
Abstract
The respiratory syncytial virus (RSV) burden and cost-effectiveness of infant RSV immunisation was evaluated by comparing seven strategies in terms of costs and Quality-Adjusted Life Years (QALYs) from health care payer’s perspective: no universal immunisation, year-round or seasonal maternal vaccination (MV), year-round or seasonal nirsevimab (NmAb) at birth, seasonal NmAb+catch-up for infants ≤ 6-month and a combined MV+NmAb with catch-up strategy. Seasonal NmAb+catch-up averted the most disease, while seasonal MV averted the least, but had the lowest incremental cost-effectiveness ratio (€11,276/QALY gained) at current list prices (MV €186, NmAb €778). Extensive trade-offs between NmAb and MV show at which cost per dose which strategy would be deemed cost-effective. At a willingness to pay of €35,000/QALY gained, seasonal NmAb + catch-up was preferred if NmAb < €210; otherwise, seasonal or year-round MV was preferred when MV < €220 or <€75, respectively. The combined strategy became preferred at low MV and NmAb costs. Besides price level, cost-effectiveness was most sensitive to RSV hospital burden.
Similar content being viewed by others

Introduction
Respiratory syncytial virus (RSV) is a major public health concern in young children, especially infants. It often causes serious illnesses like bronchiolitis and pneumonia, leading to hospitalisation and possibly paediatric intensive care unit (ICU) admissions. In high-income countries, RSV-related lower respiratory tract infections affect about 38.5 per 1000 infants annually, with the highest hospitalisation rates seen in those aged 0–3 months1,2.
A retrospective analysis of the Belgian national hospital discharges reported 8046 RSV-related hospitalisations and 4 in-hospital deaths among infants in the calendar year 2018. Among hospitalised neonates (0–28 days old), 15.9% were referred to ICU3. The associated hospitalisation incidence was 68.3 per 1000 infants <1 year and 5 per 1000 in children aged 1–4 years3. The hospitalisation incidence in infants stands well above typical European estimates of 20–40 per 1000 infants4.
RSV is highly seasonal, with peak activity concentrated typically in the winter months, alongside other respiratory pathogens. This also leads to significant organisational and economic burdens on primary, secondary and tertiary health care services. RSV-related admissions occupied an estimated 20–40% of paediatric hospital beds during the seasonal peak in 20183. Another Belgian regional study estimated that RSV-related hospitalisations in children under 3 years of age cost greater than €26 million from the perspective of the national health insurance system5. In addition, RSV causes important health-related quality of life (HRQoL) losses to both infants and their parents/caregivers6.
Monoclonal antibody palivizumab (Synagis®) has been available since the late 1990s to protect high-risk infants against RSV7, but its use has remained limited due to high cost, monthly dosing and narrow eligibility, prompting the development of broader, more practical immunisation alternatives. In 2022–2023, a single-dose long-acting monoclonal antibody nirsevimab (NmAb, Beyfortus®) and a maternal vaccine (MV, Abrysvo®) were licensed in several high income countries8,9. Another single-dose monoclonal antibody, clesrovimab (Enflonsia®), was also approved in 2025 in the United Sates. In December 2023, Belgian’s National Immunization Technical Advisory Group of the Superior Health Council, recommended using either MV or NmAb for RSV prevention in infants10. MV is recommended for pregnant women between 28–36 gestation weeks expecting to deliver from September to March, unless they are at risk of reduced vaccine effectiveness (e.g. immunocompromised or premature delivery), in which case NmAb is preferred. NmAb is recommended for all infants born to unvaccinated mothers, born prematurely (<30 weeks), or born within 2 weeks of maternal vaccination. It is to be given once at birth or during a routine immunisation visit for healthy infants ≤6 months old, and in high-risk children during their first and second RSV seasons. Both MV and long-acting monoclonal antibodies offer limited duration of protection over one RSV season11,12,13.
Both MV and NmAb were conditionally reimbursed in Belgium, subject to prior authorisation. As of May 2024, NmAb is reimbursed under specific criteria, with reimbursement for full-term infants (≥36 weeks gestation) granted temporarily until May 31, 202614. While the list price is €777.58 per dose (50 mg or 100 mg), the actual reimbursed price remains confidential15. The MV has been reimbursed since January 2025 for pregnancies with an expected delivery date during the RSV season (September–March), at a list price of €186.01 per dose16.
In order to independently inform decision making in Belgium, the current study was requested by regional authorities and coordinated through the Belgian Health Care Knowledge Centre (KCE)17. As such, the study aimed to estimate the disease burden in children under 5 years and to make a full incremental cost-effectiveness and a budget impact analysis of RSV prevention strategies to inform reimbursement, immunisation programme funding and implementation decisions.
Results
RSV-related disease and economic burden
By following the Belgian birth cohort over a 5-year time horizon, we estimated that in the absence of universal RSV immunisation approximately116 thousand RSV cases, including 40 thousand non-medically attended cases, 66 thousand outpatient cases, 8638 non-ICU hospitalisations, 428 ICU admissions and 5 deaths. The highest rates of deaths and hospital admissions occurred in infants aged 0–2 months, while this group had the fewest outpatient and non-medically attended episodes. Overall, RSV was associated with an estimated 968 undiscounted Quality-Adjusted Life Years (QALYs) lost, with over 36% due to mortality in children under 5. From the health care payer’s (HCP) perspective, RSV incurred €43 million undiscounted medical costs, over two-thirds of which were attributable to children under 1 year (Supplementary Table 12).
RSV strategies evaluated
In our base case, the following 5 immunisation programmes were compared to no intervention and to each other through a full incremental cost-effectiveness analysis in base case analysis:
-
‘MV’: Year-round single-dose maternal vaccine during pregnancy.
-
‘NmAb’: Year-round single-dose nirsevimab at birth.
-
‘MV: Sep-Mar’: Seasonal maternal vaccine during pregnancy for infants with a due delivery date from September to March.
-
‘NmAb: Oct-Mar’: Seasonal nirsevimab given at birth for infants born during the RSV season from October to March.
-
‘NmAb: Oct-Mar + catch-up’: Seasonal nirsevimab (as described above) plus a catch-up programme in September for infants (≤6 months) born outside of the RSV season from April to September.
Coverages of 40% and 90% were assumed for MV and NmAb, respectively. In the scenario analysis, we evaluated an additional ‘combined’ strategy defined as
-
‘MV + NmAb: Oct-Mar + catch-up’: Seasonal maternal vaccine (as described above) at 40% coverage, supplemented with NmAb for 90% of infants born during the RSV season and of which the mother was not vaccinated, and an out of season NmAb catch-up programme (as described above).
Impact of RSV interventions on disease and economic burden
The disease burden averted per strategy is reported in Supplementary Table 13. As protection lasts up to 6 months and no infants over 6 months were targeted, the averted disease burden was limited to infants (<1 year). Compared to no intervention, the seasonal plus catch-up NmAb strategy averted the largest RSV burden, preventing nearly 20 thousand cases and gaining 216 discounted QALYs, with €19 million in medical costs averted. The seasonal MV strategy averted the least burden, preventing 3116 cases and gaining 47 discounted QALYs at 40% coverage, and remained the least effective option at equal coverage of 90% (Supplementary Table 14). However, at list prices, the seasonal plus catch-up NmAb strategy incurred the highest intervention cost (€76 million at 90% coverage) due to the large target group and high price (€777.58 per dose)15, whereas the seasonal MV strategy, with 40% coverage and a price of €186.01 per dose16, resulted in a lower intervention cost of €5 million.
Full incremental cost-effectiveness analysis
From health care payer's (HCP) perspective, Supplementary Table 15 presents the incremental cost-effectiveness ratios (ICERs) for each RSV immunisation strategy compared to no intervention, and Supplementary Table 16 reports the ICERs compared to the next best alternatives. The preferred strategy over the range of willingness to pay (WTP) values is shown in Supplementary Fig. 7.
Base case (using list prices as unit intervention costs)
As illustrated in the cost-effectiveness plane (Fig. 1, top panel), the seasonal MV, year-round MV, and seasonal plus catch-up NmAb strategies lay on the frontier at list prices. Compared to no intervention, the seasonal and year-round MV strategies have ICERs of €11,276 and € 48,607 per QALY gained, respectively. All mAb strategies exceeded €250,000 per QALY gained (Supplementary Table 15). Compared to the next best alternative (Supplementary Table 16), the year-round MV strategy had an ICER of €168,938 (versus seasonal MV strategy), and the seasonal plus catch-up NmAb strategy had an ICER of €347,290 (versus year-round MV). Hence, apart from seasonal MV strategy, none of the strategies appear cost-effective at current list prices up to WTP value of €50,000 per QALY gained (Supplementary Fig. 7).

QALY quality-adjusted life year, EUR euro, MV year-round maternal vaccine, MV Sep-Mar seasonal maternal vaccine from September to March, NmAb year-round nirsevimab, NmAb: Oct-Mar seasonal NmAb strategy from October to March, NmAb: Oct-Mar + catch-up seasonal NmAb combined with a catch-up strategy.
Intervention cost parity scenario (deterministic analysis)
Under the cost parity assumption (€200 per dose), the NmAb seasonal and NmAb seasonal plus catch-up strategies formed the frontier, reflecting a shift in efficiency at equal costs (Fig. 1, bottom panel). Compared to no intervention, the seasonal NmAb strategy was borderline cost-saving, with an ICER of €96 per QALY gained, while the seasonal plus catch-up NmAb strategy yielded an ICER of €978 per QALY gained (Supplementary Table 15). When compared with the seasonal NmAb strategy, the seasonal plus catch-up NmAb strategy became preferred at WTP ≥ €1725 per QALY (Supplementary Table 16 and Supplementary Fig. 7).
Bivariate intervention cost probabilistic threshold analysis
All-inclusive per-dose intervention costs were varied, and the full incremental results, comparing 5 strategies to no intervention and to each other, are presented in Fig. 2. From the HCP perspective, using an arbitrary WTP threshold of €35,000 per QALY gained, ‘no intervention’ (blue) was preferred when the costs of MV and NmAb exceeded €240 and €280 per dose, respectively. The seasonal plus catch-up NmAb strategy (yellow) became the preferred option if NmAb costs fell below €210, regardless of the costs of MV. When MV cost relatively less (<€75 per dose) and NmAb cost more (>€220 per dose), the year-round MV strategy (green) was preferred. If MV cost less than €230 and NmAb cost between €220 and €850, seasonal MV strategy (grey) became the preferred strategy.

Y-axis: maternal vaccine costs ranged from €50-€30, X-axis: mAb costs from €50–€850. Each colour indicates a preferred RSV strategy, with the greatest uncertainty at the boundaries where strategies change. EUR euro, QALY quality-adjusted life-year, MV year-round maternal vaccine, MV Sept-Mar: seasonal maternal vaccine from September to March, NmAb: Oct-Mar seasonal NmAb strategy from October to March, NmAb: Oct-Mar + catch-up seasonal NmAb combined with a catch-up strategy.
Additional results for alternative thresholds of €0, €20,000 and €50,000 per QALY gained are provided in the Supplementary Fig. 9. At a higher WTP threshold (i.e. €50,000), similar trends emerged, with the colour pattern shifting right and upward, allowing higher intervention costs to remain cost-effective. At a lower WTP threshold (i.e. €20,000), the pattern shifted left and downward, indicating lower intervention costs were needed for strategies to be preferred.
The seasonal NmAb strategy was not preferred, because the seasonal NmAb was less costly but also less effective than the seasonal plus catch-up NmAb strategy. At the WTP above €20,000 per QALY gained, the seasonal plus catch-up NmAb strategy was preferred due higher QALY gained. The seasonal NmAb strategy could be the preferred strategy only over a narrow NmAb cost per dose range and given a WTP value of €0 per QALY gained. In other words, if policy makers are not willing to pay anything to gain QALYs in the population, then the seasonal NmAb strategy without catch-up could be preferred, when the costs for NmAb are around €200 per dose and for MV > €160 per dose.
The year-round NmAb strategy was dominated by the seasonal plus catch-up NmAb strategy (Fig. 1) and was therefore never preferred or shown in subsequent figures.
In scenario analysis, Fig. 3 presents the inclusion of the ‘combined’ strategy alongside the other separate strategies at an arbitrary WTP threshold of €35,000 per QALY gained. The ‘combined’ strategy (pink) occupied the region where both NmAb and MV costs were relatively low, though assuming MV ≥ €50 per dose. Given a WTP of €35,000 per QALY gained, the ‘combined’ strategy was preferred when MV costed less than NmAb, with NmAb costing between €75 and €250 per dose. Additional results for thresholds of €0, €20,000 and €50,000 per QALY are in Supplementary Fig. 13.

Y-axis: maternal vaccine costs ranged from €50-€30, X-axis: mAb costs from €50–€850. Each colour indicates a preferred RSV strategy, with the greatest uncertainty at the boundaries where strategies change. EUR euro, QALY quality-adjusted life-year, MV year-round maternal vaccine, MV Sept-Mar: seasonal maternal vaccine from September to March, NmAb: Oct-Mar seasonal NmAb strategy from October to March, NmAb: Oct-Mar + catch-up seasonal NmAb combined with a catch-up strategy, NmAb + MV: Oct-Mar + catch-up seasonal MV supplemented with NmAb for infants born during the RSV season and of which the mother was not vaccinated, and an out of season NmAb catch-up programme.
Probabilistic sensitivity analysis
Expected value of partial perfect information (EVPPI) was estimated across WTP thresholds to identify key drivers of decision uncertainty (Supplementary Fig. 10). In the base case using list prices, the most influential parameters were efficacies of MV against hospitalisation and ICU admission, and age-specific outpatient incidence. Under cost parity, NmAb’s efficacy against hospitalisation and ICU admission (assumed equal based on pooled phase 3 RCTs) was the main driver, followed by outpatient incidence, outpatient cost and hospitalisation cost. In both cases, uncertainties in efficacy against hospital and ICU admissions had a much greater impact than all other parameters.
Scenario analysis
A range of scenarios (Supplementary Table 11) were performed to explore sensitivity, uncertainty and identify key drivers. Compared to the HCP perspective, the societal perspective favoured the seasonal MV strategy at a lower WTP threshold using list prices and found the seasonal plus catch-up NmAb strategy to be cost-saving under the cost parity scenario (Supplementary Fig. 11).
As shown in Fig. 4, including recurrent wheezing and asthma up to age 3 years and 13 years significantly affected the results. With list prices, the seasonal plus catch-up NmAb strategy became cost-effective around €22,000 (age 3) and €10,000 (age 13) per QALY gained. Under cost parity, it was cost-saving in both scenarios.

EUR euro, QALY quality-adjusted life-year, MV Sept-Mar seasonal maternal vaccine from September to March, NmAb Oct-Mar seasonal NmAb strategy from October to March, NmAb Oct-Mar + catch-up seasonal NmAb combined with a catch-up strategy. Hosp hospitalisation, QALY quality adjusted life-year, y year, m month, ICD international classification of diseases, NmAb nirsevimab, non-MA non-medically attended, RWE real-world evidence, OP outpatient, S season, NLD the Netherlands. S23to24 RSV season 2023/2024.
Alternative hospital burden scenarios (Fig. 4) would lead to different findings. Hospitalisation burden in infants was estimated using four alternative approaches: (a) 10-season average, (b) primary diagnosis codes only, (c) 2022/2023 age distribution for infants aged 1–11 months and (d) a combination of (b) and (c). Compared to the base case, the cost-effectiveness bars shifted progressively from (a) to (d) approach, indicating that higher WTP thresholds were needed for the seasonal MV (list prices) and NmAb strategies (cost parity) to remain optimal.
Assuming no efficacy against RSV-related deaths led to large changes under list prices, with the seasonal MV strategy requiring a higher WTP (~€27,000 per QALY) to be cost-effective. Under cost parity, the seasonal plus catch-up NmAb strategy needed only slightly higher WTP thresholds (~€200 and ~€2000, respectively shown in Fig. 4 bottom panel). In the base case using list prices, variations in NmAb efficacy had no effect at WTP values below €50,000 per QALY, as no NmAb strategy was cost-effective due to high list price. However, under cost parity (€200), applying pooled RWE effectiveness estimates (i.e. higher than the base case) with 6 months protection17, made NmAb strategies cost-saving. When a shorter 5-month duration of protection was assumed18, the seasonal NmAb strategy became cost-effective above €1200 per QALY, while the seasonal plus catch-up strategy required a higher WTP to be preferred.
Other scenarios, including the use of Dutch and pooled outpatient incidence rates (vs. Spanish data in the base case), no efficacy against non-MA episodes and inclusion of parental QALY losses, had limited impact on the overall results.
Figure 4 also indicates that the ‘combined’ strategy had no impact on the cost-effectiveness results, whether using the list prices or cost parity. NmAb’s list price was too high for either separate or combined strategies to be cost-effective. At cost parity, seasonal NmAb with catch-up, was preferred given its higher effectiveness compared with MV. This result was consistent with Fig. 3, showing that when NmAb was too costly (>€250) or when MV cost the same as NmAb, the combined strategy was not preferred. Additional results for the ‘combined’ strategy can be found in Supplementary Fig. 12, 13.
Budget impact analysis
At 40% coverage, year-round and seasonal MV strategies were estimated to avert €5.1 million and €4.2 million in treatment costs, respectively (Supplementary Table 17). Assuming a €50–€250 per-dose cost range, MV cost range from €2.2–€10.9 million (year-round) and €1.3–€6.3 million (seasonal). At 90% coverage, the seasonal NmAb and seasonal plus catch-up NmAb strategies were projected to reduce treatment costs by €9.8 million and €19.4 million, respectively (Supplementary Table 18). With per-dose costs ranging from €50 to €850, immunisation costs reached €2.4–€41.6 million for seasonal NmAb and €4.9–€83.1 million for the seasonal plus catch-up NmAb strategy.
The Return on Investment (RoI) depended on strategy and assumed cost per dose. Intervention options that use relatively more doses (i.e. year-round and catch-up programmes) require higher investments upfront (Supplementary Table 17, 18). As such, investment cost greater than prevented medical costs (RoI ratio >1) were expected unless all-inclusive per-dose costs fall below €110 for year-round MV, €160 for seasonal MV, €200 for seasonal NmAb and €190 for seasonal plus catch-up NmAb.
Discussion
This analysis assessed the RSV burden in Belgian children under 5 years of age and evaluated the cost-effectiveness and budget impact of MV and NmAb protecting infants up to 6 months. Before the introduction of NmAb in the 2024–25 season, we estimated that RSV caused annually on average 8,638 non-ICU hospitalisations, 428 ICU admissions, 5 deaths and 968 QALYs loss and €43 million in direct healthcare costs (without discounting). Overall, NmAb strategies are expected to prevent a greater RSV disease burden than MV strategies. This is not only due to the expectation that coverage of MV would be markedly lower than coverage of NmAb in the respective target groups (40% versus 90%, respectively), but also due to NmAb’s higher overall efficacy and effectiveness over time. Even when assuming equal coverage, NmAb remained more effective. However, with current list prices (NmAb: €777.58; MV: €186.01)15,16,19, the increased effectiveness does not close the gap in terms of cost-effectiveness.
In the 2024–2025 season, NmAb was administered in hospitals to infants born during the RSV season via an age-based online application system20. However, for those born outside the season, immunisation had not yet been implemented in Mother & Child Clinics (K&G and ONE). Our analysis showed that the seasonal plus catch-up NmAb strategy could achieve the greatest reduction in disease burden, but the out-of-season catch-up presents significant implementation challenges. Administering it just before the RSV season would concentrate operational demands in September and October, covering nearly half the birth cohort. Successful implementation will require coordinated efforts, dedicated funding and adequate resources. On the other hand, the seasonal NmAb strategy was the ‘second-best alternative’ under the cost-parity scenario. It is borderline cost-saving (ICER = €96 per QALY gained at €200 per dose) compared with no intervention. Its implementation might be less challenging, as most Belgian newborns are delivered in hospitals where information and administration can be provided before or shortly after discharge. Nevertheless, our analysis showed that the seasonal plus catch-up NmAb strategy offered the greatest reduction in RSV disease burden and was cost-effective at a low WTP threshold (€1725 vs. seasonal NmAb strategy). If this strategy is implemented, relatively greater efforts would be needed for the catch-up component in the period leading up to the start of the RSV season.
For MV, our analysis showed that the seasonal MV strategy was cost-effective using the current list price as the all-in cost per dose (€186.01), and our bivariate intervention cost sensitivity analyses indicated that the year-round MV strategy could also be the preferred strategy if the MV cost low (<€75 per dose) and the NmAb cost above €220. The experience with maternal pertussis and influenza vaccination in Flanders indicates that gynaecologists typically refer patients to GPs via e-prescription rather than administer vaccines themselves. This referral process requires additional visits to both the pharmacy and GP, adding specific administration costs. The MV also has a narrow immunisation window (28–36 weeks gestation) and, while it can be given with seasonal influenza, it cannot currently be co-administered with the pertussis vaccine10. A coordinated communication strategy may help improve overall coverage of seasonal maternal vaccines.
Alternatively, the ‘combined’ strategy appears interesting in terms of cost-effectiveness, offering pregnant women/parents the choice of maternal vaccination, with the option for NmAb administration in cases of missed opportunities or other concerns. However, this approach would increase programme complexity and require healthcare providers to deliver clear, comprehensive information to support informed decision-making for individuals. Moreover, establishing a comprehensive RSV immunisation administration database is essential to prevent unnecessary repeated injections.
Both MV and NmAb have long been anticipated and are viewed as ‘game changers,’ but they come with very high price tags, especially the list price of €777.58 per dose for nirsevimab in Belgium, which is higher than the US list price of $49521. Our results indicate that prices for both interventions, especially NmAb, would need to be substantially reduced to achieve cost-effectiveness in Belgium. To date, the negotiated price of nirsevimab remains undisclosed in Belgium, as well as in Spain and France, creating transparency challenges for decision makers and the public. For comparison, the average cost of fully vaccinating a child in Europe against multiple pathogens is €33922. Such high list prices created an unsustainable financing scheme for future immunisation strategies.
Beyond intervention costs, results were highly sensitive to RSV hospitalisation burden. The RSV hospitalisation rates in Belgian infants are among the highest in Europe2 and more than double the global average for high-income countries23. This may be partly caused by differences in tertiary care accessibility and patient management practices. Moreover, the number of hospital admissions increased over time prior to the COVID-19 pandemic, despite a gradual decline in the birth cohort size. This trend in reported numbers is likely attributable to several factors, including enhanced diagnostic testing and improved medical coding practices. Additionally, the implementation of other successful childhood (e.g. pneumococcal conjugate and rotavirus vaccination) and maternal (e.g. pertussis and influenza vaccination) immunisation programmes may have contributed to relatively greater availability of paediatric hospital beds during winter seasons, thereby facilitating more admissions.
The impact of RSV immunisation on wheezing and asthma remains uncertain, both in causality and measurement2,24,25,26. However, when modelling potential long-term effects by linking severe infant RSV (proxied by hospitalisations) to later wheezing and asthma, the results showed a substantial influence, making the seasonal plus catch-up NmAb strategy potentially cost-effective even at prices closer to the current list price level.
Although an increasing number of RSV cost-effectiveness analyses have been published in Europe, most have focused on comparing RSV intervention(s) to no universal RSV immunisation, with several estimating cost-effective price thresholds based on specific official or arbitrary WTP thresholds. Conducting economic evaluation without all relevant options can mislead policy. To address this, we conducted a full incremental analysis of all feasible strategies in Belgium, in consultation with national experts. As shown in Supplementary Table 15, 16, the ICERs for the seasonal plus catch-up NmAb strategy were substantially lower (i.e. more attractive) when compared simply to no intervention rather than to the appropriate next best alternative strategy.
Our analysis can be compared with three previously published full incremental cost-effectiveness analyses: in Norway27, in six European countries28, in England29. Our analysis found for comparable intervention options higher threshold intervention costs per dose at which these interventions can be considered cost-effective than Li et al. and Getaneh et al.27,28 found for any of the seven countries using a similar static model structure in 2022–2023. The primary reason is that Belgium has substantially higher RSV-coded hospitalisation rates compared to these countries. Moreover, in our baseline analysis, in addition to assuming that these interventions prevent RSV attributable infant mortality, we were able to use more recent and more favourable information on efficacy and duration of protection (e.g. 6 months duration of protection for both NmAb and MV). Hodgson et al.29 used a dynamic transmission model, comparing four strategies both to ‘no intervention’ and to one another. They also performed a similar two-way threshold analysis using the UK’s official WTP threshold of £20,000 per QALY gained. They concluded that a seasonal NmAb programme could be cost-effective up to £84, while seasonal MV could be cost-effective up to £80 at all-inclusive cost. The main driver of the difference with our findings for Belgium was again the higher hospitalisation incidence rate used in our analysis. Moreover, the National Health Service costs per GP visit (£35), non-ICU admission (£1100) and ICU admission (£2,905) were substantially lower than the corresponding costs in Belgium. Furthermore, Hodgson et al. attributed lower QALY losses for both MA and non-MA episodes29.
This study offers several key strengths. It applied age-specific national disease burden data, representative cost and HRQoL inputs, and pooled clinical evidence from a systematic review to inform the model, supporting evidence-based decision-making. We incorporated a broad range of WTP thresholds and conducted advanced probabilistic sensitivity analyses (including value of perfect information and net loss analyses), scenario analyses and bivariate price threshold analyses in order to enhance the relevance for policymakers, especially in price negotiations and public tender processes. We also used the latest real-world effectiveness data. Finally, we included a ‘combined’ strategy and identified the price ranges for both interventions under which it would become the preferred option.
While the disease burden may be underestimated in some respects, and thus the interventions’ impact somewhat understated, we expect this to remain limited. More importantly, our conservative approach generally ensures that any adjustment for the following limitations would likely strengthen the cost-effectiveness findings rather than weaken them. First, we used a static model that does not capture herd immunity. However, this limitation has also likely minimal impact given that (i) no intervention targets infants over 6 months, (ii) both MV and NmAb offer short-term protection and (iii) infants primarily act as a ‘sink’ rather than drivers of RSV transmission. Furthermore, a formal model comparison using both static and dynamic frameworks for similar RSV interventions showed comparable outcomes when the same input parameters were applied30. Second, some RSV-associated illness, such as otitis media31, was not accounted for in our analysis due to lack of data and therefore the overall health and economic benefits of RSV prevention strategies may be underestimated. Also, we did not account for RSV protection in pregnant women receiving MV, slightly underestimating its impact. However, this is likely minimal as RSV is typically mild in healthy adults. Potential changes to preterm birth risks with MV have not been explored but are also likely to be limited since there is no conclusive evidence to this effect yet32. Furthermore, while our analysis used the current palivizumab programme as the ‘no intervention’ comparator, we did not include potential cost offsets from replacing it with NmAb in high-risk children. This omission is unlikely to affect the preferred strategy, since ‘no intervention’ is already dominated, but it may impact the budget impact analysis. Finally, our model did not assess potential age shifts following infant-targeted immunisation. RSV severity declines sharply after 6 months33,34, and dynamic models show no and limited shift for NmAb and MV, respectively29,34. Real-world evidence is still emerging, but current data suggest that any age shift would not increase severe RSV disease or hospitalisations in children aged 2–5 years, though ongoing surveillance remains important. Similar to previous post-hoc economic evaluations for rotavirus and pneumococcal vaccination strategies, retrospective economic evaluations of different regional or country approaches to RSV interventions would be informative for future evaluations and policy decisions35,36,37,38,39.
Overall, our analysis found the seasonal NmAb with catch-up strategy to be the most effective and the seasonal MV the least effective. However, at current list prices (€186.01 and €777.58 for MV and NmAb, respectively), only the seasonal MV strategy was cost-effective at a WTP threshold below €50,000 per QALY. Bivariate price threshold analysis showed that substantial reductions in per-dose immunisation costs are needed for most strategies to be cost-effective. Apart from interventions’ cost, results were highly sensitive to assumptions about RSV disease burden, especially hospitalisation rate and intervention efficacy against severe outcomes. Future research should also focus on assessing the delivery cost and clarifying the causal link between RSV and subsequent wheezing and asthma.
Methods
This section summarises our methods and key inputs (Table 1). More details are available in the Supplementary file.
Model structure
Static cohort model MCMARCEL27,28,40 was adapted to the Belgian context to reach the objectives stated above. The chosen static modelling approach was in line with WHO guidance41, which considers to be appropriate when herd immunity effects are limited and positive, particularly if supported by evidence from model comparisons, as was the case here30,41. The Belgian birth cohort was followed monthly over a time horizon of 5 years, including both full-term and preterm infants (see Fig. 5). The model incorporates QALY loss and health care costs linked to symptomatic RSV, including outpatient episodes, hospitalisations (with and without ICU), and non-medically attended cases. The evaluation followed Belgian guidelines for economic evaluation and budget impact analysis42,43, adopting the HCP perspective (federal government, federated authorities and patients) in the base case. Uncertainty was explored with value of information analyses44. In the scenario adopting a societal perspective, we included parental productivity losses due to RSV illness in their children using the human capital approach. However, the productivity losses due to premature deaths were not included to avoid double counting. Costs and QALYs beyond one year were discounted at 3% and 1.5%, respectively. All costs were adjusted to 2024 euro values using the healthcare consumer price index. In the absence of an explicitly defined threshold for the WTP for a QALY gain, we explored a range of WTP values (€0 to €50,000 per QALY).

RSV respiratory syncytial virus. § Outpatient visits include primary care consultations (either general practitioners or paediatrician consultation), hospital outpatient consultations and emergency department visits without hospital admission. ±Scenario analysis only: patients with RSV-related hospital admission within the first year of life have age-specific probabilities of (i) recurrent wheezing events up to 3 years of age and (ii) recurrent wheezing and asthma events up to 13 years of age.
Immunisation strategies
We assumed 40% coverage for MV, informed by the first year of the seasonal RSV MV programme in England45 and historical uptake for seasonal influenza and pertussis maternal vaccination in Belgium46,47,48,49. For NmAb, a higher coverage of 90% was assumed, based on uptake levels of comparable early-life immunisations such as the hexavalent vaccine in Belgium50,51,52,53, as well as the high NmAb uptake rates reported in Spain and France54,55. Given all costs are included as variable costs in our static model-based analysis, coverage levels do not impact any of our cost-effectiveness estimates, but they do affect effectiveness and budget-impact estimates.
Model input parameters and assumptions
We systematically searched PubMed to identify recent evidence on RSV burden, healthcare use, costs, and HRQoL in Belgium (details in Table 117). As highlighted in previous research3,5,56,57, data on RSV in outpatient and community settings remain scarce due to limited RSV testing. We therefore included evidence from multi-country European studies and neighbouring countries, after discussions on contextual appropriateness with a Belgian expert panel (see acknowledgements). The most recent Belgian demographic data, including birth cohort size and age-specific58 all-cause mortality rates59, were sourced from the national statistical office (Statbel).
RSV-ICD-coded hospitalisations
RSV-related ICU and non-ICU hospitalisations were analysed using Belgium’s national Technical Cell—Cellule Technique (TCT) database. The TCT obtains anonymised data from all Belgian hospitals and links it with sickness fund billing records. This analysis identified 118,025 episodes in children under 5 years over 14 calendar years (2008–2014 and 2016–2022, 2015 was excluded due to fundamental data issues)17. Overall, RSV-related hospitalisations show clear seasonality from October to March, except during the COVID-19 pandemic, when an atypical peak occurred in May during 2020/21 and hospitalisation numbers remained low without a clear peak in 2021/22.
Over 10 complete pre-COVID-19 pandemic RSV seasons (2008/09 to 2013/14 and 2016/17 to 2019/20), an average of 8,300 RSV-coded hospital admissions occurred annually, with a rising trend despite a decreasing birth cohort. The most recent 4 pre-COVID-19 seasons (2016/17–2019/20), which used consistent ICD-10 coding, were deemed most representative for the post-pandemic period by the Belgian experts and used for our base case (Supplementary Fig. 1 and Supplementary Table 1). Because the TCT database aggregates children aged 1–11 months, we used BELSARI-NET data, a 10-hospital surveillance network, which provided age-specific RSV laboratory confirmed cases from 2023–2025. Data from the 2018/2019 season were used to estimate monthly age-specific RSV hospitalisations (Supplementary Table 2 and Supplementary Fig. 2)60. Various scenarios of using this information were tested.
RSV-ICD-coded deaths in hospital
The RSV-coded in-hospital case fatality rate (hCFR) was estimated using 14 years of TCT data, with 60 RSV-related deaths recorded among Belgian children under 5 years, 27% of which occurred outside the ICU. All RSV-related deaths were assumed to occur in hospital, and age-specific hCFRs (Supplementary Table 3) were applied. Since there is disagreement among clinical experts about the inevitability of infant mortality through RSV immunisation, we also performed scenario analysis assuming no deaths would be preventable by RSV immunisation.
Non-hospitalised RSV
No age-specific incidence rates for RSV-related outpatient consultations, including primary care or emergency department visits, were identified through a published systematic review61 and our own supplementary review. The RESCEU infant study provided both medically attended (MA) RSV-ARI and hospitalisation rates, allowing us to estimate the outpatient rate per country by subtracting the latter from the former, using a lognormal sampling approach (Supplementary Table 4)2. The ComNet study followed children over 3 RSV seasons (2020–2023) in 5 European countries including Belgium62,63. Given similarities in health care use as reported by ComNet 1 to 4-year-olds matched that of the 6–11-month age group.
We also used RESCEU infant study data to estimate age-specific non-MA RSV symptomatic cases as a proportion of all medically attended cases in children under 1 year2,6 (Supplementary Fig. 3).
Resource use, direct and indirect costs
Hospitalisation costs were estimated using TCT data over 14 calendar years, with average costs stratified by age and ICU status. No major cost differences were observed before and after the COVID-19 pandemic (Supplementary Fig. 4). Out of the average total cost of €14,293 per ICU and €3,613 per non-ICU hospital episode in infants (<1 year), most of the costs were covered by national health insurance, while patients co-paid an average of €88 and €23 per ICU and non-ICU hospital episode.
In Belgium, both general practitioners (GP) and paediatricians are directly accessible, so we accounted for the age-and region-specific distribution of consultations between these primary care providers, applying the corresponding unit costs per visit. Age-specific data on the number of visits per RSV outpatient episode and associated medication costs were obtained from the ComNet study62. The estimated outpatient costs per MA and non-MA episode are shown in Supplementary Table 5. For non-MA cases, over-the-counter medication costs of €4.43 were included64,65,66.
Productivity losses, based on Belgian self-reported parental work absence data from ComNet62, were applied only to RSV cases at age above3 months, assuming no such losses during the initial 3 months, given typical maternity leave periods in Belgium (Supplementary Table 6).
Health-related quality of life loss
QALY losses due to RSV infection, based on the RESCEU infant study6, were calculated using the Belgian EQ-5D value set (Supplementary Table 7). As per the Belgian guideline, our base case included only infant QALY losses, but parental losses were also added in scenario analysis. Age-specific health utility values from the population norm67 were applied to the life-years lost due to RSV mortality, to obtain QALY losses due to RSV-related deaths.
Interventions’ characteristics: efficacy, durability, delivery costs and prices
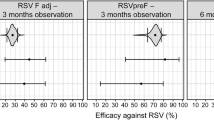
A bespoke systematic review of the literature on efficacy, effectiveness and safety of NmAb and MV was made and can be consulted elsewhere17. The efficacy of NmAb was assessed at 150 days in phase 2b/3 trials68,69,70, but the phase 3b trial demonstrated 180-day efficacy of NmAb against hospitalisation12. The efficacy values of MV were reported at monthly intervals up to 180 days12. Based on expert consensus, the latest trial data were used, in the base case assuming constant 6-month protection for NmAb and time-varying monthly efficacy for MV (Table 1 and Supplementary Fig. 5–6). These assumptions were subjected to sensitivity analysis (Supplementary Table 8).
Distribution and delivery costs, including administration, storage, cold chain, awareness campaigns and wastage, for both products across Belgian regions could not be estimated due to regionally different uncertainties in how the RSV programme of choice would be integrated in the existing programmes. Therefore, we used an all-inclusive per-dose cost approach, through which all purchase and delivery associated costs would be included. We used the current list prices (€186.01 and €777.58 for MV and NmAb, respectively) as a benchmark in the baseline, assuming they include all implementation and delivery costs.
Decision rules of cost-effectiveness analysis
Our study applied standard concepts of dominance, extended dominance based on the ICERs71,72, together with expected net loss curves (ENLCs) to identify the preferred strategy over a range of WTP thresholds44,73, as Belgium’s official guidelines for health economic evaluation explicitly state that no specific WTP threshold should be used42. In line with these guidelines, ICERs should be calculated by comparing each strategy with its next best alternative. The next best alternative strategy is less costly and less effective than the strategy under consideration, but more effective than any of the other strategies. Strongly dominated (more costly and less effective) and weakly dominated (more costly but less cost-effective) strategies are excluded in this process.
We also calculated the expected net loss for each strategy across WTP values from €0 to €50,000 and plotted the ENLCs. The strategy with the lowest expected net loss (i.e. highest expected incremental net benefit) was considered cost-effective. For the preferred strategy, its expected net loss equals the expected value of perfect information (EVPI), which measures decision uncertainty by combining both the probability and the consequence of choosing the wrong option.
Intervention cost analysis
As the negotiated Belgian prices for RSV products in non-high-risk infants are currently unknown, though likely below the public list prices, and given the need for policymakers to compare both products on a consistent cost basis, we additionally analysed a deterministic cost-parity scenario using an all-inclusive unit cost of €200 per dose.
We also applied a novel probabilistic bivariate intervention cost threshold analysis, which identifies threshold values for specific uncertain input parameters while fully accounting for uncertainty in all other model parameters (Pieters et al.)74, using four arbitrary WTP values (€0, €20,000, €35,000 and €50,000 per QALY). MV cost was sampled uniformly between €50–€300 per dose and NmAb cost between €50–€850, allowing us to assess how different cost per dose combinations affect the preferred strategy.
Probabilistic sensitivity analysis
Uncertainty in our economic evaluation was included via a probabilistic sensitivity analysis (PSA) with 1000 samples to obtain cost-effectiveness acceptability curves (CEACs). The EVPPI was used to identify key drivers and quantify the value of reducing their uncertainty.
Scenario analyses
In the scenario analysis, an additional ‘combined’ strategy (as defined above) was included in the full incremental analysis. Extensive scenario analyses also were conducted to account for non-parameterised uncertainty, using alternative data selections and/or sources in relation to hospital burden, efficacy, waning and durability (Supplementary Table 8), as well as adopting a broader societal perspective and including parental QALY losses (Supplementary Table 11). We also assessed the impact of recurrent wheezing (up to age 3) and wheezing with asthma (up to age 13) in infants hospitalised for RSV in their first year, in line with Li et al.27, using the relevant QALY and cost estimates from Belgium (Supplementary Table 9, 10).
Budget impact analysis
A budget impact analysis was conducted in accordance with Belgian guidelines to assess the affordability of implementing a new RSV strategy. Moreover, the RoI ratios were calculated by comparing net savings from the intervention to its cost.
Data availability
The hospital data analysed in this study originate from Belgium’s national Technical Cell – Cellule Technique (TCT) database (project code: KCE Reports 402C), which is managed by the Health Data Agency (HDA) Belgium and accessible via its official website (https://www.hda.belgium.be). Due to legal restrictions, these data were available exclusively for this project and cannot be publicly shared. Aggregated data supporting the findings are reported in this article, its supplementary files, and the KCE report 40217. Requests for access to the TCT data may be submitted to the Health Data Agency.
Code availability
The basic analysis code for this study is publicly available via Zenodo: https://doi.org/10.5281/zenodo.17992863. To facilitate public access to the model methods while preserving data confidentiality, we applied stochastic data perturbation to key epidemiological input data.
References
Li, Y. et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet 399, 2047–2064 (2022).
Wildenbeest, J. G. et al. The burden of respiratory syncytial virus in healthy term-born infants in Europe: a prospective birth cohort study. Lancet Respir. Med. 11, 341–353 (2023).
Bouckaert, N., Lefevre, M., Van den Heede, K. & Van de Voorde, C. RSV burden and its impact on pediatric inpatient bed occupancy in Belgium: an analysis of National hospital claims data. Pediatr. Infect. Dis. J. 42, 857–861 (2023).
Reeves, R. M. et al. Respiratory syncytial virus-associated hospital admissions in children younger than 5 years in 7 European countries using routinely collected datasets. J. Infect. Dis. 222, S599–S605 (2020).
Tilmanne, A. et al. Evaluation of the costs of care for pediatric patients hospitalized for RSV: a retrospective cohort study in Belgium. Vaccine 55, 127065 (2025).
Mao, Z. et al. Economic burden and health-related quality-of-life among infants with respiratory syncytial virus infection: a multi-country prospective cohort study in Europe. Vaccine. https://doi.org/10.1016/j.vaccine.2023.03.024 (2023).
Reeves, R. M. et al. A systematic review of European clinical practice guidelines for respiratory syncytial virus prophylaxis. J. Infect. Dis. 226, S110–S116 (2022).
European Medicines Agency. Beyfortus : EPAR—Product Information, <https://www.ema.europa.eu/en/medicines/human/EPAR/beyfortus> (2022).
European Medicines Agency. Abrysvo : EPAR—Product Information, <https://www.ema.europa.eu/en/medicines/human/EPAR/abrysvo> (2023).
Superior Health Council. Preventive strategies against RSV disease in children, <https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/20231222_shc-9760_advice_rsv_children_vweb.pdf> (2023).
Simoes, E. A. F. et al. Efficacy, safety, and immunogenicity of the MATISSE (Maternal Immunization Study for Safety and Efficacy) maternal respiratory syncytial virus prefusion f protein vaccine trial. Obstet. Gynecol. 145, 157–167 (2025).
Munro, A. P. S. et al. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): a randomised, controlled, phase 3b trial. Lancet Child Adolesc. Health 9, 404–412 (2025).
Zar, H. J. et al. Clesrovimab in infants and children at increased risk for severe RSV disease. N. Engl. J. Med. 393, 1343–1345 (2025).
Rijksinstituut voor ziekte–en invaliditeitsverzekering (RIZIV/INANI). Interpretatieregel voor vergoedingsvoorwaarden Beyfortus® (nirsevimab) na logistieke moeilijkheden, <https://www.riziv.fgov.be/nl/thema-s/verzorging-kosten-en-terugbetaling/wat-het-ziekenfonds-terugbetaalt/geneesmiddelen/interpretatieregel-voor-vergoedingsvoorwaarden-beyfortus-r-nirsevimab-na-logistieke-moeilijkheden> (2024).
Belgisch Centrum voor Farmacotherapeutische Informatie. Beyfortus: list price, <https://www.bcfi.be/nl/chapters/12?frag=8905127&view=pvt&vmp_group=48520> (2024).
Belgisch Centrum voor Farmacotherapeutische Informatie. Abrysvo: list price, <https://www.bcfi.be/nl/chapters/13?frag=mps-8904013> (2025).
Li, X. et al. Cost-effectiveness of new preventive options against RSV infections in Belgian infants. (Belgian Health Care Knowledge Centre (KCE), Brussels, 2025).
Xu, H. et al. Estimated effectiveness of nirsevimab against respiratory syncytial virus. JAMA Netw. Open 8, e250380 (2025).
Rijksinstituut voor Ziekte- en Invaliditeitsverzekering (RIZIV). Vergoedbare Geneesmiddelen en Radio-Farmaceutische Producten, <https://webappsa.riziv-inami.fgov.be/ssp/ProductSearch> (2025).
RIZIV-INAMI. Terugbetaling van Farmaceutische Specialiteiten uit Hoofdstuk IV en VIII: a priori controle, <https://www.riziv.fgov.be/nl/thema-s/verzorging-kosten-en-terugbetaling/wat-het-ziekenfonds-terugbetaalt/geneesmiddelen/geneesmiddel-terugbetalen/vergoedbare-farmaceutische-specialiteiten/lijst-van-farmaceutische-specialiteiten-de-hoofdstukken/terugbetaling-van-farmaceutische-specialiteiten-uit-hoofdstuk-iv-en-viii-a-priori-controle>.
Li, X., Bilcke, J. & Beutels, P. Pricey or priceless: cost-effectiveness of respiratory syncytial virus (RSV) prevention in infants. Lancet Reg. Health Am. 29, 100657 (2024).
Salo, H. et al. Prices of paediatric vaccines in European vaccination programmes. Vaccin. X 15, 100392 (2023).
Li, Y. et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet https://doi.org/10.1016/S0140-6736(22)00478-0 (2022).
Rosas-Salazar, C. et al. Respiratory syncytial virus infection during infancy and asthma during childhood in the USA (INSPIRE): a population-based, prospective birth cohort study. Lancet 401, 1669–1680 (2023).
Scheltema, N. M. et al. Respiratory syncytial virus prevention and asthma in healthy preterm infants: a randomised controlled trial. Lancet Respir. Med. 6, 257–264 (2018).
Zar, H. J. et al. Early-life respiratory syncytial virus disease and long-term respiratory health. Lancet Respir. Med. 12, 810–821 (2024).
Li, X. et al. Cost-effectiveness of respiratory syncytial virus disease prevention strategies: maternal vaccine versus seasonal or year-round monoclonal antibody program in Norwegian children. J. Infect. Dis. 226, S95–s101 (2022).
Getaneh, A. M. et al. Cost-effectiveness of monoclonal antibody and maternal immunization against respiratory syncytial virus (RSV) in infants: Evaluation for six European countries. Vaccine 41, 1623–1631 (2023).
Hodgson, D. et al. Protecting infants against RSV disease: an impact and cost-effectiveness comparison of long-acting monoclonal antibodies and maternal vaccination. Lancet Reg. Health Eur. 38, 100829 (2024).
Li, X. et al. Cost-effectiveness of respiratory syncytial virus preventive interventions in children: a model comparison study. Value Health 26, 508–518 (2023).
Uusitupa, E., Waris, M., Vuorinen, T. & Heikkinen, T. Respiratory syncytial virus-associated hospitalizations in children: a 10-year population-based analysis in Finland, 2008-2018. Influenza Other Respir. Viruses 18, e13268 (2024).
Boytchev, H. Maternal RSV vaccine: further analysis is urged on preterm births. BMJ 381, 1021 (2023).
Antillón, M. et al. The age profile of respiratory syncytial virus burden in preschool children of low- and middle-income countries: a semi-parametric, meta-regression approach. PLoS Med.20, e1004250 (2023).
Giannini, F., Hogan, A. B., Sarna, M., Glass, K. & Moore, H. C. Modelling respiratory syncytial virus age-specific risk of hospitalisation in term and preterm infants. BMC Infect. Dis. 24, 510 (2024).
Chen, C., Beutels, P. & Newall, A. T. Evolution over time in the cost-effectiveness of pneumococcal conjugate vaccine (PCV13) in older Australians due to herd protection from infant vaccination. Vaccine 36, 2057–2060 (2018).
Chen, C. et al. Retrospective cost-effectiveness of the 23-valent pneumococcal polysaccharide vaccination program in Australia. Vaccine 36, 6307–6313 (2018).
Newall, A. T. et al. Retrospective economic evaluation of childhood 7-valent pneumococcal conjugate vaccination in Australia: Uncertain herd impact on pneumonia critical. Vaccine 34, 320–327 (2016).
Newall, A. T. et al. Economic evaluations of implemented vaccination programmes: key methodological challenges in retrospective analyses. Vaccine 32, 759–765 (2014).
Reyes, J. F. et al. Beyond expectations: Post-implementation data shows rotavirus vaccination is likely cost-saving in Australia. Vaccine 35, 345–352 (2017).
Li, X. et al. Health and economic burden of respiratory syncytial virus (RSV) disease and the cost-effectiveness of potential interventions against RSV among children under 5 years in 72 Gavi-eligible countries. BMC Med. 18, 82 (2020).
World Health Organization. WHO Guide for Standardization of Economic Evaluations of Immunization Programmes (World Health Organization, 2019).
Neyt, M., Thiry, N. & Cleemput, I. Belgian Guidelines for Economic Evaluations and Budget Impact Analyses 3rd edn (Belgian Health Care Knowledge Centre (KCE), 2025).
Thiry, N., Neyt, M., Van De Sande, S. & Cleemput, I. Belgian guidelines for economic evaluations: second edition. Int. J. Technol. Assess. Health Care 30, 601–607 (2014).
Bilcke, J. & Beutels, P. Generating, presenting, and interpreting cost-effectiveness results in the context of uncertainty: a tutorial for deeper knowledge and better practice. Med. Decis. Mak. 42, 421–435 (2022).
UK Health Security Agency. RSV Maternal Vaccination Coverage in England: September 2024, <https://www.gov.uk/government/publications/rsv-immunisation-for-older-adults-and-pregnant-women-vaccine-coverage-in-england/rsv-maternal-vaccination-coverage-in-england-september-2024> (2025).
Sciensano. Primary Risk Assessment: Increase in Cases of Pertussis, <https://www.sciensano.be/sites/default/files/20231002_rag_pra_pertussis.pdf> (2023).
Superior Health Council. Maternal Immunisation: Belgian Guidelines, <https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/20201106_shc-8754_maternal_immunisation_vweb.pdf> (2020).
Maertens, K. et al. Coverage of recommended vaccines during pregnancy in Flanders, Belgium. Fairly good but can we do better? Vaccine 36, 2687–2693 (2018).
Theeten, H., Braeckman, T., Maertens, K., Blaizot, S. & Van Damme, P. Studie van de vaccinatiegraad in Vlaanderen 2016 (Vaccinaties Vaccin en Infectieziekten Instituut, Universiteit Antwerpen 2017).
Maertens, K. et al. Studie van de vaccinatiegraad in Vlaanderen. (2022).
World Health Organization & UNICEF. WHO/UNICEF Estimates of National Immunization Coverage, <https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage> (2025).
Robert, E., Swennen, B. & Coppieters, Y. Enquête de couverture vaccinale des enfants de 18 à 24 mois Bruxelles-Capital (ULB—École de Santé Publique, 2020).
Grammens, T. & Cornelissen, L. Couverture vaccinale des vaccinations de base (Sciensano.be, 2021).
Perez Martin, J. J. & Zornoza Moreno, M. Implementation of the first respiratory syncytial (RSV) immunization campaign with nirsevimab in an autonomous community in Spain. Hum. Vaccin Immunother. 20, 2365804 (2024).
Morris, T. et al. Lessons from implementing a long-acting monoclonal antibody (nirsevimab) for RSV in France, Spain and the US. Discov. Health Syst. 4. https://doi.org/10.1007/s44250-025-00198-7 (2025).
Del Riccio, M. et al. Burden of respiratory syncytial virus in the European Union: estimation of RSV-associated hospitalizations in children under 5 years. J. Infect. Dis. 228, 1528–1538 (2023).
Raes, M. et al. The burden and surveillance of RSV disease in young children in Belgium-expert opinion. Eur. J. Pediatr. 182, 451–460 (2023).
STATBEL. Births Annual by District 2008-2023, <https://statbel.fgov.be/en/themes/population/population-movement/births#figures> (2025).
STATBEL. Life Tables, Yearly, in Exact Age, <https://statbel.fgov.be/en/themes/population/mortality-life-expectancy-and-causes-death/life-expectancy-and-life-tables#figures> (2025).
BELSARI-NET. BELSARI-NET Research Group <https://www.sciensano.be/fr/file/belsari-net-research-group> (2025).
Heemskerk, S. et al. Disease burden of RSV infections and bronchiolitis in young children (< 5 Years) in primary care and emergency departments: a systematic literature review. Influenza Other Respir. Viruses 18, e13344 (2024).
Hak, S. F. et al. Burden of RSV infections among young children in primary care: a prospective cohort study in five European countries (2021-23). Lancet Respir. Med. https://doi.org/10.1016/S2213-2600(24)00367-9 (2025).
Sankatsing, V. D. et al. Economic impact of RSV infections in young children attending primary care: a prospective cohort study in five European countries, 2021 to 2023. Euro Surveill 30. https://doi.org/10.2807/1560-7917.ES.2025.30.20.2400797 (2025).
Li, X. et al. Direct and indirect costs of influenza-like illness treated with and without oseltamivir in 15 European countries: a descriptive analysis alongside the randomised controlled ALIC(4)E trial. Clin. Drug Investig. 41, 685–699 (2021).
Hak, S. F. et al. Substantial burden of nonmedically attended RSV infection in healthy-term infants: an international prospective birth cohort study. J. Infect. Dis. 229, S40–S50 (2024).
Li, X. et al. Cost-effectiveness of adding oseltamivir to primary care for influenza-like-illness: economic evaluation alongside the randomised controlled ALIC(4)E trial in 15 European countries. Eur. J. Health Econ. 24, 909–922 (2023).
Van Wilder, L. et al. Belgian population norms for the EQ-5D-5L, 2018. Qual. Life Res. 31, 527–537 (2022).
Hammitt, L. L. et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N. Engl. J. Med. 386, 837–846 (2022).
Muller, W. J. et al. Nirsevimab for prevention of RSV in term and late-preterm infants. N. Engl. J. Med 388, 1533–1534 (2023).
Simoes, E. A. F. et al. Efficacy of nirsevimab against respiratory syncytial virus lower respiratory tract infections in preterm and term infants, and pharmacokinetic extrapolation to infants with congenital heart disease and chronic lung disease: a pooled analysis of randomised controlled trials. Lancet Child Adolesc. Health 7, 180–189 (2023).
Briggs, A. C., K. Sculpher, M. Decision Modelling for Health Economic Evaluation (Oxford University Press, 2006).
Eckermann, S., Briggs, A. & Willan, A. R. Health technology assessment in the cost-disutility plane. Med. Decis. Mak. 28, 172–181 (2008).
Alarid-Escudero, F., Enns, E. A., Kuntz, K. M., Michaud, T. L. & Jalal, H. Time traveling is just too dangerous but some methods are worth revisiting: the advantages of expected loss curves over cost-effectiveness acceptability curves and frontier. Value Health 22, 611–618 (2019).
Pieters, Z., Strong, M., Pitzer, V. E., Beutels, P. & Bilcke, J. A computationally efficient method for probabilistic parameter threshold analysis for health economic evaluations. Med. Decis. Mak. 40, 669–679 (2020).
Bilcke, J., Hens, N. & Beutels, P. Quality-of-life: a many-splendored thing? Belgian population norms and 34 potential determinants explored by beta regression. Qual. Life Res. 26, 2011–2023 (2017).
Bergfors, S., Astrom, M., Burstrom, K. & Egmar, A. C. Measuring health-related quality of life with the EQ-5D-Y instrument in children and adolescents with asthma. Acta Paediatr. 104, 167–173 (2015).
Mayoral, K. et al. Measurement properties of the EQ-5D-Y administered through a smartphone app in children with asthma: a longitudinal questionnaire study. Health Qual. Life Outcomes 20, 51 (2022).
Willems, D. C. et al. Using EQ-5D in children with asthma, rheumatic disorders, diabetes, and speech/language and/or hearing disorders. Int. J. Technol. Assess. Health Care 25, 391–399 (2009).
STATBEL. An Overview of Belgian Wages and Salaries, <https://statbel.fgov.be/en/themes/work-training/wages-and-labourcost/overview-belgian-wages-and-salaries#news> (2024).
Kampmann, B. et al. Bivalent prefusion f vaccine in pregnancy to prevent RSV illness in infants. N. Engl. J. Med. https://doi.org/10.1056/NEJMoa2216480 (2023).
Trusinska, D. et al. Real-world uptake of nirsevimab, RSV maternal vaccine, and RSV vaccines for older adults: a systematic review and meta-analysis. EClinicalMedicine 84, 103281 (2025).
Acknowledgements
This study was co-funded by KCE—Belgian Health Care Knowledge Centre (project number: 2024-51, Health Technology Assessment) and the University of Antwerp centre of excellence VAX-ID/VAXINAID-C2P. The authors would like to thank Nivel: Valerie Sankatsing and Jojanneke van Summeren (Nivel) for providing additional analysis of the ComNet study; Hanmeng Xu and Daniel Weinberger (Yale University) for providing mean of the estimated effectiveness for the nirsevimab in the test-negative case-control study, Louis Bont (Wilhelmina Children’s Hospital in the University Medical Center Utrecht) for granting permission to re-estimate the quality-of-life data collected from the RESCEU prospective birth cohort study. The authors also like to thank Marc De Falleur (INAMI–RIZIV); Yinthe Dockx (Sciensano); Pierre Hubin (Sciensano); Marc Raes (Belgian Academy of Paediatrics) and BELSARI-NET research group https://www.sciensano.be/fr/file/belsari-net-research-group (Sciensano) for providing data and expert opinions, and Olivier Ethgen (Université de Liège (Uliège); Maarten Postma (Rijksuniversiteit Groningen); Daan Van Brusselen (Ziekenhuis aan de Stroom (ZAS)) for their critical review of the KCE study report and valuable comments.
Author information
Authors and Affiliations
Contributions
P.B. and D.R. initiated and supervised the study. X.L., L.W., D.R., J.B. and P.B. conceptualised the study. X.L. analysed input data, performed a literature review and auxiliary data collection. Z.M. performed the literature review as the second reviewer, collected and analysed the health-related quality of life data. L.W., X.L. and J.B. wrote the cost-effectiveness model codes. X.L. performed the cost-effectiveness analyses. C.D.M. conducted national database analyses. N.T. collected and validated data in Belgium. D.C.Z. conducted the systematic review and meta-analysis on efficacy, effectiveness and safety of RSV interventions. P.B., L.W., D.R., N.T., C.D.M., D.C.Z. advised on model parameters, intervention characteristics and scenario analyses. X.L., L.W., P.B. wrote the initial manuscript draft. All authors critically reviewed the manuscript and provided final approval of the manuscript.
Corresponding author
Ethics declarations
Competing interests
Outside the submitted work, P.B. declares no competing non-financial Interests but the following competing financial Interests: funding received by his institute from Merck for research on varicella-zoster and Pfizer for research on pneumococcal vaccine, but he has not received any personal fees or other personal benefits. XL declares no competing non-financial Interests but the following competing financial Interests: funding received by her institute from Icosavax, and from GSK for an educational symposium, as well as consultancy fees received from IQVIA Belgium, all unrelated to the submitted work. Other authors declare no competing financial or non-financial interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Willem, L., Roberfroid, D. et al. Cost-effectiveness of maternal vaccine and/or monoclonal antibody strategies against respiratory syncytial virus in Belgian infants. npj Vaccines 11, 52 (2026). https://doi.org/10.1038/s41541-026-01372-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41541-026-01372-5
