
Abstract
The association between vaccine efficacy (VE) and force of infection (FoI) remains incompletely understood. Previous analyses have been primarily based on trial-level summary data—not accounting for the effect of time and constrained by the number of trials. Here, we leverage individual-level data from three phase 3 randomized, placebo-controlled COVID-19 vaccine trials—the COVE trial (Moderna, CoVPN3001), the AZD1222 trial (AstraZeneca, CoVPN3002), and the ENSEMBLE trial (Janssen/Johnson & Johnson, CoVPN3003)—and contemporaneous geographic-location-specific SARS-CoV-2 surveillance data from the start of the pandemic through November 14, 2021 (including the blinded follow-up periods of the trials) to conduct five cohort- and vaccine-specific analyses: COVE (U.S.), AZD1222 overall (U.S. + non-U.S.), AZD1222 U.S., ENSEMBLE overall (U.S. + non-U.S.), and ENSEMBLE U.S. In AZD1222 U.S., higher VE was associated with higher FoI (p = 0.01). In ENSEMBLE overall, lower VE was marginally associated with higher FoI (p = 0.21), further supported by a region-specific analysis. In COVE, AZD1222 overall, and ENSEMBLE U.S., no VE-FoI association was found. These findings highlighted a new perspective: the VE–FoI association appears complex, potentially influenced by FoI levels, with patterns suggesting an inverted U-shaped relationship, showing a positive association at low FoI levels and a negative association at high levels.
Similar content being viewed by others


Introduction
As of September 2025, more than 40 COVID-19 vaccines have been authorized for use in at least one country1, with variation in population-level vaccine efficacy (VE) reported across vaccine platforms and studies2,3. Such variation likely reflects not only differences between vaccines themselves, but also susceptibility-related population characteristics and exposure-related factors, including regional lifestyle, non-pharmaceutical interventions, seasonal effects, and the prevalence of circulating variants4. These exposure-related factors can be summarized as Force of Infection (FoI), defined as the incidence rate among susceptible individuals5,6,7. The interplay between VE and FoI is often bidirectional. For example, the widespread use of an effective vaccine with high efficacy can significantly curb pathogen transmission within the population, thereby reducing FoI8,9. Conversely, in a high-FoI environment, individuals face a higher load of pathogenic exposure, which may result in more breakthrough infections and a lower VE10. Additionally, VE may be lower in such settings due to the more rapid depletion of susceptible individuals11,12.
Human challenge trials13 offer one way to study this relationship by mimicking different levels of FoI through controlled exposure. Langwig et al.14 predicted that regardless of host susceptibility heterogeneity, VE likely declines with higher pathogen challenge dose from a single exposure or cumulative exposure over time. However, their review found limited empirical support for this prediction, as only a few studies have tested vaccines across a sufficiently broad range of challenge doses. Meanwhile, a household study from Israel, which focused on infections occurring within 10 days of a SARS-CoV-2 diagnosis in another adult member of the same household, found that BNT162b2 mRNA VE was lower than estimates from broader population studies or randomized clinical trials, likely due to the high-risk real-life exposure scenarios15.
Vaccine efficacy trials offer another important source to quantify the association between VE and FoI; however, the feasibility has often been limited by the availability of data with sufficient variability in both VE and FoI. Kaslow16 reported a logarithmic inverse relationship between VE and FoI, i.e., higher VE at lower FoI, for a malaria vaccine, and linear inverse relationships for two orally administered rotavirus vaccine candidates17,18. These findings were based on summary data from a limited number of sites or countries where the clinical trials were conducted, with FoI estimated from the incidence in the placebo group aggregated over time within each site or country. Gjini19 reported an inverse association between VE and FoI for a 7-valent pneumococcal conjugate vaccine using country/territory-level summary data, where FoI was estimated at a single time-point using the prevalence of a capsular serotype of Streptococcus pneumoniae at the beginning of the trial. Additionally, Amin et al.20 observed lower VE of rotavirus vaccine in countries with higher rotavirus burden and noted that adjusting for the rotavirus exposure can reduce the variability in VE estimates across countries.
For COVID-19, Coutinho et al.21 proposed a mathematical model to calculate VE and demonstrated that spurious inverse relationships between VE and FoI can occur when clinical trials are conducted during an outbreak. They also concluded that VE may vary depending on the timing of a clinical trial relative to the peak of the outbreak. However, no quantitative relationship was developed, as VE was based on model simulations. Lastly, Sharma and Anand3 compared 20 phase 3 trials across eight COVID-19 vaccine candidates and found that VE declined as COVID-19 prevalence at trial sites increased. Their analysis was based on trial site-level summary data, with VE estimated cumulatively by a certain time and FoI estimated using prevalence rates averaged over time. As a result, temporal variation in FoI could not be captured, and the association with VE could not be disentangled from vaccine effect waning22,23,24.
In our analyses, we assessed whether VE was associated with FoI, and whether this association differed by COVID-19 vaccine and FoI levels, while addressing some of the limitations in previous investigations as mentioned above. We utilized well-curated participant-level data collected from more than 35,000 placebo recipients and 45,000 vaccine recipients enrolled in three randomized, placebo-controlled COVID-19 vaccine efficacy trials, which together captured 2043 primary endpoints for the analysis. In addition, we incorporated surveillance-data-based FoI estimates linked by geographic locations of trial participants at enrollment. Our analyses accounted for vaccine effect waning over study time, as well as changes in FoI over calendar time that previously reported analyses did not address.
Results
Data linkage and study cohort
As shown in Table 1, for COVE (U.S. only) and AZD1222 (U.S., Peru, and Chile), 100% of the per-protocol participants from the parent studies were included. The ENSEMBLE trial enrolled participants from eight countries; however, due to the unavailability of FoIS data, participants from Brazil and South Africa were excluded from the overall analysis. Baseline characteristics were comparable between the vaccine and placebo groups in our analyses, as the randomization was stratified by site within the parent study.
Trends in FoI S estimates
We found that the trend of FoIS over calendar time closely aligned with the estimated placebo hazard in each trial (Supplementary Fig. 1). This supported the use of FoIS as an estimate for the FoI among trial participants. Importantly, we observed a three- to six- fold variation in FoIS over time in both U.S. and non-U.S. regions, justifying the analyses of its association with VE.
Of note, FoIS estimates in the U.S. were substantially higher in December and January and declined thereafter. During this period, FoIS was the highest in COVE, followed by ENSEMBLE, and then AZD1222. Notably, the histograms of participants’ last dose dates indicate that only COVE participants fully experienced this winter transmission peak. In contrast, most AZD1222 participants in the U.S. received their second dose around the peak. Since endpoints were counted starting 15 days after the second dose, many likely missed the peak period of transmission. This timing difference could explain why the FoIS quantiles are considerably lower for AZD1222 U.S. compared to COVE and ENSEMBLE U.S. (Supplementary Table 1).
Associations between VE and FoI S via multivariable Cox modeling
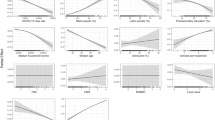
Figure 1 displays the estimated VE at specific FoIS levels based on Cox models that include interactions of the treatment group with both FoIS and time since vaccination, with results for the treatment–FoI interactions presented in Table 2. The interaction coefficient reflects how the hazard ratio between the vaccine and placebo groups changes with FoI. A negative interaction coefficient indicates that a lower hazard ratio, and therefore higher VE, is associated with higher FoI, whereas a positive coefficient indicates that a higher hazard ratio, and therefore lower VE, is associated with higher FoI. For all these models, no evidence of violation of the proportional hazard assumption was observed (Supplementary Fig. 2).

Panels a–e corresponds to results from the COVE, AZD1222 (overall and U.S.), and ENSEMBLE (overall and U.S.) Trials. The values of FoIS in the figure are expressed in units of infections per 1000 person-days. In each panel, from left to right, the values represent the 1st quantile, median, mean, and 3rd quantile. The mean and quantiles were calculated based on daily variations across all participants included in the models. VE was assessed at 45 days since vaccination (post–second dose in COVE and AZD1222 or post–single dose in ENSEMBLE).
Specifically, in the COVE trial, no significant interaction was observed between treatment group and FoIS, suggesting no detectable association between VE and FoIS (Supplementary Table 2a). Similarly, no significant interaction was found in the overall AZD1222 analysis (Supplementary Table 3a). In contrast, the AZD1222 U.S. analysis showed a significant negative interaction coefficient (p = 0.01, Supplementary Table 4), indicating a lower hazard ratio and thus a higher estimated VE was associated with higher FoIS after accounting for vaccine waning. In the overall ENSEMBLE analysis, a higher hazard ratio and thus a lower VE was associated with higher FoIS, as indicated by a positive interaction term between treatment group and FoIS, (p = 0.21, Supplementary Table 5). Figure 2 suggested a similar trend in the ENSEMBLE trial, where lower estimated VE was more evident in regions with higher placebo incidence. No significant trend was observed in the ENSEMBLE U.S. analysis (Supplementary Table 6a). Across all trials, higher FoIS was consistently associated with higher COVID-19 hazard in both vaccine and placebo groups. Detailed results for each trial are further described in Supplementary Information.

VE was estimated using a Cox proportional hazards model without covariates, with confidence intervals calculated via the delta method. Placebo incidence was defined as the number of cases divided by the total person-years of follow-up in the placebo group.
Discussion
To our knowledge, these analyses are the first to investigate the association between VE and FoI using participant-level data from clinical trials and daily FoI estimates derived from surveillance data. The unprecedented COVID-19 pandemic availed such data resources, as part of the necessary public health efforts combating the pandemic via vaccine development and incidence tracking. Another challenge in studying the VE–FoI relationship has been indirect effects5, where VE influences FoI and, in turn, FoI affects VE. The COVID-19 pandemic offered a unique opportunity to isolate this relationship, as the trials we analyzed were conducted among COVID-19 vaccine-naïve populations and completed before the large-scale vaccine rollout, when such effects were minimal.
Leveraging such data from three COVID-19 vaccine efficacy trials and surveillance data of estimated daily SARS-CoV-2 incidence rates, we assessed the association between VE and FoI for these vaccines, accounting for vaccine effect waning and time-varying and location-specific FoI. We summarize these results and provide a brief interpretation below, with further mathematical reasoning provided in Supplementary information. While the interpretations are partly conjectural, the key contribution of the study is the hypothesis that VE-FoI association is complex, varies by vaccine type, and may be influenced by FoI levels.
We found that in the overall (U.S. + non-U.S.) analysis of the ENSEMBLE trial, there was a non-significant inverse association between the estimated efficacy of Ad26.COV2.S and FoI. Such an inverse association aligns with the conclusions presented by Sharma and Anand3. A potential interpretation is that the vaccines under consideration behave like “leaky” vaccines rather than “all-or-none” vaccines25,26. A “leaky” vaccine does not provide complete immunity against a pathogen but instead reduces the likelihood of infection or disease severity upon exposure. Such vaccines result in some breakthrough infections, and their efficacy tends to decline under repeated exposures25. The ENSEMBLE trial included several non-U.S. countries with relatively higher FoI levels during the study period, which may have contributed to reduced VE under sustained exposures.
On the other hand, we found a significant positive association between the estimated efficacy of ChAdOx1 nCoV-19 and FoI in the U.S. cohort of the AZD1222 trial. This was likely due to low FoIS among participants in the U.S. cohort of the AZD1222 trial, suggesting that repeated exposures were likely not a dominant factor. At these lower FoI levels, increases in FoI potentially raised hazard rates more in the placebo group than in the vaccine group, resulting in higher VE.
In addition, we found no significant associations between VE and FoI in the COVE trial, the overall AZD1222 trial, or the U.S. cohort of the ENSEMBLE trial. These results likely reflect that FoIS levels in these trials were moderate relative to the efficacy of each vaccine. For instance, although the FoIS level in the COVE trial was higher than that in the ENSEMBLE U.S. cohort, neither showed an association between VE and FoIS. This may suggest that mRNA-1273 was able to maintain its efficacy even under relatively higher FoI levels.
Circulating variants should be another important consideration, as they can influence both VE and FoI. In the region-specific VE and placebo incidence analysis of ENSEMBLE shown in Fig. 2, although the placebo incidence in South Africa was comparable to that in Mexico, its VE was noticeably lower. This likely could be related to the emerging Delta variant at the time, as nearly all Delta cases during the blinding period occurred in South Africa27.
In comparing the FoI estimates from external surveillance data and the in-trial placebo data, we found aligned time trends but higher magnitudes in surveillance data. This discrepancy likely arose from differences in estimation methods, populations, and definition of endpoints: surveillance-based FoIS were estimated, including seroprevalence surveys capturing symptomatic and asymptomatic infections, while placebo hazards were based on participants enrolled in clinical trials capturing only symptomatic infections. Nonetheless, this discrepancy does not affect the interpretation of our findings. Moreover, unlike prior studies, our use of externally estimated FoI based on surveillance data avoids the entanglement of using placebo data for both FoI and VE estimates. An additional advantage of using external FoI is that it preserves both temporal and geographic variation, whereas placebo-based estimates may be unstable (given the smaller number of COVID-19 cases) when aggregated by location and lose spatial resolution when pooled across sites.
Our analyses have several limitations. First, despite the variability observed over time and across regions, the range of FoIS was still at most six-fold, limiting the statistical power to assess the association between VE and FoI. In the U.S. cohort, more county-level FoIS estimates were linked in the AZD1222 trial, whereas for COVE and ENSEMBLE, approximately 35% of FoIS estimates used in the analyses were at the state level, potentially reducing power. In the overall ENSEMBLE analysis, FoIS for non-U.S. participants were assessed at the country level, and the exclusion of Brazil and South Africa may have further diminished power.
Second, we did not account for variant lineages in the analysis, particularly in the overall analysis of ENSEMBLE, where circulating variants differed across non-U.S. countries. Our interpretation did not explore differences in vaccine platforms (which vary in immunogenicity) or disease severity (which may differ across FoI levels). All cases were treated equally in our analyses once they met the endpoint criteria, regardless of severity.
Third, the multivariable Cox model we used captures only the overall association between VE and FoI, limited by its ability in capturing dynamic changes in this relationship. Future work may apply the method proposed by Bellavia et al.28, which allows for modeling more complex interaction effects among covariates. Lastly, this study focused on assessing the association between VE and FoI, without establishing a causal relationship29.
Despite these limitations, this study complements previous investigations of the VE–FoI relationship by using individual-level trial data together with large-scale surveillance data. This is particularly valuable given the unique opportunity provided by the COVID-19 pandemic to revisit this question. Importantly, the findings suggest a new hypothesis that the relationship may vary in direction, potentially influenced by both VE and FoI.
A clear understanding of this relationship can inform both vaccine evaluation and development. Vaccine trials typically include multiple sites, a well-established design feature that accounts for heterogeneity in FoI. However, for single-site trials, the local FoI level should be considered as a potential explanatory variable. Likewise, when translating trial results into public health decisions, it is important to take the local FoI into account to ensure that findings are appropriately adapted to local needs. For the development of vaccines, particularly preventive vaccines against pathogens with relatively low incidence, the initial choice of trial site should carefully consider local FoI. A lower FoI reduces the risk of overwhelming exposure, but also implies that a larger cohort or longer follow-up would be needed to accrue a desired number of cases to achieve sufficient statistical power for VE assessment, making such trials more time- and resource-intensive. In contrast, very high FoI may dampen the efficacy of a candidate vaccine, as shown in our analysis. A moderate-FoI setting may therefore be preferable at the outset, with trials expanded to higher-FoI regions as development progresses.
In summary, we investigated the association between the efficacy of three COVID-19 vaccines and FoI, using individual-participant-level data and incorporating time-varying, location-specific FoI estimates for each trial participant. Our results indicate that the association between VE and FoI may differ by vaccine and FoI level: at lower FoI levels, higher VE was associated with increasing FoI, whereas at higher FoI levels, lower VE was associated with increasing FoI. While these findings require validation in future studies, they suggest that the VE-FoI association may be complex, potentially inverted U-shaped, offering new perspectives on the VE-FoI relationship and on incorporating FoI into future vaccine evaluation and development.
Methods
COVID-19 vaccine trial data
We incorporated data from the Moderna COVE trial of mRNA-1273 (CoVPN3001, ClinicalTrials.gov number: NCT04470427)30,31, the AstraZeneca/Oxford AZD1222 trial of ChAdOx1 nCoV-19 (CoVPN3002, NCT04516746)32,33, and the Janssen/Johnson & Johnson ENSEMBLE trial of Ad26.COV2.S (CoVPN3003, NCT04505722)27. These trials were funded by the U.S. government and conducted under the Operation Warp Speed program, with operational leadership provided by the COVID-19 Prevention Network (CoVPN)34,35,36,37.
Our analyses focused on the blinded periods of these trials (Table 3), during which participants received either mRNA-1273 (two doses, 28 days apart), ChAdOx1 nCoV-19 (two doses, 28 days apart), Ad26.COV2.S (one dose), or placebo27,30,33. The primary endpoint was virologically confirmed COVID-19, with definitions slightly differing across the trials38. As reported previously, the VE of mRNA-1273 was 93.2% (95% CI: 91.0–94.8) over a median follow-up of approximately 4 months after the second dose30. For ChAdOx1 nCoV-19, VE was 67.0% (95% CI: 58.9–73.5) overall (i.e., among all participants, U.S.+ non-U.S.) and 72.3% (95% CI: 64.1–78.5) among U.S. participants33, based on a median follow-up of 2.5 months after the second dose. The VE of Ad26.COV2.S was 52.9% (95% CI: 47.1–58.1) overall and 69.7% (95% CI: 60.7–76.9) among U.S. participants27, based on a median follow-up of 4 and 3.5 months after the single dose, respectively. Local or central institutional review board and ethics committee approvals were obtained by each site; all participants provided written informed consent prior to participating.
FoI estimates from surveillance data
Daily FoI estimates based on surveillance data, denoted as FoIS, were sourced from the Institute for Health Metrics and Evaluation (IHME)39,40. These estimates were derived from a model that integrated data from Johns Hopkins University and national databases41, incorporating reported COVID-19-associated hospitalizations and deaths, as well as SARS-CoV-2 seroprevalence surveys39,42. In this database, FoIS was defined as the number of new infections on a given day divided by the total population who could possibly get infected that day (at risk) in the region, regardless of vaccination status or prior infection history42. In the U.S., state-level estimates were available for all states except Alaska, and county-level data were available for 109 counties, 80 of which had at least one clinical site enrolling participants in one of the trials included in our analyses. Outside the U.S., country-level estimates were available for Peru, Chile, Argentina, Mexico, and Colombia.
Linkage between trial data and surveillance data
To obtain the daily-grid time-varying FoIS, we linked each participant’s trial site with the corresponding location in the IHME surveillance database. For U.S. participants, we used county-level FoIS when available and state-level FoIS otherwise. For non-U.S. participants, we used country-level FoIS. We also estimated hazard rates for the placebo arms in each trial using a nonparametric kernel smoothing method43 to assess whether the linked FoIS values captured the temporal incidence patterns observed among placebo recipients.
Multivariable Cox model incorporating daily-varying FoI S
We modeled the hazard of COVID-19 using a covariate-adjusted Cox regression model, applied separately to data from each of the three trials overall (U.S. + non-U.S.) and to the U.S. cohorts of the AZD1222 and ENSEMBLE trials. Analyses were conducted in the per-protocol populations, as defined in each parent trial27,30,33, among baseline SARS-CoV-2-negative participants who received the full vaccine regimen (two doses for COVE and AZD1222, one dose for ENSEMBLE). We adjusted for age, sex, and race as potential confounders, with their distributions summarized in Table 3.
Data were analyzed in the calendar time scale to incorporate daily FoIS. We included an interaction term between time-varying FoIS and treatment group (vaccine or placebo) to examine whether VE remained constant across varying levels of FoIS44. To account for potential vaccine effect waning, we also included an interaction term between treatment group and time since the most recent vaccination45,46. Interaction terms with p-values greater than 0.05 were excluded from the final models to improve interpretability. Schoenfeld residuals were used to assess the proportional hazards assumption for the time-invariant covariates47.
Region-specific VE and placebo incidence in the ENSEMBLE trial
For ENSEMBLE, we derived region-specific VE and placebo incidence estimates to examine their relationship. Specifically, U.S. participants were categorized into four regional cohorts: Northeast, Midwest, South, and West, following the United States Census Bureau’s classification48. Non-U.S. participants from South Africa, Brazil, Colombia, Argentina, Peru, Chile, or Mexico were each treated as a separate regional cohort, resulting in a total of 11 regions. For each region, VE was estimated using a Cox proportional hazards model without covariates, and confidence intervals were obtained using the delta method. Region-specific placebo incidence was computed as the number of cases divided by the total person-years of follow-up among placebo recipients in that region. This analysis was not performed for the COVE and AZD1222 trials, due to the smaller number of regions (4 and 6, respectively).
All analyses were conducted in R version 4.4.149 using the survival package50.
Ethics
The primary clinical trials were approved by their respective institutional review boards, and informed consent was obtained as described in the parent studies.
Data availability
COVE: Requests to use the data can be made to Moderna Inc., 325 Binney Street, Cambridge, MA 02142, USA. A materials transfer and/or data access agreement with the sponsor will be required for accessing shared data. AstraZeneca AZD1222: AstraZeneca’s data sharing policy is described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure. AstraZeneca Group of Companies allows researchers to submit a request to access anonymized patient-level clinical data, aggregate clinical or genomics data (when available), and anonymized clinical study reports through the Vivli web-based data request platform. Janssen ENSEMBLE: The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at https://www.janssen.com/clinical-trials/ transparency. As noted on this site, requests for access to the study data can be submitted through the Yale Open Data Access (YODA) Project site at http://yoda.yale.edu.
References
World Health Organization. Status of COVID-19 Vaccines within WHO EUL/PQ evaluation process, https://extranet.who.int/prequal/sites/default/files/document_files/Status_COVID_VAX_08AUgust2023.pdf (2023).
Rapaka, R. R., Hammershaimb, E. A. & Neuzil, K. M. Are Some COVID-19 Vaccines Better Than Others? Interpreting and Comparing Estimates of Efficacy in Vaccine Trials. Clin. Infect. Dis. 74, 352–358 (2022).
Sharma, R. & Anand, A. The effect of pandemic prevalence on the reported efficacy of SARS-CoV-2 vaccines. PLoS One 17, e0266271 (2022).
Xu, S. et al. Real-world effectiveness and factors associated with effectiveness of inactivated SARS-CoV-2 vaccines: a systematic review and meta-regression analysis. BMC Med. 21, 160 (2023).
Halloran M. E., Longini I. M. & Struchiner C. J. Design and Analysis of Vaccine Studies. (Springer New York, NY, 2010).
Anderson, R. M. & May, R. M. Infectious Diseases of Humans: Dynamics and Control. (Oxford University Press, 1991).
Keeling, M. J. & Rohani, P. Modeling Infectious Diseases in Humans and Animals. (Princeton University Press, 2008).
Fine, P. E. Herd immunity: history, theory, practice. Epidemiol. Rev. 15, 265–302 (1993).
Orenstein, W. A., Douglas, R. G., Rodewald, L. E. & Hinman, A. R. Immunizations in the United States: success, structure, and stress. Health Aff. 24, 599–610 (2005).
Amanatidou, E. et al. Breakthrough infections after COVID-19 vaccination: Insights, perspectives and challenges. Metab. Open 14, 100180 (2022).
Lipsitch, M., Goldstein, E., Ray, G. T. & Fireman, B. Depletion-of-susceptibles bias in influenza vaccine waning studies: how to ensure robust results. Epidemiol. Infect. 147, e306 (2019).
Halloran, M. E., Longini, I. M. Jr & Struchiner, C. J. Estimability and Interpretation of Vaccine Efficacy Using Frailty Mixing Models. Am. J. Epidemiol. 144, 83–97 (1996).
Adams-Phipps, J. et al. A systematic review of human challenge trials, designs, and safety. Clin. Infect. Dis. 76, 609–619 (2023).
Langwig, K. E. et al. Limited available evidence supports theoretical predictions of reduced vaccine efficacy at higher exposure dose. Sci. Rep. 9, 3203 (2019).
Gazit, S. et al. BNT162b2 mRNA Vaccine Effectiveness Given Confirmed Exposure: Analysis of Household Members of Coronavirus Disease 2019 Patients. Clin. Infect. Dis. 75, e734–e740 (2022).
Kaslow, D. C. Force of infection: a determinant of vaccine efficacy?. NPJ Vaccines 6, 51 (2021).
Efficacy and safety of RTS, S/AS01 malaria vaccine with or without a booster dose in infants and children in Africa: final results of a phase 3, individually randomised, controlled trial. Lancet 386, 31–45 (2015).
Madhi, S. A. et al. Effect of human rotavirus vaccine on severe diarrhea in African infants. N. Engl. J. Med. 362, 289–298 (2010).
Gjini, E. Geographic variation in pneumococcal vaccine efficacy estimated from dynamic modeling of epidemiological data post-PCV7. Sci. Rep. 7, 3049 (2017).
Amin, A. B., Waller, L. A., Tate, J. E., Lash, T. L. & Lopman, B. A. Accounting for local incidence when estimating rotavirus vaccine efficacy among countries: a pooled analysis of monovalent rotavirus vaccine trials. Am. J. Epidemiol. https://doi.org/10.1093/aje/kwae467 (2024).
Coutinho, F. A. B. et al. Analysing vaccine efficacy evaluated in phase 3 clinical trials carried out during outbreaks. Infect. Dis. Model 9, 1027–1044 (2024).
Menegale, F. et al. Evaluation of waning of SARS-CoV-2 Vaccine-Induced Immunity: A Systematic Review and Meta-analysis. JAMA Netw. Open 6, e2310650 (2023).
Dolgin, E. COVID vaccine immunity is waning - how much does that matter?. Nature 597, 606–607 (2021).
Lin, D. Y., Zeng, D., Gu, Y., Krause, P. R. & Fleming, T. R. Reliably assessing duration of protection for Coronavirus Disease 2019 Vaccines. J. Infect. Dis. 226, 1863–1866 (2022).
Halloran, M. E., Haber, M., Longini, I. M. Jr & Struchiner, C. J. Direct and indirect effects in vaccine efficacy and effectiveness. Am. J. Epidemiol. 133, 323–331 (1991).
Halloran, M. E. & Struchiner, C. J. Thirty-five years of leaky vaccines. Am. J. Epidemiol. 194, 918–920 (2025).
Sadoff, J. et al. Final analysis of efficacy and safety of single-dose Ad26.COV2.S. N. Engl. J. Med 386, 847–860 (2022).
Bellavia, A., Melloni, G. E. M., Park, J. G., Discacciati, A. & Murphy, S. A. Estimating and presenting hazard ratios and absolute risks from a Cox model with complex nonlinear interactions. Am. J. Epidemiol. 193, 1155–1160 (2024).
Pearl, J. Causal inference in statistics: An overview. Stat. Surv. 3, 96–146 (2009).
El Sahly, H. M. et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med 385, 1774–1785 (2021).
Baden, L. R. et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 384, 403–416 (2021).
Falsey, A. R. et al. Phase 3 safety and efficacy of AZD1222 (ChAdOx1 nCoV-19) Covid-19 Vaccine. N. Engl. J. Med 385, 2348–2360 (2021).
Sobieszczyk, M. E. et al. Durability of protection and immunogenicity of AZD1222 (ChAdOx1 nCoV-19) COVID-19 vaccine over 6 months. J. Clin. Invest. 132, https://doi.org/10.1172/JCI160565 (2022).
Collins, F. S. & Stoffels, P. Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV): An Unprecedented Partnership for Unprecedented Times. JAMA 323, 2455–2457 (2020).
Corey, L., Mascola, J. R., Fauci, A. S. & Collins, F. S. A strategic approach to COVID-19 vaccine R&D. Science 368, 948–950 (2020).
Mena Lora, A. J. et al. Rapid Development of an Integrated Network Infrastructure to Conduct Phase 3 COVID-19 Vaccine Trials. JAMA Netw. Open 6, e2251974 (2023).
National Institutes of Health. NIH to launch public-private partnership to speed COVID-19 vaccine and treatment options, https://www.nih.gov/news-events/news-releases/nih-launchpublic-private-partnership-speed-covid-19-vaccine-treatment-options.
Theodore, D. A. et al. Clinical and Demographic Factors Associated With COVID-19, Severe COVID-19, and SARS-CoV-2 Infection in Adults: A Secondary Cross-Protocol Analysis of 4 Randomized Clinical Trials. JAMA Netw. Open 6, e2323349 (2023).
Covid-Cumulative Infection Collaborators Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet 399, 2351–2380 (2022).
Wang, H. Estimation of total and excess mortality due to COVID-19 https://www.healthdata.org/research-analysis/diseases-injuries/covid/estimation-total-and-excess-mortality-due-covid-19 (2021).
Johns Hopkins Coronavirus Resource Center. COVID-19 United States Cases by County. https://coronavirus.jhu.edu/us-map (accessed January 15, 2026).
Moore, M. et al. Estimating vaccine efficacy during open-label follow-up of COVID-19 vaccine trials based on population-level surveillance data. Epidemics 47, 100768 (2024).
Gilbert, P. B., Wei, L. J., Kosorok, M. R. & Clemens, J. D. Simultaneous inferences on the contrast of two hazard functions with censored observations. Biometrics 58, 773–780 (2002).
Cox, D. R. Interaction. Int. Stat. Rev. 52, 1–24 (1984).
Lin, D. Y. et al. Effectiveness of Covid-19 Vaccines over a 9-Month Period in North Carolina. N. Engl. J. Med. 386, 933–941 (2022).
Wolkewitz, M. et al. Multiple time scales in modeling the incidence of infections acquired in intensive care units. BMC Med. Res. Methodol. 16, 116 (2016).
Schoenfeld, D. Partial Residuals for The Proportional Hazards Regression Model. Biometrika 69, 239–241 (1982).
United States Census Bureau. Guidance for Economic Census Geographies Users: Geographic Levels, https://www.census.gov/programs-surveys/economic-census/guidance-geographies/levels.html.
R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/ (accessed January 15, 2026).
A Package for Survival Analysis in R. 2024. Accessed May 16, https://CRAN.R-project.org/package=survival (2025) (accessed January 15, 2026).
Acknowledgements
The authors would like to thank the participants and site staff who contributed to the COVE, AZD1222, and ENSEMBLE trials. The COVID-19 Prevention Network (CoVPN) members are listed in Supplement 2. In addition, the authors thank the broader contributors from all vaccine developers: Moderna Inc., AstraZeneca, and Janssen Vaccines and Prevention BV. The authors thank the Institute for Health Metrics and Evaluation at the University of Washington for their provision of the force of infection estimates to Dr. Moore. This research was funded by grants UM1 AI068635 from the HIV Vaccine Trials Network Statistical and Data Management Center, UM1 AI068614 from the HIV Vaccine Trials Network Leadership and Operations Center, and the Faculty New Development Fund from Fred Hutchinson Cancer Center (Dr. Huang). The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the NIH.
Author information
Authors and Affiliations
Contributions
Xu and Huang had full access to all of the data in the study and took responsibility for the integrity of the data and accuracy of the data analysis. Concept and design: Xu, Halloran, Huang. Acquisition, analysis, or interpretation of data: Xu, Halloran, Moore, El Sahly, Baden, Goepfert, Gray, Grinsztejn, Sobieszczyk, Falsey, Zhou, Dromme, Truyers, Hirsch, Neuzil, Corey, Follmann, Janes, Gilbert, Huang. Drafting of the manuscript: Xu, Robinson, Huang. Critical review of the manuscript for important intellectual content: All authors. Statistical analysis: Xu, Halloran, Zhou, Hirsch, Truyers, Follmann, Janes, Gilbert, Huang. Obtained funding: Neuzil, Corey, Janes, Gilbert, Huang. Administrative, technical, or material support: Garcia, Moore, Huang. Supervision: Neuzil, Corey, Janes, Gilbert, Huang.
Corresponding author
Ethics declarations
Competing interests
Dr Sobieszczyk reported receiving grant support to the institution from the NIH during the conduct of the study and grant support to the institution from the Gates Foundation, Sanofi SA, Merck, Sharpe and Dohme, and Gilead Sciences Inc. outside the submitted work. Dr El Sahly reported receiving grant support from the NIAID during the conduct of the study. Dr Baden reported receiving grant support from the NIH during the conduct of the study. Dr Falsey reported receiving grant support from AstraZeneca during the conduct of the study and grant support from AstraZeneca, Pfizer Inc., and CyanVac LLC, and personal fees for serving on an advisory board from Merck & Co. Inc., GSK, ADMA Biologics Inc., and Moderna Inc. outside the submitted work. Dr Hirsch reported holding stock or stock options in AstraZeneca. Dr Neuzil reported receiving grant support from Pfizer Inc. and the National Institutes of Health (NIH) during the conduct of the study. Dr Janes reported receiving grant support from the NIH during the conduct of the study. Dr Gilbert reported receiving grant support to the institution from the NIAID and NIH during the conduct of the study and serving on the vaccine scientific advisory boards for Moderna Inc. and AstraZeneca. Dr Huang reported receiving grant support from the NIH during the conduct of the study. All other authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, J., Halloran, M.E., Moore, M. et al. Association between COVID-19 vaccine efficacy and epidemic force of infection. npj Vaccines 11, 54 (2026). https://doi.org/10.1038/s41541-026-01374-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41541-026-01374-3
