
Abstract
Vegetarian diets are increasingly popular worldwide, but their impact on healthy aging in older adults remains unclear. This study examined the association between vegetarian diets and healthy aging among 2,888 healthy older Chinese adults from the Chinese Longitudinal Healthy Longevity Survey. Dietary patterns (vegan, ovo-vegetarian, pesco-vegetarian, omnivorous) were derived from a simplified non-quantitative food frequency questionnaire. Over a median follow-up of 6 years, after accounting for sociodemographic and lifestyle factors, vegetarians had lower odds of achieving healthy aging compared to omnivores (adjusted OR = 0.65, 95% CI: 0.47-0.89), with consistent results across sensitivity analyses and individual health components. Additionally, the health effects of vegetarian diets may vary depending on diet quality, with vegetarians of higher diet quality not significantly differing in terms of overall healthy aging and individual outcomes when compared to omnivores. Accordingly, this finding highlights modest inclusion of animal-based foods may improve the overall health status of healthy older adults.
Similar content being viewed by others

Introduction
Vegetarian diets, defined as dietary patterns solely/mostly composed of plant-based foods, excluding specific or all animal-derived foods from the diet, have become increasingly popular1,2. Several studies have shown that vegetarian diets were associated with lower risks of developing cardiovascular diseases (CVDs), obesity, diabetes, and cancer in young and middle-aged adults3,4. Furthermore, vegetarian diets have been recognized for their benefits in mitigating conditions such as metabolic syndrome, obesity, and hyperlipidemia5. However, few studies have examined the potential health outcomes of vegetarian diets in older adults – a vulnerable group at risk of malnutrition when following a strict vegetarian diet due to the potential inadequate intakes of protein, vitamin B12, calcium, iron, and essential omega-3 fatty acids3. Given age-related physiological changes in digestive and metabolic systems among older adults, vegetarian diets may result in muscle loss and bone fracture, key contributors to physical disability6,7,8. Additionally, evidence regarding the associations between vegetarian diets and other health outcomes, such as mortality, major chronic diseases, cognitive function, and mental health in older adults, is scarce and remains controversial9,10,11. In this context, comprehensively examining the potential impact of vegetarian diets on overall health, especially among older adults, has important clinical and public health implications. Approaches to achieve healthy aging – commonly defined as maintaining disease-free and physically, mentally, and cognitively healthy – are urgently needed, particularly given the low prevalence of healthy aging, which range from 10% to 35% among older adults12,13,14. Identifying modifiable lifestyle factors for healthy aging can help to develop feasible intervention strategies to promote this outcome.
Here, incorporating the definition of healthy aging12,13,15, we leveraged longitudinal follow-up data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) to examine associations between vegetarian diets (including vegan, ovo-vegetarian diet, and pesco-vegetarian diet) and healthy aging, defined as survival to at least 80 years of age with no major chronic diseases (i.e., diabetes, CVDs, stroke, chronic respiratory disease, cancer and hypertension), and no impairment of physical function, cognitive function or mental health. To assess the quality of plant-based foods, we also examined the potential joint effects of vegetarian diets and healthy vs. unhealthy plant-based diet indices (based on the quality of plant-based foods).
Results
Study characteristics
The mean age of participants was 72.1 ± 4.35 years and 55.0% were male. Those who committed to the vegetarian diets tended to be female, of the Han ethnic group, with lower income level, and lower education level (Table 1), compared to omnivores.
Vegerarian diets and healthy aging
During a median follow-up period of 6 years, 572 of the 2888 participants met the criteria for healthy aging. Compared to omnivores, vegetarians were less likely to achieve healthy aging, with a multivariable-adjusted odds ratio (OR) of 0.65 (95% confidence interval [CI]: 0.47–0.89). Furthermore, the OR for vegans was 0.43 (95% CI: 0.21–0.89) compared to omnivores (Table 2).
Dietary pattern changes and healthy aging
Based on dietary pattern change from age 60 years to the study baseline, the multivariable-adjusted OR for those consistently adhering to omnivore diets was 1.78 (95% CI: 1.20–2.64), compared to participants consistently adhering to vegetarian diets. For those who shifted from vegetarian to omnivore diets, the OR decreased to 1.54 (95% CI: 0.98–2.41) (Table 3).
Individual components analyses
In the analysis of individual components of healthy aging among participants who survived to age 80 years (n = 1582), vegetarians were more likely to have major chronic disease (adjusted OR: 1.60, 95% CI: 1.17–2.18), physical function impairment (adjusted OR: 1.95, 95% CI: 1.25–3.04), and cognitive impairment (adjusted OR 2.05, 95% CI: 1.26–3.33) (Table 4). Additionally, a dose-response relationship was observed across the vegetarian diets (vegan and ovo-vegetarian), and the number of unmet healthy aging criteria (0-4) (P-trend <0.05 for all). Likewise, those adhering to vegetarian diets since 60 years of age had higher risks of major chronic diseases and physical and cognitive impairment (Table 4).
Subgroup analyses
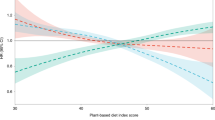
No direct associations were observed between the hPDI or uPDI and the likelihood of achieving healthy aging (Supplementary Table 3). However, vegetarians with high uPDI had an adjusted OR of 0.56 (95% CI: 0.37–0.84) for healthy aging, compared to low-uPDI omnivores. Similarly, compared to high-hPDI omnivores, vegetarians with low hPDI had a multi-adjusted OR of 0.54 (95% CI: 0.30–0.97) for achieving healthy aging (Table 5). There was no significant association between low-uPDI vegetarians and high-hPDI vegetarians and healthy aging, compared to their counterparts (Table 5). For the analysis of those individual healthy aging components, compared to low-uPDI omnivores, high-uPDI Vegetarians were more likely to to have major chronic disease (adjusted OR: 1.74, 95% CI: 1.20–2.52), physical function impairment (adjusted OR: 2.69, 95% CI: 1.59–4.57), and cognitive impairment (adjusted OR 3.00, 95% CI: 1.69–5.34). Likewise, the same pattern were also shown for those low-hPDI vegetarians. Additionally, a dose-response relationship was observed across the high-uPDI vegetarians and low-hPDI vegetarians, and the number of unmet healthy aging criteria (0-4) (P-trend <0.05 for all) (Supplementary Table 4).
Sensitivity analyses
The robustness of the observed associations in our main analysis was confirmed in sensitivity analyses (Supplementary Table 5). After excluding participants who had been followed for < 2 years and <5 years, respectively, associations were slightly attenuated but remained significant. Similar associations were observed when additionally adjusting for religion activities, redefining the criteria for healthy aging by modifying the cut-offs for the MMSE score and psychological well-being index, and by using Cox hazard regression models.
Discussion
In this large, prospective cohort study of healthy Chinese older adults, vegetarian diets, particularly vegan diets, were independently associated with lower likelihood of achieving healthy aging. Individuals who maintained omnivorous diets from age 60 years had higher odds of achieving healthy aging, compared to those who consistently followed vegetarian diets. Additionally, the heath impact of vegetarian diets may vary depending on diet quality, as our results indicated that vegetarians with higher diet quality did not significantly differ in terms of healthy aging outcomes compared to omnivores. To the best of our knowledge, this is the first prospective cohort study to investigate the association between vegetarian diets and overall health status among healthy older adults, indicating that adherence to vegetarian diets may not invariably confer the anticipated health benefits within this demographic. Accordingly, this finding highlights the need for a balanced and flexible dietary strategy that incorporates an appropriate amount of animal products, to optimize the health status of healthy older adults.
Existing studies on the health effects of vegetarian diets remain controversial, with much of the research focusing on middle-aged adults and showing heterogeneous findings regarding mortality, major chronic diseases, physical function, and mental health9,11,16,17,18,19. For example, the Adventist studies from the US showed an association between vegetarian diet and lower risks of all-cause mortality and cardiovascular diseases10,18. In contrast, the EPIC-Oxford (UK) and “45 and Up” (Australia) Study failed to find the same associations17,20. However, these studies were conducted in Western countries and focused on specific diseases/outcomes without examining the overall health impact of vegetarian diets on older adults. Of note, prior studies did not account for the diet quality within vegetarian patterns, which may partly explain the inconsistent findings regarding the health effects of vegetarian diets.
We found that vegetarian diets were associated with impaired physical function, consistent with previous research8,21,22. It is well documented that vegetarian diets may expose older adults to potential nutritional deficiencies. For instance, previous studies demonstrated that vegetarians were at an increased risk of experiencing hip fracture, compared to omnivores23. Despite supplementation with vitamin D and calcium, vegetarians exhibited poorer bone health, as measured by calcaneal quantitative ultrasound, compared to omnivores22. Similarly, the risk of sarcopenia may be increased among older adults adhering to vegetarian diets, due to the lower bioavailability and quality of plant-based proteins, which were lower in essential amino acids8.
We found that vegetarian diets were associated with higher odds of cognitive impairment at the age of 80 years. To date, research on vegetarian diets and cognitive impairment has yielded inconsistent conclusions9. Vegetarian diets, being low in saturated fats and cholesterol, have been associated with healthier blood lipid profiles, and they are rich in vitamins, antioxidants, and dietary fiber, potentially offering some protection against cognitive decline9,24. However, these diets may lack specific micronutrients, potentially leading to deficiencies in vitamin B12, vitamin D, and docosahexaenoic Acid (DHA) – which are essential for cognitive health25,26,27. Future studies on vegetarian diets and cognitive impairment should expolore supplementation with specific micronutrients to optimize potential benefits.
In our analysis, no significant associations were observed between vegetarian diets and mental health, aligning with the varied findings of existing observational studies on this topic. While several large cross-sectional studies reported higher occurrence of depressive symptoms among vegetarians, compared to non-vegetarians28,29, one study found a beneficial association between vegan diets and improved mood disturbances28. This inconsistency underscores the need for further investigation.
Our analysis revealed that older adults who consumed vegetarian diets and had poor diet quality, as suggested by lower hPDI scores or higher uPDI scores, had lower odds of achieving healthy aging, and were more likely to experience major chronic diseases, physical function impairments, and cognitive decline, compared to their counterparts with better diet quality. Importantly, the high hPDI and low uPDI vegetarian groups did not exhibit a significantly higher risk of unhealthy aging compared to their counterparts, indicating that a healthier diet overall, regardless of being vegetarian or omnivore, may play a more significant role in promoting healthy aging. These findings highlight the importance of prioritizing overall diet quality even within plant-based dietary patterns. Our results are broadly consistent with previous research that identified associations between lower hPDI / higher uPDI and increased risks of mortality30 and several major chronic diseases31,32,33,34.
The adverse health effect for healthy aging in older adults may be explained by several mechanisms. One explanation could be the higher risk of nutritional deficiencies associated with vegetarian diets in this population, which were essential for maintaining muscle mass, bone health, and cognitive function3,6. Age-related physiological changes, such as reduced nutrient absorption, may exacerbate these risks. Notably, protein intake plays a critical role. In our study, older adults following a vegan diet were most strongly associated with adverse effects on healthy aging, compared to those adhering to ovo-vegetarian or pesco-vegetarian diets. Research showed that nearly half of older adults failed to meet the recommended dietary allowance for protein, with primary sources of dietary protein being meat, eggs, dairy, and cereals35,36. Vegan diets may increase the risk of protein deficiency due to the lower protein density and suboptimal essential amino acid profiles of plant-based foods. Furthermore, plant proteins are generally of lower quality compared to animal proteins, potentially exacerbating age-related declines in muscle and bone health. These combined factors could significantly impact healthy aging outcomes in older adults8. Furthermore, socioeconomic status (SES) played a role in shaping diet quality. For instance, individuals with lower SES may adapt vegetarian diets due to relatively lower price of plant-based diets in China, potentially leading to less diverse and nutrient-rich food intake - factors that contribute to diet quality disparities within plant-based diets37. Finally, cultural and ethnic factors may influence dietary patterns, as vegetarian diets in China often differ from those in Western countries, with greater reliance on staple foods and fewer fortified products38. These findings underscored the importance of tailoring dietary recommendations to account for individual and contextual factors to promote healthy aging effectively.
Our study has several limitations. First, dietary intake data were collected using a non-quantitative dietary questionnaire, subject to measurement error in diet assessment, making it impossible to adjust for total energy intake. This limitation also means that vegetarians were defined based solely on the frequency of animal product consumption. However, the frequency of intake may be more important than portion size to distinguish between high and low consumption of fruits and vegetables, and several studies have demonstrated the reliability and validity of using non-quantitative FFQ to assess dietary patterns39,40. Additionally, the lack of data on dairy consumption precluded us from identifying the ovo-lacto-vegetarian group. Future studies with more detailed and dietary data are needed to better address these distinctions. Secondly, self-report of chronic diseases may lead to an underestimation of disease prevalence and potential misclassification. However, this underestimation is likely global in nature, potentially impacting the study population uniformly41. Thirdly, the study’s focus on the Chinese elderly population limits the generalizability of the findings to other ethnic and racial groups, necessitating further research to understand dietary patterns and health outcomes across diverse cultural contexts. Finally, the relatively small sample size of our study may limit the statistical power and stability of our analysis, posing a risk of overfitting, which may reduce the generalizability of the results. Future studies with larger sample sizes are warranted to validate our findings and ensure the robustness of the associations observed in this study.
In conclusion, we observed associations between vegetarian diets and lower likelihood of achieving healthy aging in older adults. Consistently adhering to omnivorous diets was associated with higher likelihood of achieving healthy aging outcomes, compared to those who stably followed vegetarian diets. This implies that judicious control of plant-based food intake and modest introduction of animal-based foods may improve the overall health status of healthy older adults. These results could inform personalized dietary recommendations for older adults, emphasizing the importance of balanced diets that incorporate both plant- and animal-based foods. Older adults adhering to vegetarian diets should be carefully monitored for potential nutrition deficiencies and provided with personalized nutritional advice if indicated. Promoting healthy dietary patterns that support healthy aging may help reduce the burden of age-related diseases and enhance quality of life in aging populations. Furthermore, carefully designed studies are urgently needed to elucidate the potential health benefits and risks of vegetarian diets in this demographic, ensuring that dietary guidelines are evidence-based and tailored to their unique nutritional needs.
Methods
Study design and participants
The CLHLS is a nationally representative ongoing longitudinal study initiated in 1998, designed to investigate the determinants of healthy aging. Participants in the CLHLS were aged 60 years and older, and were recruited from 22 of the 31 provinces in mainland China, covering approximately 85% of the population. The CLHLS has systematically collected data across eight survey waves, conducted in 1998, 2000, 2002, 2005, 2008, 2011, 2014, and 2018. Each survey wave involved both follow-up assessments of existing participants and the enrollment of new ones. A detailed description of the study design can be found elsewhere42. Ethics approval was obtained from the Research Ethics Committees of Peking University and Duke University (IRB00001052-13074) and signed written consent forms were obtained from all participants or their legal representatives.
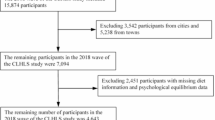
At baseline and during follow-up, participants’ health status was evaluated for self-reported major chronic diseases, and for physical, cognitive and mental health performance (details are described in Assessment of Healthy Aging). Participants were considered healthy if no issues were identified in the aforementioned aspects. For the purpose of our study, a total of 6974 (out of 34,436 total) participants, aged between 60 and 79 years at enrollment, were initially included as potential healthy aging candidates (i.e., those who could reach 80 years of age by 2018). We then excluded participants who were lost to follow-up, had missing data on dietary intake at baseline or on healthy aging components during follow-up (n = 1205), or did not meet the healthy aging criteria at baseline (n = 2881), leaving 2,888 participants for the current analyses (Supplementary Figure 1).
Assessment of healthy aging
Drawing upon the concept of healthy aging43,44, we defined healthy aging as survival to at least 80 years, coupled with no self-reported major chronic disease and no impairment in cognitive function, physical function, or mental health (Supplementary Table 1). Detailed criteria include: (1) no self-reported major chronic disease, including diabetes, CVD, stroke, chronic respiratory disease, cancer, and hypertension, assessed by self-report questionnaire; (2) no physical function impairment, as assessed with the Activities of Daily Living (ADL) index, and defined as not requiring any form of assistance (ranging from partial to complete help) in performing daily tasks such as bathing, dressing, toileting, getting out of bed, or feeding45; (3) no cognitive impairment, as assessed with the validated Chinese version of the Mini-Mental State Exam (MMSE), with a score of 18 or higher indicating the absence of cognitive impairment46; and (4) no mental health impairment: psychological well-being was measured by seven items covering positive aspects (optimism, sense of personal control, conscientiousness, and positive feelings about aging) and negative aspects (loneliness, anxiety, and loss of self-worth) using a five-point Likert scale. A psychological well-being index was constructed from the sum of these seven items (range 0–35, with higher scores indicating better mental health), and good mental health function was defined as a score ≥ 24 (the lowest quartile)47.
Assessment of vegetarian diet
Information on dietary intake at baseline and recalled habitual intake at 60 years of age was collected using a simplified food frequency questionnaire (FFQ), comprising 12 food group items, through in-person interviews by trained research staff, as detailed previously48,49. Although the use of frequency may lack detailed quality, previous studies have shown this non-quantitative form of questionnaire to be reliable and valid. In addition, previous studies also showed that frequency of intake is more important than portion size to distinguish between high and low consumption of fruits and vegetables39,40,50. Based on the consumption frequency of the following items: eggs, fish or seafood, and meat (including beef, poultry, pork, lamb, and processed meats), participants were categorized into four types of dietary patterns: the vegan diet (no consumption of eggs, fish, seafood, or meat), the ovo-vegetarian diet (consumption of eggs but no fish, seafood or meat), the pesco-vegetarian diet (consumption of fish or seafood, with or without eggs, but no meat), and the omnivore diet (consumption of meat)51. These dietary patterns were further dichotomized into vegetarian and omnivore diets by combining the first three categories, due to their common exclusion of meat and poultry as primary protein sources, in alignment with the broader definition of vegetarianism. As a secondary exposure, dietary pattern change from age 60 y to baseline was examined, and participants were classified into four groups: consistently vegetarian (vegetarian at both age 60 and baseline), vegetarian to omnivore, omnivore to vegetarian, and consistently omnivore (omnivore at both age 60 and baseline).
We further calculated the healthy plant-based diet index (hPDI), and unhealthy plant-based diet index (uPDI), using a method adapted from Satija et al.52, with modifications to food group intake frequencies to align with the qualitative nature of the FFQ, to evaluate dietary adherence to healthy/unhealthy plant-based dietary patterns. Twelve food groups were scored from 1 to 5; the animal-based food groups received negative scores, while the healthy plant-based food received positive scores for hPDI and negative scores for uPDI. Detailed scoring information is in Supplementary Table 2.
Assessment of covariates
Sociodemographic factors, including age (year), sex (male, female), ethnic group (Han, other), residence (urban vs. rural dwellers), years of education (0, 1-9, >9 years), household income (< 8000 CNY, 8000–30,000 CNY, > 30,000 CNY), and marital status (married and cohabiting, or other); and lifestyle factors, including smoking status (never, former, current), alcohol use (never, former, current), exercise status (never, former, current) were collected via questionnaires. Weight and height were measured by trained medical staff during the physical examination. Body mass index (BMI) was calculated as weight (kg) / height squared (m2), and categorized as underweight (BMI < 18.5 kg/m2), recommended (18.5 kg/m2 ≤ BMI < 24.0 kg/m2), or overweight/obese (BMI ≥ 24.0 kg/m2)53. Given that height measurements were unavailable in the first three waves (1998, 2000, 2002) of surveys, knee height was adopted to estimate individual height, using validated equations for older Chinese men (height = 67.78 + 2.01 × knee height) and women (height = 74.08 + 1.81 × knee height)54.
Statistical analysis
All statistical analyses were performed using R version 4.2. The STROBE-NUT reporting guidelines were used to report the checklist for this study (STROBE-NUT checklist)55. Baseline characteristics across dietary patterns (vegetarian vs. omnivore) were compared using t-tests for continuous variables and chi-square tests for categorical variables. Covariates with missing data were assigned to an independent category. Similar to a previous study13, logistic regression models were used to estimate the likelihood of achieving healthy aging across diet patterns (vegan, ovo-vegetarian, pesco-vegetarian, and omnivore, along with the combined vegetarian vs. omnivore) and status change diets from 60 years (consistently vegetarian, vegetarian to omnivore, omnivore to vegetarian, and consistently omnivore), ORs and 95% CIs were computed. In model 1, we adjusted for age and sex. In model 2, we further adjusted for ethnic group, residence, marital status, household income level, education level, smoking status, alcohol use, exercise status, BMI, and the year of enrollment. In the secondary analysis, we focused on participants who successfully lived to 80 years, and examined how dietary patterns and changes in these patterns were associated with individual health domains: major chronic diseases, cognitive impairment, physical function impairment, and mental health impairment) (n = 1585).
Additionally, we assessed the associations of healthful, and unhealthful plant-based dietary patterns with healthy aging, adjusting for the aforementioned covariates. The hPDI and uPDI were used as categorical variables (divided into quintiles) in the analysis, following the approach used in previous studies56. To examine interactions between the healthiness of plant-based dietary patterns and vegetarian dietary patterns, we conducted a joint analysis, based on median-divided uPDI score (high uPDI vs. low uPDI) and dietary pattern (vegetarian vs. omnivore), categorizing participants into four distinct groups: high uPDI omnivores, high uPDI vegetarians, low uPDI omnivores, and low uPDI vegetarians. A similar analysis was performed based on hPDI scores. Similar analysis was conducted in those participants who successfully lived to 80 years (n = 1585) to examine associations of these patterns with individual health domains.
Four types of sensitivity analyses were carried out to test the robustness of the results: (1) Two- and five-year lag analyses were performed by excluding participants who had been followed for less than 2 or 5 years from baseline, respectively, to reduce the possibility of reverse causation; (2) Additionally adjusted for whether participants engaged in religious activities (only availble in the first three waves); (3) Modifying the definitions of cognitive impairment and mental health impairment by adjusting the cut-off score for the MMSE to 24, and for the psychological well-being index to 27 (median), respectively; and (4) Using Cox Proportional Hazards regression to calculate hazard ratios (HR) and 95% CI for healthy aging across different dietary groups.
Data availability
This article is based on a publicly available dataset derived from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The dataset can be obtained after sending a data user agreement to the data team on the webset of Peking University Open Research Data: https://opendata.pku.edu.cn/dataset.xhtml?persistentId=doi:10.18170/DVN/WBO7LK&version=2.0. Other data that support this work are available from the corresponding author upon reasonable request.
Abbreviations
- CLHLS:
-
Chinese Longitudinal Healthy Longevity Survey;
- FFQ:
-
Food Frequency Questionnaire;
- MMSE:
-
Mini-Mental State Exam
- PDI:
-
Plant-Based Diet Index.
References
Willett, W. et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 393, 447–492 (2019).
Craig, W. J. Nutrition concerns and health effects of vegetarian diets. Nutr. Clin. Pr. 25, 613–620 (2010).
Wang, T., Masedunskas, A., Willett, W. C. & Fontana, L. Vegetarian and vegan diets: benefits and drawbacks. Eur. Heart J. 44, 3423–3439 (2023).
Pilis, W., Stec, K., Zych, M. & Pilis, A. Health benefits and risk associated with adopting a vegetarian diet. Rocz. Panstw. Zakl. Hig. 65, 9–14 (2014).
Marrone, G. et al. Vegan diet health benefits in metabolic syndrome. Nutrients https://doi.org/10.3390/nu13030817 (2021).
Bauer, J. & Walrand, S. Editorial: Vegan diets for older adults: is it a risky business? Curr. Opin. Clin. Nutr. Metab. Care 26, 1–2 (2023).
Thorpe, D. L., Beeson, W. L., Knutsen, R., Fraser, G. E. & Knutsen, S. F. Dietary patterns and hip fracture in the Adventist Health Study 2: combined vitamin D and calcium supplementation mitigate increased hip fracture risk among vegans. Am. J. Clin. Nutr. 114, 488–495 (2021).
Domić, J., Grootswagers, P., van Loon, L. J. C. & de Groot, L. Perspective: vegan diets for older adults? A perspective on the potential impact on muscle mass and strength. Adv. Nutr. 13, 712–725 (2022).
Katonova, A., Sheardova, K., Amlerova, J., Angelucci, F. & Hort, J. Effect of a vegan diet on Alzheimer’s disease. Int. J. Mol. Sci. https://doi.org/10.3390/ijms232314924 (2022).
Le, L. T. & Sabaté, J. Beyond meatless, the health effects of vegan diets: findings from the Adventist cohorts. Nutrients 6, 2131–2147 (2014).
Appleby, P. N., Crowe, F. L., Bradbury, K. E., Travis, R. C. & Key, T. J. Mortality in vegetarians and comparable nonvegetarians in the United Kingdom. Am. J. Clin. Nutr. 103, 218–230 (2016).
Depp, C. A. & Jeste, D. V. Definitions and predictors of successful aging: a comprehensive review of larger quantitative studies. Am. J. Geriatr. Psychiatry 14, 6–20 (2006).
Shi, H., Huang, T., Schernhammer, E. S., Sun, Q. & Wang, M. Rotating night shift work and healthy aging after 24 years of follow-up in the nurses’ health study. JAMA Netw. Open 5, e2210450 (2022).
Schietzel, S. et al. Prevalence of healthy aging among community dwelling adults age 70 and older from five European countries. BMC Geriatr. 22, 174 (2022).
Pac, A. et al. Influence of sociodemographic, behavioral and other health-related factors on healthy ageing based on three operative definitions. J. Nutr. Health Aging 23, 862–869 (2019).
Tong, T. Y. N. et al. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: results from the prospective EPIC-Oxford study. Bmj 366, l4897 (2019).
Key, T. J. et al. Mortality in British vegetarians: results from the European Prospective Investigation into Cancer and Nutrition (EPIC-Oxford). Am. J. Clin. Nutr. 89, 1613s–1619s (2009).
Orlich, M. J. et al. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Intern Med 173, 1230–1238 (2013).
Forestell, C. A. & Nezlek, J. B. Vegetarianism, depression, and the five factor model of personality. Ecol. Food Nutr. 57, 246–259 (2018).
Mihrshahi, S. et al. Vegetarian diet and all-cause mortality: Evidence from a large population-based Australian cohort - the 45 and Up Study. Prev. Med 97, 1–7 (2017).
Tong, T. Y. N. et al. Vegetarian and vegan diets and risks of total and site-specific fractures: results from the prospective EPIC-Oxford study. BMC Med 18, 353 (2020).
Menzel, J. et al. Vegan diet and bone health-results from the cross-sectional RBVD Study. Nutrients https://doi.org/10.3390/nu13020685 (2021).
Tucker, K. L. Vegetarian diets and bone status. Am. J. Clin. Nutr. 100, 329s–335s (2014).
Dawczynski, C. et al. Nutrient intake and nutrition status in vegetarians and vegans in comparison to omnivores - the nutritional evaluation (NuEva) study. Front Nutr. 9, 819106 (2022).
Moore, E. et al. Cognitive impairment and vitamin B12: a review. Int Psychogeriatr. 24, 541–556 (2012).
Wang, X. et al. Resolution of inflammation is altered in Alzheimer’s disease. Alzheimers Dement 11, 40–50.e41-42 (2015).
Chai, B. et al. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: an updated meta-analysis. BMC Neurol. 19, 284 (2019).
Hibbeln, J. R., Northstone, K., Evans, J. & Golding, J. Vegetarian diets and depressive symptoms among men. J. Affect Disord. 225, 13–17 (2018).
Baines, S., Brown, W. J. & Powers, J. How does the health and well-being of young Australian vegetarian and semi-vegetarian women compare with non-vegetarians? Public Health Nutr. 10, 436–442 (2007).
Kim, J., Kim, H. & Giovannucci, E. L. Plant-based diet quality and the risk of total and disease-specific mortality: A population-based prospective study. Clin. Nutr. 40, 5718–5725 (2021).
Liang, F. et al. Association of body mass index and plant-based diet with cognitive impairment among older chinese adults: a prospective, nationwide cohort study. Nutrients. https://doi.org/10.3390/nu14153132 (2022).
Qi, R., Yang, Y., Sheng, B., Li, H. & Zhang, X. Plant-based diet indices and their association with frailty in older adults: a CLHLS-based cohort study. Nutrients https://doi.org/10.3390/nu15245120 (2023).
Kim, H., Lee, K., Rebholz, C. M. & Kim, J. Plant-based diets and incident metabolic syndrome: Results from a South Korean prospective cohort study. PLoS Med 17, e1003371 (2020).
Kouvari, M. et al. Quality of plant-based diets in relation to 10-year cardiovascular disease risk: the ATTICA cohort study. Eur. J. Nutr. 61, 2639–2649 (2022).
Traylor, D. A., Gorissen, S. H. M. & Phillips, S. M. Perspective: protein requirements and optimal intakes in aging: are we ready to recommend more than the recommended daily allowance? Adv. Nutr. 9, 171–182 (2018).
Hengeveld, L. M. et al. Prevalence of protein intake below recommended in community-dwelling older adults: a meta-analysis across cohorts from the PROMISS consortium. J. Cachexia Sarcopenia Muscle 11, 1212–1222 (2020).
Kehoe, S. H. et al. Diet patterns are associated with demographic factors and nutritional status in South Indian children. Matern Child Nutr. 10, 145–158 (2014).
Hargreaves, S. M., Raposo, A., Saraiva, A. & Zandonadi, R. P. Vegetarian diet: an overview through the perspective of quality of life domains. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph18084067 (2021).
Mohammadifard, N. et al. Validation of a simplified food frequency questionnaire for the assessment of dietary habits in Iranian adults: Isfahan Healthy Heart Program, Iran. ARYA Atheroscler. 11, 139–146 (2015).
Ashfield-Watt, P. A., Welch, A. A., Day, N. E. & Bingham, S. A. Is ‘five-a-day’ an effective way of increasing fruit and vegetable intakes? Public Health Nutr. 7, 257–261 (2004).
Gao, K. et al. Association between sarcopenia and cardiovascular disease among middle-aged and older adults: Findings from the China health and retirement longitudinal study. EClinicalMedicine 44, 101264 (2022).
Zeng, Y. D. P. Jr., Vlosky, D. A. & Gu, D. Healthy longevity in China : demographic, socioeconomic, and psychological dimensions. Springe. Ebooks 63, 312–313 (2008).
Rowe, J. W. & Kahn, R. L. Human aging: usual and successful. Science 237, 143–149 (1987).
Ma, W. et al. Adult height, dietary patterns, and healthy aging. Am. J. Clin. Nutr. 106, 589–596 (2017).
Katz, S., Ford, A. B., Moskowitz, R. W., Jackson, B. A. & Jaffe, M. W. Studies of illness in the aged. The index of adl: a standardized measure of biological and psychosocial function. Jama 185, 914–919 (1963).
Gao, M. et al. The time trends of cognitive impairment incidence among older Chinese people in the community: based on the CLHLS cohorts from 1998 to 2014. Age Ageing 46, 787–793 (2017).
Gong, E., Hua, Y. & Yan, L. L. Psychological wellbeing and all-cause mortality in the oldest old in China: a longitudinal survey-based study. Lancet 388, S22 (2016).
Zhang, Y. et al. Interaction between APOE ε4 and dietary protein intake on cognitive decline: A longitudinal cohort study. Clin. Nutr. 40, 2716–2725 (2021).
Jin, X. et al. Association of APOE ε4 genotype and lifestyle with cognitive function among Chinese adults aged 80 years and older: A cross-sectional study. PLoS Med 18, e1003597 (2021).
Wong, J. E., Parnell, W. R., Black, K. E. & Skidmore, P. M. Reliability and relative validity of a food frequency questionnaire to assess food group intakes in New Zealand adolescents. Nutr. J. 11, 65 (2012).
Medawar, E., Huhn, S., Villringer, A. & Veronica Witte, A. The effects of plant-based diets on the body and the brain: a systematic review. Transl. Psychiatry 9, 226 (2019).
Satija, A. et al. Plant-based dietary patterns and incidence of type 2 diabetes in US men and women: results from three prospective cohort studies. PLoS Med 13, e1002039 (2016).
Chen, C., Lu, F. C. & Department of Disease Control Ministry of Health, P. R. C. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci. 17, 1–36 (2004).
Zhang, H., Hsu-Hage, B. H. & Wahlqvist, M. L. The use of knee height to estimate maximum stature in elderly Chinese. J. Nutr. Health Aging 2, 84–87 (1998).
Lachat, C. et al. Strengthening the reporting of observational studies in epidemiology - nutritional epidemiology (STROBE-nut): An extension of the STROBE statement. Nutr. Bull. 41, 240–251 (2016).
Baden, M. Y. et al. Changes in plant-based diet quality and total and cause-specific mortality. Circulation 140, 979–991 (2019).
Acknowledgements
This work was supported by the key projects in the three-year plan of Shanghai municipal public health system (2023–2025), GWVI-4 and GWVI-11.1-42, and National Natural Science Foundation of China (82473622). There are no financial conflicts of interest to disclose.
Author information
Authors and Affiliations
Contributions
GJ, YL and XG designed this study. GJ and YL performed the statistical analysis, coordinated the work and drafted the manuscript. KW, YL, KT, FC, and XS accessed and verified the underlying data. XG was responsible for the decision to submit the manuscript after consultation with all listed authors. YL, KT, FC, LS, and XG revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jigeer, G., Wang, K., Lv, Y. et al. Vegetarian diet and healthy aging among Chinese older adults: a prospective study. npj Aging 11, 25 (2025). https://doi.org/10.1038/s41514-025-00213-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41514-025-00213-4
