
Abstract
Clinical practice guidelines recommend defined weight loss goals for the prevention of type 2 diabetes (T2D) in those individuals with increased risk, such as prediabetes. However, achieving prediabetes remission, that is, reaching normal glucose regulation according to American Diabetes Association criteria, is more efficient in preventing T2D than solely reaching weight loss goals. Here we present a post hoc analysis of the large, multicenter, randomized, controlled Prediabetes Lifestyle Intervention Study (PLIS), demonstrating that prediabetes remission is achievable without weight loss or even weight gain, and that it also protects against incident T2D. The underlying mechanisms include improved insulin sensitivity, β-cell function and increments in β-cell-GLP-1 sensitivity. Weight gain was similar in those achieving prediabetes remission (responders) compared with nonresponders; however, adipose tissue was differentially redistributed in responders and nonresponders when compared against each other—while nonresponders increased visceral adipose tissue mass, responders increased adipose tissue in subcutaneous depots. The findings were reproduced in the US Diabetes Prevention Program. These data uncover essential pathways for prediabetes remission without weight loss and emphasize the need to include glycemic targets in current clinical practice guidelines to improve T2D prevention.
Similar content being viewed by others

Main
Globally, more than 460 million people live with type 2 diabetes (T2D) and many go through comorbidities such as neuropathy, chronic kidney disease or cardiovascular (CV) disease, making T2D one of the top 10 leading causes of death worldwide. Indeed, the increase in global mortality burden until 2050 is projected to be mostly due to neoplasms, T2D and kidney diseases1. Moreover, the current data suggest that T2D incidence will continue to rise, with most cases attributable to diet quality2. Additionally, the highest total number of affected people live in middle-income and low-income countries, where current guideline-based treatments are not as easily available as in high-income countries. Therefore, prevention must still be regarded as a major pillar in achieving the WHO’s global noncommunicable disease goals and in equitably reducing the major burden of T2D3. Prediabetes is the most prominent risk factor of T2D with a yearly progression rate of 5–10% and a lifetime progression risk of 74%4,5, and an independent risk factor for vascular diseases, cancer and neurodegenerative diseases4,6,7.
According to the American Diabetes Association (ADA), prediabetes is diagnosed when glucose regulation is impaired and/or HbA1c elevated while criteria of T2D are not met8,9. The U.S. Diabetes Prevention Program (DPP) Outcome Study (DPPOS) has demonstrated that reversal of impaired glucose regulation to normal at least once during a lifestyle intervention (LI) was effective in reducing the risk of T2D and microvascular disease10,11. In the Prediabetes Lifestyle Intervention Study (PLIS)12, we extended these findings by establishing the concept of prediabetes remission13,14. Accordingly, weight-loss-induced remission of prediabetes is reached, once the normal glucose regulation (NGR; that is, fasting glucose < 5.6 mmol l−1 (100 mg dl−1), 2 h glucose < 7.8 mmol l−1 (140 mg dl−1) and HbA1c < 39 mmol mol−1 (5.7%)) is re-established. Weight-loss-induced prediabetes remission (>5% of initial body weight) was explained by improved insulin sensitivity and reduced visceral adipose tissue (VAT) volume. At long-term follow-up, participants reaching weight-loss-induced prediabetes remission had a 73% reduced risk of developing T2D compared to those who only met the weight loss goal (but not prediabetes remission) and also had reduced signs of kidney and small vessel damage13, which may be due to reduced glycemic exposure over time as has previously been indicated10. A comparable concept to prediabetes remission has successfully been established in people with T2D in the DIRECT trial, where substantial weight loss led to a return to nondiabetic glucose levels in up to 85% of participants, although the risk of redeveloping T2D was high15,16. In general, part of weight loss targeted LIs is physical exercise, which has been linked with reduced inflammation17,18 and has been shown to improve insulin sensitivity independently of body weight change19. In individuals with T2D, it has also been demonstrated that physical exercise can improve glycemia without a substantial weight loss effect20. However, neither DIRECT nor DPP reported on the preventive outcomes of patients who did not reduce body weight but achieved remission.
Here, we provide evidence that non-weight-loss-induced remission of prediabetes protects from T2D development for up to 10 years after the LI started, and that it is characterized by increased subcutaneous adipose tissue (SCAT) compared to nonremission, where VAT increases. Moreover, we show that non-weight-loss-induced remission of prediabetes is mediated by an improvement in insulin sensitivity and insulin secretion.
Our data provide new support for the importance of implementing glycemic targets into current treatment guidelines to improve T2D prevention14, and show that the sole assessment of weight trajectories without body fat distribution is not adequately informative for the pursuit of treatment success.
Results
Study design and anthropometry
We analyzed data from the ongoing multicenter LI study PLIS that recruited individuals with prediabetes in study centers throughout Germany within the framework of the German Center for Diabetes Research (DZD e.V.), where participants received the intervention for 12 months and were followed up for up to 9 years with metabolic phenotyping including oral glucose tolerance tests (OGTTs) for glucose metabolism and whole-body magnetic resonance imaging (MRI) for assessment of body fat distribution before and after the intervention and during follow-up (see Methods for details). Of the 1,105 individuals originally included in PLIS, 234 (21.2%) did not lose or even gained weight during the year of the intervention. Of these, 51 returned to NGR, that is, were designated ‘responders’ (R; 21.8%), while 183 (78.2%) were ‘nonresponders’ (NR). Baseline characteristics for both groups are given in Extended Data Table 1. Overall, there were more women in both groups and R tended to have more women than NR (60.1% in NR versus 74.5% in R, P = 0.085). As has previously been reported for prediabetes remission11,13, R were younger (median = 54.4 ± 17.6 years) than NR (59.4 ± 15.5 years, P = 0.013), had lower fasting and 2 h glucose and slightly higher insulin sensitivity. Intervention intensity was not different between groups (Extended Data Table 1).
At first, we investigated whether weight trajectories during the 1-year intervention period were different between R and NR. However, BMI increased similarly in both groups (29.6 ± 2.1 kg m−2 to 30.6 ± 2.1 kg m−2 in R versus 30.5 ± 0.8 kg m−2 to 31.3 ± 0.9 kg m−2 in NR, P group over time = 0.24; Extended Data Fig. 1a). This was similar for body weight (84.0 ± 6.2 kg to 86.8 ± 6.5 kg in R versus 88.4 ± 2.9 kg to 90.6 ± 2.9 kg in NR, P group over time = 0.45), lean mass (56.2 ± 4.4 kg to 56.2 ± 4.7 kg in R versus 59.6 ± 2.7 kg to 59.5 ± 2.3 kg in NR, P group over time = 0.93; Extended Data Fig. 1b,c) and fat mass (30.7 ± 4.1 kg to 32.5 ± 4.5 kg in R versus 31.7 ± 2.0 kg to 32.5 ± 1.9 kg in NR, P group over time = 0.34; Extended Data Fig. 1d). Maximal aerobic capacity did not differ between groups (18 ± 2.2 ml min kg−1 to 17.6 ± 2.5 ml min kg−1 in R versus 18.5 ± 1.6 ml min kg−1 to 18.4 ± 1.9 ml min kg−1 in NR, P group over time = 0.65; Extended Data Fig. 1e). Additionally, adherence to dietary advice based on the evaluation of food diaries was not different between groups, similarly neither habitual physical activity (HPA) score nor daily distance walked (in a subgroup) or lean body mass differed between groups during the intervention and during follow-up, respectively (Extended Data Fig. 2).
Taken together, these data show that prediabetes remission without weight loss compared to nonremission was independent of weight trajectories, overall body composition and physical fitness.
Glucose and insulin metabolism
Next, we explored the underlying determinants of improved glucose regulation in R versus NR. Glucose concentrations during the OGTT were lower in R and per definition decreased over time in R only (Fig. 1a). Also, consecutive insulin concentrations during the OGTT were higher in NR than in R before, during and after the intervention, but increased in R between 30 and 60 min during the second half of the intervention (Fig. 1b).

a, Time course of glucose (R, n = 51; NR, n = 183) concentrations during the OGTT over the course of the LI. b, Insulin (R, n = 51; NR, n = 183) concentrations during the OGTT over the course of the LI. Means of raw values are depicted with error bars indicating 95% confidence intervals in all panels. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. The R (defined by NGR, that is, prediabetes remission, after 12 months of LI) group and the NR (that is, not reaching NGR) group are depicted in blue and orange, respectively. FDR-corrected group × time P values are 0.0008 for all comparisons. Dashed lines in a represent ADA criteria-based cutoff values for prediabetes for fasting glucose (5.6 mmol l−1) and 2 h OGTT glucose (7.8 mmol l−1). In b, the lower dashed line shows the insulin concentrations at 60 min during the OGTT at baseline and the upper dashed line shows the 60 min peak at 12 months to visualize the change in insulin peak concentrations during the intervention.
To better understand the increase of insulin concentrations in R, we calculated OGTT-derived indexes for insulin sensitivity, secretion and β-cell function. We found that throughout the LI, insulin sensitivity did not change in NR but increased in R. The oral glucose insulin sensitivity (OGIS) index increased from 336.45 ± 15.41 ml min−1 m−2 to 358.23 ± 18.88 ml min−1 m−2 in R, whereas it remained unchanged (299.42 ± 8.67 ml min−1 m−2 to 297.42 ± 9.09 ml min−1 m−2) in NR, P group over time: 0.0035 (Fig. 2a). Matsuda index of insulin sensitivity revealed the same development with a numeric increase from 8.94 ± 1.35 a.u. to 9.36 ± 1.47 a.u., P = 0.096 in R, but did not increase in NR (6.82 ± 0.55 a.u. to 6.39 ± 0.53 a.u. in NR, P group over time = 0.00041, Fig. 2b). An index of hepatic insulin resistance did not show differences between groups (Fig. 2c). Also, there was no indication of differences in muscle or adipose tissue insulin resistance (Fig. 2d,e). However, insulin secretion and β-cell function increased in R but not in NR. The C-peptide area under the curve (AUC)0–30 min/glucose AUC0–30 min, an index of insulin secretion, increased from 159.5 ± 17.13 pmol mmol−1 to 169.96 ± 19.3 pmol mmol−1 in R, but remained constant (157.89 ± 7.81 pmol mmol−1 to 161.81 ± 8.15 pmol mmol−1) in NR (P group over time = 0.043; Fig. 2f). The Adaptation Index, a marker of β-cell function, increased from 5.16 × 104 ± 3,833.80 a.u. to 5.78 × 104 ± 5,145.06 a.u. in R and remained unchanged (4.61 × 104 ± 2,192.89 a.u. to 4.74 × 104 ± 2,554.91 a.u.) in NR (P group over time = 0.025; Fig. 2g). An overview of the changes in the hyperbolic relationship between insulin sensitivity and insulin secretion for the two groups is given in Fig. 2h. The hyperbola shows that while R were able to increase insulin sensitivity and secretion at the same time, NR did not improve insulin sensitivity or insulin secretion. Change of hepatic insulin clearance was not different between groups (3.91 ± 0.36 a.u to 3.68 ± 0.4 a.u in R versus 3.39 ± 0.17 a.u to 3.31 ± 0.16 a.u in NR, P group over time = 0.49; Fig. 2i) and, thus, cannot explain the increase in insulin concentrations observed in R. With the increase in insulin secretion and β-cell function alongside improved insulin sensitivity, remission mechanisms without weight loss differ from weight-loss-associated prediabetes remission, where the increase in insulin secretion has not been observed previously13.

a, OGIS (R, n = 51; NR, n = 183). b, Matsuda insulin sensitivity index (R, n = 51; NR, n = 183). c, Hepatic insulin resistance (R, n = 51; NR, n = 183). d, Muscle insulin resistance (R, n = 51; NR, n = 183). e, Adipose tissue insulin resistance (R, n = 21; NR, n = 109). f, Insulin secretion (C-peptide/glucose AUC0–30 min—R, n = 51; NR, n = 183). g, Adaptation index (R, n = 51; NR, n = 183). h, The hyperbolic relationship between insulin sensitivity (OGIS) and secretion (C-peptide/glucose AUC0–30 min—R, n = 51; NR, n = 183) all derived from OGTT at baseline and 12 months. i, Hepatic insulin clearance (R, n = 51; NR, n = 183). The R (defined by NGR, that is, prediabetes remission, after 12 months of LI) group and the NR (that is, not reaching NGR) group are depicted in blue and orange, respectively. Means of raw values are depicted with error bars indicating 95% confidence intervals in a–g. In h and i, the base of the arrows depicts medians at baseline and the respective tip after 1 year of LI. Error bars depict s.e.m. P values directly above the x axes in a–g and i indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the R and the NR group as post hoc corrected comparisons derived from the respective mixed effects models. FDR-corrected group × time P = 0.013 (a), P = 0.002 (b), P = 0.89 (c), P = 0.47 (d), P = 0.47 (e), P = 0.10 (f), P = 0.081 (g) and P = 0.62 (i).
Body fat distribution
Because insulin sensitivity and secretion are linked with ectopic adipose tissue deposition21,22,23, we then determined lipid accumulation in SCAT, VAT and ectopic lipid depots based on the MRI and 1H-spectroscopy data. Intrahepatic lipid content (IHL) was slightly higher in NR versus R (Extended Data Table 1) but remained constant in both groups during the LI (5.08 ± 1.71% to 5.9 ± 1.74% in R versus 7.65 ± 1.14% to 8.13 ± 1.18% in NR, P group over time = 0.74; Fig. 3a), suggesting no critical contribution of changes in IHL for nonweight-loss remission. However, while VAT did not increase in R despite weight gain, it increased along with weight gain in NR (4.31 ± 0.69 l to 4.24 ± 0.69 l in R versus 4.99 ± 0.32 l to 5.41 ± 0.36 l in NR, P group over time = 0.031; Fig. 3b). In contrast, SCAT increased more in R versus NR (14.41 ± 2.39 l to 15.7 ± 2.06 l in R versus 14.97 ± 1.06 l to 14.66 ± 0.98 l in NR, P group over time = 0.035) showing that with weight gain, R predominantly stored additional energy in SCAT but NR in VAT (Fig. 3c). This is reflected in a substantial increase in SCAT/VAT ratio in R, whereas the ratio tended to decrease in NR (4.01 ± 0.67 to 4.94 ± 0.93 in R versus 3.42 ± 0.25 to 3.14 ± 0.26 in NR, P group over time < 0.0001; Fig. 3d). Change in intramuscular fat was not different between groups (5.85 ± 1.24% to 6.15 ± 1.49% in R versus 6.4 ± 1.45% to 6.76 ± 1.49% in NR, P group over time = 0.83; Fig. 3e). These data highlight that lipid deposition during weight gain is most likely a crucial factor for improvements in glucose regulation during non-weight-loss prediabetes remission.

a, Trajectories of hepatic lipid content as assessed with 1H-MRS (R, n = 51; NR, n = 183). b, VAT as assessed with MRI (R, n = 51; NR, n = 183). c, SCAT as assessed with MRI (R, n = 51; NR, n = 183). d, SCAT/VAT ratio (R, n = 51; NR, n = 183). e, Muscle fat content as assessed with MRI (R, n = 16; NR, n = 27). f, Group comparison of the adjusted PRS for VAT volume (R, n = 32; NR, n = 164). In a–e, means of raw values are depicted with error bars indicating 95% confidence intervals. In f, box plots are centered on medians, boxes extend to 25th and 75th percentiles and whiskers extend to 1.5× IQR (top and bottom). P values directly above the x axes in a–e indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the R and the NR group as post hoc corrected comparisons derived from the respective mixed effects models. The R (defined by NGR, that is, prediabetes remission, after 12 months of LI) group and the NR (that is, not reaching NGR) group are depicted in blue and orange, respectively. FDR-corrected group × time P = 0.83 (a), P = 0.090 (b), P = 0.092 (c), P = 0.0008 (d) and P = 0.89 (e). IQR, interquartile range.
To further investigate whether the genetic background is a key driver of ectopic lipid deposition during weight gain, we calculated a polygenic risk score (PRS) derived from a subset of single-nucleotide polymorphisms (SNPs; Methods) that have been described to be associated with VAT24. However, there were no differences in the PRS between R and NR with or without adjustments for covariates (Fig. 3f).
Similar to previously published data on weight-loss-induced prediabetes remission, there was no association between the change in IHL and the proportion of remission (Fig. 4a,b). However, lower VAT increase or even reductions in VAT were linked with higher remission success (P = 0.024; Fig. 4c,d). According to the changes in SCAT and VAT, a higher SCAT/VAT ratio after the LI was associated with higher frequency of remission, again suggesting that the distribution of adipose tissue gained may determine prediabetes remission (P < 0.0001; Fig. 4e). Finally, there was a trend toward higher remission rates with weight gain (Fig. 4f).

a, Stratification of R (defined by NGR, that is, prediabetes remission, after 12 months of LI, n = 51; blue) and NR (that is, not reaching NGR, n = 183) by postintervention hepatic lipid content as assessed with 1H-MRS. b, Change of hepatic lipid content during LI. c, Postintervention VAT volume as assessed with MRI. d, Change of VAT volume during LI. e, SCAT/VAT ratio. f, Change of body weight during LI. Top numbers inside the bars indicate stratum size (n). Large bottom numbers indicate BMI (a,c) or percent body weight change (b,d,e). Small bottom numbers indicate 95% CI, respectively.
Inflammatory markers and adipokines
VAT is associated with increased low-grade inflammation and weight-loss-associated prediabetes remission13. Thus, we measured biomarkers of inflammation suggested to contribute to insulin resistance. However, there were no substantial differences in individual trajectories of inflammatory markers between R and NR (Supplementary Tables 1 and 2). Thus, low-grade inflammation, at least at the circulation level, may not explain improved insulin sensitivity during prediabetes remission.
Because hormonal factors derived from adipose tissue are also linked with insulin sensitivity, we measured the adipokines leptin and adiponectin. Leptin levels were not different between groups and did not develop differently (37.25 ± 11.81 ng ml−1 to 43.63 ± 11.68 ng ml−1 in R versus 40.68 ± 6.24 ng ml−1 to 47.26 ± 6.49 ng ml−1 in NR). Adiponectin levels, however, were not different at baseline (3096.48 ± 535.75 ng ml−1 in R, 2412.30 ± 207.49 ng ml−1 in NR, P = 0.094), but were substantially higher after the intervention in R versus NR (3371.57 ± 596.55 ng ml−1 in R, 2337.20 ± 217.24 ng ml−1 in NR, P = 0.0040, P group over time = 0.088; Extended Data Fig. 2), suggesting that increases in SCAT may chaperone improved insulin sensitivity by increased adiponectin secretion, at least in part.
Very-low-density lipoprotein (VLDL) palmitate, incretins and glucagon
To further understand the improvement in insulin secretion and β-cell function in R, we assessed lipid content within triglyceride-containing VLDL particles, because a reduction in VLDL1 palmitate has been shown to be associated with improved β-cell secretory capacity during the remission of T2D25. Despite higher levels in total and specific lipid species-bound palmitate in NR as well as triglyceride levels, there was no difference in the trajectories during LI between R and NR (Extended Data Fig. 3a–l), suggesting that hepatic palmitate export may not have major impact on the insulin secretion phenotype during prediabetes remission.
We then assessed concentrations of glucagon-like peptide 1 (GLP-1), gastric inhibitory polypeptide (GIP) and glucagon to investigate whether incretin responses during the OGTT or sensitivity (see below) may explain improved insulin secretion in R. As expected, in both groups GLP-1 concentrations increased between 0 and 30 min, and then decreased at 120 min (Fig. 5a). While there was no substantial difference in the trajectories over time between groups (before, P = 0.13; after, P = 0.14), the GLP-1AUC substantially increased in NR (who maintained that their glucose levels in the prediabetic range or advanced to overt T2D) but remained stable in R despite reduction of glucose levels to normal (P = 0.78; Fig. 5a).

Incretin hormone levels during the OGTT at baseline and 12 months, n = 32 R versus 131 NR. a, GLP-1. b, GIP. c, Glucagon. Means of raw values are depicted with error bars indicating 95% confidence intervals. P values directly above the x axes indicate change in R (defined by NGR, that i,s prediabetes remission, after 12 months of LI) versus NR (that is, not reaching NGR) over time (that is, interaction term of group and time) derived from mixed effects models. Indicators above the time points indicate between-group difference at the respective time point derived from post hoc comparisons of the respective mixed effects models. ***P < 0.0001; FDR-corrected group × time P values: baseline—P = 0.29, 12 months—P = 0.29, AUC—P = 0.0008 (all to a); baseline—P = 0.63, 12 months—P = 0.38, AUC—P = 0.45 (all to b); baseline—P = 0.38, 12 months—P = 0.0079, AUC—P = 0.0012 (all to c). NS, nonsignificant.
GIP followed similar trajectories during the OGTT but remained elevated at 120 min in both groups (Fig. 5b). Neither group trajectories during the OGTT before or after nor GIPAUC differed between R and NR, rendering GIP unlikely to be involved in improved β-cell function during nonweight-loss prediabetes remission (Fig. 5b).
However, glucagon was lower in R and remained unchanged during the LI, whereas in NR glucagon showed an additional increase after the intervention (Fig. 5c). Interestingly, reduction in glucagon concentrations between 0 and 30 min during the OGTT remained stable in NR, but increased substantially in R (Fig. 5c), implying improved glucagonostatic and insulinotropic (considering improved insulin secretion) effects of GLP-1. Therefore, we then calculated the insulin secretion rate based on a previously published algorithm26,27,28 and plotted it against GLP-1 secretion as a measure of β-cell-GLP-1 sensitivity. Indeed, these calculations display that β-cell-GLP-1 sensitivity exhibited marked improvements in R, but not in NR (insulin secretion rate AUC—3,749 ± 401.1 to 4360 ± 382.5 in R and 4,381 ± 164.2 to 4,326 ± 170.1 in NR; GLP-1 AUC—122.1 ± 10.3 to 115.4 ± 13.3 in R and 142.5 ± 5.12 to 152.2 ± 5.96 in NR; P group over time = 0.0050; Extended Data Fig. 4).
Protection from T2D by nonweight-loss-induced prediabetes remission
Because of the recent data showing that prediabetes remission with weight loss reduces the risk for future T2D development13, we here investigated if remission of prediabetes despite the absence of weight loss or even with weight gain is also protective from future T2D development. Indeed, more NR than R developed T2D leading to a relative risk (RR) reduction of 71% in R over the period of up to 10 years (RR = 0.29, 95% CI = 0.09–0.91, P = 0.02; Fig. 6a,b) and thus prediabetes remission without weight loss was comparably protective for T2D development as prediabetes remission with weight loss (73%)13.

a, Kaplan–Meier curve representing proportion of individuals without T2D over time. Faded colors indicate s.d. from the estimand. P value is derived from log-rank tests. b, Sankey plot of glycemic categories (that is, T2D, prediabetes and NGR) over time. P value is derived from two-sided Fisher’s exact test.
Replication of results in the DPP
To exclude any potential effect that may be specific to our cohort and to enhance the generalizability of the results, we validated our findings in repository data from DPP. We also identified 494 individuals who did not lose or even gain body weight after 12 months of the intervention. Baseline characteristics are given in Supplementary Table 3. Similar to PLIS, R and NR increased BMI comparably, and NR increased VAT while R did not (Extended Data Fig. 5a–c). Additionally, R showed improved insulin sensitivity as well as insulin secretion (Extended Data Fig. 6a–c), even after adjusting for insulin sensitivity. Finally, individuals with prediabetes remission in DPP at 1 year without weight loss also had an RR reduction for future T2D of 73% (RR = 0.27, 95% CI: 0.11, 0.66, P < 0.0001) during a median follow-up time of 4.11 (IQR: 1.44, 13.48) years. These data reproduce the findings that prediabetes remission without weight loss is characterized by improved insulin sensitivity as well as improved insulin secretion and that excess lipid deposition into VAT may preclude persons from nonweight-loss prediabetes remission.
Validation using different cutoff values for prediabetes remission
Moreover, recent data indicate that the 1 h glucose OGTT value may better predict the development of T2D than the 2 h OGTT value29. We, therefore, performed the same analysis by using the proposed 1 h cutoff of 155 mg dl−1 to identify participants as having prediabetes or NGR, but this change in criteria for prediabetes did not change our findings regarding glucose and insulin metabolism during prediabetes remission (Extended Data Fig. 7).
Discussion
Our data show that remission of prediabetes without weight loss is a genuine and reproducible response to an LI in a substantial proportion of participants (up to 22%) and that the response is highly effective in preventing T2D. Individuals going into remission without losing body weight are characterized by increased SCAT/VAT ratio, indicating that the site of fat deposition during an LI determines the probability of prediabetes remission. Elegant studies have shown that physical exercise reduces glycemia with no or only marginal effects on body weight20,30. The studies in refs. 31,32 have shown that exercise without a weight loss effect can specifically reduce VAT. Additionally, diet composition has a role in VAT accumulation—diets high in polyunsaturated fatty acids have been shown to protect against VAT gain compared to those rich in saturated fats, even during overfeeding and weight gain33. Thus, physical exercise and dietary habits may have contributed to lower glycemia and to the observed SCAT and VAT distribution phenotype.
Moreover, non-weight-loss-associated prediabetes remission was characterized by a combination of higher insulin sensitivity and improved insulin secretion, which contrasts this response from weight-loss-induced prediabetes remission in PLIS and DPP where remission was characterized by improved insulin sensitivity but not secretion and T2D remission in DIRECT, which was accompanied by improved β-cell function but not insulin sensitivity13,21,34. Notably, prediabetes remission without weight loss was protective from T2D development with an RR reduction of >70%, and thus to a comparable degree as weight-loss-induced prediabetes remission in the previous study13. Taken together, these data show that distinct physiological mechanisms underlie non-weight-loss-induced remission of prediabetes and that it is essential to differentiate between weight-loss and non-weight-loss strata, when investigating the mechanisms that can mediate prediabetes remission. Moreover, our data suggest that weight loss, as recommended in current guidelines, should be complemented by remission to NGR to prevent T2D in those people with prediabetes. This is in line with recent efforts delineating the clinical heterogeneity of obesity in projection for cardiometabolic diseases, specifically when cardiometabolic risk is discordant with the risk that is to be expected when obesity is classically defined solely by the BMI35. Furthermore, new statements and definitions of expert commissions for the diagnosis and management of obesity highlight the importance of body fat distribution and function beyond adiposity and underscore the clinical manifestation of organ dysfunction for the diagnosis of clinical obesity36,37.
While body weight trajectories were similar between groups, fat accumulation in SCAT was mainly observed in R and accumulation in VAT was observed in NR. The details in ref. 38 showed that large amounts of SCAT in combination with little visceral adiposity are associated with high insulin sensitivity during a hyperinsulinemic–euglycemic clamp. Exercise can favorably influence SCAT composition, even without weight loss39, and SCAT of regularly exercising individuals is more expandable than that of sedentary people with obesity40. The importance of exercise for improving insulin sensitivity has previously been demonstrated41; however, lean body mass and VO2 max, a marker of maximum aerobic capacity, were not different between R and NR. Nonetheless, we cannot rule out that subtle differences in physical exercise (volume) may have impacted insulin sensitivity. Although we did not observe a difference in the PRS, the genetic basis of unfavorable body fat distribution and T2D risk has previously been reported42,43,44. Interestingly, thiazolidinediones (TZDs), a class of oral glucose-lowering medications that activate the transcription factor, peroxisome proliferator-activated receptor γ, led to a redistribution of fat mass from VAT to SCAT depots. TZDs act as insulin sensitizers at least in part by this mechanism45,46. They have also been shown to increase body weight and to improve insulin sensitivity and β-cell function, similar to our observation with nonweight-loss prediabetes remission45,47.
This trend toward a favorable adipose tissue composition tracks closely with systemic adiponectin concentrations. Adiponectin is released by adipose tissue and is associated with increased systemic insulin sensitivity48. This finding is in line with recent findings of a gradual decrease of adiponectin levels from metabolically healthy lean to metabolically healthy obese to metabolically unhealthy obese persons49. Also, in the data presented here, adiponectin levels were higher in R after the intervention, which may contribute to their increased insulin sensitivity.
In R, but not NR, insulin secretion and β-cell function increased during LI. Palmitate, partly a product of hepatic de novo lipogenesis, has a particularly detrimental role in reducing β-cell function, most likely by inducing β-cell dedifferentiation50. Hepatic palmitate secretion has been shown to be modifiable by LI and reduced VLDL1 palmitate export from the liver has been shown to be linked with T2D remission in the DIRECT trial as well as remission maintenance after weight-loss-dependent remission25. In our study, in the setting of non-weight-loss prediabetes remission, VLDL1 palmitate export did not change between R and NR, implying that hepatic VLDL1 palmitate export may not be responsible for the lack of increase in β-cell function in the NR. However, we did not assess VLDL-production rates, previously demonstrated to be important for T2D remission25.
We then assessed the incretin system to explain the improvement in insulin secretion observed in R, but not in NR. Both GLP-1 and GIP enhance glucose-dependent insulin secretion51. GLP-1 secretion after glucose ingestion is only minimally reduced in impaired glucose tolerance (IGT) as well as in T2D52,53. Exogenous application of GLP-1 in pharmacologically relevant doses largely maintains its effectiveness in IGT as well as in T2D54. GIP levels after glucose ingestion are in the normal range in IGT and may be elevated in T2D53,55. However, its effectiveness in augmenting insulin secretion is reduced56. In our cohort, GLP-1 and GIP time courses during OGTT were not different between groups. GLP-1AUC remained stable in R despite reduced glucose levels and increased insulin levels (Fig. 2). This may reflect improved GLP-1 sensitivity in R, potentially contributing to improved β-cell function by its improved insulinotropic effect that has been shown to be more pronounced during normoglycemic conditions57. Indeed, an index of β-cell-GLP-1 sensitivity showed increased sensitivity in R, but not in NR. Because GLP-1 has a glucagonostatic effect58, improved GLP-1 sensitivity may be supported by the finding that R showed improved glucagon suppression during the OGTT. However, we cannot exclude that this could also be a consequence of the improvements in glucose regulation restoring the glucosuppressive effect on glucagon that may also be influenced by diet59.
Prediabetes remission without weight loss reduced the risk of subsequent T2D by 71% in our study. Previous studies of people with weight-loss-induced prediabetes remission showed similar risk reductions (73%)13,60, which is comparable to T2D risk reduction induced by pharmacological interventions61. In a post hoc analysis from the PROactive trial, weight gain with pioglitazone, a TZD, which leads to weight gain with a redistribution from VAT to SCAT and improvements in insulin sensitivity62,63, was associated with improved CV outcomes (excluding heart failure)64. Interestingly, recent data from our group show that prediabetes remission, in contrast to multimodal LIs targeting mainly weight loss, is also associated with reduced CV outcomes65,66.
Together, these data indicate that there is a weight-independent component of the glycemic status, which is related to body fat distribution. Indeed, individuals reaching both prediabetes remission and the guideline-recommended weight loss target of 7% are 76% less likely to develop T2D8, compared to the group that only met the weight loss target60. These data highlight the importance of incorporating glycemic targets into practice guidelines in addition to weight loss targets. Remission of prediabetes is the most effective way to prevent future T2D cases, and our current data indicate that this is partially independent of weight loss. In fact, sustainable weight loss is rarely achievable with >90% of weight loss recidivism and the probability of obtaining normal body weight is very low with less than 1 per 1,000 for men and less than 1 per 600 for women in individuals with severe obesity67,68. Therefore, from a clinical perspective, primary treatment goals should focus on achieving metabolic health rather than weight loss alone. Bringing prediabetic hyperglycemia back to normoglycemia seems to be an important contribution and indicator for metabolic health69.
This study is limited by the surrogate parameters derived from the OGTT for estimation of insulin sensitivity and secretion/β-cell function. Additionally, we cannot rule out confounders that were not assessed, such as genetic predisposition (beyond the investigated SNPs) and environmental factors. This study is additionally limited by the lack of a priori powering due to the post hoc nature of this analysis. To strengthen the validity of the data, we have therefore included data from the DPPOS cohort that replicate and support our current findings and interpretations. Additionally, the post hoc group stratification may lead to residual confounding effects, that is, the stratification into remission and nonremission leads to baseline differences, for example, in glucose levels, as has also been observed in studies investigating T2D remission mechanisms70 and in previous analyses from DPPOS10,11, which may affect the likelihood of remission at the individual level. Nonetheless, we show that for individuals who do achieve remission, the risk of future T2D development is substantially reduced—even in the absence of weight loss. This finding underscores the importance of incorporating remission as a core element of modern T2D prevention strategies, regardless of baseline. To minimize confounding of our results by baseline misclassification, we included fasting as well as postchallenge glucose and HbA1c into our definition of remission, whereby test–retest reliability has been shown to be up to 98.6%71. While spontaneous remission from prediabetes to normoglycemia might be observable even without LI72, our findings are not likely to be influenced by an erroneous classification.
We conclude that the protective effect of LI in individuals with prediabetes is not solely dependent on weight loss, as none of the participants included in the present analysis lost weight. Non-weight-loss prediabetes remission is characterized by a ‘TZD-like’ body fat distribution. Current guideline recommendations involve multimodal LI with a focus on weight loss targets of 5–10%. In light of the current data, we recommend achieving metabolic health by incorporating glycemic targets to reach NGR (prediabetes remission) in addition to weight loss, thereby optimizing T2D risk reduction through a precision prevention approach. Specifically, LI needs to be tailored to the goal of prediabetes remission73.
Methods
Study design and PLIS cohort
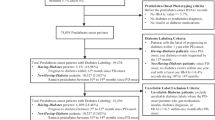
Participants of the risk-stratified, randomized, controlled and multicenter PLIS were recruited between 1 March 2012 and 31 August 2016 to assess potential superiority of an intensified LI compared to conventional DPP-based LI in improving glucose tolerance in people with prediabetes at high risk for T2D development. Sex was determined through self-report. People with prediabetes (impaired fasting glucose, IGT or both according to criteria from the ADA) between the ages of 18 and 75 years were included8. Participants with high IHL in addition to either high insulin resistance or low insulin secretion were stratified as high risk. After stratification, randomization of high-risk participants to receive either intensified LI or conventional LI and of low-risk participants to receive either conventional LI or a control intervention was performed. For this analysis, individuals from PLIS who did not experience weight loss over the 12-month period of those of the intensified LI, the conventional LI or the control intervention were included. Participants were classified as either R or NR. R were defined by return to normal fasting plasma glucose (that is, <5.6 mmol l−1), normal glucose tolerance (that is, 2 h postload glucose <7.8 mmol l−1) and HbA1c less than 39 mmol mol−1 after 12 months of all three interventions. NR were defined by fasting plasma glucose, 2 h glucose or HbA1c higher than these thresholds after 12 months of all three interventions. Glucose regulation was assessed in the morning at 8 a.m. during an overnight fast through OGTT with blood sampling at 0, 30, 60, 90 and 120 min using a 75 g glucose load (Accu-Check Dextro O.G.T.; Roche). Glucose concentrations were assessed using the glucose oxidase method in certified laboratories at each clinical study site. All insulin and C-peptide measurements were done at the Tübingen study site on an ADVIA Centaur XP system (Siemens Healthineers). Clinical chemistry parameters, including HbA1c, were assessed at the local routine diagnostic laboratories of the participating centers, and all of these were certified by the German accreditation council (DAkkS).
Volunteers participated in this study for a mean of 5.2 ± 2.8 years (max = 9.9 years). Adherence to the dietary intervention was assessed by evaluation of food diaries through the study counselors during the counseling sessions, where food diaries of 4 consecutive days were evaluated. The dietary goals were reduction of fat intake to <30% of total energy intake, reduction of saturated fat intake to <10% of total energy intake and increase of fiber intake to >15 g per 1,000 kcal total energy intake. Markers of physical activity and fitness were assessed by the VO2 max during ergometry, quantification of lean body mass and the HPA. The VO2 max was assessed as the maximal oxygen uptake during incremental physical exertion on an ergometer, lean body mass was estimated through bioelectric impedance analysis and the HPA based on the self-report that addressed the following main components: physical activity during work, physical activity during leisure time and sports during leisure time74. In a small subgroup of individuals, step counts were extracted to document daily distance walked (R/NR, n = 6/17). Further details of the intervention are provided elsewhere12. Of these measures, lean body mass and the HPA were continuously assessed. Follow-up is ongoing. Written informed consent was provided by each participant at inclusion. The study protocol is available online (https://www.dzdev.de/fileadmin/DZD/PDF/Papers/Forschung_KlinStud_Ethik_Studienprotokoll_PLIS_1.4.pdf) and approved by the ethics committee of the University Clinic of Tübingen (Tübingen, 55/2012; ClinicalTrials.gov registration: NCT01947595). Further details have been published previously12. Financial compensation for participants was granted exceptionally upon request, only if participants lived far away from the study center.
DPP study validation cohort
Repository data from the U.S. DPP study were analyzed to verify results from PLIS in a different population75,76. Participants were recruited from 23 clinical study centers in the United States between 31 July 1996 and 18 May 1999, and randomized to either LI or metformin or placebo groups. For the present analysis, data from LI and placebo group participants were used, who did not lose body weight during the first 12 months and had complete data on measurements of BMI, fasting and 30-min insulin, and fasting, 30 min and 120-min glucose during an OGTT.
Ethics approval for the study was provided by the institutional review board of each participating clinical center. Written informed consent was obtained from all DPP participants. The DPP study protocol is available online at https://repository.niddk.nih.gov/study/38.
Outcomes
This is a post hoc analysis of a prespecified endpoint in PLIS. Main outcomes are indexes of insulin secretion and sensitivity and distribution of body fat as main determinants of response or nonresponse to an LI.
The specifics of sampling and processing have been published elsewhere12. All measurements were taken from distinct participants. The following OGTT-based indexes for insulin sensitivity were calculated: OGIS index77, insulin sensitivity index78, the adipose tissue insulin resistance index79, muscle insulin sensitivity index80 and hepatic insulin resistance index81. To evaluate insulin secretion, we used C-peptide AUC divided by glucose AUC during the first 30 min of the OGTT82. The Adaptation Index was calculated as (AUCcpep0–30 divided by AUCgluc0–30) × OGIS to provide an integrated measure for insulin secretion adapted to underlying insulin resistance83. AUCcpep0–120 divided by AUCins0–120 was calculated as a marker of hepatic insulin clearance84.
Insulin secretion rate was calculated by fitting C-peptide concentrations at each time point during the OGTT to an established model of C-peptide deconvolution26,27,28. An incremental area under the first 30 min of the curve resulting from this modeling was calculated using the trapezoidal rule85. An incremental AUC was obtained from GLP-1 measurements during the OGTT in a similar fashion. These values were plotted against each other to depict β-cell-GLP-1 sensitivity, as previously described86. Insulin secretion and sensitivity were assessed from OGTT-based indexes in DPP in a similar fashion. Details have been previously published75,76.
The MRI was performed to measure muscle fat, subcutaneous and visceral fat compartments in PLIS. The applied methods are described in detail elsewhere12,87. VAT volume was determined from T1-weighted fast spin echo images that were assessed with a slice thickness of 10 mm (ref. 88). Segmentation of VAT was done between hip and thoracic diaphragm using an automatic fuzzy c-means algorithm and orthonormal snakes89. IHL was quantified in PLIS only. Localized proton magnetic resonance spectroscopy (1HMRS) applying a singlevoxel stimulated echo acquisition mode localization technique with short echo time in the posterior part of segment VII was applied for IHL assessment. The ratio of signal integrals of fat (methylene + methyl signal) and total signal (water + fat) was used to determine IHL content, which is expressed in percent. In one center, 1H-MRS was not available and IHL content was determined by a chemical-shift selective imaging technique that generates fat and water selective images as described elsewhere90. From these, manually determined regions of interest in liver segment 7 performed in fat and water selective images, respectively, were used for IHL-content assessment. To ensure comparability with MRS-guided assessments, IHL content was calculated by fat/(water + fat) × 100, including corrections for relaxation effects. Both techniques have been shown to yield comparable assessments of IHL content91. More details have been described previously92.
In DPP, VAT measurements were obtained by lumbar spine CT scans at L2, L3, L4 and L5. IHL and SCAT were not quantified in DPP. Only in PLIS, fat-selective MRI sequences were used to measure intramuscular fat fraction of musculus erector spinae and musculus spinalis thoracis. A region of interest avoiding macroscopic fat septae was manually drawn at the Th10/Th11 intervertebral level in a single axial slice90,92. Close proximity SCAT was used for reference (that is, 100%) and fat fractions were calculated12,87.
Assessment of VLDL palmitate
VLDL were isolated from plasma by ultracentrifugation applying an NaCl density gradient (ρ = 1.006 g ml−1) at 541,000g for 60 min at 4 °C on an Optima Max-XP ultracentrifuge (Beckman). Subsequently, 60 µl of the VLDL-containing fraction were used for lipid extraction and shotgun analysis as previously described93,94. Lipid extracts were resuspended in IPA/MeOH/CHCl3 (4:2:1; vol/vol/vol) with 7.5 mM ammonium acetate and then infused through the TriVersa NanoMate ion source (Advion Biosciences) into an Exploris 240 (Thermo Fisher Scientific) mass spectrometer. All spectra were imported by LipidXplorer (1.2.8.1) into a MasterScan database. Lipid identification was carried out as described95.
Inflammatory markers, adipokines, incretins and glucagon
Multianalyte profiling on the Luminex-100 system (Bio-Rad Laboratories), with a combination of Bio-Plex Pro Human Immunotherapy Panel 20-Plex, Bio-Plex Pro Huma Inflammation Panel, Bio-Plex Pro Human Cytokine Panel and the 2-Plex Panel for vascular cell adhesion molecule 1 and intercellular adhesion molecule 1, was used to assess concentrations of circulating inflammatory markers in serum. Bio-Plex Multiplex Immunoassays (Bio-Rad Laboratories) are based on the xMAP Technology licensed from Luminex; all measurements were conducted according to the manufacturer’s protocols. A detailed description of the methods is given elsewhere96. Serum concentrations of leptin (11-LEPHU-E01; Alpco) and high molecular weight adiponectin (80-ADPHU-E01; ALPCO) were determined using ELISA, following the manufacturer’s instructions.
Plasma levels of total GIP, total GLP-1 and glucagon were measured as previously described using validated immunoassays97.
Calculation of a PRS
Individuals from PLIS were genotyped onto two different versions of the Illumina Global Screening Array chip (280 on GSA-MD-24v1 and 549 on GSA-MD-24v2). A previously described set of 205 SNPs for predicted VAT, including only genome-wide substantial variants described in ref. 24 were selected and subsequently restricted to 186 SNPs. Quality control was performed on all participants using the PLINK 1.9 software. SNPs exclusion criteria included missingness threshold of >5%, minor allele frequency <1% and Hardy–Weinberg equilibrium with P < 0.05. The summary statistics were downloaded from the NHGRI–EBI GWAS on 8 October 2024 for study GCST008744 (refs. 24,98).
Statistical analysis
Linear mixed effects models with group (that is, R and NR), time point and the interaction group × time point as model terms adjusted for age, sex, BMI, risk stratification and intervention intensity as fixed effects and each individual as random effect were fitted to analyze longitudinal data. Additionally, the model evaluating insulin secretion included insulin sensitivity as fixed effect. All group × time P values were corrected for multiplicity using the Benjamini–Hochberg procedure. To avoid overreliance on significance testing and dichotomization, we report β coefficients for all models, including 95% confidence intervals in Extended Data Fig. 9. Diagnostic plots were plotted for each model to ensure normal distribution of residuals by visual inspection. For group-wise, cross-sectional comparisons, two-sided Wilcoxon rank-sum tests were performed. Resulting P values were also corrected for multiplicity of comparisons (Benjamini–Hochberg). T2D incidence up to almost 9 years after intervention end was compared through risk ratios and Fisher’s exact test using the epitools package, version 0.5-10.1. A Kaplan–Meier curve with log-rank test is also reported.
Statistical analyses were performed using RStudio (version 2024.12.0 + 467) with R (version 4.4.1). In the PLIS dataset, missing values for liver, subcutaneous, and visceral fat were imputed using the mouse package (version 3.16.0). In the DPP dataset, no imputation was performed.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The datasets from this study are not publicly accessible due to national data protection regulations and ethical restrictions designed to protect participant privacy. They can be requested after publication by contacting the corresponding author. Each request will be reviewed by the PLIS data steering committee, and approved access will require a formal data use agreement. The PLIS data steering committee will respond to requests within 3 months.
Data from the DPP referenced in this study can be obtained through the U.S. NIDDK Central Repository (https://repository.niddk.nih.gov/)99. These datasets include demographic details, anthropometric and laboratory assessments, imaging data and time-to-diabetes diagnosis.
Code availability
No custom code was generated for this study. Previously published packages and functions have been referenced.
References
Vollset, S. E. et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet 403, 2204–2256 (2024).
O’Hearn, M. et al. Incident type 2 diabetes attributable to suboptimal diet in 184 countries. Nat. Med. 29, 982–995 (2023).
Sandforth, L. et al. Prediabetes remission to reduce the global burden of type 2 diabetes. Trends Endocrinol. Metab. S1043-2760, 00004-9 (2025).
Tabák, A. G., Herder, C., Rathmann, W., Brunner, E. J. & Kivimäki, M. Prediabetes: a high-risk state for diabetes development. Lancet 379, 2279–2290 (2012).
Ligthart, S. et al. Lifetime risk of developing impaired glucose metabolism and eventual progression from prediabetes to type 2 diabetes: a prospective cohort study. Lancet Diabetes Endocrinol. 4, 44–51 (2016).
Chow, H.-M. et al. Age-related hyperinsulinemia leads to insulin resistance in neurons and cell-cycle-induced senescence. Nat. Neurosci. 22, 1806–1819 (2019).
Huang, Y. et al. Prediabetes and the risk of cancer: a meta-analysis. Diabetologia 57, 2261–2269 (2014).
ElSayed, N. A. et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care 46, S19–S40 (2023).
American Diabetes Association Professional Practice Committee. Prevention or delay of diabetes and associated comorbidities: standards of care in diabetes-2025. Diabetes Care 48, S50–S58 (2025).
Perreault, L. et al. Regression from prediabetes to normal glucose regulation and prevalence of microvascular disease in the Diabetes Prevention Program Outcomes Study (DPPOS). Diabetes Care 42, 1809–1815 (2019).
Perreault, L. et al. Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: results from the Diabetes Prevention Program Outcomes Study. Lancet 379, 2243–2251 (2012).
Fritsche, A. et al. Different effects of lifestyle intervention in high- and low-risk prediabetes: results of the randomized controlled Prediabetes Lifestyle Intervention Study (PLIS). Diabetes 70, 2785–2795 (2021).
Sandforth, A. et al. Mechanisms of weight loss-induced remission in people with prediabetes: a post-hoc analysis of the randomised, controlled, multicentre Prediabetes Lifestyle Intervention Study (PLIS). Lancet Diabetes Endocrinol. 11, 798–810 (2023).
Birkenfeld, A. L. & Mohan, V. Prediabetes remission for type 2 diabetes mellitus prevention. Nat. Rev. Endocrinol. 20, 441–442 (2024).
Lean, M. E. et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 391, 541–551 (2018).
Lean, M. E. et al. 5-year follow-up of the randomised Diabetes Remission Clinical Trial (DiRECT) of continued support for weight loss maintenance in the UK: an extension study. Lancet Diabetes Endocrinol. 12, 233–246 (2024).
Petersen, A. M. W. & Pedersen, B. K. The anti-inflammatory effect of exercise. J. Appl. Physiol. (1985) 98, 1154–1162 (2005).
Gleeson, M. et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 11, 607–615 (2011).
Hughes, V. A. et al. Exercise increases muscle GLUT-4 levels and insulin action in subjects with impaired glucose tolerance. Am. J. Physiol. 264, E855–E862 (1993).
Boulé, N. G., Haddad, E., Kenny, G. P., Wells, G. A. & Sigal, R. J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA 286, 1218–1227 (2001).
Zhyzhneuskaya, S. V. et al. Time course of normalization of functional β-cell capacity in the diabetes remission clinical trial after weight loss in type 2 diabetes. Diabetes Care 43, 813–820 (2020).
Wagner, R. et al. Lower hepatic fat is associated with improved insulin secretion in a high-risk prediabetes subphenotype during lifestyle intervention. Diabetes 72, 362–366 (2022).
Preis, S. R. et al. Abdominal subcutaneous and visceral adipose tissue and insulin resistance in the Framingham Heart Study. Obesity (Silver Spring) 18, 2191–2198 (2010).
Karlsson, T. et al. Contribution of genetics to visceral adiposity and its relation to cardiovascular and metabolic disease. Nat. Med. 25, 1390–1395 (2019).
Al-Mrabeh, A. et al. Hepatic lipoprotein export and remission of human type 2 diabetes after weight loss. Cell Metab. 31, 233–249 (2020).
van Vliet, S. et al. Obesity is associated with increased basal and postprandial β-cell insulin secretion even in the absence of insulin resistance. Diabetes 69, 2112–2119 (2020).
Cauter, E. V., Mestrez, F., Sturis, J. & Polonsky, K. S. Estimation of insulin secretion rates from C-peptide levels: comparison of individual and standard kinetic parameters for C-peptide clearance. Diabetes 41, 368–377 (1992).
Smith, G. I. et al. Influence of adiposity, insulin resistance, and intrahepatic triglyceride content on insulin kinetics. J. Clin. Invest. 130, 3305–3314 (2020).
Bergman, M. et al. International diabetes federation position statement on the 1-hour post-load plasma glucose for the diagnosis of intermediate hyperglycaemia and type 2 diabetes. Diabetes Res. Clin. Pract. 209, 111589 (2024).
Gaesser, G. A. & Angadi, S. S. Obesity treatment: weight loss versus increasing fitness and physical activity for reducing health risks. iScience 24, 102995 (2021).
Lee, S. et al. Exercise without weight loss is an effective strategy for obesity reduction in obese individuals with and without type 2 diabetes. J. Appl. Physiol. (1985) 99, 1220–1225 (2005).
Ross, R. et al. Exercise-induced reduction in obesity and insulin resistance in women: a randomized controlled trial. Obes. Res. 12, 789–798 (2004).
Rosqvist, F. et al. Overfeeding polyunsaturated and saturated fat causes distinct effects on liver and visceral fat accumulation in humans. Diabetes 63, 2356–2368 (2014).
Petersen, K. F. et al. Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes 4, 603–608 (2005).
Coral, D. E. et al. Subclassification of obesity for precision prediction of cardiometabolic diseases. Nat. Med. 31, 534–543 (2025).
Rubino, F. et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 13, 221–262 (2025).
Busetto, L. et al. A new framework for the diagnosis, staging and management of obesity in adults. Nat. Med. 30, 2395–2399 (2024).
Amati, F. et al. Lower thigh subcutaneous and higher visceral abdominal adipose tissue content both contribute to insulin resistance. Obesity (Silver Spring) 20, 1115–1117 (2012).
Ahn, C. et al. Exercise training remodels subcutaneous adipose tissue in adults with obesity even without weight loss. J. Physiol. 600, 2127–2146 (2022).
Long-term exercise training has positive effects on adipose tissue in overweight or obesity. Nat. Metab. 6, 1657–1658 (2024).
Houmard, J. A. et al. Effect of the volume and intensity of exercise training on insulin sensitivity. J. Appl. Physiol. (1985) 96, 101–106 (2004).
Smith, K. et al. Multi-ancestry polygenic mechanisms of type 2 diabetes. Nat. Med. 30, 1065–1074 (2024).
Hodgson, S. et al. Genetic basis of early onset and progression of type 2 diabetes in South Asians. Nat. Med. 31, 323–331 (2025).
Lotta, L. A. et al. Association of genetic variants related to gluteofemoral vs abdominal fat distribution with type 2 diabetes, coronary disease, and cardiovascular risk factors. JAMA 320, 2553–2563 (2018).
Mayerson, A. B. et al. The effects of rosiglitazone on insulin sensitivity, lipolysis, and hepatic and skeletal muscle triglyceride content in patients with type 2 diabetes. Diabetes 51, 797–802 (2002).
Carey, D. G. et al. Effect of rosiglitazone on insulin sensitivity and body composition in type 2 diabetic patients [corrected]. Obes. Res. 10, 1008–1015 (2002).
Gastaldelli, A. et al. Thiazolidinediones improve β-cell function in type 2 diabetic patients. Am. J. Physiol. Endocrinol. Metab. 292, E871–E883 (2007).
Klöting, N. et al. Insulin-sensitive obesity. Am. J. Physiol. Endocrinol. Metab. 299, E506–E515 (2010).
Petersen, M. C. et al. Cardiometabolic characteristics of people with metabolically healthy and unhealthy obesity. Cell Metab. 36, 745–761 (2024).
White, M. G. et al. Expression of mesenchymal and α-cell phenotypic markers in Islet β-cells in recently diagnosed diabetes. Diabetes Care 36, 3818–3820 (2013).
Nauck, M. A., Baller, B. & Meier, J. J. Gastric inhibitory polypeptide and glucagon-like peptide-1 in the pathogenesis of type 2 diabetes. Diabetes 53, S190–S196 (2004).
Vilsbøll, T., Krarup, T., Deacon, C. F., Madsbad, S. & Holst, J. J. Reduced postprandial concentrations of intact biologically active glucagon-like peptide 1 in type 2 diabetic patients. Diabetes 50, 609–613 (2001).
Toft-Nielsen, M. B. et al. Determinants of the impaired secretion of glucagon-like peptide-1 in type 2 diabetic patients. J. Clin. Endocrinol. Metab. 86, 3717–3723 (2001).
Ritzel, R. et al. Glucagon-like peptide 1 increases secretory burst mass of pulsatile insulin secretion in patients with type 2 diabetes and impaired glucose tolerance. Diabetes 50, 776–784 (2001).
Jones, I. R., Owens, D. R., Luzio, S., Williams, S. & Hayes, T. M. The glucose dependent insulinotropic polypeptide response to oral glucose and mixed meals is increased in patients with type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia 32, 668–677 (1989).
Vilsbøll, T., Krarup, T., Madsbad, S. & Holst, J. J. Defective amplification of the late phase insulin response to glucose by GIP in obese type II diabetic patients. Diabetologia 45, 1111–1119 (2002).
Bagger, J. I. et al. Glucagonostatic potency of GLP-1 in patients with type 2 diabetes, patients with type 1 diabetes, and healthy control subjects. Diabetes 70, 1347–1356 (2021).
Nauck, M. A. et al. Effects of glucagon-like peptide 1 on counterregulatory hormone responses, cognitive functions, and insulin secretion during hyperinsulinemic, stepped hypoglycemic clamp experiments in healthy volunteers. J. Clin. Endocrinol. Metab. 87, 1239–1246 (2002).
Schuppelius, B. et al. Alterations in glucagon levels and the glucagon-to-insulin ratio in response to high dietary fat or protein intake in healthy lean adult twins: a post hoc analysis. Nutrients 16, 3905 (2024).
Jumpertz von Schwartzenberg, R., Vazquez Arreola, E., Sandforth, A., Hanson, R. L. & Birkenfeld, A. L. Role of weight loss-induced prediabetes remission in the prevention of type 2 diabetes: time to improve diabetes prevention. Diabetologia 67, 1714–1718 (2024).
Kahn, S. E. et al. Effect of semaglutide on regression and progression of glycemia in people with overweight or obesity but without diabetes in the SELECT trial. Diabetes Care 47, 1350–1359 (2024).
Pajvani, U. B. et al. Complex distribution, not absolute amount of adiponectin, correlates with thiazolidinedione-mediated improvement in insulin sensitivity. J. Biol. Chem. 279, 12152–12162 (2004).
Riera-Guardia, N. & Rothenbacher, D. The effect of thiazolidinediones on adiponectin serum level: a meta-analysis. Diabetes Obes. Metab. 10, 367–375 (2008).
Doehner, W. et al. Inverse relation of body weight and weight change with mortality and morbidity in patients with type 2 diabetes and cardiovascular co-morbidity: an analysis of the PROactive study population. Int. J. Cardiol. 162, 20–26 (2012).
Arreola, E. V. et al. Prediabetes remission and cardiovascular morbidity and mortality: a post-hoc analysis from DPPOS and DaQingDPOS. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5317664 (2025).
Vazquez Arreola et al. Prediabetes Remission and Cardiovascular Morbidity and Mortality: A post-hoc analysis from the Diabetes Prevention Program Outcome Study and the DaQing Diabetes Prevention Outcome Study. Lancet Diabetes Endocrinology; provisionally accepted.
Grattan, B. J. & Connolly-Schoonen, J. Addressing weight loss recidivism: a clinical focus on metabolic rate and the psychological aspects of obesity. ISRN Obes. 2012, 567530 (2012).
Fildes, A. et al. Probability of an obese person attaining normal body weight: cohort study using electronic health records. Am. J. Public Health 105, e54–e59 (2015).
Sandforth, L. et al. Subphenotype-dependent benefits of bariatric surgery for individuals at risk for type 2 diabetes. Diabetes Care 48, 996–1006 (2025).
Taylor, R. et al. Remission of human type 2 diabetes requires decrease in liver and pancreas fat content but is dependent upon capacity for β cell recovery. Cell Metab. 28, 547–556 (2018).
Chadha, C. et al. Reproducibility of a prediabetes classification in a contemporary population. Metab. Open 6, 100031 (2020).
Lazo-Porras, M. et al. Regression from prediabetes to normal glucose levels is more frequent than progression towards diabetes: the CRONICAS cohort study. Diabetes Res. Clin. Pract. 163, 107829 (2020).
Birkenfeld, A. L., Franks, P. W. & Mohan, V. Precision medicine in people at risk for diabetes and atherosclerotic cardiovascular disease: a fresh perspective on prevention. Circulation 150, 1910–1912 (2024).
Baecke, J. A., Burema, J. & Frijters, J. E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 36, 936–942 (1982).
Knowler, W. C. et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 346, 393–403 (2002).
Fowler, S. Diabetes Prevention Program (DPP) (version 9). NIDDK Central Repository https://doi.org/10.58020/3HW5-CF91 (2024).
Mari, A., Pacini, G., Murphy, E., Ludvik, B. & Nolan, J. J. A model-based method for assessing insulin sensitivity from the oral glucose tolerance test. Diabetes Care 24, 539–548 (2001).
Matsuda, M. & DeFronzo, R. A. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22, 1462–1470 (1999).
Gastaldelli, A. et al. Importance of changes in adipose tissue insulin resistance to histological response during thiazolidinedione treatment of patients with nonalcoholic steatohepatitis. Hepatology 50, 1087–1093 (2009).
O’Donovan, S. D. et al. Improved quantification of muscle insulin sensitivity using oral glucose tolerance test data: the MISI calculator. Sci. Rep. 9, 9388 (2019).
Abdul-Ghani, M. A., Matsuda, M., Balas, B. & DeFronzo, R. A. Muscle and liver insulin resistance indexes derived from the oral glucose tolerance test. Diabetes Care 30, 89–94 (2007).
Tura, A., Kautzky-Willer, A. & Pacini, G. Insulinogenic indices from insulin and C-peptide: comparison of β-cell function from OGTT and IVGTT. Diabetes Res. Clin. Pract. 72, 298–301 (2006).
Ahrén, B., Pacini, G., Foley, J. E. & Schweizer, A. Improved meal-related β-cell function and insulin sensitivity by the dipeptidyl peptidase-IV inhibitor vildagliptin in metformin-treated patients with type 2 diabetes over 1 year. Diabetes Care 28, 1936–1940 (2005).
Piccinini, F. & Bergman, R. N. The measurement of insulin clearance. Diabetes Care 43, 2296–2302 (2020).
Allison, D. B., Paultre, F., Maggio, C., Mezzitis, N. & Pi-Sunyer, F. X. The use of areas under curves in diabetes research. Diabetes Care 18, 245–250 (1995).
de Jesús Garduno-Garcia, J. et al. Older subjects with β-cell dysfunction have an accentuated incretin release. J. Clin. Endocrinol. Metab. 103, 2613–2619 (2018).
Yamazaki, H. et al. Fat distribution patterns and future type 2 diabetes. Diabetes 71, 1937–1945 (2022).
Machann, J. et al. Follow-up whole-body assessment of adipose tissue compartments during a lifestyle intervention in a large cohort at increased risk for type 2 diabetes. Radiology 257, 353–363 (2010).
Würslin, C. et al. Topography mapping of whole body adipose tissue using a fully automated and standardized procedure. J. Magn. Reson. Imaging 31, 430–439 (2010).
Liu, C.-Y., McKenzie, C. A., Yu, H., Brittain, J. H. & Reeder, S. B. Fat quantification with IDEAL gradient echo imaging: correction of bias from T(1) and noise. Magn. Reson. Med. 58, 354–364 (2007).
Kim, H. et al. Comparative MR study of hepatic fat quantification using single-voxel proton spectroscopy, two-point Dixon and three-point IDEAL. Magn. Reson. Med. 59, 521–527 (2008).
Machann, J. et al. Hepatic lipid accumulation in healthy subjects: a comparative study using spectral fat-selective MRI and volume-localized 1H-MR spectroscopy. Magn. Reson. Med. 55, 913–917 (2006).
Bligh, E. G. & Dyer, W. J. A rapid method of total lipid extraction and purification. Can. J. Biochem. Physiol. 37, 911–917 (1959).
Coman, C. et al. Simultaneous metabolite, protein, lipid extraction (SIMPLEX): a combinatorial multimolecular omics approach for systems biology. Mol. Cell. Proteomics 15, 1453–1466 (2016).
Herzog, R. et al. LipidXplorer: a software for consensual cross-platform lipidomics. PLoS ONE 7, e29851 (2012).
Liu, M. Y. et al. Multiplexed analysis of biomarkers related to obesity and the metabolic syndrome in human plasma, using the Luminex-100 system. Clin. Chem. 51, 1102–1109 (2005).
Rasmussen, C. et al. Preanalytical impact on the accuracy of measurements of glucagon, GLP-1 and GIP in clinical trials. Scand. J. Clin. Lab. Invest. 83, 591–598 (2023).
Sollis, E. et al. The NHGRI–EBI GWAS catalog: knowledgebase and deposition resource. Nucleic Acids Res. 51, D977–D985 (2023).
NIDDK-CR Resources for Research (R4R). NIDDK Central Repository https://repository.niddk.nih.gov/home (2025).
Acknowledgements
The authors would like to thank all participants who participated and are still participating in the respective studies. Furthermore, the authors would like to acknowledge the fundamental work of the technical and nursing staff, without whom this work would not have been possible.
PLIS and this post hoc analysis were supported by the German Center for Diabetes Research, which is funded by the German Federal Ministry for Education and Research and the German states where its partner institutions are located (01GI0925). R.J.v.S. was supported by the Helmholtz Young Investigators Groups funding programme (Project ID: VH-NG-1619) and the Cluster of Excellence EXC 2124 (project 03.007). The study was additionally funded by a grant from the German Research Foundation (DFG; GRK2816 to A.L.B.). Part of the work was supported by the European Foundation for the Study of Diabetes Future Leader Award (NNF21SA0072746 to N.J.W.A.), Independent Research Fund Denmark (1052-00003B, 10.46540/4308-00056B and 10.46540/4285-00131B to N.J.W.A.) and Novo Nordic Foundation (NNF23OC0084970, NNF19OC0055001 and NNF24OC0088402 to N.J.W.A.). K.M. was supported by the Deutsche Forschungsgemeinschaft (German Research Foundation (DFG))—CRG/TRR 412. A.S. and L.S. are supported by the DFG Clinician Scientist Program ‘MINT-CS’ of the Medical Faculty of the University of Tübingen.
Additionally, this work was supported in part by the Intramural Research Program of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The DPP was conducted by the DPP Research Group and supported by the NIDDK, the General Clinical Research Center Program, the National Institute of Child Health and Human Development, the National Institute on Aging, the Office of Research on Women’s Health, the Office of Research on Minority Health, the Centers for Disease Control and Prevention and the ADA. Mass spectrometry work was supported by funds of ‘Bundesministerium für Bildung, Wissenschaft und Forschung’ (BMBFW) within the project DigiOmics4Austria (https://bit.ly/44A30s1, to R.A.). The authors gratefully acknowledge the support provided by the Mass Spectrometry Centre at the Faculty of Chemistry, University of Vienna. The data (and biospecimens) from the DPP were supplied by the NIDDK Central Repository. This manuscript was not prepared under the auspices of the DPP and does not represent analyses or conclusions of the DPP Research Group, the NIDDK Central Repository or the NIH. The funders had no role in the design, implementation, analysis or writing up of the manuscript.
Funding
Open access funding provided by Helmholtz Zentrum München - Deutsches Forschungszentrum für Gesundheit und Umwelt (GmbH).
Author information
Authors and Affiliations
Contributions
A.L.B., R.J.v.S. and A.S. conceptualized this post hoc analysis. A.S., E.V.A. and R.J.v.S. accessed and analysed the data. A.S., R.J.v.S. and A.L.B. drafted the manuscript and A.S. created the first draft of the manuscript. All authors edited the manuscript, interpreted the data, contributed to data acquisition, approved the final version, and agreed to submit it for publication.
Corresponding author
Ethics declarations
Competing interests
S.K. receives grants from the German Diabetes Association, Wilhelm Doerenkamp Foundation and California Walnut Commission, and lecture fees from Sanofi, Boehringer Ingelheim, Berlin Chemie, Lilly Deutschland and Juzo Akademie. R.W. receives lecture fees from Eli Lilly, Novo Nordisk and Sanofi, and participates in a Data Safety Monitoring Board and Advisory Board for Eli Lilly. N.P. receives lecture fees from Novo Nordisk and Gesellschaft für Wissenschaftstransfer Dresden, advisory board fees from Bayer Vital and holds patent WO2021/092265A1 for diagnosis and treatment of nonalcoholic fatty liver disease and liver fibrosis. J.J.H. is consulting with Novo Nordisk. N.J.W.A. has received research support and speaker fees from Mercodia, Novo Nordisk, Merck/MSD and Boehringer Ingelheim. All other authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Neda Rajamand Ekberg, Nathan R. Weeldreyer, Peng Wei and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Liam Messin, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Anthropometric characteristics in PLIS.
Anthropometric characteristics in PLIS: BMI, R: n = 51; NR: n = 183 (a), body weight, R: n = 49; NR: n = 170 (b), lean mass, R: n = 49; NR: n = 170 (c), fat mass R: n = 49; NR: n = 171 (d) and maximal aerobic capacity, R: n = 17; NR: n = 47 (e) during the intervention. Means of raw values are depicted with error bars indicating 95% confidence intervals. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) as post-hoc corrected comparisons derived from the respective mixed effects models. Exact p-values: a: R p = 3.03 × 10−13; NR p < 2 × 10−16; b: R p = 6.67 × 10−13; NR p < 2 × 10−16.
Extended Data Fig. 2 Diet adherence and physical activity.
Assessment of markers of diet adherence and physical activity during and after the lifestyle intervention (LI) in PLIS. a, Adherence to the diet recommendations assessed during diet counseling sessions. b, Daily distance walked inferred by pedometer data after 6 months of LI in a subgroup of individuals (R: n = 6; NR: n = 17). c–g, The habitual physical activity score during LI and at follow-up. h–l, Lean body mass during LI and at follow-up. Chi-squared test was used for a, all other p values are derived from two-sided Wilcoxon rank sum tests. Means of raw values are depicted and error bars indicate s.d. in b–l. N for each panel is depicted in the respective group bars.
Extended Data Fig. 3 Adiponectin and leptin concentrations during the lifestyle intervention.
Concentrations of circulating adiponectin, R: n = 43; NR: n = 169 (a) and R: n = 43; NR: n = 149 (b) before and after the intervention in PLIS. Means of raw values are depicted with error bars indicating 95% confidence intervals. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) and those directly above the panels comparing the group comparisons at each timepoint, all derived from post-hoc corrected comparisons from the respective mixed effects models.
Extended Data Fig. 4 VLDL palmitate subclasses during the livestyle intervention.
VLDL palmitate subclasses, R: n=47; NR: n=169 for all panels, in PLIS. Cholesterol ester palmitate (CE, a), diacylglycerol palmitate (DAG, b), lysophosphatidylcholine palmitate (LPC, c), lysophosphatidylethanolamine palmitate (LPE, d), lysophosphatidylglycerol palmitate (LPG, e), phosphatidylcholine palmitate (PC, f), phosphatidylcholine oxidized palmitate (PCO, g), phosphatidylethanolamine palmitate (PE, h), phosphatidylethanolamine oxidized palmitate (PEO, i), phosphatidylinositol palmitate (PI, j), triacylglycerol palmitate (TAG, k), combined very low-density lipoprotein palmitate (VLDL1, l). Means of raw values are depicted with error bars indicating 95% confidence intervals. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) as post-hoc corrected comparisons derived from the respective mixed effects models.
Extended Data Fig. 5 Change in β-cell incretin sensitivity during the lifestyle intervention.
β-cell incretin sensitivity expressed as area under the curve of the insulin secretion rate during the first 30 min of the OGTT plotted against the area under the curve of GLP-1 secretion during the first 30 min of the OGTT83. The base of the arrows depicts medians at baseline and the respective tip after 1 year of LI. Error bars depict s.e.m. Arrow base indicates coordinate at baseline, arrow tip indicates coordinate at 12 months for the responder group (blue) and the non-responder group (orange), respectively. R: n = 32; NR: n = 131 in PLIS.
Extended Data Fig. 6 Antropometry in DPP.
BMI, R: n = 25; NR: n = 469 (a) and visceral adipose tissue trajectories, R: n = 8; NR: n = 160 (b, c) in individuals participating in DPP. Means of raw values are depicted with error bars indicating 95% confidence intervals. P values directly above the x axes indicate change in R versus NR over time (that is interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) as post-hoc corrected comparisons derived from the respective mixed effects models. Exact p-values: a: R, p = 2.13 × 10−6; NR, p = 1 × 10−8; b: NR, p = 5.85 × 10−6.
Extended Data Fig. 7 Insulin sensitivity and secretion DPP.
Indexes of insulin sensitivity (a) and insulin secretion (b) in DPP as described in the methods. c, The hyperbolic relationship between insulin sensitivity and secretion. Arrow base indicates coordinate at baseline, arrow tip indicates coordinate at 12 months for the R group (blue) and the NR group (orange), respectively. In panel C, means of raw values are depicted with error bars indicating 95% confidence intervals. The base of the arrows depict medians at baseline and the respective tip after 1 year of LI. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) as post-hoc corrected comparisons derived from the respective mixed effects models. R: n = 25; NR: n = 469 for each panel. Exact p-values: a: NR, p = 2.48 × 10−7.
Extended Data Fig. 8 Prediabetes defined by 60-min glucose levels—insulin sensitivity and secretion.
Indexes of insulin sensitivity (a, b), insulin secretion (c) and beta cell function (d) in PLIS with response defined as return of 60min glucose during the OGTT below 155 mg/dL. P values directly above the x axes indicate change in R versus NR over time (that is, interaction term of group and time) derived from mixed effects models. P values directly above the colored bars indicate the difference between baseline and 12 months for the responder group (blue) and the non-responder group (orange) as post-hoc corrected comparisons derived from the respective mixed effects models. e, The hyperbolic relationship between insulin sensitivity and secretion. Arrow base indicates coordinate at baseline, arrow tip indicates coordinate at 12 months for the R group and the NR group, respectively. Means of raw values are depicted with error bars indicating 95% confidence intervals for a-d. In e, the base of the arrows depict medians at baseline and the respective tip after 1 year of LI. Error bars depict s.e.m. R: n = 61; NR: n = 171 for each panel.
Extended Data Fig. 9 β Coefficients from linear mixed effects models.
β coefficients for group (baseline) and group: time (6 months, 12 months) with 95% confidence intervals from linear mixed effects models reported above. Glucose (a, R: n = 51; NR: n = 183), insulin (b, R: n = 51; NR: n = 183), weight (c, R: n = 51; NR: n = 183), BMI (d, R: n = 51; NR: n = 183), lean mass (e, R: n = 49; NR: n = 170 NR), fat mass (f, n = 49; NR: n = 171), VO2 max (g, R: n = 17; NR: n = 47), insulin sensitivity index (h, R: n = 51; NR: n = 183), oral glucose insulin sensitivity index (i, R: n = 51; NR: n = 183), adipose tissue insulin resistance index (j, R: n = 21; NR: n = 109), muscle insulin resistance index (k, R: n = 51; NR: n = 183), hepatic insulin clearance (l, R: n = 51; NR: n = 183), C-peptide AUC 0-30 min/glucose AUC 0-30min (m, R: n = 51; NR: n = 183), adaptation index of β-cell function (n, R: n = 51; NR: n = 183), hepatic lipid content (o, R: n = 51; NR: n = 183), visceral adipose tissue (p, R: n = 51; NR: n = 183), subcutaneous adipose tissue (q, R: n = 51; NR: n = 183), ratio of subcutaneous to visceral adipose tissue (r, R: n = 51; NR: n = 183), muscle fat (s, R: n = 16; NR: n = 27), glucagon-like peptide 1 (t, R: n = 32; NR: n = 131), gastric inhibitory peptide (u, R: n = 16; NR: n = 27), glucagon (v, R: n = 16; NR: n = 27), adiponectin (w, R: n = 43; NR: n = 169), leptin (x, R: n = 43; NR: n = 149) in PLIS. β-coefficients are depicted as point estimates and 95% confidence intervals.
Supplementary information
Supplementary information (download PDF )
Supplementary Tables 1–3.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sandforth, A., Arreola, E.V., Hanson, R.L. et al. Prevention of type 2 diabetes through prediabetes remission without weight loss. Nat Med 31, 3330–3340 (2025). https://doi.org/10.1038/s41591-025-03944-9
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-025-03944-9
