
Abstract
Netrin1, a developmental cue, is a master regulator of tumour epithelial-to-mesenchymal transition (EMT)1, a mechanism that is known to drive resistance to chemotherapy2. A netrin1 antibody (NP137)3 has been shown to inhibit tumour EMT in preclinical1 and clinical4 settings. In animal models of pancreatic cancer, netrin1 and its receptor neogenin have been shown to promote tumour progression5, EMT5 and metastasis6. Here we report the results of a phase 1b study that assesses the combination of NP137 with modified FOLFIRINOX (mFOLFIRINOX) in first line patients with locally advanced pancreatic cancer (ClinicalTrials.gov: NCT05546853). Forty-three patients were enrolled and received mFOLFIRINOX plus NP137 every other week for up to 12 cycles. NP137 was well tolerated. Median progression-free survival (PFS) was 10.85 months (95% confidence interval, 10.03–15.61) and median overall survival was 16.43 months (95% confidence interval, 12.75–non-reached), with 21 patients remaining alive at the time of data cut-off. Post-therapy conversion surgery occurred in 23% of patients. Laser capture microdissection was performed on pre-therapeutic biopsies and surgical specimens. Microbulk RNA sequencing confirmed that the main pathway that was down-regulated with the combination of mFOLFIRINOX plus NP137 was EMT. Moreover, survival outcomes were extended for patients with tumour cells that expressed high levels of the netrin1 receptor neogenin—median PFS 15.65 months in neogenin-high versus 10.22 months in neogenin low. Our results support the idea that netrin1 blockade alleviates resistance to chemotherapy by inhibiting EMT, particularly in neogenin-high pancreatic cancer.
Similar content being viewed by others


Main
Pancreatic ductal adenocarcinoma (PDAC) is a highly aggressive malignancy and currently ranks as the fourth leading cause of cancer-related death worldwide7, with a 5-year survival rate below 5%. Locally advanced PDAC (LAPC) is an intermediate stage that is found in roughly 30% of PDAC cases at diagnosis. These tumours are mostly unresectable due to vascular involvement, even though they lack distant metastases. LAPC has been sparsely studied, as these patients are usually excluded from metastatic trials and are not eligible for neoadjuvant or peri-operative trials owing to a poor resection rate. As a result, current treatment options for LAPC are limited, even in first line8. Median overall survival (OS) for LAPC is about 12–17 months (ref. 9), despite systemic chemotherapy regimens such as FOLFIRINOX (5-fluorouracil, leucovorin, irinotecan and oxaliplatin) or gemcitabine-based combinations, which generally yield a median PFS of 6–10 months (LAP-07; NEOPAN)10,11. There is a need for new treatment options that could increase tumour resection rate and enhance survival.
Netrin1 is an embryonic, secreted, laminin-related glycoprotein that has key roles in neuronal navigation, angiogenesis and cell survival12,13,14. Despite being expressed mainly during embryonic development, it has been shown to be regained by cancer cells as well as by the tumour microenvironment in a large fraction of human neoplasms12,15. Recent works have shown that netrin1 promotes early steps of tumour EMT, and a netrin1 monoclonal antibody NP137 is able to drive tumour re-epithelialization in preclinical mouse settings1 and in paired pre-treatment/C3D1 biopsies from patients with cancer treated with NP137 as monotherapy in a first-in-human trial4.
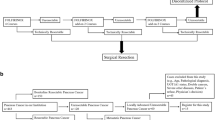
A significant hurdle in treating LAPC is chemoresistance, which frequently develops via EMT. This transition enables PDAC cells to become more invasive, promoting metastasis and further complicating treatment efforts16. Moreover, EMT-high or quasi-mesenchymal pancreatic cancer subtype has been shown to have worse prognosis17. Consequently, concurrent inhibition of EMT by targeting netrin1 with the NP137 monoclonal antibody during chemotherapy has been proposed in the Lap-NET1 trial (ClinicalTrials.gov: NCT05546853) as a strategy to enhance therapeutic efficacy and reduce resistance to chemotherapy (study design described in Fig. 1a and Supplementary Information). We investigated whether NP137 could bring clinical benefit to patients with locally advanced pancreatic cancer treated with mFOLFIRINOX. Here we report safety and efficacy results of NP137 in combination with mFOLFIRINOX during 12 cycles in a first line setting for patients with LAPC.

a, Design of the Lap-NET1 clinical trial. CnDn, cycle n, day n; EOT, end of treatment; NCCN, National Comprehensive Cancer Network; Q2W, Every 2 weeks. b, A patient presented with a locally advanced lesion of the pancreatic uncinate process. On baseline, contrast-enhanced CT in the arterial (top left) and venous (bottom left) phases show the lesion, measuring 35 mm on its longest axis (red arrowhead), encasing the superior mesenteric artery by more than 180° (red arrow). On follow-up, enhanced CT at week 24 of mFOLFIRINOX plus NP137 (arterial, top right; venous, bottom right) shows that the residual lesion has markedly decreased in size to 18 mm (red arrowhead) and no longer encases the superior mesenteric artery (red arrow). c, Waterfall plot of the maximum percentage change from baseline in tumour target lesion sum in evaluable patients. PD, progressive disease.
Lap-NET1 clinical trial results
The study objectives and design are described in Methods. Between March 2023 and June 2024, a total of 43 patients from 9 centres were enrolled, including 3 in the safety lead-in phase of the study, where the dose of 14 mg kg−1 every 2 weeks for NP137 was confirmed. Demographics of the safety analysis population (n = 43) were consistent with general trends among patients with LAPC: median age was 65, 51% were male, patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 (60%) or 1 (40%). Vascular encasement of aorta, mesenteric superior artery and celiac trunk was present in 5%, 58% and 51% of participants, respectively. Patients were considered at baseline as never resectable (54%) or potentially resectable (46%), with baseline CA 19.9 of more than 500 UI ml−1 in 42% of patients (Supplementary Table 1 and Supplementary Information). Of note, two patients were enrolled despite a metastatic disease.
Safety is reported in all 43 participants who received at least one dose of treatment. All patients experienced at least one adverse event: 58% experienced at least one adverse event of grade 3 or higher, 47% experienced at least one NP137-related adverse event, including 12% who experienced a NP137-related adverse event of grade 3 or higher (Table 1 and Supplementary Table 2). Two grade 5 adverse events corresponding to septic shock were reported and assessed as related to the disease and potentially related to mFOLFIRINOX. Common adverse events were diarrhoea (67% of patients; 2% grade 3 or higher), nausea (60% of patients; 2% grade 3 or higher), asthenia (58% of patients; 5% grade 3 or higher), thrombocytopenia (40% of patients; 2% grade 3 or higher), anaemia (40% of patients; no grade 3), neutropenia (21% of patients; 2% grade 3 or higher) and mucositis (14% of patients; no grade 3). The most common NP137-related adverse event was infusion-related reactions, which occurred in 9% of patients. These infusion-related reactions were generally of mild to moderate intensity (no grade 3 or higher) as a result of systematic premedication. Other common NP137-related adverse events were blood disorders such as anaemia (9%), neutropenia (9%) and thrombocytopenia (9%). The incidence of treatment-related grade 3/4 adverse events in this study was 37%, similar to what is expected for the mFOLFIRINOX alone.
The median number of treatment cycles administered for NP137 was 12 (range 11–12) and the median follow-up was 13.1 months at the time of data cut-off (Table 1). Efficacy was assessed in the intention-to-treat (ITT) population (n = 43) except for objective response rate (ORR), which included treated patients with at least one post-baseline tumour imaging computed tomography (CT) scan. ORR was evaluated on 41 patients using RECIST 1.1 (Response Evaluation Criteria in Solid Tumors) confirmed investigator-assessed responses as the 2 grade 5 events occurred before the first CT scan assessment. Overall, 12 out of 41 evaluable patients achieved a response, all partial response (PR) (ORR 29%, 95% confidence interval 0.16–0.46) (Fig. 1b,c). Notably, responses were durable, with a median duration of response of 9.02 months (5.84, non-computable), and 27 patients achieved stable disease (SD) as best response leading to a disease control rate of 95% (95% confidence interval, 83–99) (Figs. 1c and 2a). Out of RECIST v1.1 criteria, 88% of patients experienced a decrease in tumours (Fig. 1c). The median PFS was 10.85 months (95% confidence interval, 10.03–15.61) with 6- and 12-month PFS of 88% (95% confidence interval, 75–96) and 45% (95% confidence interval, 30–61), respectively (Fig. 2a,b). The median OS was 16.43 months (95% confidence interval, 12.75, non-reached (NR)) with 6- and 12-month OS of 91% (95% confidence interval, 78–97) and 62% (95% confidence interval, 46–77) (Fig. 2a,c). At week 24, a CA 19.9 reduction of more than 50% of the baseline value was observed in 69% of evaluable patients (20 out of 29) (95% confidence interval, 49–85%) (Extended Data Fig. 1). Finally, the ITT resection rate was 23% (10 out of 43 patients) (Table 2 and Supplementary Table 3).

a, Swimmer plot of events and follow-up durations for all 43 ITT patients. NA, non-evaluable. b, Kaplan–Meier estimates of PFS. The shaded area (light grey) represents the 95% confidence interval. c, Kaplan–Meier estimates of OS. The shaded area (light grey) represents the 95% confidence interval.
NP137 inhibits EMT in patients with LAPC
Pancreatic tumours treated with mFOLFIRINOX have been reported to shift towards a more mesenchymal state18 and EMT has been described as one of the main pathways that is up-regulated in tumour cells in response to this treatment regimen19. This phenomenon has been proposed as a mechanism of resistance to this treatment regimen18,19. We thus hypothesized that co-administration of NP137 could mitigate this tumour EMT induced by mFOLFIRINOX. Per protocol, fine needle aspiration at diagnosis was collected from 32 patients regardless of clinical outcomes, alongside resection material from 7 patients who benefited from surgery post-treatment. Owing to the challenges associated with aspiration-derived material, which often yields low-quality specimens with limited cellularity, laser capture microdissection (LCM) was systematically performed on both aspiration and surgical samples (Fig. 3a). The collected tumour cells were then processed for microbulk RNA sequencing (RNA-seq). Quality control was validated for pre-treatment samples from 22 patients and surgery samples of 6 patients including 4 paired pre-treatment surgery samples. High tumour cell content of the LCM was verified by measuring epithelial purity using the Estimate plugin (Extended Data Fig. 2a). We first blindly compared all the 22 pre-treatment materials to all 6 post-treatment samples altogether. Using a false discovery rate (FDR) threshold of 0.05, we identified 260 differentially expressed genes (DEGs), with 232 up-regulated genes and 28 down-regulated genes after treatment (Fig. 3b and Extended Data Fig. 2b,c). Gene set enrichment analysis (GSEA) revealed that whereas the pancreatic beta cell pathway was the only pathway that was enriched, a global downregulation of inflammatory pathways, including IL-6–JAK–STAT3 signalling or IFNγ response was observed after treatment (Fig. 3c). Of interest and consistent with the previously described mode of action of NP137, the EMT pathway was significantly down-regulated following treatment (normalized enrichment score = −1.5, adjusted P value = 0.025) (Fig. 3c). The same downregulation of the EMT pathway was observed when the GSEA analysis was restricted to paired pre- and post-treatment samples (Extended Data Fig. 2d). Further analysis of the 200 EMT genes in the Hallmark dataset revealed that only 45 genes accounted for the observed inhibition of EMT between pre- versus post-treatment biopsies. We thus defined a core EMT signature of 45 genes (Supplementary Table 4). This core EMT signature was shown to be strongly down-regulated when comparing pre- versus post-treatment biopsies from the phase 1 study reported previously4 (Extended Data Fig. 2e). As shown in Fig. 3d and Extended Data Fig. 2f, there was a strong core EMT signature decrease upon NP137 plus mFOLFIRINOX treatment in patients experiencing a PR or a SD. When analysing this core EMT in an available dataset of patients with LAPC treated with mFOLFIRINOX alone (Linehan-seq; Gene Expression Omnibus (GEO) accession GSE13105020,21), this core EMT was increased (Fig. 3e). We thus compared the paired pre- and post-treatment Lap-NET1 samples (NP137 plus mFOLFIRINOX) to the paired pre- and post-treatment samples of patients with LAPC treated with mFOLFIRINOX alone (mFOLFIRINOX, Linehan-seq dataset) and further observed that the main Hallmark that was down-regulated between NP137 plus mFOLFIRINOX versus mFOLFIRINOX alone was EMT (Fig. 3f). Notably, although high EMT or mesenchymal status is generally associated with a worse prognosis in patients with pancreatic cancer who are receiving standard chemotherapy17,20, we observed no correlation between EMT score and PFS in patients in the Lap-NET1 cohort who were treated with mFOLFIRINOX and NP137 (Fig. 3g). Similarly, although molecular subgroups using Moffit’s or PurIST scoreshave shown different prognostic values between classical and basal-like subgroups21,22, we did not observe any significant difference between classical and basal-like subgroups in PFS or OS in the 22 patients in Lap-NET1 with available transcriptomic data (Extended Data Fig. 3a–d). Together, these pre- versus post-treatment analyses performed on more than half of the patients treated in the Lap-NET1 trial support the view that NP137 strongly inhibits tumour EMT and counteracts the EMT-associated resistance induced by mFOLFIRINOX.

a, Experimental workflow. Schematic created in BioRender; Paradisi, A. https://biorender.com/iivtmrk (2026). b, Volcano plot depicting transcriptional changes between pre- and post-treatment tumours. Genes are highlighted based on non-adjusted P value and fold change (FC), both derived from a negative binomial generalized linear model, glmQLFit. NS, not significant. c, GSEA identifies the top 10 Hallmark pathways that are enriched in the Lap-NET1 dataset comparing all pre-treatment to all post-treatment samples. The dot plot (left) indicates the pre-ranked gene set enrichment FDR-adjusted P value; the ridge plot (right) highlights the enrichment score. Both are sorted by P value. d, Quantification of the core EMT signature (45 EMT genes explaining GSEA results), showing a reduced EMT score in post-treatment samples (two-sided Wilcoxon rank-sum test, P = 0.0012) in the Lap-NET1 dataset. e, Quantification of the core EMT signature (45 EMT genes explaining GSEA results) showing an increased EMT score in post-treatment samples (two-sided Wilcoxon rank-sum test, P = 0.84) in the Linehan dataset. The underlying distribution is shown via violin plots. Box plots in d,e indicate the median (centre line), interquartile range (box) and 1.5× interquartile range (whiskers). f, GSEA identifies the top 10 Hallmark pathways enriched in the post versus pre-treatment comparison between the Lap-NET1 (NP137 plus mFOLFIRINOX) and Linehan (mFOLFIRINOX) dataset. The dot plot on the left indicates the pre-ranked gene set enrichment FDR-adjusted P value, the ridge plot on the right highlights the enrichment score. Both are sorted by P value. g, Correlation between the Hallmark EMT signature score and PFS in the Lap-NET1 cohort (two-sided Pearson’s R = –0.24, P = 0.28). The line represents a fitted linear model, with the shaded area (light pink) representing the 95% confidence interval of the regression estimate.
Predictive value for efficacy of neogenin
In the cohort of 22 patients with available pre-treatment transcriptomic analysis, 21 were not considered as primary refractory (either SD or PR at 6 weeks). In this cohort of 21 patients, we explored molecular pathways and genes that could be associated with improved PFS. Given the target of NP137, we focused on components of the netrin1 signalling pathway. Among these, NEO1, which encodes the netrin1 receptor neogenin, showed a significant positive correlation between its expression and PFS (Extended Data Fig. 4a). To further assess the predictive relevance of neogenin NP137 efficacy, we assessed whether it is a prognostic factor in patients treated with mFOLFIRINOX alone. We analysed an independent dataset from which PFS and OS data of patients could be extracted23; in this cohort of 42 patients with LAPC treated with mFOLFIRINOX alone, we observed a trend towards higher NEO1 expression associated with poorer prognosis (Extended Data Fig. 4b). Consistently, patients with high neogenin treated with mFOLFIRINOX alone exhibited a trend towards shorter median PFS compared with patients with low neogenin (Fig. 4a) without the corresponding difference in OS (Extended Data Fig. 4c). We next assessed the correlation between neogenin expression and survival criteria in the 21 patients treated with mFOLFIRINOX plus NP137. Patients with high neogenin expression had a markedly higher median PFS of 15.65 months, than those with low neogenin expression (median PFS of 10.22 months; P = 0.003), representing an improvement of over 5 months (Fig. 4b). Moreover, for the high-neogenin group, median OS was not reached (Fig. 4c) and conversion surgery was performed in 40% (4 out of 10). Similar data were obtained when considering the full cohort of 22 patients (Extended Data Fig. 4d,e). The predictive value of neogenin expression was further evaluated by immunohistochemistry (IHC), performed by two independent pathologists (Fig. 4d). Considering sample availability and the rarity of tumour cell contingents, only 19 pre-treatment samples could be processed. We first compared the mRNA data from the microbulk RNA-seq and protein expression levels by IHC and observed a good correlation (Fig. 4e and Extended Data Fig. 4f). Of interest, we observed very similar effect on PFS and OS in patients with high neogenin, with a median PFS of 14.6 months and a median OS not reached in the high-neogenin population (Fig. 4f,g). Together, these findings strongly suggest that neogenin expression may stratify patients who are more likely to benefit from NP137-based therapy and support its potential as a biomarker for better population targeting.

a, Kaplan–Meier estimates of PFS in 42 patients with LAPC who were treated with mFOLFIRINOX in Nicolle et al.23, stratified by neogenin expression based on the median. Patients with low NEO1 expression exhibit a longer PFS (P = 0.17). b, Kaplan–Meier estimates of PFS in the Lap-NET1 cohort of 21 patients with SD or PR with available pre-treatment transcriptomic analysis, stratified by high and low neogenin expression based on the median. Patients with high NEO1 expression exhibit better PFS (P = 0.003). c, Kaplan–Meier estimates of OS in the Lap-NET1 cohort of 21 patients with SD or PR with available pre-treatment transcriptomic analysis, stratified by high and low neogenin expression based on the median. Patients with high NEO1 expression exhibit better OS (P = 0.0094). d, Representative IHC of neogenin, showing a negative case (top) and a highly positive case (bottom). Scale bar, 20 µm. e, Dot plot representing epression of NEO1 mRNA measured by RNA-seq after LCM according to the two groups identified by neogenin IHC. Number of patients (n) = 9 (neg/low) and n = 10 (high). Centre lines are mean and error bars indicate s.e.m. Mann–Whitney two-sided test, ***P < 0.0001. TPM, transcripts per million. f, Kaplan–Meier estimates of PFS in the Lap-NET1 cohort of 19 patients with identifiable tumour cells on a pre-treatment slice stained for neogenin by IHC, stratified by neg/low and high neogenin expression. Patients with high neogenin expression have longer PFS (P = 0.024). g, Kaplan–Meier estimates of OS in the Lap-NET1 cohort of 19 patients with identifiable tumour cells on a pre-treatment slice stained for neogenin by IHC, stratified by neg/low and high neogenin expression. Patients with high neogenin expression exhibit longer OS (P = 0.032).
Because neogenin expression appears here as a pre-requirement for clinical benefit to the anti-netrin1 therapy, we explored whether netrin1 or neogenin were implicated in pancreatic cancer progression. Of note, a recent study implicated neogenin in pancreatic cancer progression, and NP137 was shown to inhibit EMT and tumour growth in animal models through a neogenin-dependent mechanism5. We thus silenced neogenin expression using small interfering RNA (siRNA) in the Panc02 mouse pancreatic tumour model (Extended Data Fig. 5a,b and Supplementary Fig. 1). As a surrogate marker for EMT, we evaluated the migratory potential of Panc02 cells in a wound-healing assay in the presence or absence of NP137. As shown in Extended Data Fig. 5c–e, netrin1 blockade with NP137 inhibits cell migration in a neogenin-dependent manner. Moreover, using a MAPK inhibitor we further observed that the MAPK–ERK pathway is required for netrin1–neogenin pro-tumoural activity (Extended Data Fig. 5d,e).
Discussion
Here we provide the first evaluation of the netrin1 monoclonal antibody NP137 in combination with mFOLFIRINOX therapy in first line settings for patients with LAPC. Although the single-arm design prevents definitive comparative conclusions, several important observations emerge from these data.
The combined treatment was well tolerated and did not lead to a meaningful increase in adverse events beyond the established safety profile of mFOLFIRINOX alone. NP137-related adverse events were manageable and predominantly of low grade, supporting the feasibility of adding anti-netrin1 treatment to an intensive cytotoxic regimen.
Additionally, the combined treatment demonstrated antitumour activity in a well-defined LAPC population. The observed median PFS of 10.85 months and median OS of 16.43 months compare favourably with benchmark studies such as NEOPAN. Notably, 23% of patients underwent surgical R0 resection following treatment, a substantially higher rate than typically reported in LAPC, representing a clinically meaningful outcome, as surgical resection is strongly associated with improved survival in this population. Indeed, secondary surgery remains very uncertain in this patient population, with prospective data from literature showing resections rate around 5–18%, with 6% and 18% of R0 resection under FOLFIRINOX in the NEOPAN11 and CONKO-00724 trials, respectively, and 10.8% under GEMBRAX in the PANOVA3 trial25. The Lap-NET1 population was comparable with patients from these trials regarding vascular involvement and baseline CA 19.9 plasmatic level. Even though this trial was not designed for survival analyses and further randomized data are needed, these results suggest that NP137 may enhance the effectiveness of mFOLFIRINOX and increase the likelihood of potentially curative interventions. The translational analysis also provides mechanistic insights into the biological activity of NP137. Transcriptomic analyses of microdissected tumour samples revealed a consistent downregulation of EMT pathways following treatment. Given the established role of such pathways in chemoresistance in PDAC, these data support the idea that netrin1 blockade may restore chemosensitivity by promoting tumour re-epithelialization. One limitation of the present study is the pre-planned discontinuation of the experimental treatment. In line with the known continuous phenotypic plasticity of cancer cells, a longer duration of treatment with NP137 may yield additional survival benefit for the patients without increased toxicity, in line with the expected excellent tolerance profile of NP137 with a maintenance chemotherapy such as 5-fluorouracil.
Furthermore, pre-planned exploratory analyses identified neogenin as a predictive marker of the combination treatment benefit. Neogenin is a receptor of netrin1 and was recently shown to drive netrin1-mediated pancreatic cancer progression in preclinical settings5. In the Lap-NET1 study, patients with high neogenin expression, based on tumour RNA-seq and IHC, experienced an extended PFS (around 5 months in neogenin-high patients) and improved OS when treated with mFOLFIRINOX plus NP137. These preliminary results will need to be confirmed in randomized trials. They support patient stratification strategies as mFOLFIRINOX plus NP137 might be particularly beneficial in pre-defined molecular subgroups with high neogenin expression on pre-therapeutic tumour samples.
Conclusion and perspective
NP137 in combination with mFOLFIRINOX demonstrates a favourable safety profile, promising clinical activity, and a mechanistically distinct mode of action supported by translational analyses. These results warrant further investigation of netrin1 blockade and provide a rationale for a biomarker-driven development of NP137 in pancreatic cancer. The Lap-NET1 study was conducted in patients with locally advanced pancreatic cancer with the idea that EMT drives the metastatic process. Given that EMT being also active in metastatic lesions, we speculate that patients with metastatic PDAC may similarly benefit from NP137 plus chemotherapy. The next step in the development for NP137 therapy in pancreatic cancer is a randomized phase 2 trial to assess the combination of NP137 with standard of care for the first line treatment of patients with metastatic PDAC. One of the main objectives of this study will be to confirm the predictive value of the neogenin IHC test on efficacy.
Methods
Lap-NET1 clinical trial
Study design and participants
Lap-NET1 is a multicentric, prospective, single-arm phase 1b trial. This study included a safety lead-in phase to confirm the recommended dose of NP137 in combination with mFOLFIRINOX (ClinicalTrials.gov identifier: NCT05546853). Patients were enrolled and treated between March 2023 and June 2024 at nine sites in France.
Eligible patients were 18 years and older with histological or cytological confirmed diagnosis of locally advanced PDAC. The tumour was considered unresectable according to the NCCN Guidelines v2.2021. Prior systemic therapy, radiation therapy or resection for pancreatic cancer were not allowed. Patients had an ECOG performance status of 0 or 1 and a measurable disease per RECIST v1.1.
Ethics statement
The protocol was approved by the ethical committee and the French National Agency for Medicines and Health Products Safety (ANSM); the approvals were recorded via the EU Clinical Trials Information System (CTIS) (CTIS number 2022-500905-42-00). The trial was registered at http://www.clinicaltrials.gov under ID NCT05546853. All participants provided written informed consent prior to enrolment.
Procedures
During the safety lead-in phase, 3 to 12 patients would be enrolled to confirm the dose of 14 mg kg−1 (intravenously) every 14 days for NP137 in combination with mFOLFIRINOX (oxaliplatin (85 mg m−2), calcium levofolinate (200 mg m−2), irinotecan (150 mg m−2) on day 1 and 5-fluorouracil (2.4 g m−2 over 46 h)) administered every 14 days.
After the safety lead-in, 40 additional patients were treated with intravenous NP137 at the recommended dose, associated with modified FOLFIRINOX every 14 days until progression or the maximum treatment duration is reached (6 months, 12 cycles), or unacceptable tolerability. After completion, the investigator chose whether to stop the treatment and follow the patient, or use a follow-up treatment such as radiotherapy, radio-chemotherapy, maintenance chemotherapy or surgical resection (for eligible patients). Patients were followed up until progression and death.
End-points
The primary end-point was the proportion of patients experiencing adverse events of any grade and grade 3/4 adverse events as defined by the National Cancer Institute–CTCAE v5.0 related to the experimental treatment.
Secondary end-points included best overall ORR, disease control rate, duration of response, proportion of surgical resection, PFS and OS.
Exploratory analysis included the effect of specific mutational and expression status, including EMT markers, associated with the patient’s benefit. Descriptive study in spatial transcriptomics and IHC of the evolution of EMT markers, netrin1 expression and tumour microenvironment by comparing pre-therapeutic biopsies to tumour samples obtained during surgical tumour resection.
Statistical analysis
The data cut-off date was May 2025, and the safety analysis population includes all patients who received at least one dose of study drug (n = 43). Safety end-points were tabulated by organ class and grade, using NCI-CTCAE whenever possible. The efficacy evaluable set includes all ITT patients except for ORR including treated patients with at least one post-baseline tumour imaging scan. Descriptive statistics were used to summarize trial results. Continuous variables were summarized by their median and interquartile range, and qualitative variables by counts and percentages. Objective response was expressed as empirical proportions with their exact 95% confidence interval calculated using the Clopper–Pearson method. Duration of response, PFS and OS were summarized using the Kaplan–Meier method, and median survival times with their 95% confidence interval were provided. All analyses were done using R v4.3.
Laser capture microdissection
Tumour samples were formalin-fixed paraffin-embedded (FFPE) for further histologic analysis. Paraffin blocks were sectioned at 3 μm and dried for 1 h at 65 °C. One slide was submitted to HPS histological staining in order to determine tumour cell clusters. Five additional slides were stored at –80 °C prior to LCM. For each experiment, slides were deparaffinized and stained as follows: 2 min xylene, 1 min ethanol (100%), 30 s ethanol (95%, 75%, 50%), 30 s cresyl violet (1%), followed by 30 s ethanol (50%, 75%, 95%) and 2× 30 s ethanol (100%).
LCM was performed on a PALM MicroBeam system (v4.6, P.A.L.M. Microlaser Technologies) with RoboSoftware. Regions of interest were identified on serial scans at 5× magnification and precisely dissected at 20×. Because archived glass slides without membrane coating were used, dissection was carried out in ROBO-LPC mode, allowing automated catapulting of tissue fragments by multiple laser pulses. Laser settings (power and duration) were optimized for capture efficiency.
Microdissected material was collected in 0.5 ml Zeiss adhesive cap tubes (Carl Zeiss Microscopy; one tube per slide). Dissections were completed within 60 min, with dissected areas ranging from ~7 × 104 to 1.4 × 106 µm2. RNA was extracted in 150 µl PKD buffer using the RNeasy FFPE Micro Kit (Qiagen) according to the manufacturer’s protocol. RNA integrity (RIN) and DV200 were assessed with the Agilent 2100 Bioanalyzer (Agilent Technologies).
Whole transcriptome was captured from 1 ng of tumoural RNA. Libraries were prepared using Takara Bio SMART-Seq mRNA LP reagents following the manufacturer’s recommendations. Libraries were sequenced using the NovaSeq6000 Illumina sequencer in 100 bp paired-end.
Bioinformatic analysis
After Illumina sequencing, standard bioinformatics analysis were used to generate fastq files, followed by quality assessment (fastqc v0.11.9 and MultiQC v1.23). Sequencing reads were trimmed to remove adapter sequences and low-quality bases using Trim Galore! v0.6.10. Trimmed reads were then aligned to the human reference genome (GRCh38/hg38) using the align function of Rsubread v2.18.0. Following alignment, gene-level read counts were quantified from the aligned BAM files using the featureCounts function from the Rsubread package.
The counts were then loaded into a DGEList object using the edgeR package v4.6.2 for downstream differential expression analysis. Genes with low expression were filtered out using the edgeR filterByExpr function. The calcNormFactors function was used to normalize for library size and RNA composition bias. DEGs were extracted based on an FDR-adjusted P value < 0.05. Counts per million (CPM) values were calculated with a prior count of 2 and log-transformed for visualization and estimation of signature scores using singscore v1.28.0.
Molecular classification was performed using tte PDACMOC R package v2.5.2 (ref. 26) to classify samples based on several established PDAC molecular subtyping schemes, including those from Collisson27, Moffitt22, Bailey28, Puleo29, Chan-Seng-Yue30 and a PDAC consensus classifier. In addition, the PurIST (Purity Independent Subtyping of Tumors) algorithm21, specifically developed for pure tumour samples, was applied to the count data to distinguish between basal-like and classical subtypes. A PurIST basal-like score (PBP) greater than 0.5 was used to classify samples as basal-like, while scores less than or equal to 0.5 were classified as classical.
GSEA was performed to identify biological pathways and functions enriched in the DEGs between experimental groups (for example, pre- versus post-treatment, or PR versus SD, according to the RECIST 1.1 classification). The analysis was conducted using the GSEA function of clusterProfiles v4.16.0 and the MSigDB H (Hallmarks) gene sets.
Raw counts of the dataset GSE253260 corresponding to the study by Nicolle et al.23 were downloaded directly from the GEO website and processed with edgeR, as described above.
Survival curves were estimated using the Kaplan–Meier method, and survival outcomes were compared between groups with a log-rank test, using the survival v3.8-3 package.
All R/Bioconductor analyses were based on R v4.5.1 (2025-06-13) (https://cran.r-project.org/) using Rstudio software (https://posit.co/download/rstudio-desktop/). Most visualizations are based on ggplot2 (https://ggplot2.tidyverse.org/).
To infer tumour purity, we used the ESTIMATE algorithm31, which uses single-sample GSEA (ssGSEA) with stromal and immune cell signatures. To this end, ESTIMATE scores were calculated in normalized counts of the Lap-NET1 dataset and next transformed to relative purity scores for visualization.
In some analyses, the Lap-NET1 dataset was integrated at the count level with the Linehan-seq dataset (GSE131050) originally described by Nywening et al.32. This cohort includes RNA-seq data of LAPC samples obtained with fine needle aspiration, including pre-treatment samples for nine patients subsequently treated with FOLFIRINOX, five of which also having matched post-treatment RNA-seq data. To minimize batch effects, we used raw fastq data (Sequence Read Archive (SRA) study SRP197641) processed with the same alignment/mapping pipeline (Rsubread) for both datasets before integration. In the combined dataset, we isolated the unique effect of NP137 that goes beyond the effect of FOLFIRINOX, by using a paired interaction strategy (between pre and post timepoint and treatment).
Neogenin IHC
IHC was performed on the Leica Bond RX automated immunostainer (Leica biosystems) using Bond Polymer Refine Detection Kit according to the manufacturer’s instructions. Slides were dewaxed at 72 °C with Bond Dewax Solution (Leica Biosystems, AR9222) and antigen retrieval was performed using Bond Epitope Retrieval Solution 2 (ph9, Leica, AR9640) for 20 min at 97 °C. Sections were incubated with a rabbit recombinant monoclonal neogenin antibody (diluted at 1:1,000, Abcam, Ab324107) for 30 min. Staining was visualized with 3,3′-diaminobenzidine as a chromogenic substrate. Finally, the sections were counterstained with haematoxylin. Finally, sections were scanned with panoramic scan II (3D Histech, Budapest, Hungary) at 20×. All the scans were interpreted by two independent pathologists specialized in digestive oncology.
Cell line and cell culture
The mouse cell line Panc02 was grown in low-glucose Dulbecco’s Modified Eagle’s Medium (DMEM, Gibco) complemented with 10% fetal bovine serum (FBS, Gibco) and 1% penicillin/streptomycin (Gibco). Cells were maintained in culture at 37 °C under humidified atmosphere consisting of 20% O2 and 5% CO2.
RNA extraction and RT–qPCR
Total RNA was isolated from cells using NucleoSpin RNA Plus kit (Macherey-Nagel) according to the manufacturer’s instructions, after washing the cells with PBS pH 7.4 (Gibco). Expression of mRNA was measured using a NanoDrop1000 (Thermo Fisher Scientific). RNA was retrotranscribed using the T100 ThermoCycler (Bio-Rad) and the iScript cDNA Synthesis Kit (Bio-Rad) according to the manufacturer’s instructions. Quantitatyive PCR with reverse transcription (RT–qPCR) was performed using QuantStudio 3 (Thermo Fisher Scientific) and OneGreen Fast qPCR Premix (Ozyme) according to the manufacturers’ instructions.
Cell lysate collection, western blot and antibodies
Confluent cells were washed with cold PBS and scrapped in lysis buffer (Tris 10 mM pH 7.6; SDS 5; Glycerol 10%; Triton X-100 1%, DTT 100 mM). After sonication, proteins were quantified using Pierce 660 nm Protein Assay Reagent (Thermo Fisher Scientific) and loaded on 7.5% SDS–polyacrylamide gels (Bio-Rad) transferred to nitrocellulose membranes using Trans-Blot Turbo Transfer (Bio-Rad). Membranes were blocked for 1 h at room temperature with 5% of nonfat dried milk for netrin1 GAPDH and with 5% of BSA for neogenin. Staining was performed overnight with following antibodies: anti-netrin1 (diluted at 1:1,000, Ab126729, Abcam), anti-neogenin (diluted at 1:1,000, D7M8E, Cell Signaling Technology) and anti-GAPDH (diluted at 1:1,000, 5174, Cell Signaling Technology). After washing, membranes were incubated with secondary antibody, goat anti-rabbit coupled with HRP (diluted at 1:10,000, ARG65351, Arigo), for 1 h at room temperature. West Dura Chemiluminescence System (Thermo Fisher Scientific) was used to intensify the signal. Imaging was performed using Chemidoch Touch (Bio-Rad).
Wound-healing migration assays
Panc02 cells were transfected overnight with negative control (Life Technologies) or mouse NEO1-targeting siRNAs (L-047750-00-0005, Dharmacon) at a final concentration of 10 nM, using Lipofectamine RNAiMAX reagent (Thermo Fisher Scientific) and OptiMEM medium (Gibco). Cells were then plated in Incucyte ImageLock 96-well plates (Sartorius) at a final concentration of 25,000 cells per well and pretreated for 24 h with netrin1 antibody NP137 or isotypic control NP001 (20 µg ml−1). After 24 h, confluent cells were wounded and washed twice with PBS to remove detached cells. Medium was changed and supplemented with either control, NP137 and/or MEK1/2 inhibitor (PD0325901, 10 nM, Sigma-Aldrich). Wound recovery was monitored for 48 h using Sartorius Incucyte S3 Live Cell-Analysis System.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The raw RNA-seq data of this study have been deposited into the Gene Expression Omnibus (GEO) GSE319924. Individual participant data are not freely available for ethical and/or legal issues. De-identified data may be shared upon request, subject to the signing of a data use agreement, provided that the request is consistent with the purpose of use to which participants consented at the time of inclusion. These can be requested from admin@netrispharma.com and will be answered within 30 working days.
Code availability
For version control, sharing and reproducibility, all bioinformatic code related to the study will be kept in a Github repository https://github.com/Genomics-Consulting/Netris_LapNet.
References
Lengrand, J. et al. Pharmacological targeting of netrin-1 inhibits EMT in cancer. Nature 620, 402–408 (2023).
Lambert, A. W., Pattabiraman, D. R. & Weinberg, R. A. Emerging biological principles of metastasis. Cell 168, 670–691 (2017).
Grandin, M. et al. Structural decoding of the Netrin-1/UNC5 interaction and its therapeutical implications in cancers. Cancer Cell 29, 173–185 (2016).
Cassier, P. A. et al. Netrin-1 blockade inhibits tumour growth and EMT features in endometrial cancer. Nature 620, 409–416 (2023).
Ochiai, Y. et al. Netrin-1 promotes pancreatic tumorigenesis and innervation through NEO1. Cancer Res. https://doi.org/10.1158/0008-5472.CAN-25-2243 (2026).
Dudgeon, C. et al. Netrin-1 feedforward mechanism promotes pancreatic cancer liver metastasis via hepatic stellate cell activation, retinoid, and ELF3 signaling. Cell Rep. 42, 113369 (2023).
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263 (2024).
Sally, Á, McGowan, R., Finn, K. & Moran, B. M. Current and future therapies for pancreatic ductal adenocarcinoma. Cancers 14, 2417 (2022).
Eshmuminov, D. et al. FOLFIRINOX or gemcitabine-based chemotherapy for borderline resectable and locally advanced pancreatic cancer: a multi-institutional, patient-level, meta-analysis and systematic review. Ann. Surg. Oncol. 30, 4417–4428 (2023).
Hammel, P. et al. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: the LAP07 randomized clinical trial. JAMA 315, 1844–1853 (2016).
Ducreux, M. et al. PRODIGE 29-UCGI 26 (NEOPAN): A phase III randomized trial comparing chemotherapy with FOLFIRINOX or gemcitabine in locally advanced pancreatic carcinoma. J. Clin. Oncol. 43, 2255–2264 (2025).
Mehlen, P., Delloye-Bourgeois, C. & Chédotal, A. Novel roles for slits and netrins: axon guidance cues as anticancer targets? Nat. Rev. Cancer 11, 188–197 (2011).
Brisset, M., Grandin, M., Bernet, A., Mehlen, P. & Hollande, F. Dependence receptors: new targets for cancer therapy. EMBO Mol. Med. 8, e14495 (2021).
Wu, Z. et al. Long-range guidance of spinal commissural axons by netrin1 and sonic hedgehog from midline floor plate cells. Neuron 101, 635–647.e4 (2019).
Sung, P.-J. et al. Cancer-associated fibroblasts produce netrin-1 to control cancer cell plasticity. Cancer Res. 79, 3651–3661 (2019).
Aiello, N. M. et al. EMT subtype influences epithelial plasticity and mode of cell migration. Dev. Cell 45, 681–695.e4 (2018).
Zheng, X. et al. Epithelial-to-mesenchymal transition is dispensable for metastasis but induces chemoresistance in pancreatic cancer. Nature 527, 525–530 (2015).
Porter, R. L. et al. Epithelial to mesenchymal plasticity and differential response to therapies in pancreatic ductal adenocarcinoma. Proc. Natl Acad. Sci. USA 116, 26835–26845 (2019).
Werba, G. et al. Single-cell RNA sequencing reveals the effects of chemotherapy on human pancreatic adenocarcinoma and its tumor microenvironment. Nat. Commun. 14, 797 (2023).
Nywening, T. M. et al. Phase 1b study targeting tumour associated macrophages with CCR2 inhibition plus FOLFIRINOX in locally advanced and borderline resectable pancreatic cancer. Lancet Oncol. 17, 651–662 (2016).
Rashid, N. U. et al. Purity independent subtyping of tumors (PurIST), a clinically robust, single-sample classifier for tumor subtyping in pancreatic cancer. Clin. Cancer Res. 26, 82–92 (2020).
Moffitt, R. A. et al. Virtual microdissection identifies distinct tumor- and stroma-specific subtypes of pancreatic ductal adenocarcinoma. Nat. Genet. 47, 1168–1178 (2015).
Nicolle, R. et al. Predictive genomic and transcriptomic analysis on endoscopic ultrasound-guided fine needle aspiration materials from primary pancreatic adenocarcinoma: a prospective multicentre study. eBioMedicine 109, 105373 (2024).
Fietkau, R. et al. Benefit of chemoradiotherapy versus chemotherapy after induction therapy for conversion of unresectable into resectable pancreatic cancer: the randomized CONKO-007 trial. J. Clin. Oncol. 43, 3266–3278 (2025).
Babiker, H. M. et al. Tumor treating fields with gemcitabine and Nab–paclitaxel for locally advanced pancreatic adenocarcinoma: randomized, open-label, pivotal phase III PANOVA-3 study. J. Clin. Oncol. 43, 2350–2360 (2025).
Villoslada-Blanco, P. et al. Development of a consensus molecular classifier for pancreatic ductal adenocarcinoma. Genome Med. 17, 142 (2025).
Collisson, E. A. et al. Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat. Med. 17, 500–503 (2011).
Bailey, P. et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature 531, 47–52 (2016).
Puleo, F. et al. Stratification of pancreatic ductal adenocarcinomas based on tumor and microenvironment features. Gastroenterology 155, 1999–2013.e3 (2018).
Knox, J. J. et al. Whole genome and transcriptome profiling in advanced pancreatic cancer patients on the COMPASS trial. Nat. Commun. 16, 5919 (2025).
Yoshihara, K. Inferring tumour purity and stromal and immune cell admixture from expression data. Nat. Commun. 4, 2612 (2013).
Nywening, T. M. et al. Targeting tumour-associated macrophages with CCR2 inhibition in combination with FOLFIRINOX in patients with borderline resectable and locally advanced pancreatic cancer: a single-centre, open-label, dose-finding, non-randomised, phase 1b trial. Lancet Oncol. 17, 651–652 (2016).
Acknowledgements
This work was mainly supported by Netris Pharma and the Fondation ARC. It was also supported by institutional grants from CNRS, University of Lyon, Centre Léon Bérard and from, INCA and ANR (ANR-10-LABX-0061, ANR-17-CONV-0002 and ANR-18-RHUS-0009). This work benefited from the support of the PUMA – Tissue and Cell Isolation Facility, thanks to M. Maitre and H. Doat of the NeuroCentre Magendie Inserm U1215. This study received financial support from the French government in the framework of the University of Bordeaux’s IdEx ‘Investments for the Future’ programme/GPR BRAIN_2030.
Author information
Authors and Affiliations
Contributions
G.R., P.A., N.W., J.G., A.T., A.L., J.-F.B., C.E., J.-B.B., P.P., M.R., A. Borowik, V.G., A.D., C.d.E., E. Girard, M.C., E. Georges, S.H., T.D., M.M. and O.B. designed the clinical trial and managed patient follow-up and clinical data analysis. B.D., H.H.-V., E.M., N.R., N.B., E. Georges, J.-Y.S., J.C. and A. Bernet performed and/or analysed translational studies. G.R., E. Georges, S.H. and P.M. wrote the manuscript. P.M secured funding for the overall study. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
G.R. declares honoraria as consultant and research funding from NETRIS Pharma. A. Bernet and P.M. are founders and shareholders of NETRIS Pharma. B.D., E. Georges and S.H. are employees of NETRIS Pharma. The NP137 patent is fully owned by NETRIS Pharma; none of the authors of this study are inventors on this patent. The other authors declare no competing interests.
Peer review
Peer review information
Nature thanks Michel Ducreux and Jean Luc Van Laethem for their contribution to the peer review of this work. Peer review reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Fig. 1 NP137 + mFolfirinox decreases circulation CA19.9.
a, Spaghetti plot showing the CA19.9 levels of patients at baseline and 6 months, with one line per patient and a log scale to better see the evolution of all patients’ levels. Non responders (red), responders (blue) and Not Available (Gray). b, Boxplot showing the distribution of the log of CA19.9 levels at baseline (n = 43) and 6 months (n = 32). Boxplots indicate the median (center line), interquartile range (box), and whiskers (1.5x IQR).
Extended Data Fig. 2 EMT modulation in pre/post tumoral specimens.
a, Analysis of tumor cell purity with the Estimate plugin. To verify the high tumor content, the LCM of tumoral material used in the following analysis (red circles) was compared to LCM of stromal contingent (green circles). The solid line represents the purity prediction model, flanked by dashed lines indicating the 95% confidence intervals of the original calibration model. b, Heat map illustrating unsupervised clustering of the 2 conditions based on differentially expressed genes between pre-treatment (n = 22) and post-treatment (n = 6) samples (FDR < 0.01, log2FC | > 1). c, Boxplot presenting genes regulated by NP137 + mFolfirinox between pre [(n = 22) and post treatment (n = 6)] tumor samples. Expression data (logCPM) presented as boxplots showing the median, quartiles, and 1.5x IQR (whiskers). Individual genes are displayed in separate facets. d, GSEA analysis performed on the repository Hallmark pathways on paired pre/post treatment samples (n = 4 patients). Dot plot (left) and ridge plot (right) are sorted based on the preranked gene set enrichment FDR-adjusted p-value. e, Comparison of the core EMT signature between pre and post treatment sample. Data were extracted from Cassier et al.4 and correspond to the analysis of a scRNAseq performed on pre/post tumor samples of endometrial cancer patients treated with NP137 as monotherapy. Only tumor cells were analyzed. P valued is based on a two-sided Wilcoxon rank-sum test. f, Comparison of the core EMT signature between pre and post treatment samples from the LAPNET study. Patients were segregated in SD vs PR groups. Boxplots indicate the median (center line), interquartile range (box), and whiskers (1.5x IQR). The underlying distribution is shown via violin plots. P valued is based on a two-sided Wilcoxon rank-sum test. Effectives are 17 for SD (13 pre and 4 post) and 10PR (8 pre and 2 post) .
Extended Data Fig. 3 Molecular Subgroup Analysis in LAPNET01.
a, Kaplan–Meier estimates of PFS in the LAPNET-01 cohort of 22 patients with available pre-treatment transcriptomic analysis, stratified by high and low score for Moffit’s signature based on the median. b, Kaplan–Meier estimates of OS in the LAPNET-01 cohort of 22 patients with available pre-treatment transcriptomic analysis, stratified by high and low score for Moffit’s signature based on the median. c, Kaplan–Meier estimates of PFS in the LAPNET-01 cohort of 22 patients with available pre-treatment transcriptomic analysis, stratified by high and low score for PurIST’s signature based on the median. d, Kaplan–Meier estimates of OS in the LAPNET-01 cohort of 22 patients with available pre-treatment transcriptomic analysis, stratified by high and low score for PurIST’s signature based on the median.
Extended Data Fig. 4 Neogenin level as a potential predictive marker of response.
a, Correlation analysis between Neogenin expression and progression-free survival (PFS) in the LAPNET-01 cohort of 21 SD or PR patients with available pre-treatment transcriptomic analysis. The line represents a fitted linear model with the shaded area (light pink) representing the 95% confidence interval of the regression estimate. The p-value is based on a two-sided Pearson test. b, Correlation analysis between Neogenin expression and progression-free survival (PFS) in 42 patients with locally advanced pancreatic cancer (LAPC) treated with mFOLFIRINOX, extracted from Nicolle et al. The line represents a fitted linear model with the shaded area (light green) representing the 95% confidence interval of the regression estimate. The p-value is based on a two-sided Pearson test. c, Kaplan–Meier estimates of overall survival (OS) in 42 patients with LAPC treated with mFOLFIRINOX extracted from Nicolle et al., stratified by high and low Neogenin expression based on the median. d, Kaplan–Meier estimates of progression-free survival (PFS) in the LAPNET-01 cohort of 22 with available pre-treatment transcriptomic analysis, stratified by high and low Neogenin expression based on the median. Patients with high Neo1 expression exhibit better PFS. e, Kaplan–Meier estimates of OS in the LAPNET-01 cohort of 22 patients with available pre-treatment transcriptomic analysis, stratified by high and low Neogenin expression based on the median. Patients with high Neo1 expression exhibit better OS. f, Correlation of mRNA and Protein levels in the LapNet-01 cohort. The p-value is based on a two sided Pearson test, p < 0.0001 and R2 = 0.696.
Extended Data Fig. 5 Netrin-1 drives neogenin-dependent pancreatic cancer cell migration.
a, Neogenin mRNA expression levels in Panc02 cells transfected with either control or Neo1-targeting siRNA, by RT-qPCR. Values were normalized with HPRT gene expression. Bars are mean values +/− S.E.M, n = 5, t-Test two-sided, *p < 0.05. b, Representative Western blot of neogenin and netrin-1 expression in Panc02 cells transfected with either control or Neo1-targeting siRNA. GAPDH was used as a loading control. Full membrane acquisitions are available in supplementary materials with two replicates. c, Relative wound density of siCtl and siNeo1 Panc02 cells 24 h post-scratch in a wound healing assay, pretreated with either control IgG NP001 or the anti-netrin-1 antibody NP137 for 24 h. Center lines are Mean values +/− S.E.M., n = 4, one-way ANOVA test p < 0.0001 and ad hoc multiple comparisons ***p = 0.0002). d, Relative wound density of Panc02 cells Ctl and treated with U0126/MEKi, 24 h post-scratch in a wound healing assay, pretreated with either control IgG NP001 or the anti-netrin-1 antibody NP137 for 24 h. Center lines are Mean values +/− S.E.M., n = 4, one-way ANOVA test p = 0.0056 and ad hoc multiple comparisons **p = 0.0074 NP001 vs NP137, * p = 0.0244 NP001 +/− MEKi or *p = 0.0168 NP001 vs NP137 + MEKi. e. Representative images of wound healing assay of Panc02 cells 24 h post-scratch among 5 to 8 technical replicates per conditions. Blue lines represent the initial wound, yellow areas represent the remaining would area at 24 h.
Supplementary information
Supplementary Information (download PDF )
Clinical protocol LAPNET01 (protocol approved by ANSM).
Supplementary Data 1 (download PDF )
LAPNET1- Final Statistical Analysis Report.
Supplementary Data 2 (download PDF )
LAPNET- Statistical Analysis Plan.
Supplementary Figure 1 (download EPS )
Representative raw gels of Extended Data 5.
Supplementary Table 1 (download XLSX )
Demographic and baseline characteristics of patients enrolled in the LAPNET-01 clinical trial. Continuous variables were summarized by their median and interquartile range, and qualitative variables by counts and percentages. Weight loss represents the change between the participants’ usual weight and their reported weight at inclusion, providing an indication of nutritional status prior study enrolment. BMI, body mass index; IQR, interquartile range.
Supplementary Table 2 (download XLSX )
Extended Safety.
Supplementary Table 3 (download XLSX )
Treatments received before progression in the ITT population (n = 43 patients).
Supplementary Table 4 (download XLSX )
Composition of the core EMT signature. Genes list of the core EMT signature extracted from Hallmark EMT signature.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Roth, G., Artru, P., Bouche, O. et al. Netrin1 blockade alleviates resistance to chemotherapy in pancreatic cancer. Nature (2026). https://doi.org/10.1038/s41586-026-10436-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41586-026-10436-4
