
Abstract
Motor dysfunction in Parkinson’s disease (PD) has been linked to widespread oscillatory changes within the basal ganglia-thalamic-cortical network, particularly in the beta frequency range. However, the evolution of cortical neurophysiological alterations and their relationship to clinical progression remain poorly understood. We conducted a longitudinal resting-state magnetoencephalography (MEG) study in 27 persons with PD and 30 healthy individuals with a mean follow-up time of 4 years. Source-reconstructed MEG data were parcellated into cortical regions, from which power spectra were parameterized to separate oscillatory peaks from the aperiodic component. An increase in the aperiodic exponent in the left postcentral region was associated with progression of rigidity. Peak beta power in parieto-temporo-occipital regions was elevated at baseline, correlating with less severe bradykinesia. This negative relationship weakened over time in patients with progressive symptoms, suggesting an association with compensatory mechanisms. Using partial least squares regression to predict future disease course from baseline neurophysiological features, 19.5% of the variability in motor progression was explained in an independent validation cohort. Our results emphasize the importance of separating aperiodic neural activity from periodic oscillations as a progressive alteration of the aperiodic component represented the most prominent PD-related neurophysiological change. Further, our findings highlight the potential predictive value of resting-state neurophysiology for future disease progression.
Similar content being viewed by others


Introduction
Slowness of movement or bradykinesia and muscle stiffness or rigidity are core motor symptom of Parkinson’s disease (PD) traditionally considered a result of altered basal ganglia output to the motor cortex1,2. One potential neuromarker of impaired motor functioning in PD is oscillatory brain activity in the beta frequency range (13-30 Hz). Increased beta band power at the level of the basal ganglia has been consistently linked to severity of bradykinesia and to treatment response in PD3,4,5. These findings align well with the conceptualization of beta as an antikinetic rhythm governing the “status quo” over initiation of a new movement4.
The relationship between cortical beta oscillations and motor symptoms, on the other hand, is far less clear. Indeed, some findings contradict a straightforward interpretation of beta as a purely antikinetic rhythm. For instance, previous evidence suggests that cortical beta power in the central sensorimotor region may be highest in early, untreated PD while it may decrease later in the disease course, eventually falling below healthy levels with lower sensorimotor beta power scaling with higher motor symptom burden6,7. Additionally, resting state cortical beta activity may increase or remain unchanged with successful amelioration of motor symptoms by dopamine-replacement therapy (DRT)6,8,9,10.
Beyond the motor cortex, global oscillatory slowing across the neocortex11, and widespread changes in cortical oscillatory network organization have been described in PD12,13,14. This generalized slowing results from power increases in low-frequency bands (e.g., delta (2–4 Hz), theta (5–8 Hz) and concurrent power reduction in higher frequency bands (e.g., alpha (8–12 Hz) and beta). Recently, slowing of cortical activity in PD has been shown to exhibit a spatial adverse-to-compensatory gradient from superior parietal regions to the inferior prefrontal cortex15.
Spontaneous neuronal activity consists of two physiologically distinct components: On the one hand side, periodic or oscillatory fluctuations and on the other side, aperiodic, i.e., non-oscillatory fluctuations. In the frequency domain, the aperiodic component can be described as the offset and slope of the power spectrum which tends to follow a 1/f power law distribution16. Aperiodic activity is hypothesized to reflect neuronal spiking activity and the so-called excitatory-inhibitory (E/I) balance where a steeper slope can be interpreted as increased inhibition over excitation and vice versa17. When controlling for this aperiodic activity using parameterization of the power spectrum, periodic activity (i.e., true significant rhythmicity or oscillations) can thus be identified as any spectral peaks rising above the aperiodic component and described with its amplitude (or power), peak frequency and width18.
Recent re-appraisal of the cortical activity in PD considering the aperiodic component, has led to the conclusion that the slope of aperiodic component of the neuronal activity spectrum is steeper in PD compared with healthy individuals across central sensorimotor, parietal, temporal and occipital regions, indicating a shift of the excitatory/inhibitory balance in the direction of increased inhibition19,20. That we have previously shown and replicated in a second cohort that beta band activity in the sensorimotor cortex is not different from healthy individuals when controlling for this aperiodic component10,21 raises the question how much of earlier PD-related findings were due to the lack of parametrization of the power spectrum into periodic and aperiodic components (but see also ref. 15).
Very few longitudinal MEG studies on PD exist and, to the best of our knowledge, all report on the same patient cohort without separating the periodic and aperiodic components of the neurophysiological signal7,13,22. In this longitudinal MEG study, we therefore aimed to investigate changes in the oscillatory and aperiodic components of neuronal activity across the entire cortex in relation to clinical progression of PD over a period of 4 years controlling for general effects of aging by inclusion of a matched healthy control group. Further, we aimed to build and externally validate a predictive model for future disease progression derived from simple resting-state neuronal activity measures.
Results
Longitudinal progression of symptom severity
Complete clinical and MEG data were collected from 28 persons with PD and 31 healthy individuals matched for age and sex. After data collection, the diagnosis in one participant in the PD group was revised to the Parkinsonian type of Multiple System Atrophy (MSA-P) and the participant was subsequently excluded from our analysis. One healthy participant with a positive family history for Essential Tremor displayed postural and kinetic tremor and mild bradykinesia at follow-up (MDS-UPDRS part III 9 points) and was therefore excluded from further analysis.
Please see Table 1 for a summary of demographics and clinical characteristics of the final cohort consisting of 30 healthy individuals and 27 persons with PD (17 with right-lateralized and 11with left-lateralized symptoms, respectively).
The mean follow-up period was 48.8 ± 7.3 months. In the PD group, motor symptom severity progressed only slightly over the follow-up period with a mean increase in MDS-UPDRS III score of 1.4 ± 8.6 points without reaching statistical significance (Table 1). On an individual level, motor disease progression was highly variable ranging from a reduction by 18 points in MDS-UPDRS III to an increase by 16 points in MDS-UPDRS III (Supplementary Fig. 2). Eleven patients (41%) showed a clinically meaningful decline in motor functions defined as an increase in MDS-UPDRS III of >4.6 points23 whereas nine patients remained stable and seven showed clinically relevant improvement in motor function. Here, it is important to mention that the levodopa equivalent daily dosage increased in all patients with almost double the baseline dose at follow-up on a group level (Table 1). However, the relationship between LEDD adjustments and clinical progression seems to be complex as there was no evidence supporting that change in LEDD alone could explain change in MDS-UPDRS III or its subscores in a linear regression model (total MDS-UPDRS III: r = -1.130, p = 0.226, Supplementary Fig. 2).
General cognitive abilities measured in MoCA remained stable in both groups (Table 1). While three persons with PD and two healthy control participants scored under the cut-off for potential cognitive impairment of 23/24 points in MoCA, none of the recruited participants fulfilled clinical criteria for a diagnosis of dementia.
PD-related neurophysiological alterations
At baseline, there was evidence for a decreasing effect of PD on peak alpha frequency in bilateral superior temporal (right: t(27) = -3.767, pFDR = 0.020; left: t(27) = -3.294, pFDR = 0.023), right transverse temporal (t(27) = -4.582, pFDR = 0.004) region, and right pars triangularis of the inferior frontal gyrus (t(27) = -3.711, pFDR = 0.023) (28% of ROI excluded from analysis for which values were available for < 10 participants per group, Supplementary Fig. 3). Further, we identified an increasing effect of PD on peak beta power in a large range of cortical areas accentuated in parietal, temporal and occipital regions (Fig. 3). Likewise, both the exponent and offset of the aperiodic component were higher in the PD group compared to healthy participants with a similar spatial pattern (Supplementary Fig. 3). No evidence for group differences was found for peak beta frequency or peak alpha power.
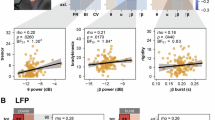
Within the PD group, peak beta power was negatively correlated with bradykinesia in the right superior parietal region (t(22) = -3.250, pFDR = 0.049), left lateral occipital region (right: t(22) = -3.423, pFDR = 0.044), right fusiform gyrus (t(22) = -3.671, pFDR = 0.044) and left caudal anterior cingulate cortex (t(22) = -3.395, pFDR = 0.044) with the same trend in the right inferior parietal (t(22) = -3.089, pFDR = 0.052) and right lateral occipital regions (t(22) = -3.091, pFDR = 0.052) (Fig. 3).
Longitudinal change of aperiodic and periodic components
We first aimed to compare the change in the distribution of peaks in the entire frequency spectrum between 1 and 35 Hz across the whole cortex, i.e., without a priori delineation of the signal into traditional frequency bands (Fig. 1, lower row). From visual inspection, one may appreciate that PD was associated with a progressive reduction of peak frequency in the alpha and low beta frequency ranges over time.

The upper plot shows the full spectrum, the plots on the right show the aperiodic and periodic (“flattened spectrum”) components separately. Lower Row: Histogram of the distribution of oscillatory peaks across all regions by group and time point. Bin width 0.5 Hz. The beta band was extended to include frequencies up to 35 Hz for this visualization.
In the analysis by region and frequency band, no evidence for significant group*time interaction in the mixed-effects models for any of the oscillatory neurophysiological variables of interest was found (ROI exclusion rate in the extended alpha band: 37%). A trend towards an effect of the group*time interaction for peak beta power in the left caudal middle frontal gyrus (t(51.4) = 3.146, pFDR = 0.09) and left paracentral region (t(51.5) = 3.387, pFDR = 0.09) did not survive correction for multiple comparison. Since we had a strong a priori hypothesis about PD-related changes in beta power over time, we conducted an exploratory by-group analysis. Here, we did not find evidence for any regional changes in peak beta power in the healthy control group (all pFDR > 0.05). The PD group, on the other hand, showed an increase in peak beta power in several additional regions encompassing the left pre- and postcentral region, parts of the inferior and posterior middle frontal gyrus, and right temporal lobe and insula. Furthermore, there was evidence for a decrease in peak beta power over time in the left lateral occipital region and bilateral cuneus, whereby the raw peak beta power at follow-up was still higher than in the healthy control group (Supplementary Fig. 4).
Regarding longitudinal change of the aperiodic component, there was a significant group*time interaction for the exponent of the aperiodic component in the left postcentral (t(55) = 3.424, pFDR = 0.047) and right paracentral regions (t(55) = 3.367, pFDR = 0.047). In group-wise post-hoc comparison, the PD group exhibited an increase over time in the left postcentral region (t(26) = 3.358, pFDR = 0.032) while the healthy control group did not display significant change with a general tendency towards a decreasing exponent in the central region (Fig. 2).

Left panel: Upper row: Group x time interaction across brain regions for the aperiodic exponent, only displaying t statistics for regions with a significant interaction effect defined by pFDR < 0.05. Middle rows: Main effects of time per group for illustration of the overall trends over time. Lowest row illustrating the results of the ANCOVA for the relationship between change in aperiodic exponent and rigidity progression. Asterix indicates regions with for which the ANCOVA model described in the main text resulted in a significant effect with an FDR-corrected p-value < 0.05. Coloring represents the respective t-values of this effect. Right panel: Upper row: Aperiodic component of the neuronal signal as derived from parametrization by group and time point in the left postcentral region. Lower row: Relationship between change in the aperiodic exponent and annual rigidity progression rate. R² in the upper right corner is the partial R² indicating how much of the variance in clinical change is explained by adding change in the aperiodic exponent to the ANCOVA model. The gray area represents the 95%-confidence interval around the fitted regression line in pink.
Relationship of longitudinal neurophysiological changes with symptom progression
Based on the evidence for a significant PD-related longitudinal change in the aperiodic exponent, we next aimed to explore whether this change related to clinical progression, as measured in MDS-UPDRS III and its subscores.
The ANCOVA model resulted in a significant positive association of the change in exponent of the aperiodic exponent with the annual LEDD-adjusted change in rigidity in the left postcentral gyrus (t(26) = 3.445, pFDR = 0.030), right supramarginal gyrus (t(26) = 3.544, pFDR = 0.030) as well as parts of the left superior temporal lobe and bilateral insula (Fig. 2). The same trend was found for additional adjacent regions, including bilateral precentral and paracentral, right postcentral, and left paracentral and supramarginal gyrus (all pFDR = 0.068). For completeness, it is worth mentioning that there was evidence for a significant effect of the baseline aperiodic exponent on the annual progression rate of bradykinesia in bilateral precuneus (right: t(26) = 3.372, pFDR = 0.045; left: t(26) = 4.593, pFDR = 0.009), bilateral superior parietal (right: t(26) = 3.489, pFDR = 0.045; left: t(26) = 3.595, pFDR = 0.045), and left paracentral regions (t(26) = 3.278, pFDR = 0.045).
Furthermore, we identified significant positive associations between change in the aperiodic offset and progression of bradykinesia in bilateral entorhinal (right: t(26) = 3.103, pFDR = 0.043; left: t(26) = 3.453, pFDR = 0.043), parahippocampal (right: t(26) = 3.450, pFDR = 0.043; left: t(26) = 3.317, pFDR = 0.043), inferior temporal (right: t(26) = 3.140, pFDR = 0.043; left: t(26) 3.674, pFDR = 0.043), and right fusiform gyri (t(26) = 3.258, pFDR = 0.043) (Supplementary Fig. 5).
Lastly, we explored whether the negative relationship between peak beta power and severity of bradykinesia found at baseline changed over the follow-up period. Here, we hypothesized that this relationship might weaken over time if it paralleled compensatory mechanisms and their assumed break down with disease progression. To this end, we built a mixed-effects model with bradykinesia as dependent variable, and peak beta power, time, their interaction, and LEDD as fixed effects and subject as a random effect. In this model, there was evidence for a significant peak beta power x time interaction in the right superior parietal region (t = 3.011, pFDR = 0.019), indicating a significant change in the relationship between peak beta power and bradykinesia over time (Fig. 3). For post-hoc comparison, we further divided the PD cohort based on whether they progressed in bradykinesia over time (defined by LEDD-adjusted annual change > 0). To test whether the temporal change of the relationship between parietal beta peak power and bradykinesia differed between stable patients and progressors, we used emtrends to estimate and compare slopes at baseline and follow-up between these subgroups. The three-way interaction of beta power, time and subgroup did not reach statistical significance (t = 1.35, p = 0.19), indicating no evidence that the rate of change in the beta-bradykinesia relationship over the mean follow-up time of 49 months differed between progressors and non-progressors. Still, the direction was consistent with our hypothesis (positive coefficient indicating greater weakening in progressors) which may have clinical relevance despite limited statistical power in this subgroup analysis.

Left panel: Upper row: Only showing color-coded t statistics for regions with a significant group effect defined by pFDR < 0.05 across all cortical regions. There was a general trend towards a further increase of peak beta band power over time except for the occipital lobe (not shown here, Supplementary Fig. 4). Lower rows: Results of the regression model for the association between peak beta power and bradykinesia corrected for LEDD and age at baseline and follow-up, respectively. Asterix indicating an FDR-corrected p < 0.05. Right panel: Exemplary results from the superior parietal region. Dashed lines represent insignificant effects of peak beta power on bradykinesia. Shaded areas show the 95%-confidence interval around the fitted regression lines. In the lower row, patients were post-hoc sub-divided by annual progression rate of bradykinesia with progressors showing a rate > 0, i.e., an increase of bradykinesia severity over time.
Predicting symptom progression from neurophysiology
We next wanted to explore how much of the longitudinal clinical progression could be explained by simple aperiodic and periodic features of the neuronal signal at baseline. So far, our analysis focused on the effects of one of these features at a time. However, they showed collinearity which is reflected by our results suggestive of associations of several features (peak beta power, aperiodic exponent and offset) with aspects of motor symptoms (bradykinesia and rigidity) and their longitudinal progression, respectively (see Supplementary Fig. 6 for correlation matrix). Combining all these features into one prediction model is further complicated by the multicollinearity across the 68 parcellated brain regions. Additionally, our PD sample was relatively small resulting in a risk for overfitting. We therefore opted for a combined approach with dimension reduction across neurophysiological features using PCA followed by partial least squares regression of the first component with the LEDD-adjusted annual progression rate of the MDS-UPDRS III score across regions.
Our validation cohort consisted of 18 persons with PD, well-matched to the training cohort in terms of age, sex, baseline motor symptom severity, and LEDD (age: 65.4 ± 10.2 years, t(43) = -0.24, p = 0.8, baseline MDS-UPDRS III: 19.1 ± 12.1, t(43) = 0.37, p > 0.9, Supplementary Table 1). Paralleling the longitudinal motor symptom progression in our original training sample, the validation cohort did not show significant change in MDS-UPDRS III (t (17) = -1.35, p = 0.195) while considerably increasing LEDD over time (t (17) = -4.24, p = 0.001).
In the training cohort, the region-wise PCA resulted in the first component (PC1) explaining 62.8 ± 8.5% of variance across regions (range 44.6−80.0%). Partial least squares regression with leave-one-out cross-validation identified two components as optimal for progression rate prediction. The model achieved a moderate effect size on training data (R² = 0.365, RMSE = 1.676) while external validation revealed reduced generalization (R² = 0.195, RMSE = 3.674). Using a permutation test, the observed R² in the validation cohort exceeded 93.1% of values in the null distribution, yielding a non-significant permutation p-value of 0.069 (10,000 permutations). Adding age, sex, and baseline MDS-UPDRS III to the model increased performance to 25.0% in the validation cohort (training: R² = 0.578, RMSE = 1.366, validation: R² = 0.250, RMSE = 3.475, p = 0.030 (10,000 permutations).
The performance difference between the training and validation cohorts suggests overfitting to the training data that increased further when adding clinical variables, likely reflecting the relatively high-dimensional nature of the neuroimaging input relative to sample size (2.5:1). Still, we can conclude that 25% of variance in motor progression in the independent sample was explained by the first component of the PCA constructed from peak beta power, peak alpha frequency and the aperiodic component of the neuronal data when adding age, sex and motor symptom severity at baseline.
Next, we explored the differential contributions of brain regions and neurophysiological variables to the overall model. The aperiodic component showed the highest average contribution to regional PC1 (exponent: mean squared loading = 0.350 ± 0.049, offset: 0.303 ± 0.055, followed by peak beta power (0.258 ± 0.074), and peak alpha frequency (0.089 ± 0.071)). Likewise, aperiodic features contributed most to PC1 in a total of 62 regions with predominantly positive loadings (Fig. 4). Peak beta power was most influential in the remaining six regions, including negative loadings in bilateral inferior parietal and left superior parietal regions (max squared loading = 0.317) and positive loadings in the right fusiform and parahippocampal regions (max squared loading = 0.349). Similar patterns emerged when the loadings were weighted by VIP scores derived from the PLS, suggesting that variations in the aperiodic component were also most consistently associated with clinical progression across high-importance brain regions. Bilateral central and superior parietal cortices were identified as the most contributing regions, showing the highest VIP scores and a consistent at least small effect size (Cohen’s d > 0.2) for the correlation between the regional PC1 and progression rate at both baseline and follow-up (Fig. 4).

Upper row: Mean squared loading of each of the four spectral features (aperiodic exponent, aperiodic offset, peak beta power and peak alpha frequency from left to right) color-coded for each region. Lower row: Largest regional contributions to the partial least square regression color-coded by variable importance in projection (VIP), only displaying values for regions for which PC1 and annual progression rate were correlated with at least small effect size (Cohen’s d = 0.2) at both baseline and follow-up. Higher VIP, i.e., darkest color, representing largest contribution.
Discussion
In this longitudinal study, we analysed the relationship between changes in motor symptoms and changes in whole-cortex neurophysiological activity in a cohort of persons with PD over an average period of 4 years. Our results show that the exponent of the aperiodic component of the neurophysiological signal in the central sensorimotor region showed a PD-related increase over time that went beyond healthy aging, and longitudinal change of the aperiodic component (represented by its exponent and offset) was associated with progression rates of rigidity and bradykinesia, respectively.
The progressive PD-related alteration of the aperiodic component over time emphasizes the need for including as well as correcting for aperiodic activity when assessing oscillatory brain activity in PD. After removal of the aperiodic component and stringent correction for multiple comparison, we did not find evidence for consistent PD-related longitudinal change in peak power or frequency in the beta or alpha frequency bands in any of the parcellated brain regions. However, at baseline, there were wide-spread temporo-occipito-parietal increases of peak beta power in PD compared with healthy individuals that persisted over time. A negative association between parieto-occipital peak beta power and bradykinesia at baseline changed significantly over time in the right superior parietal cortex, in particular in patients that experienced clinically progressive bradykinesia. Taken together, these findings suggest that increased parietal beta power in early PD may be associated with compensation.
Lastly, we predicted longitudinal clinical symptom progression based on aperiodic (exponent and offset) and periodic features (peak beta power and peak alpha frequency) of the neurophysiological signal. Here, 19.5% of the variance in the clinical progression over time was explained by these basic features of the neuronal signal in an independent validation cohort.
Previous cross-sectional evidence suggests disease-stage-dependent PD-related alterations of beta band activity in the motor cortex in early PD with an increase of beta power in de-novo and early PD that decreases with disease progression, eventually falling below healthy levels6,24. Our results do not support this claim; instead, we found a trend towards a further increase from early to mid-stage PD (at least in the left hemisphere). Here, it is worth noting that, despite a follow-up period of >4 years, our cohort did only exhibit a marginal increase in motor symptoms in on-medication state on a group level with considerable variability between patients. The lack of significant change in oscillatory cortical activity may in part reflect the lack of clinical progression in approximately half of our sample.
Likewise, participants included in our follow-up assessment remained cognitively stable which may contribute to the lack of a relationship of cognitive performance with cortical activation patterns over time. Thus, our findings may not be generalizable to cohorts with progressive cognitive impairment. On the other hand, the fact that our sample remained cognitively stable (NB, according to a cognitive screening test) is an advantage as it supports that the effects seen with motor progression are less likely to be influenced by concomitant cognitive decline.
The previous longitudinal study of neurophysiological resting state activity in PD estimated relative power in several frequency bands without separating or controlling for the effects of the aperiodic component of the signal from that of the periodic component. In their sample with a follow-up period of up to 7 years, “oscillatory slowing” (manifested as an increase in theta power and decrease in alpha power) was progressive7 and most pronounced in centro-parieto-temporal regions22. Here, it is worth noting that publications on this cohort averaged either across the entire cortex (in sensor space) or into large subregions roughly corresponding to lobes, respectively. Our analysis approach adds to these prior studies by considering and compensating for the aperiodic component and by performing a more fine-grained analysis of the spatial distribution. While we found evidence to support a shift in alpha activity to lower frequencies when averaging across the entire cortex (Fig. 1), this was not further substantiated by specific regional PD-related patterns of longitudinal decrease in peak alpha frequency (4–12 Hz) when controlling for multiple comparison. In agreement with our findings, Boon et al. found a longitudinal association of lower relative beta band power with worse motor performance (measured as UPDRS III) with a maximum of this effect located in the temporal, occipital and inferior parietal regions7. However, they attributed the progressing reduction in relative beta power to the pathological shift of the overall signal to lower frequencies. In line with this interpretation, a longitudinal increase in theta power in the PD group was associated with more severe motor symptoms across several brain regions sparing the frontal lobe (in sensor space) in the earlier paper reporting longitudinal findings in the same cohort22. These previous results indicating a general progressing oscillatory slowing in PD should be interpreted with caution given our results of a progressive alteration of the aperiodic component. A steeper slope of the aperiodic component could lead to a similar pattern of change even if the underlying oscillatory activity in the theta and alpha / beta frequency ranges, respectively, remained unchanged. Our results offer a new perspective to neurophysiological changes in PD as they emphasize that the most prominent PD-related longitudinal change in resting state neuronal activity is a steepening of the aperiodic slope or aperiodic slowing. Furthermore, we found that longitudinal change in the aperiodic component was associated with clinical progression of bradykinesia and rigidity. Our findings (a relationship of change in the aperiodic and change in clinical symptom severity, but not with absolute values at each timepoint) is in line with recent work on aperiodic activity in the subthalamic nucleus where changes in the aperiodic slope after levodopa intake correlated with motor symptom alleviation25. Within-subject trajectories of the aperiodic component may have larger predictive value of clinical status than static, cross-sectional measures, potentially due to high inter-individual variability.
Computational models and subcortical recordings suggest that an increased exponent of the aperiodic component reflects a shift in the E/I balance towards inhibition (nb, strongest in the 30-70 Hz range which is outside of the scope of this study)1. Yet, this interpretation conflicts with evidence from PD animal models and human spectroscopy studies demonstrating hyperexcitability of pyramidal neurons2, reduced activity of inhibitory interneurons3, and decreased GABA in the motor cortex4, all of which would lead to the opposite change in E/I balance. Pathologically increased neuronal synchrony is a recurrent finding in PD even at the macroscale in MEG studies5. The underlying pathophysiology may involve increased neuronal synchrony generating temporal correlation in both excitatory an inhibitory synaptic inputs that alter the aperiodic component through mechanisms distinct from E/I imbalance6. Steeper aperiodic slopes may instead indicate a reduced repertoire of neural states due to this pathological synchronization, as suggested a strong inverse relationship between aperiodic slope and measures of neural signal diversity7. The methods employed in the present study are not suitable to determine which of these mechanisms constitutes the pathophysiological substrate underlying the observed cross-sectional and longitudinal PD-related changes in aperiodic activity. Nevertheless, the observed relationship between aperiodic exponent and rigidity indicates that our findings are directly relevant to clinical motor symptom progression.
As described in the introduction, the relationship between cortical beta and motor symptoms in PD seems to be more complex than in the subcortex where most studies identified a clear link between higher beta power and more severe bradykinesia or rigidity (see26 for review). Our findings add to the existing cross-sectional evidence for paradoxical effects of PD itself and its treatment on cortical beta activity, challenging the interpretation of beta as universally antikinetic. Interestingly though, studies on cortical beta (oscillations and bursts) still report the strongest relationship with bradykinesia above other motor symptoms (if any)10,21, indicating shared underlying mechanisms. Here, it is also worth noting that negative relationships between cortical beta power and motor symptoms have occasionally been reported before both cross-sectionally27 and longitudinally7. However, in contrast to previous interpretations, we do not consider this relationship to be fully explainable with an oscillatory slowing effect as beta power was increased compared to healthy individuals across many brain regions at both time points in our study. Instead, we argue that parieto-temporo-occipital beta increases may be associated with compensation. Indeed, the temporo-parieto-occipital spatial distribution of this relationship at baseline is in line with recent work from Wiesman et al. reporting (aperiodic) neurophysiological slowing with a similar spatial pattern was associated with less motor symptoms15. Furthermore, roles of the parietal cortex, the posterior cingulate, and occipito-temporal areas for compensation in PD have been postulated before in several fMRI studies28,29,30. Regarding beta activity, elevated beta coherence in the superior parietal cortex as well as between the supplementary motor cortex and the primary motor cortex has previously been discussed as a compensatory mechanism31,32. Different roles of beta activity in different cortical regions may be explained by a proposed functional polymorphism of beta activity33. Potentially, parieto-temporo-occipital beta oscillations may reflect strategies to compensate for impaired subcortical automaticity by leveraging preserved cortical networks for externally-guided movement control. This interpretation is supported by evidence in healthy humans for a role of temporo-occipital beta in mediating top-down attentional control over sensory weighting8. That the negative relationship of parietal beta with bradykinesia tended to weaken over time paralleling clinical progression while it remained intact in clinically stable patients further supports the potential association with compensation. Still, lacking information about the individual degree of subcortical neurodegeneration (and its progression over time), this interpretation remains speculative.
Most cross-sectional predictive MEG/EEG studies in PD so far focused on models for diagnosis or current symptoms rather than prediction of future motor symptoms. Prediction of future clinical progression in PD based on M/EEG data has been most successful in foreseeing cognitive decline34,35,36,37,38.
In our cohort, almost 20% of the longitudinal variation in motor symptom progression could be predicted from baseline resting-state MEG recordings in an early motor disease stage in an independent cohort. Adding basic demographics and motor performance at baseline to the model increased the predictive value to 25% with an average prediction error of 3.5 points in MDS-UPDRS III which is below the threshold that is considered meaningful clinical change23. Hence, our results outperform the few previous neuroimaging studies with external validation of continuous models for future motor progression reporting R² values below 10%39. While the accuracy of our model is still far from clinically useful, these results offer valuable new insights into the relationship between periodic and aperiodic cortical activity and disease mechanisms of PD. It is noteworthy that the aperiodic component tended to be more influential in predicting future motor symptom progression than oscillatory activity at rest. Furthermore, negative loadings of peak beta power as the most influential feature in the right superior and inferior parietal cortex provide additional support for the potential association with compensation discussed above.
Several limitations of our work have to be discussed. First and foremost, the relatively small sample size of our study may have limited statistical power to detect subtle effects and increased the risk of type II errors, potentially leading to an underestimation of true associations between neurophysiological measures and clinical outcomes. However, the use of an independent validation cohort in the predictive part of our study strengthens our findings by demonstrating that the observed relationships can be replicated in a separate sample, thereby reducing concerns about overfitting and chance findings.
We cannot exclude effects of dopamine-replacement therapy on our results because participants were recorded in on-medication state only. The majority of previous studies did not find a significant impact of DRT on cortical activity in resting-state10,14,38,40,41,42,43, but evidence is mixed with some studies pointing towards a levodopa-induced increase in beta power localized to the motor cortex8. Likewise, evidence whether or not the aperiodic component is influenced by dopaminergic medication is mixed. However, recent studies with slightly larger sample sizes comparing on- and off-medication states suggest no acute effect of dopamine replacement therapy on aperiodic slope or offset10,19,21,42,43,44,45,46,47. Still, that all data was collected in on-medication state limits direct comparison with healthy individuals and interpretation of disease-specific neural signatures as treatment effects likely have influenced our results.
In addition, variable times to follow-up might have influenced our results. We accounted for these limitations by interpreting LEDD-adjusted annual clinical change rates in our longitudinal analysis. Still, a linear approach to calculating progression rates may be an oversimplification of the real-life complex and variable clinical trajectories in PD.
Beyond effects of DRT and follow-up period, the lack of significant clinical progression on a group-level is likely in part explained by selection and attrition bias, such as that the least and most severely affected individuals got lost to follow-up. While we can confirm that this was the case in the PD group, we can only assume similar effects in the healthy control group it since we do not have any clinical follow-up data on healthy individuals.
Although it is a strength of our approach that the persons with PD included in the validation were recorded with an identical MEG and MRI protocol at baseline and clinically assessed by the same neurologists at follow-up, we acknowledge that the validation cohort did not perfectly match the training cohort in terms of disease progression (Supplementary Material). The small sample size of our validation cohort precluded matching the distribution of this prediction target between training and validation samples, meaning our validation represents a more stringent out-of-distribution test of model generalization. Here, substantial discrepancy between training and validation performance of our PLS model indicates limited generalizability of the current model to new patients with slightly different clinical progression. These findings thereby do not support clinical utility of our approach to derive personalized predictions for individual patients. They highlight the challenge of reliable biomarker discovery in small neuroimaging cohorts and suggest that either larger sample sizes or alternative analytical approaches may be necessary to achieve clinically meaningful prediction accuracy. Given previous promising results in cross-sectional cohorts, our results still encourage future work including more sophisticated neurophysiological measures, e.g., functional connectivity and complementary non-oscillatory features such as beta bursts10,19,21,40,44,48,49. The identified spatial pattern of predictive brain regions and neurophysiological measures, while biologically plausible, requires validation in larger external cohorts. Optimally, these new patients would be assessed at multiple time points and with even longer follow-up periods in the future to capture individual trajectories of patients with both slow and fast disease progression.
Our results let us to the hypothesis that some of the PD-related beta power increases located in parieto-temporo-occipital regions may be associated with compensation. So far, we focused solely on resting-state activity. Given that we collected data from the same individuals during active and passive motor tasks, we will next test this hypothesis on task-related activity in relation to individual task performance.
Supporting endogenous compensatory mechanisms to delay or reverse clinical disease progression may be a disease-modifying treatment approach. As the cortex is primarily spared from PD-causing pathology, it seems promising to enhance cortical activity patterns associated with compensatory efforts to support the brain’s inherent ability to cope with or eventually overcome neurodegeneration. This potential long-term application of our results requires replication and external validation of our findings.
To conclude, this longitudinal study reveals that resting-state neurophysiological changes in PD are characterized by distinct, functionally heterogeneous alterations that differentially relate to clinical progression. Progressive alteration of the aperiodic component emerged as the most prominent PD-related change over time, showing the strongest correlation with clinical progression of bradykinesia and rigidity. In contrast, oscillatory beta activity demonstrated regional specificity: while beta power was elevated across widespread parieto-temporo-occipital regions in PD compared with healthy individuals, its relationship with clinical symptoms was region-dependent with parietal beta power showing a negative association with bradykinesia, consistent with a potential compensatory role. These findings underscore that neurophysiological alterations in PD reflect a complex interplay between neurodegenerative processes and adaptive compensatory mechanisms. Critically, the ability to predict variability in longitudinal motor progression using these basic neurophysiological features derived from short, non-invasive MEG recordings highlights the clinical relevance of this nuanced understanding and emphasizes the importance of distinguishing between aperiodic and oscillatory components when examining brain activity in PD. These findings warrant future investigations into the predictive value of these neurophysiological signatures and their mechanistic relationship with underlying neurodegenerative and compensatory processes.
Methods
Participants
Participants were enrolled at the Swedish National Facility for MEG (NatMEG, https://natmeg.se/). The study protocol was approved by the responsible ethics committee (Swedish Ethical Review Authority, DNR: 2019-00542) and followed the Declaration of Helsinki. All participants gave written informed consent before participating.
At baseline, a total of 66 cognitively intact patients with PD according to MDS diagnostic criteria and 68 healthy age- and sex-matched individuals were included in the study50. Three years after finishing the initial data collection, we offered a follow-up visit to participants. We decided to include two pre-selection criteria in the PD group based on available clinical follow-up data: Those who suffered from severe PD-dementia, were known to be wheelchair-bound or treated with advanced therapies (deep brain stimulation, intrajejunal levodopa pump) were primarily excluded. A flowchart for details about the recruitment process at follow-up can be found in Supplementary Fig. 1. Twenty-eight patients with PD (42% of the baseline cohort) and 32 healthy individuals (47%) were recruited for the follow-up study with a mean follow-up time of 4.1 ± 0.6 years (Table 1).
Clinical assessment
Clinical assessments and MEG recordings were performed in on-medication state, i.e., after intake of regular dopamine replacement therapy and all participants confirmed that they felt “on” before starting the MEG recording. Motor function was assessed using the motor scale of the Movement Disorder Society-sponsored revised version of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS-III) immediately before or after recording the MEG data51. The MDS-UPDRS-III score was further divided into its symptom-specific subscales, i.e., bradykinesia (items 3.2, 3.4–3.8, 3.14), rigidity (items 3.3a–e), tremor (items 3.15–3.18), and axial symptoms (items 3.1, 3.9–3.13). General cognitive ability was assessed with Montreal Cognitive Assessment (MoCA)52. Levodopa equivalent daily dosages (LEDD) were calculated according to ref. 53.
To account for the confounding effect of medication adjustments on clinical progression, we developed LEDD-adjusted progression rates for the total MDS-UPDRS III and its subscores. Clinical progression was defined as the absolute change in MDS-UPDRS III scores from baseline to follow-up (Δ = follow-up - baseline) such that a positive change score indicates an increase in MDS-UPDRS III or, in other words, a worsening of symptoms. Medication dose change was calculated as the relative change in levodopa equivalent daily dose. To estimate the relationship between medication changes and clinical outcomes, we empirically derived an alpha coefficient by fitting a linear regression model (Supplementary Fig. 2):
Using the estimated alpha coefficient, we calculated the annualized medication-adjusted motor progression as:
Neuroimaging acquisition
The recording procedure was identical at baseline and follow-up and has been described in detail before21. The MEG data was recorded on an Elekta Neuromag TRIUX 306-channel MEG system in a two-layer magnetically shielded room. The MEG system consists for 102 magnetometers and 204 planar gradiometers. Head position and any head movements were continuously recorded with head-position indicator coils (HPI), which were attached to the subjects’ heads and digitalized with Polhemus FASTRAK Motion tracker during the preparations. Electrooculogram (EOG) and electrocardiogram (ECG) were recorded to enable removal of muscle and heartbeat artifacts.
Eyes-open resting-state MEG data were collected using a at a sampling rate of 1000 Hz with an online 0.1 Hz high-pass filter and 330 Hz low-pass filter. Recordings lasted between 5 and 8 min and were conducted with participants in an upright position fixating a centrally presented crosshair. Data from one healthy participant had to be excluded due to technical failure during MEG recordings. Continuous head position was recorded during all except for two sessions (due to technical failure in one healthy control at baseline and one person with PD at follow-up). Empty-room recordings lasting at least 2 min were collected on the same day and were processed using the same pipeline to model environmental noise for source reconstruction.
Source spaces for MEG source reconstruction were created based on individual 3D T1-weighted magnetization-prepared rapid gradient-echo (MPRAGE) sequence structural MRI images (voxel size: 1 x 1 x 1 mm) obtained on a General Electric Discovery 3.0 T MR scanner at baseline, and a General Electric Signa-PremierXT scanner at follow-up, respectively. No structural MRI was available at baseline for seven participants due to restrictions during the Covid-19 pandemic (four HC, three PD), and at follow-up for seven participants with PD and one healthy individual. Baseline images were used in these participants for source reconstructions at follow-up and vice versa. Note that at least one individual MRI scan was available for all participants except for two persons with PD in which an MRI template was used for source reconstruction.
Neuroimaging data processing
Using MaxFilter software54, raw MEG data was pre-processed by applying temporal signal space separation with a buffer length of 10 s and a cut-off correlation coefficient of 0.95 with to suppress artefacts from outside the scanner helmet. Correction for head movements was done by shifting the head position to a position based on the median of the continuous head position.
Additional processing was executed with MNE-Python55 in Python 3.9. Data was 50 Hz-notch filtered to remove line noise, and band-pass filtered between 2 and 47 Hz. The continuous data were cut into 1.0 s epochs to subsequently reject epochs with extreme values or muscle artefacts using 5000 fT for magnetometers and 4000 fT/cm for gradiometers as cut-offs. An independent component analysis was performed using the fastica algorithm56 to identify and remove artefacts from blinks, eye movements (limited to a maximum of two components) and heartbeats (limited to a maximum of three components) based on their correlation with EOG and ECG data, respectively. This resulted in 3.31 ± 1.18 components to be rejected without evidence for a difference between groups or time points.
The individual T1-weighted MRI images were processed with Freesurfer (version 5.3) to obtain surface reconstructions of the cortical mantle using an automatic routine (Freesurfer recon-all). MEG data were co-registered to each individual’s segmented T1-weighted MRI using ~100 digitized head points. The cortex surface was parcellated into 68 ROIs (34 per hemisphere) according to the Desikan-Killiany Atlas57. Noise-weighted minimum-norm estimates with dynamic statistical parametric mapping (dSPM)58 were used for source reconstruction with a source space consisting of 5,124 evenly spaced points sampled across the white matter surfaces. The inner skull boundary was estimated from the MRI to create a single shell volume conductor model. Time series from each ROI were extracted by singular value decomposition of all source points within the respective ROI.
Parametrization of power spectra
The time series data were analysed for its the spectral properties by calculating the power spectral density (PSD) from 1 to 47 Hz across the entire ROI time series using Welch’s method by segmenting the continuous data into 5 s segments with 50% overlap. The aperiodic component of the power spectrum was estimated and subsequently separated from the periodic component (i.e., peaks rising above the aperiodic component representing putative oscillations) using the fitting oscillations & one over f (FOOOF) toolbox16. This parameterizing algorithm fits a log-linear regression to the PSD which is subtracted before fitting Gaussian functions to the peaks in the PSD. The midpoint of the Gaussian function fitted to a given frequency band corresponds to the peak frequency in that frequency band and the height represents the signal power. The fitting parameters were set to a maximum of six peaks, peak threshold of 2 and a minimum peak height of 0.15, with a bandwidth between 1 and 10 Hz. The average R2 of the fit were 0.958 ± 0.028 at baseline and 0.960 ± 0.030 at follow-up for the PD group, and 0.947 ± 0.039 and 0.952 ± 0.032, respectively in the HC group. The estimated aperiodic component was subtracted from the full spectrum to obtain a flattened spectrum for each ROI. Spectral power peaks were initially identified for the theta (4–8 Hz), alpha (8–12 Hz), and beta frequency bands. However, given our relatively small sample and that oscillatory peaks are not expected in all frequency band across all cortical regions, there was a substantial amount of missing oscillatory peaks in the theta and alpha frequencies in many regions. In combination with the fact that the PD group exhibited a trend towards “alpha slowing” (i.e., shift of peak frequency from the lower alpha to the higher theta frequency range, Fig. 1), we therefore decided to extend alpha to include the entire frequency range from 4−12 Hz. A version of the analysis considering alpha and theta frequency ranges separately can be found in the Supplementary Material.
Statistical analysis
As described above, we computed the aperiodic component (exponent and offset) and peak frequency and power at peak frequency in two frequency bands (extended alpha and beta) from 68 ROI (in the following referred to as our variables of interest) from a total of 57 participants divided in two groups and at two timepoints.
Since no whole-cortex outcomes from this cohort at baseline have been reported before, we first compared baseline differences between the groups. To this end, we fit linear regression models with each outcome of interest as dependent variable and group as independent variable controlling for effects of age and sex:
Likewise, associations of neurophysiological measures with motor performance at baseline in the PD group were inferred as follows:
For group comparison of the longitudinal change in each of the pre-defined oscillatory and aperiodic variables of interest, linear mixed-effect models were fitted for each ROI using the lmer4 package in R59 with group*time interaction, age, and sex as fixed effects and subject as random effect:
At baseline, time was set to zero, and at follow-up, time was defined as the number of months since baseline. For significant group × time interactions, post-hoc pairwise comparisons were performed to examine within-group changes over time using the emmeans package. Estimated marginal means were calculated for each group at baseline and 48-month follow-up, and pairwise contrasts were computed to assess the magnitude and significance of longitudinal change within each group separately.
We used an ANCOVA approach to test whether changes in neurophysiological variables of interest that showed a PD-related change over time also correlated with clinical progression, controlling for its baseline value, change in LEDD, and time to follow-up:
False Discovery Rate (FDR) method was used to control for multiple comparison across all models, unless otherwise specified in the text. Visualization of results was achieved using the ggseg package in R.
Prediction of future symptom progression based on baseline neurophysiological data
Given our results presented below indicating that different aspects of the neuronal signal were differentially associated with clinical symptoms, we next wanted to know to which extent the combination of these features is predictive of future clinical progression of motor symptoms across brain regions and how well this prediction is transferable to a new set of persons with PD. To this end, non-demented patients from our baseline cohort who did not participate in the follow-up MEG recordings but for whom clinical follow-up data was available were included in the validation cohort. Note that here only the total MDS-UPDRS III scores were available.
Because of the expected multicollinearity of the features of the neurophysiological signal across brain regions, it was deemed inappropriate to include them into the same mixed model. Instead, we used a combination of Principal Component Analysis (PCA) and Partial Least Square Regression (PLS).
First, baseline neurophysiological variables of interest (aperiodic exponent, aperiodic offset, peak alpha frequency and peak beta power) underwent region-wise PCA to reduce dimensionality while preserving regional neurophysiological signatures. For each brain region, the first principal component (PC1) was extracted, accommodating missing data through dynamic feature selection without imputation. I.e., in case of missing values for one of the oscillatory features, the PCA for this region was calculated considering only the remaining three features. This approach created regional summary scores (i.e., PC1) that captured the dominant pattern of spectral variation within each region. The resulting regional PC1 scores served as predictors in a partial least squares regression to predict the LEDD change-adjusted annual MDS-UPDRS III progression rate. Leave-one-out cross-validation was used to determine the optimal number of PLS components. Next, variable importance was assessed using Variable Importance in Projection (VIP) scores, where regions exceeding VIP > 1.0 are generally considered highly predictive. Model performance was evaluated using coefficient of determination (R²) and root mean square error (RMSE) on both training data and then on the independent external validation cohort (details see below) to assess generalization capability.
Data availability
The full dataset cannot be made publicly available, as the ethical permits for the study do not allow for open data sharing. We have released baseline MEG data used in this analysis in anonymised form50,60. The data is available through the EBRAINS data-sharing platform61. Access to the data requires that the acceptance of the EBRAINS Data Usage Agreement for human data requires all users to create an account and identify themselves using an institutional email address.
Code availability
All custom code used to process the data and run the analysis presented in the paper is available at: https://github.com/JoWld/pd_longitudinal.
References
Albin, R. L., Young, A. B. & Penney, J. B. The functional anatomy of basal ganglia disorders. Trends Neurosci. 12, 366–375 (1989).
Bologna, M., Paparella, G., Fasano, A., Hallett, M. & Berardelli, A. Evolving concepts on bradykinesia. Brain 143, 727–750 (2020).
Kühn, A. A. et al. Event-related beta desynchronization in human subthalamic nucleus correlates with motor performance. Brain 127, 735–46 (2004).
Little, S. & Brown, P. The functional role of beta oscillations in Parkinson’s disease. Parkinsonism Relat. Dis. 1, S44–8 (2014).
Weinberger, M. et al. Beta oscillatory activity in the subthalamic nucleus and its relation to dopaminergic response in Parkinson’s disease. J. Neurophysiol. 96, 3248–3256 (2006).
Heinrichs-Graham, E. et al. Hypersynchrony despite pathologically reduced beta oscillations in patients with Parkinson’s disease: a pharmaco-magnetoencephalography study. J. Neurophysiol. 112, 1739–1747 (2014).
Boon, L. I. et al. Cortical and subcortical changes in MEG activity reflect Parkinson’s progression over a period of 7 years. Brain Topogr 36, 566–580 (2023).
Cao, C. et al. L-dopa treatment increases oscillatory power in the motor cortex of Parkinson’s disease patients. NeuroImage: Clinical 26, 102255 (2020).
Melgari, J.-M. et al. Alpha and beta EEG power reflects L-dopa acute administration in parkinsonian patients. Front Aging Neurosci 6, 302 (2014).
Vinding, M. C. et al. Reduction of spontaneous cortical beta bursts in Parkinson’s disease is linked to symptom severity. Brain Commun. 2, fcaa052 (2020).
Stoffers, D. et al. Slowing of oscillatory brain activity is a stable characteristic of Parkinson’s disease without dementia. Brain 130, 1847–1860 (2007).
Bosboom, J. L. W. et al. Resting state oscillatory brain dynamics in Parkinson’s disease: An MEG study. Clin. Neurophysiol. 117, 2521–2531 (2006).
Olde Dubbelink, K. T. E. et al. Disrupted brain network topology in Parkinson’s disease: A longitudinal magnetoencephalography study. Brain 137, 197–207 (2014).
Stoffers, D., Bosboom, J. L. W., Wolters, E. C., Stam, C. J. & Berendse, H. W. Dopaminergic modulation of cortico-cortical functional connectivity in Parkinson’s disease: An MEG study. Exp. Neurol. 213, 191–195 (2008).
Wiesman, A. I. et al. Adverse and compensatory neurophysiological slowing in Parkinson’s disease. Prog. Neurobiol. 231, 102538 (2023).
Donoghue, T. et al. Parameterizing neural power spectra into periodic and aperiodic components. Nat. Neurosci. 23, 1655–1665 (2020).
Gao, R., Peterson, E. J. & Voytek, B. Inferring synaptic excitation/inhibition balance from field potentials. NeuroImage 158, 70–78 (2017).
Donoghue, T., Schaworonkow, N. & Voytek, B. Methodological considerations for studying neural oscillations. Eur. J. Neurosci. 55, 3502–3527 (2022).
Helson, P., Lundqvist, D., Svenningsson, P., Vinding, M. C. & Kumar, A. Cortex-wide topography of 1/f-exponent in Parkinson’s disease. NPJ Parkinsons Dis 9, 109 (2023).
Monchy, N., Modolo, J., Houvenaghel, J.-F., Voytek, B. & Duprez, J. Changes in electrophysiological aperiodic activity during cognitive control in Parkinson’s disease. Brain Commun. 6, fcae306 (2024).
Vinding, M. C. et al. Oscillatory and non-oscillatory features of the magnetoencephalic sensorimotor rhythm in Parkinson’s disease. NPJ Parkinsons Dis 10, 51 (2024).
Olde Dubbelink, K. T. E. et al. Cognitive decline in Parkinson’s disease is associated with slowing of resting-state brain activity: a longitudinal study. Neurobiol. Aging 34, 408–418 (2013).
Horváth, K. et al. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Parkinsonism Relat. Disord. 21, 1421–1426 (2015).
Vardy, A. N. et al. Slowing of M1 activity in Parkinson’s disease during rest and movement-an MEG study. Clin. Neurophysiol. 122, 789–795 (2011).
Sayfulina, K. et al. Periodic and aperiodic components of subthalamic nucleus activity reflect different aspects of motor impairment in Parkinson’s disease. Eur. J. Neurosci. 61, e16648 (2025).
Chen, L., Chehade, H. D. & Chu, H.-Y. Motor cortical neuronal hyperexcitability associated with α-synuclein aggregation. npj Parkinsons Dis 11, 18 (2025).
Minetti, A. et al. Parkinsonism disrupts cortical function by dysregulating oscillatory, network and synaptic activity of parvalbumin positive interneurons. npj Parkinsons Dis 11, 194 (2025).
van Nuland, A. J. M. et al. GABAergic changes in the thalamocortical circuit in Parkinson’s disease. Hum Brain Mapp 41, 1017–1029 (2020).
Swanson, O. K., Yevoo, P. E., Richard, D. & Maffei, A. Altered thalamocortical signaling in a mouse modelof Parkinson’s Disease. J. Neurosci. 43, 6021–6034 (2023).
Medel, V., Irani, M., Crossley, N., Ossandón, T. & Boncompte, G. Complexity and 1/f slope jointly reflect brain states. Sci. Rep. 13, 21700 (2023).
van Wijk, B. C. M., de Bie, R. M. A. & Beudel, M. A systematic review of local field potential physiomarkers in Parkinson’s disease: from clinical correlations to adaptive deep brain stimulation algorithms. J. Neurol. 270, 1162–1177 (2023).
Miladinović, A. et al. EEG changes and motor deficits in Parkinson’s disease patients: correlation of motor scales and EEG power bands. Procedia Comput. Sci. 192, 2616–2623 (2021).
Sarasso, E. et al. Neural correlates of bradykinesia in Parkinson’s disease: a kinematic and functional MRI study. NPJ Parkinsons Dis 10, 167 (2024).
van Nuenen, B. F. L. et al. Compensatory activity in the extrastriate body area of Parkinson’s disease patients. J. Neurosci. 32, 9546–9553 (2012).
Sparks, H. et al. Dorsal visual stream is preferentially engaged during externally guided action selection in Parkinson disease. Clin Neurophysiol 136, 237–246 (2022).
Pollok, B. et al. Increased SMA–M1 coherence in Parkinson’s disease — Pathophysiology or compensation? Exp. Neurol. 247, 178–181 (2013).
Jenkinson, N. & Brown, P. New insights into the relationship between dopamine, beta oscillations and motor function. Trends Neurosci 34, 611–8 (2011).
Cozac, V. V. et al. Increase of EEG Spectral theta power indicates higher risk of the development of severe cognitive decline in parkinson’s disease after 3 years. Front Aging Neurosci 8, 284 (2016).
Limanowski, J., Litvak, V. & Friston, K. Cortical beta oscillations reflect the contextual gating of visual action feedback. Neuroimage 222, 117267 (2020).
Olde Dubbelink, K. T. E. et al. Predicting dementia in Parkinson disease by combining neurophysiologic and cognitive markers. Neurology 82, 263–270 (2014).
Bertrand, J.-A. et al. Brain connectivity alterations are associated with the development of dementia in parkinson’s disease. Brain Connect 6, 216–224 (2016).
George, J. S. et al. Dopaminergic therapy in Parkinson’s disease decreases cortical beta band coherence in the resting state and increases cortical beta band power during executive control. Neuroimage Clin 3, 261–270 (2013).
Wang, Z. et al. Separating the aperiodic and periodic components of neural activity in Parkinson’s disease. Eur. J. Neurosci. 56, 4889–4900 (2022).
McKeown, D. J. et al. Medication-invariant resting aperiodic and periodic neural activity in Parkinson’s disease. Psychophysiology 61, e14478 (2024).
Olde Dubbelink, K. T. E. et al. Resting-state functional connectivity as a marker of disease progression in Parkinson’s disease: a longitudinal MEG study. NeuroImage: Clin 2, 612–9 (2013).
Pauls, K. A. M. et al. Cortical beta burst dynamics are altered in Parkinson’s disease but normalized by deep brain stimulation. Neuroimage 257, 119308 (2022).
Luo, C. Y. et al. Reduced functional connectivity in early-stage drug-naive Parkinson’s disease: A resting-state fMRI study. Neurobiol. Aging 35, 431–41 (2014).
Kozak, V. V. et al. EEG The Swedish National slowing and axial motor impairment are independent predictors of cognitive worsening in a three-year cohort of pa Parkinson’s disease. Front Aging Neurosci 12, 171 (2020).
Zeighami, Y. et al. Assessment of a prognostic MRI biomarker in early de novo Parkinson’s disease. NeuroImage Clin 24, 101986 (2019).
Vinding, M. C. et al. The Swedish National facility for magnetoencephalography parkinson's disease dataset. Sci. Data 11, 150 (2024).
Goetz, C. G. et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s disease rating scale (MDS-UPDRS): scale presentation and clinimetric testing results: MDS-UPDRS: clinimetric assessment. Mov. Disord. 23, 2129–2170 (2008).
Nasreddine, Z. S. et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatrics Soc. 53, 695–9 (2005).
Tomlinson, C. L. et al. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Dis. 25, 2649–53 (2010).
Taulu, S. & Simola, J. Spatiotemporal signal space separation method for rejecting nearby interference in MEG measurements. Phys. Med. Biol. 51, 1759–68 (2006).
Gramfort, A. et al. MEG and EEG data analysis with MNE-python. Front. Neurosci. 7, 267 (2013).
Hyvarinen, A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans. Neural Netw 10, 626–634 (1999).
Desikan, R. S. et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. NeuroImage 31, 968–980 (2006).
Dale, A. M. et al. Dynamic statistical parametric mapping: combining fMRI and MEG for high-resolution imaging of cortical activity. Neuron 26, 55–67 (2000).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48 (2015).
Vinding, M. C. & Oostenveld, R. Sharing individualised template MRI data for MEG source reconstruction: a solution for open data while keeping subject confidentiality. NeuroImage 254, 119165 (2022).
Vinding, M. C. et al. The Swedish National facility for magnetoencephalography parkinson's disease dataset (v1.0). Sci. Data. 11, 150 (2023).
Acknowledgements
This work was supported by the Swedish Research Council (Project-ID 2021-01593: “Finding a cognitive needle in a neural haystack”). The authors thank Niklas Edvall and Karolina af Edholm for assistance with parts of the data collection, and Pascal Helson and Alex Wiesman for their thoughtful feedback discussing the results. Assistance by AI in the form of a Large Language Model tool (Claude, Anthropic) was used for analysis code review and language improvements of the manuscript.
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
JW: Conceptualization, Methodology, Software, Formal Analysis, Investigation, Data Curation, Writing - Original Draft, Visualization, Supervision, Project administration. IC: Software, Validation, Formal Analysis, Investigation, Data Curation, Writing—Review and Editing, Project administration. DL: Conceptualization, Resources, Writing—Review and Editing, Supervision, Funding acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Waldthaler, J., Comarovschii, I. & Lundqvist, D. Magnetoencephalography-based prediction of longitudinal symptom progression in Parkinson’s disease. npj Parkinsons Dis. 12, 29 (2026). https://doi.org/10.1038/s41531-025-01240-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41531-025-01240-4
