
Abstract
Cranial nerves densely innervate the heart and vasculature, with sensory neurons reporting on blood pressure, respiratory gases and tissue damage1. The roles of arterial baroreceptors in systemic physiology are well appreciated2, but the functions of vagal cardiac mechanoreceptors have been more difficult to parse, in part due to the closed-loop structure of the cardiovascular system. Here we use genetic tools in mice to identify a small group of neurons that are acutely sensitive to circulating blood volume and initiate a reflex that compensates for decreased filling of the heart in an upright posture and haemorrhage. Vagal PIEZO2 neurons form characteristic end-net endings in the heart, lower blood pressure in response to optogenetic stimulation and display blood-volume-dependent responses with every heartbeat that are time-locked to atrial and ventricular systole. Knockout of Piezo2 and/or ablation of PIEZO2 neurons in vagal ganglia eliminates this heartbeat-coupled nerve activity, causes orthostatic hypotension and compromises cardiovascular stability during trauma-induced blood loss. Together, these findings demonstrate that vagal mechanoreceptors monitor the cardiac cycle and initiate a blood-volume-dependent reflex that defends the constancy of circulation.
Similar content being viewed by others

Main
The brain supervises the physiology of our internal organs to ensure bodily homeostasis. Sensory signals from the body provide constant feedback to the brain about the ongoing performance of each major physiological system3. Within the cardiovascular system, specialized sensory neurons report on the pressure, volume and chemical composition of blood to ensure appropriate cardiac output and tissue perfusion1,4,5,6. Neuronal surveillance helps to enable adaptation to environmental stressors such as reduced oxygen during a high-altitude hike or the effect of gravity on blood circulation when standing up. Failure to regulate blood pressure, even for a moment, can lead to dizziness, fainting and injury7. Moreover, cardiovascular signals can drive some of our most basic emotions, as optogenetic induction of a racing heart can cause anxiety8. The heart–brain axis therefore provides essential control over physiology, behaviour and mood.
The vagal and glossopharyngeal nerves provide the dominant sensory innervation of the heart and nearby vasculature and mediate four major cardiovascular reflexes: the baroreceptor reflex, the hypoxic ventilatory response, the Bezold–Jarisch reflex and the Bainbridge reflex1,4,5,6. The baroreceptor reflex detects momentary changes in arterial blood pressure, providing feedback to stabilize cardiovascular output in real time2,9. Baroreceptor terminals are strategically located in the great arteries, at the carotid sinus and aortic arch, and detect stretch of the blood vessel wall with every heartbeat. Knockout of both Piezo1 and Piezo2 in baroreceptor neurons, but not either one alone, eliminates the baroreceptor reflex2. The hypoxic ventilatory response is mediated by arterial chemoreceptors located in the carotid body and aortic arch, which detect low oxygen levels through tissue-resident glomus cells, and trigger a neural arc that increases respiration10. Other receptors in the heart mediate the Bainbridge and Bezold–Jarisch reflexes. The Bezold–Jarisch reflex is a defensive reflex that may be evoked by cytokines, injury-associated chemicals and/or abnormal ventricular contraction, leading to bradycardia and hypotension11. The Bainbridge reflex is a reported mechanical reflex whereby rapid infusion of saline evokes a reflexive heart rate increase through vagal fibres in heart atria12. However, the Bainbridge reflex is weak or non-apparent in some species, including humans13,14, so the physiological roles of cardiac mechanoreceptors have remained obscure.
Recent single-cell RNA-sequencing studies have enabled genetic access to a variety of vagal and glossopharyngeal sensory neuron types15,16. For example, different genetically defined sensory neurons in the respiratory system detect airway stretch17, airway closure18, irritants that cause cough19, and pathogen- and inflammation-induced cytokines20. Other sensory neurons in the digestive system detect nutrients, osmolarity changes, toxins, cytokines, and stretch of the stomach or intestine15,21,22,23. Expression atlases and genetic approaches have also revealed orphan neuron types whose sensory properties and functions are not understood9,16. Neuronal responses to blood volume changes have been difficult to parse because the cardiovascular system is a closed loop and volume changes simultaneously impact sensors at different locations. Here we used genetic tools for selective loss of function to distinguish the roles of different vagal mechanoreceptors in the cardiovascular system. We first focused on sensation of mechanical signals during posture change, which can cause widespread effects on blood volume and blood pressure throughout circulation.
Neuronal compensation to posture change
When we stand up, gravity exerts powerful effects on the cardiovascular system, reducing venous return to the heart as well as blood flow to the head and upper body24. A prolonged reduction in carotid blood pressure upon standing up (called orthostatic hypotension) can cause dizziness and fainting. Several sensory pathways have been proposed to help compensate for the effects of gravity on the cardiovascular system during posture change25,26,27, but their relative importance is unclear.
Orthostatic hypotension is assessed clinically using a tilt-table test28, in which blood pressure and heart rate are measured while patients are rotated from a horizontal to an upright position. Here we adapted the tilt-table test for mice to assess posture-dependent blood pressure changes after genetic manipulation of different sensory pathways. Anaesthetized mice were placed securely onto a platform that allowed for 180 degrees of rotation from supine to upright to prone position. During rotation, arterial blood pressure (carotid and femoral) and heart rate were continuously monitored. Rotation to an upright position caused an immediate drop in arterial blood pressure through gravity that was rapidly corrected for and accompanied by a sustained heart rate increase (Fig. 1a,b and Extended Data Fig. 1a). Conversely, rotation to a supine or prone position caused an increase in arterial blood pressure that was also rapidly corrected for and accompanied by a sustained heart rate decrease. The compensation setpoint was primarily determined by the original carotid blood pressure, as overcompensation of femoral blood pressure was observed during recovery (Extended Data Fig. 1b). Aligning the systemic setpoint with carotid blood pressure presumably prioritizes the constancy of blood flow to the brain. Together, these data indicate that mice, like humans on a tilt table24, have a robust feedback control mechanism that compensates for the effects of gravity on the cardiovascular system.

a, Representative traces of blood pressure (mean carotid) and heart rate while mice are rotated through different postures on a tilt table. bpm, beats per minute. b, The initial and recovered changes in blood pressure after tilt to the indicated position. Initial change, maximal deviation within first 5 s; recovery BP, the average blood pressure from 1 min after tilt to 1 min and 5 s after tilt; baseline, the average blood pressure for the 5 s before tilt. The individual circles show the average response of one mouse over at least three trials. n = 7 mice. c, Cartoons depicting the anatomy of the vestibular system and vagus nerve. ADN, aortic depressor nerve; CSN, carotid sinus nerve. d, Representative traces of blood pressure (mean carotid) while mice are rotated through different postures on the tilt table. e, Representative blood pressure responses (average across at least three tilts) during upright tilt in the indicated mice. Baroreceptors cut, transection of the glossopharyngeal nerve and SLN. The control mice are littermates lacking Phox2b-cre. f, Quantification of blood pressure recovery after upright rotation. BP recovery % = (ΔI − ΔR)/ΔI, where ΔI is the initial blood pressure change from the baseline and ΔR is the recovery blood pressure change from the baseline. Data are mean ± s.e.m. From left to right, n = 7, 5, 5, 4, 4, 4, 5, 6 and 11 mice. KO, knockout; Subdiaph. vagotomy, subdiaphragmatic vagotomy. The individual circles show the average response of one mouse over at least three trials. Statistical analysis was performed using one-way ANOVA with Bonferroni correction for multiple comparisons, compared with the WT; ****P < 0.0001. Mouse diagrams in a created in BioRender. Liu, Z. (2025) https://BioRender.com/y44s465. Mouse diagram in c created in BioRender. Liu, Z. (2025) https://BioRender.com/z28w571. Heart diagram in c created in BioRender. Liu, Z. (2025) https://BioRender.com/a34i357.
We next used various surgical and genetic manipulations to define sensory pathways for gravity compensation (Fig. 1c–f and Extended Data Fig. 1c). We first examined a candidate role for the vestibular system in the inner ear, which has an important role in maintaining balance and stabilizing the visual field during motion and position changes. However, mutant mice that lack vestibular sensation (through Tmie29 or Otop130 knockout) displayed normal haemodynamic responses on the tilt table. We next performed surgical nerve transections to examine the roles of different peripheral nerves. Complete cervical transection of both vagal and glossopharyngeal nerves proximal to the ganglia (cervical vagotomy), which eliminates all sensory and motor fibres, abolished compensation to posture change, resulting in sustained hypotension after upright rotation. Vagus nerve transection below the diaphragm (subdiaphragmatic vagotomy) had no effect, while partial responses were observed after transection of (1) both the glossopharyngeal nerve and superior laryngeal nerve (SLN), which eliminates arterial baroreceptors, or (2) the vagus nerve trunk below the SLN departure point (vagal trunk cut), which preserves arterial baroreceptors but eliminates fibres to the heart. The partial effect observed following baroreceptor transection suggested a second residual sensory pathway important for gravity compensation.
PIEZO ion channels and posture change
PIEZOs are mechanosensory ion channels that directly sense force, mediate our sense of gentle touch31, and contribute to internal organ sensations such as airway stretch17, airway closure18, bladder fullness32 and the baroreceptor reflex2,9,33. Global knockout of Piezo2 is lethal17, but targeted knockout of Piezo2 in PHOX2B cells (Phox2b-cre;loxP-Piezo2, hereafter Vagal-ΔPiezo2), which includes petrosal and nodose ganglia, is tolerated and mice can survive to adulthood. We note that Phox2b-cre does not drive detectable reporter expression in intrinsic cardiac neurons, dorsal root ganglia or other intrinsic cells of the heart, while reporter expression was observed in stellate ganglia and brainstem neurons that do not express PIEZO217,34 (Extended Data Fig. 2). These findings are consistent with previous work indicating that the intersection of Piezo2 expression and Phox2b-cre-based reporters is largely or exclusively confined to placode-derived cranial sensory neurons2,17,35,36.
Phox2b-cre-driven knockout of Piezo2 eliminates the vagal sensation of airway stretch17 but not the baroreceptor reflex2, which instead is lost only after knockout of both Piezo1 and Piezo2 (Phox2b-cre;loxP-Piezo1;loxP-Piezo2; hereafter Vagal-ΔPiezo1/2). Here we confirmed that the baroreceptor reflex is normal in Vagal-ΔPiezo2 mice across a wide range of stimulus conditions (Extended Data Fig. 3). We next analysed both Vagal-ΔPiezo2 and Vagal-ΔPiezo1/2 mice using the tilt-table test. Notably, we observed a significant impairment in gravity compensation after knockout of Piezo2 alone (Fig. 1d–f), even though these mice have a normal baroreceptor reflex, as additionally evidenced by quantitative analysis of baroreflex sensitivity (Δheart rate/Δblood pressure or ΔHR/ΔBP) on the tilt table (Extended Data Fig. 1c). Knockout of both Piezo1 and Piezo2 also caused a response characteristic of orthostatic hypotension. Tilt-table responses were normal in mice lacking another candidate mechanoreceptor, GPR6837. Together, these findings indicate a collaborative role for at least two neuron types in gravity compensation: the baroreceptors and a separate neuron type dependent only on PIEZO2. Moreover, nerve transection experiments suggested that the residual PIEZO2-dependent pathway resides in the vagus nerve trunk below the SLN departure point, consistent with a role for sensory neurons that innervate the heart.
PIEZO2 neurons in the heart
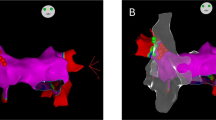
We next examined whether vagal PIEZO2 neurons project to the heart. To map the anatomical projections of Cre-defined vagal sensory neurons, we injected vagal ganglia of cre knock-in mice with an adeno-associated virus (AAV) containing a Cre-dependent tdTomato reporter (AAV-flex-tdTomato)9,38,39. Initial experiments involved Vglut2-ires-cre mice to label all vagal sensory neurons, followed by whole-mount light-sheet imaging of the entire heart (Fig. 2a). We observed extensive innervation across all four cardiac compartments (left and right atria and ventricles), as well as dense innervation of the nearby aortic arch and carotid sinus. Major vagal nerve branches approach and innervate the dorsal side of the heart, with finer nerve fibres ramifying across the entire cardiac surface toward the ventral side. Injection of different reporters in the left and right vagal ganglia showed no obvious difference in heart innervation (Extended Data Fig. 4), although the left and right vagal ganglia accessed different arterial sites with a similar repertoire of terminal types9.

a, Representative whole-mount images of tdTomato immunofluorescence in the heart (left, dorsal view; right, ventral view) of a Vglut2-ires-cre mouse injected with AAV-flex-tdTomato in the vagal ganglia. Scale bar, 1 mm. LA, left atrium; RA, right atrium. b, Representative confocal images (maximum-intensity projection, two replicates) of a heart from a showing flower-spray terminals (top) and end-net endings (bottom). Scale bars, 200 μm. c, Uniform manifold approximation and projection (UMAP) plots depicting expression (natural log scale) of Piezo2 (top) and Npy2r (bottom) across a previously published vagal/glossopharyngeal cell atlas16. d, Representative confocal images (maximum-intensity projection) of a heart from a Piezo2-ires-cre mouse (top, from eight replicates) or Npy2r-ires-cre mouse (bottom, from six replicates) injected with AAV-flex-tdTomato (magenta) and a Cre-independent AAV-eGFP (green) in the vagal ganglia. Scale bars, 200 μm. e, Quantification of the relative distribution of terminal types observed in each Cre line. Data are mean ± s.e.m. n = 6 (NPY2R) and 9 (PIEZO2) mice. Each dot represents cumulative data from one mouse involving both intact atria and a 1 mm ventricle section. f, Piezo2-ires-cre and Npy2r-ires-cre mice were injected bilaterally in the vagal ganglia with DT (vagalABLATE) or PBS (control) and the BP recovery was quantified after upright rotation across conditions. Data are mean ± s.e.m. The individual circles show the average response of one mouse over at least three trials. From left to right, n = 8, 4, 5 and 6 mice. Statistical analysis was performed using a two-sided Mann–Whitney U-test; **P = 0.004.
We observed two morphologically distinct types of vagal terminals within the heart: large arrays of interconnected end-net endings and complex arborizations called flower sprays, consistent with previous reports39,40,41 (Fig. 2b). It has been speculated that these endings may have different sensory functions, but the lack of selective genetic tools has hindered investigation.
Anatomical mapping experiments were similarly performed using Cre lines that mark smaller groups of vagal sensory neurons. We used Piezo2-ires-cre and Npy2r-ires-cre mice, which mark predominantly discrete populations of sensory neurons according to vagal cell atlases16,38 (Fig. 2c). PIEZO2 neurons densely innervated the heart, and exclusively formed end-net endings; PIEZO2-containing flower-spray terminals were not readily observed (Fig. 2d,e). In the atrium, PIEZO2 terminals were enriched near the junction with the vena cava (Extended Data Fig. 5). Vagal NPY2R neurons represent a substantial fraction of vagal sensory neurons16, and were previously shown to form a variety of terminals throughout the body, including free endings in the lung38 and intraganglionic laminar endings in the stomach and intestinal wall23. NPY2R neurons evoke rapid and shallow breathing, and also elicit cardiovascular responses underlying the Bezold–Jarisch reflex11,38. Here we observed that NPY2R neurons mark a large cohort of heart-innervating sensory neurons, including separate neurons that form end-net endings and flower sprays (Fig. 2d,e); we note that a previous report described some NPY2R terminals as varicose surface endings or ventricular intramuscular arrays39, and we have summarized them both as end-net endings due to structural differences between atrial and ventricular muscles. NPY2R-containing end-net terminals were 4.0-fold more abundant than end-net endings containing PIEZO2, and were more distributed across the heart atria and ventricles (Extended Data Fig. 5). These findings suggest that there are probably at least three types of vagal neurons in the heart: NPY2R-containing flower sprays, NPY2R-containing end-net endings and PIEZO2-containing end-net endings.
Next, we examined which terminal type might contribute to cardiovascular compensation during the tilt-table test. We ablated vagal PIEZO2 and NPY2R neurons using a previously established approach involving diphtheria toxin (DT)9,20. In brief, the DT receptor (DTR) was expressed in PIEZO2-expressing cells (Piezo2-ires-cre;lsl-DTR) or NPY2R-expressing cells (Npy2r-ires-cre;lsl-DTR), and vagal ganglia were then injected bilaterally with DT to achieve efficient and selective neuronal ablation; the resulting mice are termed PIEZO2-vagalABLATE and NPY2R-vagalABLATE mice. Note that the ablation of PIEZO2 neurons also eliminates baroreceptors, as reported previously9, presumably because PIEZO1 and PIEZO2 are co-expressed in baroreceptor neurons. Ablation of vagal PIEZO2 neurons reduced neuronal compensation during posture change, while ablation of NPY2R neurons had no effect (Fig. 2f and Extended Data Fig. 6). The different phenotypes of NPY2R-vagalABLATE and PIEZO2-vagalABLATE mice suggest that end-net endings marked by PIEZO2 and NPY2R are functionally different, with only PIEZO2 endings required for normal posture compensation.
Heartbeat-coupled vagal responses
We investigated the response properties of vagal PIEZO2 fibres in the heart to understand how their activity patterns might vary with posture. Classical studies have reported that some myelinated vagal sensory neurons fire at particular phases of the cardiac cycle42,43,44; we therefore performed electrophysiological recordings of the mouse vagus nerve while simultaneously recording cardiac activity by electrocardiogram. In some animals, we additionally measured right atrial and left ventricular pressure as well as left ventricular volume through sensors introduced by a cardiac catheter. We excluded contributions from arterial baroreceptors, which display heartbeat-coupled responses with each arterial pressure pulse42, by recording from the sensory end of the vagus nerve trunk below the SLN departure point (Fig. 3a). We also excluded contributions from airway stretch receptors by subtraction of breathing-coupled responses (Methods).

a, Cartoon of electrophysiological recordings of the thoracic vagus nerve trunk. Heart diagram created in BioRender. Liu, Z. (2025) https://BioRender.com/a34i357. Scissors diagram created in BioRender. Liu, Z. (2025) https://BioRender.com/s08uo8h. b, Representative, simultaneously recorded electrocardiograms (ECG) and vagal activity from WT (top) and vagal-ΔPiezo2 (bottom) mice at the baseline (left, raw activity) and after intravenous injection (black arrow) of serotonin (right, integrated activity over a 5 s window). c, Representative spike raster of vagal activity (the black dashes show action potentials) across 159 cardiac cycles in a WT mouse. d, The average physiological measurements over 30 s (around 250 cardiac cycles) in four WT mice. RAP, right atrial pressure; LVP, left ventricular pressure; LVV, left ventricular volume. e, Representative spike histograms of average vagal activity patterns (30 s). f, Quantification of phase I (left) and phase II (right) responses from e. Data are mean ± s.e.m. The individual circles show the average response of one mouse over at least 100 heartbeats. From left to right, n = 12, 6, 6, 7, 6 and 5 mice. g, Vagal nerve responses recorded in WT mice during slow withdrawal of blood (500 μl over 3 min). Right, representative responses (averaged from 10 s) after depletion of the volumes indicated, or reinfusion to the baseline volume (the x axis shows the timeline normalized to cardiac cycle; Methods). Left, quantitative analysis of average phase I (red) and phase II (blue) responses across a range of depletion volumes. Data are mean (dark lines) ± s.e.m. (shading). n = 4. Mouse diagram created in BioRender. Liu, Z. (2025) https://BioRender.com/k0bf0ej. h, Vagal nerve spike counts (left) over 10 s after the volume change indicated, normalized to the serotonin response. Data are mean ± s.e.m. n = 5, 5 and 3 (blood withdrawal); and 4, 3 and 3 (saline infusion). The slope of vagus nerve activity to changing blood volume normalized to body weight (right). Data are mean ± s.e.m. n = 12, 6, 9, 6, 6 and 7 (blood withdrawal); 9, 5, 6, 4, 5 and 7 (saline infusion). For f and h, statistical analysis was performed using one-way ANOVA with Bonferroni correction for multiple comparisons, compared with the WT; from left to right, *P = 0.01, ***P = 0.0007, **P = 0.0015, **P = 0.0044, **P = 0.0029 and **P = 0.005 (f), and ****P < 0.0001, ***P = 0.0006, ***P = 0.0002, **P = 0.0026, *P = 0.0104 and **P = 0.0014 (h).
In wild-type (WT) mice, we observed that the vagus nerve trunk fired with every heartbeat at two specific phases of the cardiac cycle, just after the P wave and after the QRS complex in the electrocardiogram (Fig. 3b–f). The first peak (phase I) was synchronous with atrial systole, matching Paintal type A atrial receptors43,45, while the second peak (phase II) was synchronous with ventricular systole44. We did not observe prominent activity during the V wave of atrial pressure, which occurs during atrial filling and would have corresponded to Paintal type B fibres5,43.
We next examined whether and how PIEZO2 neurons might contribute to heartbeat-coupled vagal responses by measuring vagal responses across the cardiac cycle after targeted neuron ablation. Phase I and phase II responses were intact in NPY2R-vagalABLATE mice, but were lost in PIEZO2-vagalABLATE mice (Fig. 3e,f). Paired with anatomical data in Fig. 2, these findings demonstrate that vagal mechanoreceptors responsible for physiological responses during the cardiac cycle form end-net terminals and not flower sprays.
PIEZO2 marks about a third of vagal sensory neurons38, including different cell types that express P2ry1, Pvalb, Oxtr or Glp1r. We ablated subsets of vagal PIEZO2 neurons marked in P2ry1-ires-cre, Pvalb-t2a-cre, Oxtr-t2a-cre and Glp1r-ires-cre mice using genetic ablation approaches involving DT, but heartbeat-coupled responses remained partly (P2RY1) or completely (PVALB, OXTR, GLP1R) intact (Extended Data Fig. 7). These studies provide exclusionary data that help to refine which transcriptome-defined PIEZO2 neurons fire across the cardiac cycle.
To examine a role for PIEZO proteins themselves, we analysed heartbeat-coupled vagal responses in Vagal-ΔPiezo1 (Phox2b-cre;loxP-Piezo1), Vagal-ΔPiezo2 and Vagal-ΔPiezo1/2 mice (Fig. 3b–f). Heartbeat-coupled vagal trunk responses were normal after deletion of Piezo1 alone, but were lost after deletion of Piezo2 or Piezo2 together with Piezo1. These findings indicate a key difference between mechanoreceptors activated during cardiac contractions, which require only PIEZO2, and arterial baroreceptors, which require either PIEZO1 or PIEZO22.
PIEZO2 neurons measure blood volume
Baroreceptors fire with every heartbeat42, and the intensity of activity informs about changing blood pressure46. Given the key role for vagal PIEZO2 neurons in posture responses, we reasoned that the intensity of cardiac mechanoreceptor activity across the cardiac cycle might vary with posture. Electrophysiological recordings on the tilt table were not technically achievable; we therefore measured how key cardiovascular parameters changed with posture to examine how such parameters may influence phase I and phase II nerve responses.
We obtained a pressure–volume (PV) loop of WT mice on the tilt table. Rotation to an upright position caused a transient decrease in systolic pressure in the left ventricle that returned to the baseline, similar to changes in arterial pressure (Extended Data Fig. 8a). However, the stroke volume of the left ventricle was reduced to 70% and did not recover, similar to human clinical data24 and consistent with a sustained decrease in venous return due to gravitational pull. These findings raised the possibility that central blood volume might be a key variable that influences the firing of cardiac mechanoreceptors.
To test this idea, we measured vagal trunk responses during the cardiac cycle while changing circulating blood volume by withdrawing blood or adding saline across a broad physiological range (Fig. 3g). Integrated vagal nerve activity decreased as blood was withdrawn and increased as saline was introduced, and the magnitude of the nerve response varied with the extent of blood volume change. Smaller volumes of blood withdrawal impacted phase I nerve responses more substantially than phase II nerve responses, suggesting differential tuning of atrial and ventricular mechanoreceptors to blood loss. We note that, in some species, increasing blood volume evokes the Bainbridge reflex13, but we did not observe a heart rate increase after saline infusion (Extended Data Fig. 8b). Knockout of Piezo2 or ablation of PIEZO2 neurons caused a striking reduction in heartbeat-coupled responses, and this low activity level was not changed further by volume manipulations (Fig. 3h). Knockout of Piezo1 alone or ablation of NPY2R had no effect on the volume-dependent modulation of heartbeat-associated vagal responses. These findings indicate that the magnitude of PIEZO2 neuron activity during atrial and ventricular systole provides information on circulating blood volume.
We used vagal ganglion calcium imaging to understand the cellular relationship between blood volume sensors and other PIEZO2 neurons in the lung that respond to airway stretch. Real-time calcium transients were recorded after airway distension or intravenous saline infusion in individual vagal sensory neurons of Vglut2-cre;lsl-SALSA mice, which express a GCaMP6f–tdTomato fusion protein in all vagal sensory neurons, or Snap25-GCamp6s;Piezo2-ires-cre;lsl-tdTomato mice in which PIEZO2+ and PIEZO2− neurons can be imaged in parallel (Fig. 4a). We note that calcium imaging does not provide sufficient temporal resolution to distinguish the timing of responses across the cardiac cycle, but does resolve the responses of single cells. Small groups of vagal neurons responded (Fig. 4b,c) to either airway stretch (92 out of 1,842 neurons, 5.0%) or venous saline infusion (116 out of 1,842 neurons, 6.3%), and these populations were largely non-overlapping (10 out of 1,842 neurons (0.5%) responded to both). The majority of neurons responsive to each stimulus expressed PIEZO2 (Fig. 4d and Extended Data Fig. 9; airway stretch: 28 out of 37; venous saline infusion: 21 out of 28). Previous work showed that some PIEZO2− neurons receive mechanosensory signals from neuroepithelial bodies; these neurons are not relevant for the Hering–Breuer reflex or breathing-coupled responses, mediate responses to airway closure and display high-threshold and rapidly adapting responses to large distensions of the conducting airways18. In electrophysiological experiments, PIEZO2− neurons do not respond with every heartbeat, so the responses observed by calcium imaging in PIEZO2 negative neurons may represent another sensory pathway or be due to a secondary physiological change. Taken together, these findings indicate that separate cohorts of PIEZO2 neurons mediate the major responses to airway stretch and blood volume infusion.

a, Cartoon depicting vagal ganglia imaging (left) and a two-photon image (right) of SALSA fluorescence in a representative vagal ganglion (of six replicates) from Vglut2-cre;lsl-SALSA mice. Scale bar, 50 µm. Heart image created in BioRender. Liu, Z. (2025) https://BioRender.com/a34i357. Microscope objective image created in BioRender. Liu, Z. (2025) https://BioRender.com/quy3reu. b, Heat map (left) and the distribution (right) of calcium responses from vagal neurons from Vglut2-cre;lsl-SALSA mice (ΔF/F colour coded, 1,382 imaged neurons, 6 mice) to blood volume infusion (red), airway stretch (black) or both (purple). In total, 140 responsive and some randomly selected non-responsive (grey) neurons are shown. c, Representative calcium activity traces from individual vagal neurons (right) responding to changes in blood volume (B, red) or airway stretch (A, black), and a representative field of view (left) showing the average GCaMP6f fluorescence intensity during peak stimulus application. Scale bars, 20 µm. Representatives were chosen from 1,382 neurons, 6 mice. d, The neuronal responses in PIEZO2+ and PIEZO2− neurons in Snap25-GCamp6s;Piezo2-ires-cre;lsl-tdTomato mice. n = 163 (PIEZO2+) and 297 (PIEZO2−) neurons, 4 mice.
PIEZO2 neurons evoke hypotension
In previous studies, optogenetic activation of all vagal PIEZO2 neurons caused a robust decrease in heart rate and blood pressure characteristic of the baroreceptor reflex. However, little or no effect was observed after optogenetic activation of PIEZO2 neurons in the vagus nerve trunk below the SLN2, which included vagal fibres to the heart. We revisited these studies by varying optogenetic stimulus conditions in mice (Piezo2-ires-cre;lsl-ChR2) expressing channelrhodopsin (ChR2) in PIEZO2 neurons. We observed no effect of vagal nerve illumination at frequencies between 1 and 5 Hz, but did observe a significant drop in blood pressure and heart rate at illumination frequencies between 10 and 50 Hz (Extended Data Fig. 10). This frequency range matches the natural heart rhythm, so we also used a closed-loop optogenetic stimulation paradigm in which illumination was time-locked to each P and QRS peak of the cardiac cycle, and observed a similar reduction in blood pressure (Extended Data Fig. 10). The effect magnitude was smaller than that observed after optogenetic stimulation of baroreceptors, but was comparable to physiological changes observed during the tilt-table test. We note that optogenetic stimulation of PIEZO2 neurons in the distal vagus nerve trunk caused a mild bradycardia, not a tachycardia, which would have been expected for the Bainbridge reflex.
Vagal reflex compensation for blood loss
In addition to posture changes, other physiological challenges also alter blood volume. Acute trauma and injury can cause massive blood loss, and subsequent unloading of blood volume receptors. To examine whether vagal volume receptors trigger physiological responses that compensate for blood loss, we developed a model involving tail-bleeding-induced haemorrhage. Mice were anaesthetized and treated with heparin to block clotting, and the tail was transected. Within the first 30 min of haemorrhage, WT mice lost 20–25% of their blood volume on average (Extended Data Fig. 8c). During this time, blood pressure was sustained, presumably through increased vascular resistance and heart rate was increased, which would help to preserve cardiac output with a lower circulating blood volume; the survival rate was 58% (11 out of 19 mice) at 2 h and 0% at 4 h (Fig. 5). Vagal-ΔPiezo2 mice lost blood at a similar rate (Extended Data Fig. 8c) but lacked appropriate physiological compensation (Fig. 5), as they were unable to maintain blood pressure or a similarly elevated heart rate and died more rapidly. Similarly, acute blood withdrawal from the jugular vein caused a rapid blood pressure drop which was corrected for in WT mice but not Piezo2-knockout mice (Extended Data Fig. 8d). These findings reveal a protective role for vagal volume receptors during traumatic haemorrhage.

a, Analysis of heart rate (HR) and blood pressure (BP) over time after tail transection in the indicated genotypes. Data are mean (dark lines) ± s.e.m. (shading). n = 17 (Vagal-ΔPiezo2) and 19 (control, Cre-negative littermates) mice (top), and n = 5 (Vagal-ΔPiezo2) and 6 (control, age- and sex-matched WT) mice. Mouse diagram created in BioRender. Liu, Z. (2025) https://BioRender.com/89tllig. b, The average heart rate and blood pressure change between minutes 25 and 35 after haemorrhage onset from the mice in a. Data are mean ± s.e.m. Statistical analysis was performed using two-sided Mann–Whitney U-tests; **P = 0.0043, ****P < 0.0001. c, The survival rate over time of mice after tail-transection-induced haemorrhage. n = 19 (control, including 14 Cre-negative littermates and 5 age- and sex-matched WT) and 20 (Vagal-ΔPIEZO2) mice. Statistical analysis was performed using the log-rank (Mantel–Cox) test; *P = 0.0173.
Discussion
The functions of cardiac mechanoreceptors have remained obscure, with blood volume changes proposed to elicit the Bainbridge reflex through vagal afferents12. However, we did not observe a vagally mediated tachycardia response in mice to volume infusion or optogenetic stimulation of thoracic PIEZO2 neurons that would be characteristic of a Bainbridge reflex. Instead, using genetic tools, we report that thoracic PIEZO2 neurons evoke a reflex that tunes vascular resistance and heart rate in accordance with central blood volume. Loss of this reflex causes orthostatic hypotension and a compromised ability to sustain tissue perfusion after traumatic blood loss.
Effective neural control of circulation is achieved through an intricate interplay between classes of mechanoreceptors located at different strategic hotspots in the cardiovascular system. The brain receives collaborative information from at least three classes of mechanoreceptors that fire at different stages of the cardiac cycle: atrial systole (cardiac mechanoreceptors phase I), ventricular systole (cardiac mechanoreceptors phase II) and the arterial pressure pulse (baroreceptors). Using these receptors, the nervous system can track blood flow through key central sites in the circulatory system.
Despite many similarities, there are important functional differences between blood volume receptors and arterial baroreceptors. While both neuron types fire with every heartbeat and, therefore, provide information about heart rate, their response intensities report on different haemodynamic features. Baroreceptor activity changes with blood pressure while cardiac mechanoreceptor activity changes with central blood volume. These features are often correlated, which, together with anatomical challenges that prevent selective denervation of cardiac sensory fibres, has hindered physiological analysis of the cardiac mechanoreceptors. Here we find that optogenetic stimulation of thoracic PIEZO2 neurons causes hypotension and mild bradycardia, while unloading them, as occurs during upright tilt and haemorrhage, evokes a compensatory drive to increase blood pressure and heart rate. Thus, like the baroreceptors, the blood volume receptors can, in principle, act bidirectionally, with loss-of-function approaches so far revealing a required role for these neurons during hypovolemic challenge. The complete absence of PIEZO2 and the blood volume reflex is not reflected in long-term setpoint dysfunction but, instead, in the loss of shorter-term volume-dependent modulation; in analogy, the major phenotype of baroreceptor ablation is acute, causing increased blood pressure variability (labile hypertension). Genetically guided anatomical mapping revealed that cardiac mechanoreceptors form end-net endings in the heart, not flower-spray terminals, and, similarly, arterial baroreceptors form end-net endings in the aorta9. However, the baroreceptors and blood volume receptors have a key genetic difference. Arterial baroreceptors and blood volume receptors can be genetically distinguished through selective Piezo2 knockout, as arterial baroreceptors but not volume receptors can use either PIEZO1 or PIEZO22. Knockout of Piezo2 alone eliminated heartbeat-synchronized responses in the thoracic vagus nerve trunk, and compromised physiological responses to decreased central blood volume associated with posture change and haemorrhage, even though the baroreceptors were intact. As baroreceptor denervation also accelerates the decompensatory phase of haemorrhage47 and causes orthostatic hypotension (Fig. 1), the baroreceptors and volume receptors closely collaborate to maintain cardiovascular homeostasis. In future studies, it will be interesting to examine contributions from volume receptors during hypervolemic challenges, and other aspects of fluid regulation, including thirst, urination and kidney function4,48.
On the basis of these and previous findings, the vagus and glossopharyngeal nerves contain at least six types of terminals in the cardiovascular system: (1) arterial baroreceptors that sense blood pressure; (2) arterial chemoreceptors that mediate the hypoxic ventilatory response; (3) arterial flower sprays of unknown function; (4) blood volume receptors that mediate the reflex described here; (5) cardiac end-net endings marked in Npy2r-ires-cre mice of unknown function; and (6) cardiac flower sprays marked in Npy2r-ires-cre mice of unknown function. PIEZO2 neurons measure blood volume and respond with every heartbeat to atrial and ventricular contraction, and PIEZO2 neurons innervate the heart; a parsimonious interpretation is that these are the same neurons and heart-innervating neurons mediate the blood volume response. This interpretation is consistent with classical single-unit recordings showing that neurons responsive to particular phases of the cardiac cycle are also directly responsive to mechanical probing or stretching of heart tissue1,5,43. At least some NPY2R neurons mediate the Bezold–Jarisch reflex11, but there remain at least two orphan populations of vagal cardiovascular neurons, as well as heart-innervating spinal neurons, whose functions remain unclear.
Optogenetic stimulation of the Bezold–Jarisch reflex in mice induces a massive bradycardia and blood pressure drop, which is sufficient to cause fainting11. Here we find an alternative cause for low carotid blood pressure that involves dysfunction rather than gain-of-function within vagal afferents. Neurogenic orthostatic hypotension has been attributed to baroreceptor deficits, which we find can be one cause. Moreover, we find that inefficient gravity compensation after loss of PIEZO2-containing blood volume receptors also leads to orthostatic hypotension, a prominent cause of dizziness, fainting and injury upon standing or rising from bedrest in susceptible patients.
Methods
Animals
All animal procedures followed ethical guidelines outlined in the NIH Guide for the Care and Use of Laboratory Animals, and all procedures were approved by the Institutional Animal Care and Use Committee at Harvard Medical School. Mice were maintained under constant environmental conditions (23 ± 1 °C, 46 ± 5% relative humidity) with food and water provided ad libitum under a 12 h–12 h light–dark cycle. All of the studies used adult male and female mice (aged 6–24 weeks) in comparable numbers from mixed genetic backgrounds. Tmie-, Gpr68- and Otop1-knockout mice were gifts from J. Holt, A. Patapoutian and E. Liman. All of the other mice were purchased from Jackson Laboratory, made in the laboratory and then deposited at Jackson Laboratory, or received as gifts and later deposited in the Jackson Laboratory: C57BL/6J (00664), Vglut2-ires-cre (16963), Npy2r-ires-cre (29285), Piezo2-ires-cre (27719), Phox2b-cre (16223), P2ry1-ires-cre (29284), Pvalb-t2a-cre (12358), Glp1r-ires-cre (29283), Oxtr-t2a-cre (31303), lsl-ChR2 (12569), lsl-DTR (07900), lsl-SALSA (31968), lsl-tdTomato (07914), loxP-Piezo2 (27720), loxP-Piezo1 (29213) and Snap25-GCamp6s (25111).
Physiological measurements
Arterial blood pressure was measured in anaesthetized mice (1.5–2% isoflurane in oxygen). The carotid artery or femoral artery was cannulated through a custom-built fluid catheter (Braintree Scientific RPT015, MRE033, MRE065) attached to a pressure transducer (BioPac, TSD104A; Sensor, RX104A) amplified by the Biopac DA100C system. Right atrial pressure was measured by inserting a catheter through the external jugular vein to access the atrium. Electrocardiograms were performed using needle electrodes placed subcutaneously on the right forepaw and left hindpaw, amplified using the Biopac ECG100C system. Breathing was measured using a pressure transducer (Harvard Apparatus, Differential Pressure Transducers MPX) within the isoflurane delivery device, amplified by the Biopac DA100C system. For some experiments, the jugular or femoral veins were cannulated for blood withdrawal or saline (0.9% NaCl) infusion manually or with a syringe pump (NE-1000, New Era Pump Systems). Data were acquired using the Biopac MP160 system with the Acknowledge software.
Tilt-table test
Anaesthetized mice (1.5–2% isoflurane in oxygen) were immobilized on a surgical platform with adhesive, and prepped for measurements of blood pressure, heart rate and breathing. The isoflurane concentration was then reduced to 1.2–1.5% until the breathing rate stabilized at around 60 breaths per minute. The blood pressure transducer was kept level with the catheter site to avoid a hydrostatic effect during rotation. The surgical platform with the mouse was magnetically secured to a tilt table, which was connected to an accelerometer for movement recording. The mouse was manually tilted to different positions, remaining in each position for at least 1 min while the physiological parameters were recorded (Biopac).
Haemorrhage model
Mice were anaesthetized (1.5–2% isoflurane in oxygen) and placed onto a heating pad to maintain the body temperature above 35°C. Heparin (200 U kg−1 in PBS) was administered through the right external jugular vein or tail vein and isoflurane was lowered (1.2–1.5%) until the breathing rate stabilized at around 60 breaths per minute. After 10 min, the tail was transected (2 cm from the tip) with a scalpel to induce bleeding. Blood was collected in an Eppendorf tube and weighed at 30 min and at the survival end point. Survival was continuously assessed by detectable breathing. Animals of different genotypes were used in a random order to which the experimenter was blinded for analyses of survival and heart rate.
Neuron ablation
Vagal sensory neurons were ablated as previously described by serial injection (10–20 injections of 10 nl) of DT (Sigma-Aldrich, D0564) solution (5–20 μg ml−1 DT, 0.05% Fast Green FCF Dye with PBS) into surgically exposed nodose/jugular/petrosal (NJP) superganglia with a Nanoject III injector (Drummond). Control mice were injected with PBS lacking DT. Mice were allowed to recover for at least 3 weeks after injection, and nodose ganglia were collected and immunostained for DTR after experiments to determine the extent of ablation.
AAV injection
The AAVs AAV-flex-tdTomato (Addgene, 28306-AAV9), AAV-eGFP (Addgene, 105542-AAV9) and AAV-flex-eGFP (Addgene, 51502-AAV9) were purchased. For the experiments in Fig. 2a,b and Extended Data Figs. 4 and 5, surgically exposed NJP superganglia were serially injected (20 injections of 10 nl) with AAV-flex-tdTomato (AAV titre > 1 × 1013 vg per ml, 0.05% Fast Green FCF Dye, Sigma-Aldrich). For Fig. 2d, NJP superganglia were injected (30 injections of 10 nl) with a 2:1 injection solution of AAV-flex-tdTomato (AAV titre > 1 × 1013 vg per ml and 0.05% Fast Green FCF Dye, Sigma-Aldrich) and AAV-eGFP (AAV titre > 1 × 1013 vg per ml and 0.05% Fast Green FCF Dye, Sigma-Aldrich). For Extended Data Fig. 4, the left NJP superganglion was injected with AAV-flex-eGFP (AAV titre > 1 × 1013 vg per ml, 0.05% Fast Green FCF Dye, Sigma-Aldrich) and the right NJP superganglion was injected with AAV-flex-tdTomato (AAV titre > 1 × 1013 vg per ml, 0.05% Fast Green FCF Dye, Sigma-Aldrich). All injections were performed using the Nanoject III injector (Drummond).
Whole-tissue clearing and immunostaining
Mice were anaesthetized (avertin, 1 ml, 12.5 mg ml−1) and perfused with PBS (20 ml) and paraformaldehyde (10 ml, 4%, PBS) administered through the left ventricle. The heart and attached vasculature were removed by dissection, fixed (4% PFA, PBS, overnight, 4 °C) and washed twice in PBS with 0.05% NaN3 (2 h at room temperature). For Fig. 2a, whole-heart clearing with Adipo-Clear was performed as previously described with modifications49. In brief, refractive index matching was conducted using ethyl cinnamate (Sigma-Aldrich 112372). After clearing, the samples were degassed in a vacuum desiccator for several hours to remove bubbles trapped in the heart chambers. The samples were imaged using light-sheet microscopy (UltraMicroscope II by LaVison, ImSpector v.7.1.4). For Fig. 2b,d and Extended Data Figs. 4 and 5, thick section clearing was performed on intact left atria, intact right atria, intact aorta and thick ventricle slices (1 mm, Zivic Instruments, Mouse Heart Slicer Matrix, HSMA001-1). Thick tissue samples were cleared using the CUBIC protocol as previously described50,51. Tissues were incubated (2 h, 37 °C) in blocking solution (2% normal donkey serum (Jackson ImmunoResearch, 017-000-121), 0.1% Triton X-100 (Sigma-Aldrich, X100), 0.1% Tween-20 (Sigma-Aldrich, P1379) in PBS). All heart and ganglion samples were incubated with primary antibody in blocking solution (1:1,000 rabbit anti-RFP, Rockland, 600-401-379; 1:1,000 chicken anti-GFP, Aves Labs, GFP-1020; 1:1,000 chicken anti-PGP9.5, Novus Biologicals, NB110-58872; 5 μg ml−1 goat anti-HB-EGF (human), R&D Systems, AF-259-NA), and secondary antibody in blocking solution (1:500 donkey anti-rabbit Cy3, Jackson ImmunoResearch, 711-165-152; 1:500 donkey anti-chicken 647, Jackson ImmunoResearch, 703-605-155; 1:500 donkey anti-chicken 488, Jackson ImmunoResearch, 703-545-155; 1:500 anti-goat 647, Jackson ImmunoResearch, 705-605-147) for 3 days at 37 °C. Stained samples were imaged by confocal microscopy (Nikon Ti2).
Whole-nerve electrophysiology
Whole-vagus-nerve electrophysiology recording was performed in anaesthetized mice (1.5–2% isoflurane in oxygen) as previously described with modifications2,18,38. In brief, the left vagus nerve was exposed and then transected below the SLN branching point. The nerve stump proximal to the heart was desheathed and placed onto a bipolar electrode (platinum–iridium). A ground electrode was placed on nearby muscle, and the nerve was immersed in halocarbon oil. The nerve activity was amplified (CP511, Grass Technologies), digitized (MP160, Biopac) and recorded (AcqKnowledge software, Biopac). Serotonin (1 mM, 50 µl, saline) was infused (intravenously) at the end of every experiment. Stimulus-induced responses were calculated as the percentage change from the baseline activity and normalized to the serotonin response. For serotonin responses (Fig. 3b) and nerve responses after blood withdrawal (Fig. 3g), nerve activity was integrated over a moving window (serotonin: 5 s, Fig. 3g: 5 ms) using the root-mean-squared method.
PV loop measurement
Left ventricular pressure and volume were measured using a Millar PV catheter (SPR-839) inserted into the carotid artery and advanced into the left ventricle. Data were acquired on the Millar MPVS-300 system with the LabChart software. After the measurements, volume calibration was performed with injection of hypertonic saline into the jugular vein and dip-well cuvettes. Analysis was performed with PV loop module in LabChart.
Optogenetics
Optogenetics experiments were performed as described with minor modifications16,18,38. The vagus nerve trunk was exposed near the carotid bifurcation, and isolated from the carotid artery and jugular vein. The nerve was transected below the SLN close to the heart above the thoracic wall, and the nerve stump proximal to the brain was illuminated to exclude motor efferent contribution (10 mW, 1 min, 10 ms pulse duration, frequencies indicated, controlled by a pulse train generator from Prizmatix). For ECG entrainment, real-time peak detection of the ECG signal (OpenEphys, crossing detector module) was coupled to optic fibre illumination at the P and QRS waves.
Two-photon calcium imaging
In vivo imaging of vagal ganglia was performed using an Olympus FVMPE resonant-scanning two-photon microscope equipped with a piezoelectric objective Z-stepper (P-915, Physik Instrumente) as previously described with minor modifications18,23. In brief, mice were anaesthetized with urethane (2 mg per g, intraperitoneal, at least 30 min before surgery) and tracheostomized to allow constant low-level air flow (40 ml min−1; 100% oxygen) delivered by a ventilator in freely breathing mice. The left vagal ganglion was surgically exposed with branches superior to the ganglion and trunk transected, and immobilized on an imaging platform attached to a manipulator. Airway stretch was achieved by increasing airflow through a ventilator (15–25 ml min−1 g−1 body weight, 5 s). For blood volume manipulation, intravenous saline was administered in the jugular vein (0.9% NaCl, 30% of total blood volume estimated by body weight or 24 µl saline infused per g body weight). Saline was administered slowly over 20 s, volume was held for 30 s and then an equal blood volume was withdrawn over 1 min. The number of healthy neurons imaged was defined by responses to stepwise electrical stimulation of the cervical vagus nerve trunk (2 ms pulses at 5 Hz over around 5 s; Grass Stimulator) of increasing current (stepwise from 0.1 mA to 5 mA). Two-channel images were processed, analysed and classified as previously described using Fiji ImageJ and Microsoft Excel18. Non-responsive neurons were selected for inclusion in heat maps based on computer randomization.
Data analysis
Haemodynamic quantification
Haemodynamic signals were analysed using custom scripts in MATLAB (MathWorks). The mean arterial blood pressure (BP) was computed from systolic (SBP) and diastolic (DBP) pressures as BP = (1/3 × SBP) + (2/3 × DBP). The heart rate (HR) was derived from beat-to-beat intervals, either from R–R intervals when ECG was available, or from the intervals between successive systolic peaks of the arterial pressure waveform when ECG was unavailable. BP and HR traces were then smoothed with a 3 s moving window, and sometimes downsampled and smoothed with a 30 s moving window for long recordings. For tilt-table experiments, each mouse underwent at least three prone-to-upright tilt trials, and each tilt onset was determined by the onboard accelerometer. The BP and HR were temporally aligned to tilt onset, and trials from multiple tilts were averaged. The baseline was the mean value during the 5 s preceding tilt. The initial BP response was defined as the maximum deviation within the first <5 s after tilt; the recovered response was the 5 s mean at 1 min after tilt. BP recovery (%) was calculated as 100 × (Δinitial BP − Δrecovered BP)/Δinitial BP, where Δ denotes the change from the baseline. For tail-bleeding experiments, BP and HR were quantified as the mean response after tail transection, expressed relative to the pretransection baseline.
Anatomical quantification
Nerve fibre innervation was quantified in confocal images (maximum intensity projection) of whole atria and ventricle slices. Nerve fibres were assigned by image segmentation using Ilastik (Ilastik, Pixel Classification) and smoothened (Otsu’s method). Nerve fibre skeletons were created using scikit-image (Python v.3.9), and nerve terminal locations were defined as branch endpoints of the skeletons. Data were curated to remove noise, including small objects (<1,500 µm2) and short branches (<17 µm). Terminal structures (defined within an 86 µm × 86 µm square centred around branch end points) were classified as end-net and flower-spray endings using a machine-learning program (Ilastik, Object Classification) after manual entrainment. A relative distribution of terminal types was calculated using a denominator of total terminals identified in a given mouse.
Nerve signal quantification
Whole-nerve electrophysiology recordings were analysed using custom-written MATLAB codes. Spikes were identified using a derivative method in which a time-shifted (250 µs) trace was subtracted from the original trace to identify acute changes in activity (events) of which the magnitude was over three times the s.d. of activity in the entire trace. Once events were identified, the difference between the minimum and maximum values in the original trace within 500 µs of the event was defined as event amplitude. An additional noise-exclusion threshold was applied to include only events of which the amplitude was over four times the s.d. of the activity in the original trace.
Removal of breathing-coupled responses in nerve recordings
The vagus nerve trunk responds both with every heartbeat and with every breath. To isolate heartbeat-coupled responses, breathing was measured using a pressure transducer within the isoflurane delivery device. The breathing trace was smoothened over a rolling 2 s window, peak inspiratory and expiratory events were identified, and inter-breath intervals (IBIs) calculated. The breathing window was defined to start 10% IBI before peak expiration and end 30% IBI after peak expiration, and all spike events within the breathing window were excluded from further analysis.
Temporal alignment to ECG recordings
To control for variations in cardiac cycle duration during nerve recordings and physiological measurements, the time axis of each cardiac cycle was normalized to the PR interval.
UMAP plots
UMAP plots were generated by analysis of published single-cell transcriptomic data of vagal sensory neurons16 using Seurat in R.
Statistics and reproducibility
Data in the graphs are presented as the mean ± s.e.m. unless otherwise indicated. Statistical analyses were performed using Prism (GraphPad), and statistical tests and sample sizes are reported in figures and legends. All replicates were biological and statistical tests were two-sided. Sample sizes were chosen based on previous studies of the vagus nerve23,38.
Materials availability
All reagents that are not commercially available will be made freely available on reasonable request.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Raw microscopy images and calcium imaging data are large files, and are available on request. Source data are provided with this paper.
Code availability
Custom-written codes used in analyses of haemodynamic responses, electrophysiological recordings and histology are posted at GitHub (https://github.com/zhikai-liu/posture_project).
Change history
06 March 2026
This paper was originally published under Creative Commons Attribution 4.0 International license, CC-BY-NC-ND, © The Author(s). It is now available under a Creative Commons Attribution 4.0 International license, CC-BY, © The Author(s). The error has been corrected in the online version of the article.
References
Hainsworth, R. Reflexes from the heart. Physiol. Rev. 71, 617–658 (1991).
Zeng, W. Z. et al. PIEZOs mediate neuronal sensing of blood pressure and the baroreceptor reflex. Science 362, 464–467 (2018).
Prescott, S. L. & Liberles, S. D. Internal senses of the vagus nerve. Neuron 110, 579–599 (2022).
Linden, R. J. Reflexes from receptors in the heart. Cardiology 61, 7–30 (1976).
Paintal, A. S. Vagal sensory receptors and their reflex effects. Physiol. Rev. 53, 159–227 (1973).
Bishop, V. S., Malliani, A. & Thorén, P. Cardiac mechanoreceptors. Compr. Physiol. 1983, 497–555 (1983).
Rutan, G. H. et al. Orthostatic hypotension in older adults—the cardiovascular health study. Hypertension 19, 508–519 (1992).
Hsueh, B. et al. Cardiogenic control of affective behavioural state. Nature 615, 292–299 (2023).
Min, S. et al. Arterial baroreceptors sense blood pressure through decorated aortic claws. Cell Rep. 29, 2192–2201 (2019).
Guyenet, P. G. & Bayliss, D. A. Neural control of breathing and CO2 homeostasis. Neuron 87, 946–961 (2015).
Lovelace, J. W. et al. Vagal sensory neurons mediate the Bezold-Jarisch reflex and induce syncope. Nature 623, 387–396 (2023).
Bainbridge, F. A. The influence of venous filling upon the rate of the heart. J. Physiol. 50, 65–84 (1915).
Crystal, G. J. & Salem, M. R. The Bainbridge and the “reverse” Bainbridge reflexes: history, physiology, and clinical relevance. Anesth. Analg. 114, 520–532 (2012).
Boettcher, D. H., Zimpfer, M. & Vatner, S. F. Phylogenesis of the bainbridge reflex. Am. J. Physiol. 242, R244–R246 (1982).
Bai, L. et al. Genetic identification of vagal sensory neurons that control feeding. Cell 179, 1129–1143.e1123 (2019).
Prescott, S. L., Umans, B. D., Williams, E. K., Brust, R. D. & Liberles, S. D. An airway protection program revealed by sweeping genetic control of vagal afferents. Cell 181, 574 (2020).
Nonomura, K. et al. Piezo2 senses airway stretch and mediates lung inflation-induced apnoea. Nature 541, 176–181 (2017).
Schappe, M. S. et al. A vagal reflex evoked by airway closure. Nature 627, 830–838 (2024).
Canning, B. J., Mori, N. & Mazzone, S. B. Vagal afferent nerves regulating the cough reflex. Respir. Physiol. Neurobiol. 152, 223–242 (2006).
Tränkner, D., Hahne, N., Sugino, K., Hoon, M. A. & Zuker, C. Population of sensory neurons essential for asthmatic hyperreactivity of inflamed airways. Proc. Natl Acad. Sci. USA 111, 11515–11520 (2014).
Bellono, N. W. et al. Enterochromaffin cells are gut chemosensors that couple to sensory neural pathways. Cell 170, 185–198 (2017).
Li, M. et al. Gut-brain circuits for fat preference. Nature 610, 722–730 (2022).
Williams, E. K. et al. Sensory neurons that detect stretch and nutrients in the digestive system. Cell 166, 209–221 (2016).
Smith, J. J., Forth, C. M. & Erickson, M. Hemodynamic-response to the upright posture. J. Clin. Pharmacol. 34, 375–386 (1994).
Doba, N. & Reis, D. J. Role of cerebellum and vestibular apparatus in regulation of orthostatic reflexes in cat. Circ. Res. 34, 9–18 (1974).
Freeman, R. et al. Orthostatic hypotension JACC state-of-the-art review. J. Am. Coll. Cardiol. 72, 1294–1309 (2018).
Yates, B. Vestibular influences on the sympathetic nervous-system. Brain Res. Rev. 17, 51–59 (1992).
Kapoor, W., Smith, M. & Miller, N. Upright tilt testing in evaluating syncope—a comprehensive literature-review. Am. J. Med. 97, 78–88 (1994).
Zheng, W. & Holt, J. R. The mechanosensory transduction machinery in inner ear hair cells. Annu. Rev. Biophys. 50, 31–51 (2021).
Teng, B. et al. Cellular and neural responses to sour stimuli require the proton channel Otop1. Curr. Biol. 29, 3647–3656 (2019).
Ranade, S. S. et al. Piezo2 is the major transducer of mechanical forces for touch sensation in mice. Nature 516, 121–125 (2014).
Marshall, K. et al. PIEZO2 in sensory neurons and urothelial cells coordinates urination. Nature https://doi.org/10.1038/s41586-020-2830-7 (2020).
Szczot, M., Nickolls, A., Lam, R. & Chesler, A. The form and function of PIEZO2. Annu. Rev. Biochem. 90, 507–534 (2021).
Wang, T., Tufenkjian, A., Ajijola, O. A. & Oka, Y. Molecular and functional diversity of the autonomic nervous system. Nat. Rev. Neurosci. 26, 607–622 (2025).
Kazci, Y. E. et al. Anatomical characterization of vagal nodose afferent innervation and ending morphologies at the murine heart using a transgenic approach. Auton. Neurosci. 242, 103019 (2022).
Scott, M. M., Williams, K. W., Rossi, J., Lee, C. E. & Elmquist, J. K. Leptin receptor expression in hindbrain Glp-1 neurons regulates food intake and energy balance in mice. J. Clin. Invest. 121, 2413–2421 (2011).
Xu, J. et al. GPR68 senses flow and is essential for vascular physiology. Cell 173, 762–775 (2018).
Chang, R. B., Strochlic, D. E., Williams, E. K., Umans, B. D. & Liberles, S. D. Vagal sensory neuron subtypes that differentially control breathing. Cell 161, 622–633 (2015).
Zhao, Q. et al. A multidimensional coding architecture of the vagal interoceptive system. Nature 603, 878–884 (2022).
Cheng, Z. X., Powley, T. L., Schwaber, J. S. & Doyle, F. J. Vagal afferent innervation of the atria of the rat heart reconstructed with confocal microscopy. J. Compar. Neurol. 381, 1–17 (1997).
Miller, M. R. & Kasahara, M. Studies on nerve endings in heart. Am. J. Anat. 115, 217 (1964).
Adrian, E. D. Afferent impulses in the vagus and their effect on respiration. J. Physiol. 79, 332–358 (1933).
Paintal, A. S. A study of right and left atrial receptors. J. Physiol. 120, 596–610 (1953).
Coleridge, H. M., Coleridge, J. C. & Kidd, C. Cardiac receptors in the dog, with particular reference to two types of afferent ending in the ventricular wall. J. Physiol. 174, 323–339 (1964).
Coleridge, J. C., Hemingway, A., Holmes, R. L. & Linden, R. J. The location of atrial receptors in the dog: a physiological and histological study. J. Physiol. 136, 174–197 (1957).
Kirchheim, H. R. Systemic arterial baroreceptor reflexes. Physiol. Rev. 56, 100–176 (1976).
Cornish, K. G., Gilmore, J. P. & McCulloch, T. Central blood volume and blood pressure in conscious primates. Am. J. Physiol. 254, H693–H701 (1988).
Gauer, O. H. & Henry, J. P. Circulatory basis of fluid volume control. Physiol. Rev. 43, 423–481 (1963).
Chi, J., Crane, A., Wu, Z. & Cohen, P. Adipo-Clear: a tissue clearing method for three-dimensional imaging of adipose tissue. J. Vis. Exp. https://doi.org/10.3791/58271 (2018).
Matsumoto, K. et al. Advanced CUBIC tissue clearing for whole-organ cell profiling. Nat. Protoc. 14, 3506–3537 (2019).
Susaki, E. A. et al. Advanced CUBIC protocols for whole-brain and whole-body clearing and imaging. Nat. Protoc. 10, 1709–1727 (2015).
Acknowledgements
We thank J. Holt, E. Liman and A. Patapoutian for providing mice; E. K. Williams for manuscript comments; and the Harvard Medical School Core for Imaging Technology and Education, Neurobiology Imaging Facility, Cardiovascular Physiology Core at Mass General Brigham, and the Imaging Analysis Collaboratory for technical assistance. This work was supported in part by a grant from the Lisa Yang Brain Body Center and the NIH (DP1 AT009497). S.M. was supported by the American Heart Association; M.J. by the American Diabetes Association (11–23-PDF-04); A.A.A. by a John S. LaDue Fellowship; and J.C. by a Helen Hay Whitney Fellowship. S.D.L. is an investigator of the Howard Hughes Medical Institute.
Author information
Authors and Affiliations
Contributions
Z.L., S.L., I.A.H., M.S.S., S.M., M.J., A.A.A., J.C., M.K. and S.D.L. designed experiments and analysed data. Z.L., M.J. and I.A.H. performed tilt-table experiments. S.L., Z.L., J.C., M.K. and A.A.A. performed anatomical analyses. Z.L. and S.M. performed whole-nerve electrophysiology. I.A.H. and Z.L. performed haemorrhage studies. M.S.S. and Z.L. performed calcium imaging. Z.L. and S.D.L. wrote the manuscript.
Corresponding author
Ethics declarations
Competing interests
S.D.L. is a founder of and consultant for Nilo Therapeutics. S.M. is now an employee of Novartis. The other authors declare no competing interests.
Peer review
Peer review information
Nature thanks Alexander Chesler and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Fig. 1 Physiological measurements during the tilt table test.
a, Blood pressure (top) and heart rate (bottom) traces upon rotation to upright posture in individual mice (grey) or all mice averaged (black), for individual mice, responses are averaged over at least 3 trials, n = 7 mice. b, Representative carotid and femoral blood pressure traces (top) and associated quantification (bottom) upon rotation to upright posture, initial: maximal deviation within first 5 sec, recovered: 2 sec baseline after 1 min, individual circles: average response of one mouse over at least 3 trials, n = 7 mice. c, Measurements in mice of genotypes indicated of baseline blood pressure (BP) in the supine position and the ratio of largest increase in HR to the largest drop in BP within the first 5 s after rotation to an upright posture. Controls include littermates lacking Phox2b-Cre (top left) or heterozygotes containing one Tmie or Otop1 knockout allele, mean ± sem, n = 11 Vagal-ΔPiezo1/2 mice and 9 Cre-negative littermate controls, 6 Vagal-ΔPiezo2 mice and 5 Cre-negative littermate controls, 8 Tmie knockout mice and 8 heterozygote littermate controls, 4 Otop1 knockout mice and 4 heterozygote littermate controls, **p = .0097 by a two-sided Mann-Whitney test.
Extended Data Fig. 2 Expression driven by Phox2b-Cre.
Representative wholemount images of tdTomato (Phox2b, magenta) and PGP9.5 (green) immunofluorescence in cleared tissues indicated, scale bar: 100 µm except 1 mm for heart, 3 replicates. We note that tdTomato signal in the heart is from extrinsic fibres not intrinsic heart cells.
Extended Data Fig. 3 Normal dose-dependent baroreflex in mice lacking only PIEZO2.
a, Representative blood pressure and heart rate traces from control (loxP-Piezo2 lacking a Cre allele) and Vagal-ΔPiezo2 mice in response to intravenous infusion of various doses of PBS or phenylephrine (PE). b, Quantitative analysis of baroreflex sensitivity across mice reveals a similar slope (ΔHR/ΔBP) of -7.1 in control mice and -8.9 in Vagal-ΔPiezo2 mice, Control: black dots, 30 trials from 5 mice, Vagal-ΔPiezo2: red dots, 24 trials from 4 mice, lines fitted by linear regression, ns: p > 0.05 between slopes by an analysis of covariance (ANCOVA) test.
Extended Data Fig. 4 Symmetry of vagal sensory axons in the cardiovascular system.
a, Cartoon of two-colour anatomical tracing of vagal sensory neurons in the heart, heart and syringe images created in BioRender. Lu, S. (2025) https://BioRender.com/ebmngtc. The left and right vagal ganglia of Vglut2-ires-Cre mice were injected with AAV-flex-tdTomato and AAV-flex-eGFP respectively and later, two-colour wholemount immunostaining was performed on the heart. Representative low magnification (b, c, scale bar: 1 mm) and high magnification (d, scale bar: 200 µm) confocal images (maximum intensity projection) of ventricle tissue sections, intact aorta or intact atria, 4 replicates.
Extended Data Fig. 5 Regionalization of vagal sensory axons in the atrium.
Representative confocal image of tdTomato immunofluorescence (5 replicates) near the atrium-vena cava junction of Piezo2-ires-Cre (a, left) and Npy2r-ires-Cre (b, right) mice previously injected in vagal ganglia with AAV-flex-tdTomato, scale bars: 1 mm, heart image created in BioRender. Lu, S. (2025) https://BioRender.com/h0xd2qa.
Extended Data Fig. 6 Normal hemodynamic responses on the tilt table require PIEZO2 neurons.
Representative traces of mean carotid blood pressure while mice are rotated from supine to upright (1), upright to prone (2), prone to upright (3) and upright to supine (4). Piezo2-ires-Cre; lsl-DTR and Npy2r-ires-Cre; lsl-DTR mice were injected in vagal ganglia with DT (VagalABLATE) or PBS (Control), and were selected from mice used in Fig. 2f.
Extended Data Fig. 7 Subtypes of PIEZO2-positive vagal sensory neurons that are dispensable for heartbeat-coupled responses.
a, UMAP plots depicting expression (natural log scale) of Phox2b, Piezo2, P2ry1, Glp1r, Pvalb and Oxtr based on a previously published vagal/glossopharyngeal cell atlas16. b, DTR immunostaining of vagal ganglia from P2ry1-ires-Cre; loxP-DTR, Pvalb-ires-Cre; loxP-DTR, Oxtr-ires-Cre; loxP-DTR and Glp1r-ires-Cre mice (left to right: 10, 7, 7, 6 replicates) that received no injection (top) or unilateral DT injection (bottom), scale bars: 500 µm. c, Representative (from replicates above) and simultaneously recorded electrocardiograms (ECG) and vagal nerve activity traces from the vagus nerve trunk corresponding to DT-injected ganglia of mice in b. d, Quantification of heartbeat-coupled vagal nerve trunk activity and intravenous saline infusion-induced vagal nerve trunk activity, mean ± sem, n = 12, 10, 7, 7, 6 mice, WT mice are the same reported in 3f and 3h. No statistical significance observed (p > .05) or **p = .0098 by a one-way ANOVA compared to wild-type (WT) with a Bonferroni correction for multiple comparisons.
Extended Data Fig. 8 Physiological responses during blood volume change.
a, Representative traces of peak left ventricle (LV) pressure and stroke volume measured by a cardiac catheter during upright tilt in wild type mice (left, normalized to 2 sec baseline before the tilt) and quantification (right) of the ratio of LV pressure and stroke volume in upright to prone mice, mean ± sem, n = 7. b, Representative traces of heart rate (HR) after saline infusion (10 s, volume: percentage of total blood volume estimated by weight) with subsequent trials initiated after return of HR to baseline (at least 2 min). c, Blood loss was measured 30 min after tail transection (left) or at survival endpoint (right) in genotypes indicated, mean ± sem. Blood loss was measured and normalized to total expected blood volume, which was determined by body weight, n (30 min)= 36 Vagal-ΔPiezo2, 39 Control (6 WT, 33 Cre-negative littermates), n (survival endpoint)= 19 Vagal-ΔPiezo2, 20 Control (Cre-negative littermates), circles: individual mice, ns: not significant (p > .05) by a two-sided Mann-Whitney test. d, Average blood pressure traces following blood removal from the jugular vein (15% of total blood volume estimated by weight) in 3 Vagal-ΔPiezo2 and Cre-negative control littermates, mean ± sem.
Extended Data Fig. 9 Responses of PIEZO2+ and PIEZO2- neurons to mechanosensory stimuli.
Heat map depicting calcium responses (ΔF/F colour coded) of vagal sensory neurons in Snap25-GCamp6s; Piezo2-ires-Cre; lsl-tdTomato mice to airway stretch (black) and venous saline infusion (red) in tdTomato+ (left) or tdTomato- (right) neurons, 4 mice.
Extended Data Fig. 10 Changes in blood pressure upon optogenetic activation of vagal trunk PIEZO2 neurons.
a, cartoon depicting optogenetic stimulation paradigm, image of scissors created in BioRender. Liu, Z. (2025) https://BioRender.com/s08uo8h and image of heart created in BioRender. Liu, Z. (2025) https://BioRender.com/a34i357. Representative traces (b) and quantification (c) of blood pressure (BP) and heart rate (HR) changes following optogenetic stimulation at frequencies indicated (blue bar, 1 min) of the vagus nerve trunk below the SLN departure point in Piezo2-ires-Cre; lsl-ChR2 mice, ECG entrained: illumination was time-locked to P and QRS peaks (blue shading) in the electrocardiogram (ECG), mean ± sem, n = 7 mice for 1–50 Hz stimulation, 5 for ECG entrained.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, Z., Lu, S., Haskell, I.A. et al. Vagal blood volume receptors compensate for haemorrhage and posture change. Nature 651, 1068–1076 (2026). https://doi.org/10.1038/s41586-025-10010-4
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41586-025-10010-4
This article is cited by
-
Vagal mechanoreceptors in the heart sense changes in blood volume
Nature Reviews Cardiology (2026)
