferring sleep recovery until the weekend. However, interventional studies are necessary before firm clinical recommendations can be established. It is also important to note that despite attenuated mortality risks, chronic sleep debt-rebound cycles may still exert adverse impacts on cardio-metabolic and brain health.
Our study has several strengths. We advanced beyond traditional approaches, including controlled experimental settings, weekday-weekend cycle analyses, and the intra-individual sleep variability measures, by characterizing day-to-day sleep restriction-rebound patterns that provide nuanced information on real-world sleep behaviors. By analyzing groups with different baseline sleep durations, we revealed that SR and rebound might carry distinct health implications depending on an individual’s baseline sleep duration. The large sample size of 85,618 participants from the UK Biobank, encompassing 574,230 person-nights, enhanced the reliability of our findings. The prospective study design allowed for examining longitudinal relationships between sleep restriction-rebound patterns and all-cause mortality. Accelerometer-derived sleep measurements provided objective and accurate data, minimizing self-report bias. Additionally, we performed multiple sensitivity analyses and replication analyses to ensure the robustness of the results.
However, several limitations warrant consideration when interpreting our findings. First, the UK Biobank participants were predominantly European, older, healthier, and socioeconomically advantaged53, potentially limiting generalizability. Future research could examine sleep-mortality associations in diverse populations. Nonetheless, we replicated the associations between sleep restriction-rebound patterns and their frequencies with mortality in NHANES. Second, our focus on all-cause mortality limits our ability to assess whether associations with sleep restriction-rebound patterns differ across specific disease processes. While we included CVD and cancer mortality in sensitivity analyses, future research should consider other specific causes of death and a wider range of health outcomes. Third, the accelerometer measurement period of 3–7 days might not fully capture long-term sleep patterns, potentially reflecting a temporary state rather than a habitual behavior. Although a large study of commercial wearables has suggested that average daily sleep duration and its SD remain relatively stable in adults over several years54, this brief window represents a notable limitation of our study. There is a need for extended measurement periods in future studies. Fourth, the thresholds used to define sleep restriction-rebound patterns were somewhat subjective. Nevertheless, they were grounded in experimental evidence16,55 (Supplementary Fig. 25). Moreover, our findings remained consistent across varying thresholds of SR, severe SR, and sleep rebound, supporting the robustness of our approach. Fifth, some covariates (e.g., BMI) may serve as mediating factors in the association between SR or severe SR without rebound and mortality risk. Accordingly, Models 2 and 3 may yield conservative estimates of the relationship between these exposures and mortality. Sixth, our proxy for sleep need may introduce bias by overestimating sleep need in natural short sleepers and misclassifying long sleepers with underlying morbidity as having high sleep need. We further conducted sensitivity analyses using age- and sex-specific group means to define sleep need, which yielded largely robust results. Future work should aim to further refine approaches for quantifying individual sleep needs that reflect both physiology and measurement characteristics (e.g., actigraphy, biomarkers). Seventh, the observational design precludes causal inference between sleep restriction-rebound patterns and mortality. While our findings remained consistent after additional adjustments and the exclusions of participants with baseline comorbidities or medication use, both SR and severe SR without rebound may still reflect underlying frailty rather than represent causal determinants of mortality. Finally, covariates (e.g., alcohol frequency) were assessed at a median of 5.4 years prior to accelerometry. Although these variables tend to remain stable over time56, this strategy may have introduced biases into our results.
In conclusion, our analyses of accelerometer data from 85,618 UK Biobank participants showed that SR was associated with higher mortality risk, with short sleepers being the most vulnerable. Sleep rebound appeared to attenuate these associations. These findings suggest that individuals, especially short sleepers, may benefit from two protective strategies: avoiding SR and achieving acute sleep rebound when sleep loss occurs.
Methods
Study participants
The UK Biobank has received ethical approval from the North West Multi-centre Research Ethics Committee (REC reference number 21/NW/0157), and all participants provided written informed consent at recruitment. Participants received no financial or material inducements for their contribution, though reasonable participation-related expenses, such as travel, were reimbursed. This research was conducted under UKB Resource application number 91486. To replicate findings from the UK Biobank, we utilized data from an independent cohort, NHANES (2011–2014). NHANES (2011–2014) was approved by the National Center for Health Statistics Ethics Review Board (Protocol #2011-17). Written informed consent was obtained from all NHANES participants, who also received financial compensation for their participation.
Data for the main analyses came from the UK Biobank, a prospective population-based study involving over 500,000 adults aged 40–69 years, recruited across the UK from 2006 to 201057. The initial UK Biobank sample included 502,250 participants; after excluding those who withdrew consent, 502,166 participants remained. A subsample comprising 103,720 UK Biobank participants wore a triaxial accelerometer (Axivity AX3) continuously for up to 7 days with data collected by the study team. We retrieved raw accelerometer data (data-field 90001) for 103,623 participants in the format of binary continuous wave accelerometer (cwa) files for the analyses of sleep restriction-rebound patterns.
Consistent with the approach of Jones et al.58, we applied quality control criteria to exclude participants, specifically those who (a) were recorded as having a sex mismatch or sex-chromosome aneuploidy (field 22019), (b) had cwa data problems (field 90002), poor wear time (field 90015), poor calibration (field 90016), or were unable to calibrate activity data on the device worn itself (field 90017), or (c) had number of data recording errors (field 90182), interrupted recording periods (field 90180), or duration of interrupted recoding periods (field 90181) greater than the respective variable’s 3rd quartile + 1.5 × IQR.
We further excluded participants who were recorded as having (a) short (<3 h) and long (>12 h) average sleep duration, (b) early (≤19:00) and late (≥6:00) average bed-time, (c) less than 3 days of valid accelerometer wear, (d) average cumulative sleep loss (calculated relative to individual sleep need and averaged across restriction periods) above the 99th percentile, (e) missing data on post-restriction periods despite having valid data on restriction periods, or (f) missing data on baseline periods. The final analytical sample in the UK Biobank comprised 85,618 eligible participants (Supplementary Fig. 1).
The initial NHANES sample included 19,931 participants who completed the interview. We restricted the analyses to a subsample of 5439 NHANES participants aged 45 years and older who wore an accelerometer (ActiGraph GT3X+). Similar to our approach in UK Biobank, we applied quality control criteria to exclude participants, specifically those who had (a) valid daily wear time less than 12 h, (b) short (<3 h) and long (>12 h) average sleep duration, (c) less than 3 days of valid accelerometer wear, (d) missing data on post-restriction periods despite having valid data on restriction periods, or (e) missing data on baseline periods. The final analytical sample in NHANES comprised 4586 eligible participants (Supplementary Fig. 20).
Sleep restriction-rebound patterns
In the UK Biobank, accelerometer-derived daily sleep characteristics included sleep period time (SPT), sleep duration, and sleep duration SD, each based on the daily main sleep period. These were obtained by processing raw accelerometer data for 103,623 participants using the open-source R package GGIR (version 3.0.2).
SPT was defined as the longest inactivity block (formed by non-movement bouts lasting ≥30 min and movement bouts lasting <60 min), utilizing an algorithm implemented in GGIR59. Sleep duration was calculated as the sum of sleep episodes (periods of at least 5 min with no change larger than 5° associated with the z-angle) within SPT60. In addition, sleep duration SD was calculated for individuals based on valid days of accelerometer wear.
In NHANES, the accelerometer-derived daily sleep characteristic was valid sleep time in the calendar day (midnight-to-midnight), which was estimated based on an open-source algorithm and made publicly available by NHANES61.
Interindividual differences in sleep need are well acknowledged62, yet defining it as the necessary quantity and quality of sleep for optimal neurocognitive function29 is impractical to measure for large cohorts. Natural short sleepers—those with a genetic predisposition to sleep only 4–6 h per night and still feel well-rested—are rare in the population63,64, and shorter sleep duration often reflects self-selected SR or wake extension65 rather than true need. Moreover, sleep need should be considered in the context of age and sex, as associations between sleep duration and mortality risk vary across these factors66,67. In our analyses, sleep need represents the typical sleep duration required that reflects individual habits and meets sociodemographic norms. Therefore, we estimated sleep need for each participant as the greater of two values: (1) their own average sleep duration (calculated over valid accelerometer wear days); and (2) the average sleep duration among individuals with valid accelerometer-derived sleep data in the same age and sex category as the participant. This approach leverages objective measurements to enhance reliability, corrects for individual potential sleep deficiency or outliers using population average, accounts for individual and demographic variability and reflects adaptation to environmental, cultural, psychological, and physiological factors, overcoming the operational challenges of traditional definitions. In the UK Biobank, participants were stratified into 64 groups based on 32 age categories (<45 years, ≥75 years, and 30 single-year groups from 45 to 74 years) and 2 self-reported sex categories (female and male). The number of participants in each age-sex group is displayed in Supplementary Fig. 26. In NHANES, participants were stratified into 72 groups based on 36 age categories (single-year groups from 45 to 80 years) and 2 self-reported sex categories (female and male), presented in Supplementary Fig. 27. Age patterns in sleep need from UK Biobank and NHANES were further displayed in Supplementary Figs. 28 and 29.
Next, we identified restriction, post-restriction, and baseline nights, and constructed corresponding periods across valid accelerometer wear days for each participant. We defined restriction nights as nights with sleep duration at least 2.5 h below individual sleep need. Each restriction period comprised single or consecutive restriction nights. Post-restriction night was defined as the first night following each restriction period68. Each post-restriction period comprised only one post-restriction night. Baseline nights were defined as nights excluding restriction and post-restriction nights. Baseline periods included all baseline nights. One participant could experience multiple restriction and post-restriction periods during monitoring days. Although the first night of accelerometer measurement could have been mistakenly classified as a baseline night instead of a post-restriction night due to missing data on the preceding night, the small difference in sleep duration between first night and the baseline average suggests that this possible classification error has a negligible impact on baseline sleep duration estimates (Supplementary Fig. 30). Furthermore, this scenario does not affect the SR and rebound estimates, as we accounted for paired SR and post-restriction periods.
Building on the definitions of sleep need, restriction, post-restriction, and baseline periods, we characterized participants’ sleep restriction-rebound patterns. For our main analyses, we used average cumulative sleep loss of 2.5–3.5 h relative to the participant’s sleep need to define SR and average cumulative sleep loss greater than 3.5 h relative to the participant’s sleep need to define severe SR. The rationale for selecting these thresholds was provided in Supplementary Fig. 25. Sleep rebound was defined as average extra sleep more than 0 h relative to individual sleep need across post-restriction periods. Sleep restriction-rebound patterns were categorized into five groups: regular sleep (no restriction or post-restriction periods), SR without rebound, SR with rebound, severe SR without rebound, and severe SR with rebound.
Sleep restriction-recovery period frequencies
To fully describe sleep restriction-rebound patterns, we included sleep restriction-recovery period frequencies as additional indicators, capturing the number and type of restriction and post-restriction periods experienced by each participant. SR was defined as cumulative sleep loss of at least 2.5 h relative to individual sleep need in each restriction period, while sleep recovery was defined as an extra sleep duration of more than 0 h relative to individual sleep need in each post-restriction period. Based on these definitions, we identified episodes of sleep restriction-recovery periods across valid accelerometer wear days for each participant. These episodes were classified into two types: SR without recovery, and SR with recovery. One participant could experience both types and multiple instances of such episodes during monitoring days. The frequency of sleep restriction-recovery periods was separately categorized as 0, 1, or ≥2 occurrences. Definitions of the terms were provided in Supplementary Table 43.
All-cause mortality
In the UK Biobank, mortality data were obtained from death certificates held by National Health Service (NHS) England for participants in England and Wales, and by the NHS Central Register and National Records of Scotland for participants in Scotland, up to November 30, 2022. An event was ascertained if death was recorded between the accelerometry date and the end of follow-up, with the end of follow-up defined as the earlier of the date of death or the censor date (November 30, 2022).
In NHANES, mortality status and follow-up time were extracted from the National Death Index dataset updated to December 31, 2019.
Covariates
In the UK Biobank, covariates were obtained from self-reported questionnaires closest to the accelerometer measurements. Covariates included age, sex, ethnicity (white, non-white), employment status (employed, not employed), education (no or other qualifications, college or university degree), body mass index (BMI; underweight/normal: <25 kg/m², overweight: 25–29.9 kg/m², obese: ≥30 kg/m²), smoking status (never, current, previous), alcohol frequency (occasional/never, 1–3 times per month/1–2 times per week, 3–4 times per week, daily), physical activity, night shift work (yes, no), early chronotype (yes, no), and baseline sleep duration (≤6 h, (6, 7] hours, (7, 8] hours, >8 h). For sensitivity analyses, we also accounted for TDI, sleep duration SD, fruit and vegetable intake, major chronic diseases (CVD, cancer, and diabetes), mental health disorders (depression and anxiety), medication use, and frailty status. Specifically, employment status was categorized into two groups: employed (including those in paid employment or self-employed) and not employed (all other categories except “prefer not to answer”). Physical activity was measured as weekly summed metabolic equivalent minutes for walking, moderate and vigorous activity, self-reported via the International Physical Activity Questionnaire69. Early chronotype was binary: yes (including those self-reporting as “definitely a “morning” person”, “more a “morning” than “evening” person”) and no (all other categories except “do not know” or “prefer not to answer”).
In NHANES, covariates included age, self-reported sex, ethnicity (Hispanic, non-Hispanic), employment status (employed, not employed), education (less than college education, some college or equivalent, college graduate or above), BMI (underweight/normal: <25 kg/m², overweight: 25–29.9 kg/m², obese: ≥30 kg/m²), smoking history (never, ever), drinking status (never, current, and previous), physical activity, and baseline sleep duration (≤7 h, (7, 8] hours, >8 h). For smoking history, never smokers were defined as participants who had smoked fewer than 100 cigarettes in their lifetime. Physical activity was measured as weekly summed metabolic equivalent minutes for walking or bicycling for transportation, moderate leisure-time physical activity and vigorous leisure-time physical activity.
Further details are provided in Supplementary Table 44.
Statistical analyses
Analyses were performed both in the overall sample of 85,618 participants with sleep restriction-rebound patterns and separately within each baseline sleep duration group. Short, medium, and long baseline sleep durations were defined according to tertiles of average baseline sleep duration derived from the accelerometer among 85,618 participants.
We described sample characteristics by sleep restriction-rebound patterns. We then plotted the Kaplan–Meier cumulative incidence of all-cause mortality by sleep restriction-rebound patterns. Cox proportional hazards regression models were employed to assess the longitudinal associations of sleep restriction-rebound patterns with the risk of all-cause mortality, with the regular sleep group as the reference. Continuous covariates were modeled using restricted cubic splines with three knots placed at the 10th, 50th, and 90th percentiles of their distributions. For the overall sample analyses, Model 1 was adjusted for age, sex, and ethnicity. Model 2 additionally included employment status, education, BMI, smoking status, alcohol frequency, physical activity, night shift work, and early chronotype. Model 3 further accounted for baseline sleep duration. For the baseline sleep duration stratified analyses, models were adjusted for the same covariates as in Model 2 for the overall sample. Some covariates, such as BMI, may lie on the causal pathway between sleep restriction-rebound patterns and mortality risk. Covariates with time-varying effects (non-proportional hazards) were identified using Schoenfeld residuals and modeled with time interval-specific coefficients70. Specifically, for analyses of the overall sample, time-varying coefficient for age was measured across discrete time intervals (≤1500 days, >1500 days). Stratified analyses were performed to investigate age (≤65 and >65 years) and sex (female and male) differences in the associations between sleep restriction-rebound patterns with the risk of all-cause mortality. Wald tests were used to derive two-sided P values for interaction terms with age and sex. We applied consistent model specifications when analyzing two types of sleep restriction-recovery period frequencies in relation to mortality risk, with 0 as the reference group for each type. The models additionally controlled for the number of days of valid accelerometer wear. Linear trend tests were performed by assigning the median value to each category of two sleep restriction-recovery period frequency measures, which were then modeled as separate continuous variables. The specifications for Cox proportional hazards regression models are presented in Supplementary Table 45.
We performed a series of sensitivity analyses. First, we tested alternative thresholds for SR and severe SR. For SR, we considered two conditions: (1) cumulative sleep loss relative to the participant’s sleep need, averaged across restriction periods, between 2 and 3.5 h, and (2) average cumulative sleep loss between 3 and 3.5 h. In both cases, severe SR was defined as cumulative sleep loss greater than 3.5 h relative to the participant’s sleep need, averaged across restriction periods. For severe SR, we assessed two conditions: (1) SR defined as cumulative sleep loss, averaged across restriction periods between 2.5 and 3 h, with severe SR defined as average cumulative sleep loss greater than 3 h, and (2) SR as average cumulative sleep loss between 2.5 and 4 h, with severe SR greater than 4 h. Second, we tested alternative thresholds for sleep rebound. We considered two conditions: (1) 0.5 h of average extra sleep relative to the participant’s sleep need across post-restriction periods, and (2) 1 h of average extra sleep relative to the participant’s sleep need across post-restriction periods. Third, we further adjusted for a broader range of covariates in separate models, including TDI, sleep duration SD, fruit and vegetable intake, history of CVD and cancer, history of depression and anxiety, and use of sedatives and antidepressants. Fourth, we replaced the outcome with CVD and cancer mortality. Fifth, we re-estimated sleep need using age- and sex-specific group means. Lastly, we conducted analyses on restricted samples by separately excluding: night shift workers, participants with major chronic diseases (CVD, cancer, and diabetes), participants with mental health disorders (depression and anxiety) or medication use, and frail participants. The specifications for Cox proportional hazards regression models are presented in Supplementary Table 45.
Replication analyses in NHANES
To assess the robustness of findings on associations between sleep restriction-rebound patterns and sleep restriction-recovery period frequencies with mortality, we conducted replication analyses using data from the independent NHANES dataset.
We characterized participants and estimated the cumulative incidence of all-cause mortality using Kaplan–Meier curves according to sleep restriction-rebound patterns, consistent with the approach applied in the UK Biobank. Mortality associations in the UK Biobank overall sample were repeated using Cox proportional hazards regression models. Model 1 was adjusted for age, sex, and ethnicity. Model 2 additionally included employment status, education, BMI, smoking history, drinking status, and physical activity. Model 3 further accounted for baseline sleep duration. Covariates with time-varying effects (non-proportional hazards) were identified using Schoenfeld residuals and modeled with time interval-specific coefficients70. Linear trends were tested using category medians of two sleep restriction-recovery frequency measures as separate continuous variables. Replication analyses using NHANES were weighted following the NHANES Analytic Guidelines71. The specifications for Cox proportional hazards regression models are presented in Supplementary Table 45.
All analyses were performed using R software, version 4.2.3 (https://www.r-project.org/).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data supporting the findings from this study are provided in the Supplementary Information and Source data file. The UK Biobank data are available under restricted access for eligible researchers conducting health-related research in the public interest, access can be obtained by applying at https://www.ukbiobank.ac.uk/use-our-data/apply-for-access/. Raw data are protected and not available due to data privacy laws. Access-related inquiries should be addressed to the UK Biobank Access Team (access@ukbiobank.ac.uk). Data are typically released within 15 weeks of application submission. Approved projects receive an initial 36-month access period, with extensions possible upon request. The original NHANES data used in this study are available on the NHANES website: https://www.cdc.gov/nchs/nhanes/. This study was conducted after approval by the UK Biobank under application 91486 (release date: 8 Jan 2024). Source data are provided with this paper.
Code availability
GGIR is implemented as an open-source R package available at https://github.com/wadpac/GGIR/tree/3.0-272. GGIR v3.0.2 was used to extract raw accelerometer data.
References
Liu, T.-Z. et al. Sleep duration and risk of all-cause mortality: a flexible, non-linear, meta-regression of 40 prospective cohort studies. Sleep Med. Rev. 32, 28–36 (2017).
Wang, C. et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: a study of 116 632 people from 21 countries. Eur. Heart J. 40, 1620 (2018).
Centers for Disease Control and Prevention (CDC). Unhealthy sleep-related behaviors-12 states, 2009. Morb. Mortal Wkly. Rep. 60, 233–238 (2011).
Hirshkowitz, M. et al. National sleep foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. J. Natl. Sleep Found. 1, 40–43 (2015).
Ross, R. et al. Canadian 24-hour movement guidelines for adults aged 18-64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 45, S57–S102 (2020).
Chaput, J.-P. et al. Sleep duration and health in adults: an overview of systematic reviews. Appl. Physiol. Nutr. Metab. 45, S218–S231 (2020).
Kocevska, D. et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat. Hum. Behav. 5, 113–122 (2021).
Sletten, T. L. et al. The importance of sleep regularity: a consensus statement of the National Sleep Foundation Sleep Timing and Variability Panel. Sleep Health. J. Natl. Sleep Found. 9, 801–820 (2023).
Huang, T., Mariani, S. & Redline, S. Sleep irregularity and risk of cardiovascular events: the multi-ethnic study of atherosclerosis. J. Am. Coll. Cardiol. 75, 991–999 (2020).
Chung, J. et al. Multi-dimensional sleep and mortality: the multi-ethnic study of atherosclerosis. Sleep 46, zsad048 (2023).
Windred, D. P. et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep 47, zsad253 (2024).
Kianersi, S. et al. Association between accelerometer-measured irregular sleep duration and type 2 diabetes risk: a prospective cohort study in the UK Biobank. Diabetes Care 47, 1647–1655 (2024).
Chaput, J.-P. et al. Sleep timing, sleep consistency, and health in adults: a systematic review. Appl. Physiol. Nutr. Metab. 45, S232–S247 (2020).
Shokri-Kojori, E. et al. β-amyloid accumulation in the human brain after one night of sleep deprivation. Proc. Natl. Acad. Sci. USA. 115, 4483–4488 (2018).
Krause, A. J. et al. The sleep-deprived human brain. Nat. Rev. Neurosci. 18, 404–418 (2017).
Spiegel, K., Leproult, R. & Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 354, 1435–1439 (1999).
Meier-Ewert, H. K. et al. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J. Am. Coll. Cardiol. 43, 678–683 (2004).
Tobaldini, E. et al. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat. Rev. Cardiol. 16, 213–224 (2019).
van Alphen, B., Semenza, E. R., Yap, M., van Swinderen, B. & Allada, R. A deep sleep stage in Drosophila with a functional role in waste clearance. Sci. Adv. 7, eabc2999 (2021).
Muto, V. et al. Local modulation of human brain responses by circadian rhythmicity and sleep debt. Science 353, 687–690 (2016).
Broussard, J. L., Wroblewski, K., Kilkus, J. M. & Tasali, E. Two nights of recovery sleep reverses the effects of short-term sleep restriction on diabetes risk. Diabetes Care 39, e40–e41 (2016).
Depner, C. M. et al. Ad libitum weekend recovery sleep fails to prevent metabolic dysregulation during a repeating pattern of insufficient sleep and weekend recovery sleep. Curr. Biol. 29, 957–967 (2019).
Giri, B. et al. Sleep loss diminishes hippocampal reactivation and replay. Nature https://doi.org/10.1038/s41586-024-07538-2 (2024).
Han, K.-M., Lee, H.-J., Kim, L. & Yoon, H.-K. Association between weekend catch-up sleep and high-sensitivity C-reactive protein levels in adults: a population-based study. Sleep 43, zsaa010 (2020).
Liu, Y., Yin, J., Li, X., Yang, J. & Liu, Y. Examining the connection between weekend catch-up sleep and depression: insights from 2017 to 2020 NHANES information. J. Affect Disord. 358, 61–69 (2024).
Im, H.-J. et al. Association between weekend catch-up sleep and lower body mass: population-based study. Sleep 40, zsx089 (2017).
Zhang, R. et al. Sleep inconsistency between weekends and weekdays is associated with changes in brain function during task and rest. Sleep 43, zsaa076 (2020).
Chaput, J.-P. et al. Device-measured weekend catch-up sleep, mortality, and cardiovascular disease incidence in adults. Sleep https://doi.org/10.1093/sleep/zsae135 (2024).
Fjell, A. M. & Walhovd, K. B. Individual sleep need is flexible and dynamically related to cognitive function. Nat. Hum. Behav. 8, 422–430 (2024).
Zhang, S. et al. Health risks and genetic architecture of objectively measured multidimensional sleep health. Nat. Commun. 16, 7026 (2025).
Vecsey, C. G. et al. Sleep deprivation impairs cAMP signalling in the hippocampus. Nature 461, 1122–1125 (2009).
Donga, E. et al. Partial sleep restriction decreases insulin sensitivity in type 1 diabetes. Diabetes Care 33, 1573–1577 (2010).
Greer, S. M., Goldstein, A. N. & Walker, M. P. The impact of sleep deprivation on food desire in the human brain. Nat. Commun. 4, 2259 (2013).
Spiegel, K., Tasali, E., Penev, P. & Van Cauter, E. Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 141, 846–850 (2004).
Knutson, K. L., Spiegel, K., Penev, P. & Van Cauter, E. The metabolic consequences of sleep deprivation. Sleep Med. Rev. 11, 163–178 (2007).
Spiegel, K., Sheridan, J. F. & Van Cauter, E. Effect of sleep deprivation on response to immunizaton. JAMA 288, 1471–1472 (2002).
Sang, D. et al. Prolonged sleep deprivation induces a cytokine-storm-like syndrome in mammals. Cell 186, 5500–5516 (2023).
Vaccaro, A. et al. Sleep loss can cause death through accumulation of reactive oxygen species in the gut. Cell 181, 1307–1328 (2020).
Meerlo, P., Sgoifo, A. & Suchecki, D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med. Rev. 12, 197–210 (2008).
Konduru, S. S. et al. Sleep deprivation exacerbates seizures and diminishes GABAergic tonic inhibition. Ann. Neurol. 90, 840–844 (2021).
Xu, Y., Schneider, A., Wessel, R. & Hengen, K. B. Sleep restores an optimal computational regime in cortical networks. Nat. Neurosci. 27, 328–338 (2024).
Kim, D. J. et al. Beneficial effects of weekend catch-up sleep on metabolic syndrome in chronic short sleepers. Sleep Med. 76, 26–32 (2020).
Kleitman, N. Sleep and Wakefulness (University of Chicago Press, 1987).
Buxton, O. M. et al. Adverse metabolic consequences in humans of prolonged sleep restriction combined with circadian disruption. Sci. Transl. Med. 4, 129ra43 (2012).
Irwin, M. R. Sleep and inflammation: partners in sickness and in health. Nat. Rev. Immunol. 19, 702–715 (2019).
McAlpine, C. S. et al. Sleep exerts lasting effects on hematopoietic stem cell function and diversity. J. Exp. Med. 219, e20220081 (2022).
Huynh, P. et al. Myocardial infarction augments sleep to limit cardiac inflammation and damage. Nature 635, 168–177 (2024).
Cappuccio, F. P., D’Elia, L., Strazzullo, P. & Miller, M. A. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep 33, 585–592 (2010).
Li, X. et al. Associations of sleep-disordered breathing and insomnia with incident hypertension and diabetes. The Hispanic community health study/study of Latinos. Am. J. Respir. Crit. Care Med. 203, 356–365 (2021).
McSorley, V. E., Bin, Y. S. & Lauderdale, D. S. Associations of sleep characteristics with cognitive function and decline among older adults. Am. J. Epidemiol. 188, 1066–1075 (2019).
Shankar, A., Koh, W.-P., Yuan, J.-M., Lee, H.-P. & Yu, M. C. Sleep duration and coronary heart disease mortality among Chinese adults in Singapore: a population-based cohort study. Am. J. Epidemiol. 168, 1367–1373 (2008).
Hublin, C., Partinen, M., Koskenvuo, M. & Kaprio, J. Sleep and mortality: a population-based 22-year follow-up study. Sleep 30, 1245–1253 (2007).
Fry, A. et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am. J. Epidemiol. 186, 1026–1034 (2017).
Zheng, N. S. et al. Sleep patterns and risk of chronic disease as measured by long-term monitoring with commercial wearable devices in the All of Us Research Program. Nat. Med. 30, 2648–2656 (2024).
Covassin, N. et al. Effects of experimental sleep restriction on energy intake, energy expenditure, and visceral obesity. J. Am. Coll. Cardiol. 79, 1254–1265 (2022).
Strain, T. et al. Wearable-device-measured physical activity and future health risk. Nat. Med. 26, 1385–1391 (2020).
Sudlow, C. et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12, e1001779 (2015).
Jones, S. E. et al. Genetic studies of accelerometer-based sleep measures yield new insights into human sleep behaviour. Nat. Commun. 10, 1585 (2019).
van Hees, V. T. et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci. Rep. 8, 12975 (2018).
van Hees, V. T. et al. A novel, open access method to assess sleep duration using a wrist-worn accelerometer. PLoS ONE 10, e0142533 (2015).
National Center for Health Statistics. NHANES 2013–2014 Data Documentation, Codebook and Frequencies: Physical Activity Monitor (PAXDAY_H), https://wwwn.cdc.gov/Nchs/Data/Nhanes/Public/2013/DataFiles/PAXDAY_H.htm (2020).
Van Dongen, H. P. A., Vitellaro, K. M. & Dinges, D. F. Individual differences in adult human sleep and wakefulness: leitmotif for a research agenda. Sleep 28, 479–496 (2005).
He, Y. et al. The transcriptional repressor DEC2 regulates sleep length in mammals. Science 325, 866–870 (2009).
Shi, G. et al. A rare mutation of β1-adrenergic receptor affects sleep/wake behaviors. Neuron 103, 1044 (2019).
Klerman, E. B. & Dijk, D.-J. Interindividual variation in sleep duration and its association with sleep debt in young adults. Sleep 28, 1253–1259 (2005).
Svensson, T. et al. Association of sleep duration with all- and major-cause mortality among adults in Japan, China, Singapore, and Korea. JAMA Netw. Open 4, e2122837 (2021).
Lok, R., Qian, J. & Chellappa, S. L. Sex differences in sleep, circadian rhythms, and metabolism: implications for precision medicine. Sleep Med. Rev. 75, 101926 (2024).
Dubowy, C. et al. Genetic dissociation of daily sleep and sleep following thermogenetic sleep deprivation in Drosophila. Sleep 39, 1083–1095 (2016).
Guo, W., Bradbury, K. E., Reeves, G. K. & Key, T. J. Physical activity in relation to body size and composition in women in UK Biobank. Ann. Epidemiol. 25, 406–413 (2015).
Therneau, T. M. & Grambsch, P. M. Modeling Survival Data: Extending the Cox Model, https://doi.org/10.1007/978-1-4757-3294-8 (Springer, 2000).
Chen, T.-C. et al. National Health and Nutrition Examination Survey: estimation procedures, 2011-2014. Vital Health Stat. 2, 1–26 (2018).
van Hees, V. & Migueles, J. H. GGIR. Zenodo https://doi.org/10.5281/zenodo.10372684 (2023).
Acknowledgements
This study uses the UK Biobank Resource under application ID 91486. We thank all participants and researchers from the UK Biobank and NHANES for their valuable contributions. We would like to acknowledge Freepik (https://www.freepik.com/) for the icons used in our illustrations. Specifically, the icons for women and men in Fig. 1a and the participant in Fig. 1b were created by Shashank Singh, while the accelerometer icon in Fig. 1b was created by Kanyanee Watanajitkasem.
Author information
Authors and Affiliations
Contributions
X.Y.L., M.R.Z. designed the study. M.R.Z., Z.Y.L., S.K.Z., and X.Y.L. developed the definition of sleep restriction-rebound patterns. S.R., M.K.R., T.Y.H., and S.M.B. provided critical feedback. M.R.Z., X.Y.L. conducted the analyses, drafted the manuscript, and revised it according to the co-authors’ suggestions. All authors critically reviewed the manuscript and approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare the following competing interests: M.K.R. reports consulting for Eli Lilly and modest stock ownership in GSK, both unrelated to the submitted work. S.R. reports consulting for Eli Lilly; she serves as editor-in-chief of sleep health and is an unpaid board member of the National Sleep Foundation and Alliance of Sleep Apnea Partners. The other authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Jean-Philippe Chaput; Monica Andersen and Sergio Tufik for their contribution to the peer review of this work. [A peer review file is available].
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Zhang, M., Li, Z. et al. Acute sleep rebound following sleep restriction is associated with reduced mortality risk. Nat Commun 17, 3820 (2026). https://doi.org/10.1038/s41467-026-72461-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-72461-1
