
Abstract
Chronic obstructive pulmonary disease (COPD) often accompanies type 2 diabetes mellitus (T2DM). However, background factors affecting these diseases in the elderly remain unclear. Eligible patients with T2DM were divided into two age groups—non-elderly (<65 years) and elderly (≥65 years); COPD, ratio of forced expiratory volume in one second to forced expiratory volume (FEV1/FVC ratio), and percent predicted forced expiratory volume in one second (FEV1% predicted) were examined, and factors related to reduced respiratory function according to age group were evaluated. In total, 371 patients with T2DM were analysed. COPD was found in 9 patients (5.3%) in the non-elderly group and 45 (22.5%) in the elderly group. In the elderly, male sex, low body mass index (BMI), insulin therapy, and high C-peptide immunoreactivity levels were factors related to COPD. In the non-elderly, age, female sex, high BMI were factors related to decreased FEV1% predicted. Female sex was factor related to decreased FEV1% predicted in both age groups. Low BMI was a factor related to reduced respiratory function in elderly patients and high BMI was a factor related to reduced respiratory function in non-elderly patients. Thus, BMI needs to be managed according to the age and general condition of T2DM patients.
Similar content being viewed by others


Introduction
According to figures from 2017, approximately 420 million individuals worldwide are diagnosed with diabetes. Approximately 90% of diabetes patients in high-income countries are type 2 diabetes mellitus (T2DM)1. In Japan, it is estimated that more than 10 million people have diabetes, with the rate of increase in incidence particularly high for elderly individuals2. Decreased muscle mass and increased visceral fat due to aging increase the risk of developing T2DM through insulin resistance; these factors also increase the risk of geriatric syndromes such as sarcopenia and frailty3. Chronic obstructive pulmonary disease (COPD) is a lifestyle-related inflammatory disease of the lungs caused by long-term exposure to harmful substances, such as cigarette smoke. The number of patients with COPD worldwide is at least 210 million4 and COPD is the third leading cause of death5. In the Nippon COPD Epidemiology (NICE) study in Japan, the prevalence of COPD was estimated to be 8.6% in those over 40 years of age, an approximate total of 5.3 million patients6. The prevalence of COPD increases with age, and thus, it is a typical respiratory disease of the elderly.
COPD has many comorbidities including T2DM and these complications exacerbate COPD7,8. Inflammation and obesity have been suggested to enable co-existence of T2DM and COPD. Excess adipocytes produce inflammatory cytokines, such as interleukin-6 and tumor necrosis factor-α, which drive systemic inflammation9, increasing the risk of development of T2DM10,11 and COPD12. Obesity reduces the functional residual capacity and expiratory reserve volume through fat accumulation in the abdomen and chest, adversely affecting respiratory function13,14. Leone et al. examined the relationship between metabolic syndrome and respiratory function in 120,000 men and found that the odds ratios [95% CI] of abdominal obesity to reduced forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were 1.94 [1.80–2.09] and 2.11 [1.95–2.29], respectively15.
Conversely, low body mass index (BMI) has also been reported as a risk factor for COPD. In a group of 105 COPD patients (mean age 64.6 years), Mete et al. found 8.6% had a BMI <18 and significantly lower FEV1 and FEV1/FVC ratio16. Furthermore, Landbo et al. reported that among patients with FEV1/FEV ratio <70%, those with a low BMI had significantly higher mortality compared with those with a normal or high BMI (relative risk [95% CI]: 1.64 [1.20–2.23])17. Rates reported for obese patients vary depending on COPD severity ranked according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD): stage 1 (16.1%), stage 2 (23.5%), stage 3 (9.3%), and stage 4 (5.9%)18. These data indicate that there are fewer obese patients with severe rather than mild or moderate COPD. COPD progresses with aging, and a patient’s physical activity, vulnerability, and BMI change as COPD becomes more severe. It is plausible that body fat affects both T2DM and respiratory function. However, the relationship between body fat and respiratory function in elderly patients with T2DM remains unclear. Therefore, we examined factors influencing respiratory function in patients of two age groups with T2DM.
Results
Patient characteristics
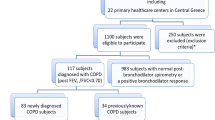
Of 539 eligible patients, 168 were excluded from analysis owing to incomplete data (Fig. 1). The remaining 371 patients were divided into either non-elderly (<65 years, n = 171, 46.1%) or elderly (≥65 years, n = 200, 53.9%) groups. Patient characteristics are shown in Table 1. The mean age was 54.3 years for the non-elderly group and 71.3 years for the elderly group; mean BMIs were 27.6 and 24.0, respectively. The rate of patients receiving insulin therapy was 25.1% in the non-elderly group and 70.5% in the elderly group. COPD was found in 5.3% of the non-elderly group and in 22.5% of the elderly group.

Patient flow. The analysis was carried out in the patients population with data for all items.
Factors influencing respiratory function
There were no significant variables affecting COPD in the non-elderly group (Table 2). In the elderly group, male sex, low BMI, insulin therapy, and increased C-peptide immunoreactivity (CPR) levels were significant variables for COPD. In the non-elderly group, pack-years was a significant variable for reduced FEV1/FVC ratio (Table 3). In the elderly group, low BMI, insulin therapy, and increased CPR levels were factors related to reduced FEV1/FVC ratio. The relationship between BMI and FEV1/FVC ratio were evaluated by sex. Regression equations for BMI and FEV1/FVC ratio were as follows; male non-elderly group: FEV1/FVC ratio = 0.17 × BMI + 75.9, male elderly group: FEV1/FVC ratio = 0.42 × BMI + 64.2, female non-elderly group: FEV1/FVC ratio = −0.02 × BMI + 84.1, female elderly group: FEV1/FVC ratio = 0.31 × BMI + 69.4. The effect of BMI on FEV1/FVC ratio was evaluated separately for males and females via an analysis of covariance (ANCOVA) with age group as a covariate. The model incorporated BMI and age group interactions. The results showed that low BMI was a significant factor influencing FEV1/FVC ratio in men (Table 4). Considering the regression equations for BMI and FEV1/FVC ratio, low BMI was a factor influencing reduced FEV1/FVC ratio in men. Neither BMI nor age group was a significant factor for reduced FEV1/FVC ratio in women. In the non-elderly group, age, female sex, and high BMI were found to be factors related to reduced percent predicted forced expiratory volume in one second (FEV1% predicted) (Table 5). In the elderly group, female sex, insulin therapy, increased CPR levels, and pack-years were factors related to reduced FEV1% predicted. The above factors related for COPD and reduced FEV1/FVC ratio and FEV1% predicted by age group are shown in Table 6.
Discussion
Among the patients with T2DM who underwent respiratory function tests, COPD was found in 5.3% of the non-elderly group and 22.5% of the elderly group. We found that low BMI, insulin therapy, and increased CPR levels were factors related to COPD and reduced FEV1/FVC ratio in the elderly group. High BMI was a factor related to reduced FEV1% predicted in the non-elderly group. Female sex was determined to be a factor related to reduced FEV1% predicted in both age groups.
In the NICE study in Japan, the prevalence of COPD was 8.6% in people over 40 years of age and 17.4% in those over 70 years of age6. In our study, the prevalence of COPD in the same age class was found to be 14.6% for those over 40 years of age and 20.9% for those over 70 years of age (22.5% for those over 65 years of age). Thus, our results indicate that the prevalence of COPD in T2DM patients may be higher than in the general population.
This study showed an association between increased CPR levels and decreased respiratory function in the elderly group. CPR levels reflect increases in insulin secretion in response to insulin resistance19. Therefore, our results indicate that insulin resistance is a factor related to COPD and reduced FEV1/FVC ratio. T2DM impairs both large and micro-vessels; thus, alveolar capillary beds might also be affected20,21. Indeed, diffusing capacity of lung for carbon monoxide (DLCO), an indicator of CO binding from alveoli to pulmonary capillary hemoglobin, was reduced in diabetic patients22. DLCO values also vary with morphological or functional changes in alveolar capillaries23. In pulmonary tissues of diabetic model animals, inflammatory changes in pulmonary vascular tissues, decreased antioxidant enzyme activity, thickening of pulmonary capillary basement membrane and decreased ventilation capacity in alveoli have been reported24. Considering the above, the influence of T2DM on respiratory function may be due to alveolar morphological changes through increased oxidative stress associated with inflammation. Furthermore, it has been reported that phrenic nerve conduction velocity was decreased in diabetic patients25. These effects may be related to the relationship between increased CPR and decreased respiratory function found in this study.
We found low BMI to be a factor related to reduced respiratory function in elderly patients with T2DM. Table 7 shows patient distribution and BMI according to severity of COPD. In this study, there were only two patients with stage III and no patient with stage IV. Due to the small sample size of severe cases, no clear result was obtained; however, mean BMI was relatively low in patients with Stage III compared with those of Stage I or II in the elderly group. This may be due to systemic vulnerability associated with aging. The prevalence of frailty in diabetic patients is reportedly three to five times higher than in non-diabetic patients26,27. Frailty is caused by various factors including loss of muscle mass. Insulin increases protein synthesis and decreases protein degradation in the muscle; thus, insulin resistance may lead to reduce muscle mass and strength in T2DM28,29. Furthermore, insulin-like growth factor-1 (IGF-1), which affects muscle and bone strength, also decreases in T2DM patients29,30. Thus, T2DM patients are prone to frailty, which in turn affects respiratory function and physical activity, leading to further complications31. Therefore, low BMI as a factor related to reduced respiratory function in elderly patients is considered to reflect systemic vulnerability.
Contrastingly, high BMI was found to be a factor related to reduced FEV1% predicted in the non-elderly group. Fat accumulation in the rib cage and visceral cavity reduces respiratory function by adversely affecting functional residual capacity14,32. While the mean BMI for the general Japanese population is 23.7 kg/m2 for men and 22.5 kg/m2 for women33, the non-elderly group in this study had a mean BMI of 27.4 kg/m2. Thus, high BMI might have affected reduced respiratory function in the non-elderly group. However, this relationship was not found for FEV1/FVC ratio. Since increased body fat decreases FVC and FEV131,32, it is possible that sensitivity for respiratory function was higher for FEV1% predicted compared to FEV1/FVC ratio in the study population. Low BMI was a factor related to reduced FEV1/FVC ratio in men of all ages. This indicates that the influence of low BMI was a dominant for reduced FEV1/FVC ratio in men in the integrated evaluation of high BMI in the non-elderly group and low BMI in the elderly group, both of which were factors related to reduced FEV1/FVC ratio. Therefore, although low BMI was a factor related to reduced FEV1/FVC ratio in men, it should be noted that the effect of BMI differs between non-elderly and elderly patients.
Male sex was a factor related to COPD only in the elderly group and female sex was a factor related to reduced FEV1% predicted in both age groups. Smoking rates in Japan were higher for men (27.8%) than for women (8.7%) in 201834 and correspondingly, there are more men with COPD (183,000) than women (79,000)35. However, women are more sensitive to cigarette smoke than men, and thus, they likely to be more susceptible to respiratory function problems36. Taking these data into account, our results suggest that men are at higher risk of developing COPD, but women are at higher risk of reduced respiratory function, including non-COPD.
In the analysis of all patients, we found a weak positive correlation between the FEV1/FVC ratio and BMI, and no significant correlation between FEV1% predicted and BMI (data not shown). However, the effect of BMI on respiratory function differs between elderly and non-elderly patients, and also varies by sex. These results indicate that, in T2DM patients, factors affecting respiratory function differ depending on their background, making it difficult to elucidate the relationship between T2DM and respiratory function. An important finding in this study is that the factors affecting respiratory function in T2DM patients differed by age and sex.
This was a single-site study with a small sample size of 371. The mean BMI for patients was 27.4 for the non-elderly group and 24.0 for the elderly group; the analysed population seems more likely to be obese compared with the general population. Therefore, the results of our study need to be interpreted with consideration of these limitations.
Both T2DM and COPD are affected by BMI, and each disease affects each other. Therefore, in patients with T2DM, respiratory function tests are important for risk management of COPD as well as T2DM itself. Our study showed that T2DM was a factor related to COPD and that BMI needs to be managed according to patient age and general condition.
Methods
Patients
Eligible patients for this study included those with T2DM who had visited Okamoto Internal Medicine Clinic, Shizuoka, Japan, from April 2017 to September 2018 and met the following inclusion criteria: (1) patients with established diagnosis of T2DM ≥ 40 years of age, (2) patients without respiratory disease or those having a history of disease other than COPD that may affect the spirometry, and (3) provision of written consent for a respiratory function test.
This study was conducted in compliance with the Declaration of Helsinki and according to the Ethical Guidelines for Medical and Health Research Involving Human Subjects established by the Ministry of Health, Labour, and Welfare in Japan. The study protocol was approved by the ethical review committees of the Seishinkai Group and Okamoto Internal Medicine Clinic. Written informed consent was obtained from all study patients.
Methods
Respiratory function tests using spirometry were performed after bronchodilation in eligible patients. FEV1/FVC ratio and FEV1% predicted were measured, and the absence or presence of COPD was ascertained. COPD was diagnosed when the FEV1/FVC ratio after inhalation of bronchodilator was less than 70% and other diseases that might result in obstructive disorders were ruled out. Patient background data, including age, sex, BMI, duration of T2DM, number of oral hypoglycemic agents (OHAs), smoking history, pack-years, presence of insulin therapy, HbA1c and CPR levels, were collected. Current and former smokers were designated as having a smoking history. The number of OHAs was the sum of prescribed agents including metformin, sulfonylureas, thiazolidines, alpha-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors, sodium-glucose cotransporter-2 inhibitors, and glinides. The analysis was carried out in the patient population with data for all items above. The analytical population was divided into the non-elderly and the elderly groups. The factors influencing COPD, FEV1/FVC ratio, and FEV1% predicted were evaluated for each age group. The influence of age and BMI on FEV1/FVC ratio was assessed by sex. FEV1% predicted was calculated as percentage of measured value of FEV1 to FEV1 predicted value. FEV1% predicted was calculated as the percentage of the measured value of FEV1 of the FEV1 predicted value. The FEV1 predicted value was estimated from the following formulas by The Japanese Respiratory Society37: Male: FEV1 (L) = 0.036 × height (cm) − 0.028 × age − 1.178, Female: FEV1 (L) = 0.022 × height (cm) − 0.022 × age − 0.005. Pack-years were calculated using the following formula: pack-years = (number of cigarettes smoked per day/20) × number of years smoked.
Statistics
Descriptive statistics were expressed as n (%) and mean ± standard deviation. Factors influencing COPD were evaluated using stepwise multiple logistic analysis with age, sex, BMI, HbA1c, duration of T2DM, insulin therapy, number of OHAs, CPR level, and pack-years as independent variables. For the evaluation of factors influencing FEV1/FVC ratio and FEV1% predicted, stepwise multiple regression analysis was used with the same variables as the independent variables. An ANCOVA with age as a covariate was used to evaluate the effect of BMI on FEV1/FVC ratio. Two-sided α was set to be 0.05. Statistical analysis was performed using SPSS Statistics ver. 25 (IBM Corp., Armonk, N.Y., USA).
Data availability
The datasets analyzed will be available from the corresponding author on reasonable request.
Change history
13 February 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
IDF Diabetes atlas Eighth edition Chapter 2. Available at, https://diabetesatlas.org/resources/2017-atlas.html (2017).
Ministry of Health, Labour and Welfare. National Health and Nutrition Survey Available at, https://www.mhlw.go.jp/file/04-Houdouhappyou-10904750-Kenkoukyoku-Gantaisakukenkouzoushinka/kekkagaiyou_7.pdf (in Japanese) (2016).
Yanase, T., Yanagita, I., Muta, K. & Nawata, H. Frailty in elderly diabetes patients. Endocr J. 65, 1–11 (2018).
Soriano, J. B. & Rodríguez-Roisin, R. Chronic obstructive pulmonary disease overview: epidemiology, risk factors, and clinical presentation. Proc Am Thorac Soc. 8, 363–367 (2011).
López-Campos, J. L., Tan, W. & Soriano, J. B. Global burden of COPD. Respirology. 21, 14–23 (2016).
Fukuchi, Y. et al. COPD in Japan: the Nippon COPD Epidemiology study. Respirology. 9, 458–465 (2004).
Feary, J. R., Rodrigues, L. C., Smith, C. J., Hubbard, R. B. & Gibson, J. E. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 65, 956–962 (2010).
Mannino, D. M., Thorn, D., Swensen, A. & Holguin, F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 32, 962–969 (2008).
Mancuso, P. Obesity and lung inflammation. J Appl Physiol (1985). 108, 722–728 (2010).
Pradhan, A. D., Manson, J. E., Rifai, N., Buring, J. E. & Ridker, P. M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 286, 327–334 (2001).
Hu, F. B., Meigs, J. B., Li, T. Y., Rifai, N. & Manson, J. E. Inflammatory markers and risk of developing type 2 diabetes in women. Diabetes. 53, 693–700 (2004).
Attaran, D. et al. Interleukin-6 and airflow limitation in chemical warfare patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 5, 335–340 (2010).
Gifford, A. H., Leiter, J. C. & Manning, H. L. Respiratory function in an obese patient with sleep-disordered breathing. Chest. 138, 704–715 (2010).
Salome, C. M., King, G. G. & Berend, N. Physiology of obesity and effects on lung function. J Appl Physiol (1985). 108, 206–211 (2010).
Leone, N. et al. Lung function impairment and metabolic syndrome: the critical role of abdominal obesity. Am J Respir Crit Care Med. 179, 509–516 (2009).
Mete, B., Pehlivan, E., Gülbaş, G. & Günen, H. Prevalence of malnutrition in COPD and its relationship with the parameters related to disease severity. Int J Chron Obstruct Pulmon Dis. 13, 3307–3312 (2018).
Landbo, C., Prescott, E., Lange, P., Vestbo, J. & Almdal, T. P. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 160, 1856–1861 (1999).
Steuten, L. M., Creutzberg, E. C., Vrijhoef, H. J. & Wouters, E. F. COPD as a multicomponent disease: inventory of dyspnoea, underweight, obesity and fat free mass depletion in primary care. Prim Care Respir J. 15, 84–91 (2006).
Sonoda, R. et al. C-Peptide Level in Fasting Plasma and Pooled Urine Predicts HbA1c after Hospitalization in Patients with Type 2 Diabetes Mellitus. PLoS One. 11, e0147303 (2016).
van den Oever, I. A., Raterman, H. G., Nurmohamed, M. T. & Simsek, S. Endothelial dysfunction, inflammation, and apoptosis in diabetes mellitus. Mediators Inflamm. 2010, 792393 (2010).
Jermendy, G. Vascular memory: can we broaden the concept of the metabolic memory? Cardiovasc Diabetol. 11, 44 (2012).
Guazzi, M., Brambilla, R., De Vita, S. & Guazzi, M. D. Diabetes worsens pulmonary diffusion in heart failure, and insulin counteracts this effect. Am J Respir Crit Care Med. 166, 978–982 (2002).
Mirrakhimov, A. E. Chronic obstructive pulmonary disease and glucose metabolism: a bitter sweet symphony. Cardiovasc Diabetol. 11, 132 (2012).
Forgiarini, L. A. Jr., Kretzmann, N. A., Porawski, M., Dias, A. S. & Marroni, N. A. Experimental diabetes mellitus: oxidative stress and changes in lung structure. J Bras Pneumol. 35, 788–91 (2009).
Fierro, B., Bennici, S. & Raimondo, D. M. Phrenic nerve conduction in diabetic patients. A preliminary study. Acta Neurol (Napoli). 4, 357–361 (1982).
Perkisas, S. & Vandewoude, M. Where frailty meets diabetes. Diabetes Metab Res Rev. 32(Suppl 1), 261–267 (2016).
Saum, K. U. et al. Frailty prevalence and 10-year survival in community-dwelling older adults: results from the ESTHER cohort study. Eur J Epidemiol. 29, 171–179 (2014).
Dimitriadis, G., Mitrou, P., Lambadiari, V., Maratou, E. & Raptis, S. A. Insulin effects in muscle and adipose tissue. Diabetes Res Clin Pract. 93(Suppl 1), S52–59 (2011).
Rolland, Y. et al. Sarcopenia: its assessment, etiology, pathogenesis, consequences and future perspectives. J Nutr Health Aging. 12, 433–450 (2008).
Kalyani, R. R., Corriere, M. & Ferrucci, L. Age-related and disease-related muscle loss: the effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2, 819–829 (2014).
Bone, A. E., Hepgul, N., Kon, S. & Maddocks, M. Sarcopenia and frailty in chronic respiratory disease. Chron Respir Dis. 14, 85–99 (2017).
Kamal, R., Kesavachandran, C. N., Bihari, V., Sathian, B. & Srivastava, A. K. Alterations in Lung Functions Based on BMI and Body Fat % Among Obese Indian Population at National Capital Region. Nepal J Epidemiol. 5, 470–479 (2015).
National Institute of Health and Nutrition. The second term of National Health Promotion Movement in the twenty first century. Available at, http://www.nibiohn.go.jp/eiken/kenkounippon21/eiyouchousa/keinen_henka_shintai.html (in Japanese).
Japan health promotion fitness foundation. Adult smoking rate. Available at, http://www.health-net.or.jp/tobacco/product/pd090000.html (in Japanese).
Ministry of Health, Labour and Welfare Japan. Total number of patients with major diseases. Available at, https://www.mhlw.go.jp/toukei/saikin/hw/kanja/14/dl/05.pdf. (in Japanese).
Gut-Gobert, C. et al. Women and COPD: do we need more evidence? Eur Respir Rev. 28, pii: 180055 (2019).
The Japanese respiratory society, Lung physiology committee. Reference values for spirogram and arterial blood gas partial pressure in Japanese. Available at, http://journal.jrs.or.jp/ (in Japanese).
Acknowledgements
This work was partly supported by the Grant-in-Aid for Scientific Research (C) from Japan Society for the Promotion of Science (JSPS KAKENHI Grant Number 20724438). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
M.I., Y.Y. and H.H. conceived and designed the research, reviewed data; S.O. and M.A. made critical revision of the manuscript; M.I. and M.I. collected data, performed the statistical analysis and drafted the manuscript. All authors had reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ishii, M., Yamaguchi, Y., Hamaya, H. et al. Characteristics of factors for decreased lung function in elderly patients with type 2 diabetes. Sci Rep 9, 20206 (2019). https://doi.org/10.1038/s41598-019-56759-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-019-56759-3
This article is cited by
-
Pharmacotherapies in Older Adults with COPD: Challenges and Opportunities
Drugs & Aging (2023)
