
Abstract
Higher baseline glomerular filtration rate (GFR) may yield subsequent steeper GFR decline, especially in patients with diabetes mellitus (DM). However, this correlation in patients with chronic kidney disease (CKD) and the presence or absence of DM remains controversial. We conducted a longitudinal cohort study in a single medical center between 2011 and 2018. Participants with CKD stage 1 to 3A were enrolled and divided into DM groups and non-DM groups, and then followed up at least every 6 months. We used a linear mixed regression model with centering time variable to overcome the problem of mathematical coupling in the analysis of the relation between baseline GFR and the changes, and compared the results from correct and incorrect specifications of the mixed models. A total number of 1002 patients with 285 diabetic and 717 non-diabetic persons was identified. The linear mixed regression model revealed a significantly negative correlation between baseline GFR and subsequent GFR change rate in both diabetic group and non-diabetic group (r = − 0.44 [95% confidence interval [CI], − 0.69 to − 0.09]), but no statistical significance in non-diabetic group after within-subject mean centering of time variable (r = − 0.09 [95% CI, − 0.41 to 0.25]). Our study showed that higher baseline GFR was associated with a subsequent steeper GFR decline in the DM group but not in the non-DM group among patients with early-stage CKD. Exact model specifications should be described in detail to prevent from a spurious conclusion.
Similar content being viewed by others

Introduction
Chronic kidney disease (CKD), affecting more than 10% of the people worldwide, becomes a growing public health issue1,2,3. With the progression of CKD, the risk of developing end-stage renal disease (ESRD) increases gradually and so do the cardiovascular complications and deaths4,5. Traditional risk factors of CKD progression include hypertension, diabetes mellitus (DM), and higher body mass index (BMI)6; however, these factors do not provide a very accurate prediction of the speed of glomerular filtration rate (GFR) decline. Some patients’ GFR show rapid decline, while others remain stable7,8.
Several investigations indicated that higher baseline GFR, such as renal hyperfiltration, may relate to subsequent rapid GFR decline. Higher baseline GFR have been found in early stages of DM if hyperglycemia was not well controlled9,10,11,12,13. The pathophysiology of hyperfiltration in DM comprised several possible mechanisms, such as ultrastructural changes caused by imbalanced release of cytokines and growth factors, and disturbance of vascular tone due to an imbalance of vasoactive humoral factors in response to hyperglycemia12,14,15. Moreover, most observational studies and meta-analyses have shown a significant relation between higher baseline GFR and subsequent rapid GFR decline in patients with DM16,17,18,19.
The phenomenon of higher baseline GFR was also found in people with intolerant fasting glucose, obesity, pregnancy, or high protein diet20,21,22. However, there is limited information about the relation between higher baseline GFR and subsequent GFR decline in patients without DM. A recent study showed that higher baseline GFR was significantly related to more rapid decline in GFR over time in patients without DM by using a linear mixed regression model with a random intercept and slope, i.e. the variations in the baseline GFR and in the changes in GFR respectively, to resolve the statistical issue of mathematical coupling17. Mathematical coupling, defined as one variable containing the whole or part of another, could yield a spurious correlations between two variables irrespective of any true association, thereby leading to questionable conclusions3,17,23,24,25. Although linear mixed model can tackle the issue of mathematical coupling, correct specification of the random effects is essential for yielding a meaningful interpretation of the correlation between the random intercept and slope26. However, previous studies did not always describe their model specifications in detail, and it is, therefore, unclear whether the issue of mathematical coupling has indeed been resolved.
To investigate the relationship between the baseline GFR and subsequent GFR change, we used an early stages of CKD cohort comprising patients with DM and without DM. We used linear mixed model to overcome the mathematical coupling in the analysis of the relation between the baseline GFR and its changes. We also compared results from correct and incorrect specifications of mixed models to assess the impact of mathematical coupling. We hypothesized that higher baseline GFR is a risk factor of a rapid GFR decline in patients with DM but not in those without DM.
Methods and materials
Study population
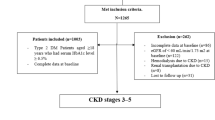
This study is a retrospective analysis of data from a single medical center, National Taiwan University Hospital. Patients, who agreed to participate the early CKD program between 2011 and 2018, were included, if their ages were between 18 and 80 years and were diagnosed with chronic kidney disease stage 1 to 3A, which was defined as a 45 ml/min/1.73 m2 < GFR < 60 ml/min/1.73 m2 or GFR ≥ 60 ml/min/1.73 m2 with a urinary protein-to-creatinine ratio (UPCR) ≥ 150 mg/g or significant findings of renal pathology for at least 3 months27,28. Patients, who had acute kidney injury within three months, Child Pugh class B to C liver cirrhosis, or terminal malignancies, were excluded. We then divided the cohort into DM (including type 1 and type 2 DM) and non-DM groups to proceed with statistical analyses. This study has been approved by the Research Ethics Committee of the National Taiwan University Hospital (202006020RINB). As this study was retrospective and observational, participants written informed consent was waived by the Research Ethics Committee of the National Taiwan University Hospital.
Early chronic kidney disease program
The early CKD program was initiated by the National Health Insurance Bureau, the Ministry of Health and Welfare in Taiwan, to care patients with CKD stages 1 to 3a in high-risk population since 201129. The high-risk population of CKD progression includes people of being older than 65 years old, family history of CKD, diabetes mellitus, and hypertension.
These patients were invited to join this program on their visits to outpatient clinics. A comprehensive educational program, consisting of basic knowledge of chronic kidney disease, risk factors, lifestyle modification and medical treatment, was provided. The participants returned to the clinic every 3–6 months, according to the clinical presentations of patients and judgments of primary care physicians. They attended classes of the educational programs and undertook routine laboratory tests at least every 6 months. Once patients’ GFR was lower than 45 ml/min/1.73 m2 or UPCR≧1000 mg/gm, they were transferred to the Pre-ESRD program for further management29.
Data collection
Basic personal information of age, sex and underlying comorbidity were recorded. Body height, weight, blood pressure and biochemical data, including serum creatinine, low-density lipoprotein cholesterol, fasting glucose and HbA1c (only for DM patients) and UPCR were recorded at baseline and every 3 to 6 months. The estimated GFR (eGFR) was calculated by the Taiwanese MDRD equation [1.309 × (186 × (serum creatinine)−1.154 × Age −0.203 × 0.742 (if female)) 0.912] , which was developed by using linear regression of the difference on the average of log-transformed inulin clearance and the MDRD, CKD-Epidemiology Collaboration (CKD-EPI) equations, and has been validated and shown to be more accurate and precise than MDRD-4 variables and CKD-EPI equations for Taiwanese adults28,30.
Statistical analyses
We used the mean ± standard deviation (SD) to summarize continuous variables, and relative frequency for categorical variables. The differences between the two groups were analyzed by using the t-test or the chi-squared test. Variables with a non-normal distribution were analyzed by the Mann–Whitney U test. A two-level linear mixed regression model with the random intercept and slope was used to analyze eGFR measurements and solving the statistical problems of mathematical coupling. The dependent variable was the absolute value of eGFR. The time variable was the duration of observation starting from the date of the first visit up to that of the last visit in nephrology outpatient department. To test the appropriate null hypothesis in multivariable linear mixed regression model, we undertook within-subject mean centering for the duration of observation to correct for the effects of mathematical coupling between random intercept and slope23,24,25,26. The basic linear mixed model is written as:
where \(eGF{R}_{ij}\) is the observed eGFR for the jth patient on ith occasion; \({b}_{0j}\) is the intercept for the jth patient \({\beta }_{0}\) is the average intercept for the whole patient population, and \({u}_{0j}\) is the random intercept, i.e. the variations in the intercepts of the whole patient population, which is assumed to follow a normal distribution with the mean of zero and variance of \({\sigma }_{u0}^{2}\); Time is the centered time variable, i.e. the centered duration of observation in years for each patient; \({b}_{1j}\) is the slope for the jth patient \({\beta }_{1}\) is the average slope for the whole patient population, and \({u}_{1j}\) is the random slope, i.e. the variations in the slopes of the whole patient population, which is assumed to follow a normal distribution with the mean of zero and variance of \({\sigma }_{u1}^{2}\); and \({e}_{ij}\) is the residual error term for \(eGF{R}_{ij}\). \({u}_{0j}\) and \({u}_{1j}\) follow a bivariate normal distribution, and the parameter \({\sigma }_{u01}\) is the covariance between random intercept and slope and can be used to calculate the correlation r between the baseline eGFR and the subsequent changes in eGFR by using the formulae: \(r=\frac{{\sigma }_{u01}}{\sqrt{{\sigma }_{u0}^{2}*{\sigma }_{u1}^{2}}}\). The effect of an independent variable on GFR change rate in mL/min per year was evaluated by using 2-way interaction between the independent variables and the centered time variable. The relation between baseline eGFR (ml/min/1.73 m2) and succeeding eGFR changes (ml/min/1.73 m2 per year) was evaluated by the correlation between the random intercept and slopes. We also conducted the same analyses without centering the time variables to assess the impact of mathematical coupling on the estimation of the correlation between the baseline eGFR and the change. We performed covariates adjustment, including sex and age in model 1, then plus BMI and systolic blood pressure (SBP) in model 2, and added current smoking status, HbA1c (only in diabetes mellitus group) and urine protein-creatinine ratio in model 3. A P-value < 0.05 was considered statistically significance. The statistical software Stata version 14 (Stata Corp College Station, Texas, USA) (https://www.stata.com/) was used for data analysis. All methods carried out were in accordance with relevant guidelines and national legal regulations.
Results
Baseline characteristics of study population
The baseline characteristics of diabetes mellitus and non-diabetes mellitus groups is shown in Table 1. A total number of 1002 patients with early-stage CKD (717 in non-DM group and 285 in DM group, respectively) and 7621 nephrology clinic visits were identified between January 1, 2011, and December 31, 2018. More than 70 percent of patients in both DM and non-DM groups were male (79.6% and 72.9%, respectively). Patients in DM group were 4.4 years older than those in non-DM group (68.0 vs 63.6 years old, p < 0.001) and had a higher BMI (mean BMI 26.0 vs 24.8 kg/m2, p < 0.001, respectively). Mean baseline eGFR was 58.5 ± 18.1 (SD) ml/min/1.73 m2 in the non-DM group and 57.4 ± 16.3 (SD) ml/min/1.73 m2 in DM group by the Taiwanese MDRD equation. The eGFR declined gradually in both DM and non-DM groups (Fig. 1), but the lengths of follow-up varied greatly among participants.

The graph of estimated glomerular filtration rate (eGFR) change without within-subject mean centering for the time variable.
Fixed effects of risk factors on the baseline eGFR and changes of eGFR
Our multivariable mixed model (model 3) showed that males and older age had a significantly negative association with baseline eGFR; the average baseline eGFR of men was 4.61 ml/min/1.73 m2 lower than that of women, and the average baseline eGFR decreased by 0.50 ml/min/1.73 m2 when a patient’s age increased by 1 year. UPCR had a significantly negative relationship to the changes of eGFR in the DM group; the average change in eGFR decreased by 0.10 ml/min/1.73 m2 as UPCR increased by 10 mg/g (Table 2). In the non-DM group, male and older age also had a negative association with baseline eGFR; the average baseline eGFR of men was 10.85 ml/min/1.73 m2 lower than that of women, and the average baseline eGFR decreased by 0.44 ml/min/1.73 m2 when a patient’s age increased by 1 year, and higher systolic blood pressure showed greater changes in eGFR; the average change in eGFR increased by 0.02 ml/min/1.73 m2 when systolic blood pressure increased by 1 mmHg (Table 3).
Association between baseline eGFR and subsequent eGFR change
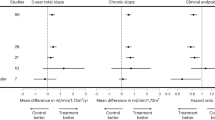
In the DM group, a significantly consistent negative correlation between GFR at baseline (random intercept) and GFR change rate (random slope) was found after multivariable adjustment (r = − 0.46 [95% CI, − 0.62 to − 0.27] in model 1, r = − 0.51 [95% CI, − 0.68 to − 0.30] in model 2, and r = − 0.65 [95% CI, − 0.81 to − 0.39] in model 3, respectively). After within-subject mean centering for the time variable, the correlations decreased substantially (r = − 0.25 [95% CI, − 0.44 to − 0.04] in model 1, r = − 0.30 [95% CI, − 0.51 to − 0.05] in model 2, and r = − 0.40 [95% CI, − 0.67 to − 0.05] in model 3, respectively) (Table 4) (Fig. 2).

The relation between baseline glomerular filtration rate (GFR) and GFR change rate. The figure shows the best linear unbiased predictors (BLUPs) of random slopes and intercepts, indicating the relation between baseline GFR (the random intercept) and GFR change rate (random slope) in a linear mixed model after using within-subject mean centering for the time variable. DM, diabetes mellitus; CI, confidence interval. Stata version 14 (Stata Corp College Station, Texas, USA) (https://www.stata.com/).
In the non-DM group, multivariable mixed linear regression model also showed a significantly negative correlation between GFR at baseline and GFR change rate (r = − 0.22 [95% CI, − 0.36 to − 0.06] in model 1, r = − 0.36 [95% CI, − 0.52 to − 0.17] in model 2, and r = − 0.44 [95% CI, − 0.69 to − 0.09] in model 3, respectively). However, after within-subject mean centering for the time variable, the negative correlation between GFR at baseline and GFR change became much smaller and no longer statistically significant (r = 0.05 [95% CI, − 0.11 to 0.21] in model 1, r = − 0.06 [95% CI, − 0.26 to 0.15] in model 2, and r = − 0.09 [95% CI, − 0.41 to 0.25] in model 3, respectively) (Table 5) (Fig. 2).
Discussion
To our best knowledge, this study is the first to explore the relation between baseline eGFR and subsequent GFR decline in DM and non-DM patients with early-stage CKD in a long-term population-based cohort. After multivariable adjustment, we found that male and increased age had a significantly negative effect on the baseline eGFR, and only UPCR showed a significant relation to the decrease in eGFR in patients with CKD and DM. In patients with CKD and non-DM, males and older age also showed a significantly negative association with the baseline eGFR but males (in model 1 and 2) and higher systolic pressure were associated with a significantly smaller decrease in eGFR. Naïve analyses without centering of the time variable found a significantly negative correlation between GFR at baseline and GFR change in DM and non-DM patients with CKD. After within-subject mean centering, a significant but moderate correlation were observed only in DM patients with CKD. This indicates the impact of mathematical coupling on the estimation of the correlation between GFR at baseline and GFR change cannot be overlooked, and this is consistent with findings in the previous methodological studies23,25,31,32,33.
It is still controversial whether hyperfiltration with higher baseline GFR is related to subsequent GFR decline. Some studies revealed that hyperfiltration with higher eGFR was associated with more rapid eGFR decline in patients with type 1 or type 2 DM16,17,18,19,34,35,36. Moreover, Melsom et al. showed that this significant correlation existed not only in patients with DM but also in those without DM17. In contrast, no substantial correlation between baseline GFR and subsequent GFR decline was also found in other investigations37,38. This inconsistency may be attributed to considerable GFR variations over time, such as age-related GFR decline, GFR measurements, and inappropriate statistical methods for assessing the relation between GFR at baseline and its changes39,40. In our study, a negative relation between the baseline eGFR and subsequent decline was found only in patients with DM but not in patients without DM.
The accurate measurement of GFR should examine the clearance of materials which are only through renal filtration, such as iohexol, iothalamate, inulin, etc.41. However, the estimated GFR was more readily available and cost-effective in the clinical practice than GFR via direct measurement, which was difficult to replicate due to different physiological conditions and great variations over time. Two of the most common equations for estimating GFR were MDRD-4 variables and CKD-EPI worldwide. However, the MDRD-4 equation was created by using data from Caucasians and African Americans with CKD and is likely to underestimate GFR, when eGFR greater than 60 mL/min/ 1.73 m242,43. The KDIGO 2012 guidelines recommend using the CKD-EPI equation in adults, unless an alternative equation has been shown to be more accurate in the specific population44. In our study, we used a corrected MDRD equation (Taiwanese MDRD), because it has been shown to have better precision and a lower bias than the equations of the MDRD-4 and CKD-EPI in Taiwanese population30.
Analysis of the relation between the baseline and changes suffered from mathematical coupling, which gives rise to misleading results and invalid testing of the null hypothesis23,25. Some studies applied a linear mixed regression model with random intercept and slope to resolve this statistical issue and to attain correct results17. However, the correct null hypothesis for testing the correlation between the baseline value and subsequent change is not zero, because these two variables have an underlying mathematical relation by sharing a common component of the baseline value23,25. It has been shown that centering the time variable could overcome this underlying mathematical relation and then attain an accurate result of null hypothesis test23,24,25,45. In this study, we undertook within-subject mean centering for the time variable to investigate the relationship between the baseline eGFR and its changes. We observed that the negative correlations are always attenuated after centering when compared with those given by the conventional approach without centering, in DM and non-DM patients with CKD. Moreover, in non-DM patients, this negative correlations were no longer statistically significant, after correct methodologies were used. This implied that higher baseline eGFR or renal hyperfiltration may be only a subclinical indicator but not the major cause of renal damage in patients with DM and early-stage CKD. Furthermore, when patients’ GFR was lower than 45 ml/min/1.73 m2, they would be transferred to the Pre-ESRD program, and their eGFR values were no longer being included in our analysis. This may lead to the truncation of low eGFR values, resulting in the reduction in the variances of follow-up eGFR and the over-estimation of the negative relation between the baseline eGFR and its changes. Our study suggests that previous evidence on the relation between the baseline eGFR and the decline in eGFR should be interpreted with great cautions and may require reevaluation.
Limitations
Our study has some limitations. First, we included a relatively small number of participants, especially in patients with DM. Despite this problem, our study collected sufficient data of repeated measurements during the long-term follow-up to achieve robust inference. Second, our study included a higher proportion of men and elderly in DM and non-DM groups. According to previous national study, near two thirds of adults with CKD was more than 60 years old (63.3%), and men had a higher prevalence of early-stage CKD than did women (11.7% versus 9.9%)46. These data showed a similar distribution to our study. Therefore, it needs to be cautious to apply findings in our study to other populations with different sex proportions or age distributions. Third, the mean eGFR in our study was lower than the traditional definition of hyperfiltration with high GFR. The focus of our study is not the consequence of renal hyperfiltration but proper analyses of the relation between higher baseline GFR and subsequent GFR change. Moreover, the number of nephrons varied among individuals and usually decreased with age or renal injury39. Glomerular hyperfiltration or single-nephron hyperfiltration in people with fewer numbers of nephrons may show a normal or mildly low level of whole-kidney GFR, which is equal to single-nephron GFR multiplied by nephron numbers47. Therefore, results from our study still provides evidence on the relation between higher eGFR and subsequent eGFR changes. Finally, patients with GFR lower than 45 ml/min/1.73 m2 or UPCR≧1000 mg/gm were transferred to the Pre-ESRD program for further management. Therefore, informative censoring may be a concern, since the information from those with rapidly deteriorating kidney function were selectively missing. This may be regarded as a problem with the truncated data, since GFR lower than a threshold was unavailable. This is likely to lead to a decrease in the variance of GFR with the increase in follow-up of the cohort, yielding a spurious, negative correlation between the baseline GFR and changes in GFR25. Therefore, the negative correlation between GFR at baseline and GFR changes in patients with CKD and DM may be weaker than what has been observed.
Conclusion
In conclusions, a significantly negative correlation between GFR at baseline and GFR changes was found in patients with CKD and DM, but no such correlation was found in non-DM patients with CKD when correct statistical analyses were undertaken. Higher baseline eGFR or renal hyperfiltration may be only a subclinical indicator but not the major cause of renal damage in patients with DM and early stage CKD. Our findings suggest that higher baseline GFR was associated with a greater GFR decline in DM patients but not in non-DM patients. Investigations about baseline value to subsequent changes should describe model specifications in detail to assure resolving mathematical coupling and then prevent from a spurious conclusion.
References
Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 385(9963), 117–171 (2015).
Plantinga, L. C. et al. Patient awareness of chronic kidney disease: trends and predictors. Arch. Intern. Med. 168(20), 2268–2275 (2008).
Archie, J. P. Jr. Mathematic coupling of data: A common source of error. Ann. Surg. 193(3), 296–303 (1981).
Pinkau, T., Hilgers, K. F., Veelken, R. & Mann, J. F. How does minor renal dysfunction influence cardiovascular risk and the management of cardiovascular disease?. J. Am. Soc. Nephrol. 15(3), 517–523 (2004).
Lambers Heerspink, H. J. et al. GFR decline and subsequent risk of established kidney outcomes: A meta-analysis of 37 randomized controlled trials. Am. J. Kidney Dis. 64(6), 860–866 (2014).
Coresh, J. et al. Prevalence of chronic kidney disease in the United States. JAMA 298(17), 2038–2047 (2007).
Muntner, P. Longitudinal measurements of renal function. Semin. Nephrol. 29(6), 650–657 (2009).
Eriksen, B. O. et al. Elevated blood pressure is not associated with accelerated glomerular filtration rate decline in the general non-diabetic middle-aged population. Kidney Int. 90(2), 404–410 (2016).
Hostetter, T. H., Olson, J. L., Rennke, H. G., Venkatachalam, M. A. & Brenner, B. M. Hyperfiltration in remnant nephrons: A potentially adverse response to renal ablation. Am. J. Physiol. 241(1), F85-93 (1981).
Brenner, B. M. Hemodynamically mediated glomerular injury and the progressive nature of kidney disease. Kidney Int. 23(4), 647–655 (1983).
Brenner, B. M., Lawler, E. V. & Mackenzie, H. S. The hyperfiltration theory: A paradigm shift in nephrology. Kidney Int. 49(6), 1774–1777 (1996).
Tonneijck, L. et al. Glomerular hyperfiltration in diabetes: Mechanisms, clinical significance, and treatment. J. Am. Soc. Nephrol. 28(4), 1023–1039 (2017).
Jerums, G., Premaratne, E., Panagiotopoulos, S. & MacIsaac, R. J. The clinical significance of hyperfiltration in diabetes. Diabetologia 53(10), 2093–2104 (2010).
Vallon, V. & Komers, R. Pathophysiology of the diabetic kidney. Compr. Physiol. 1(3), 1175–1232 (2011).
Bak, M., Thomsen, K., Christiansen, T. & Flyvbjerg, A. Renal enlargement precedes renal hyperfiltration in early experimental diabetes in rats. J. Am. Soc. Nephrol. 11(7), 1287–1292 (2000).
Thomson, H. J. et al. Elevated baseline glomerular filtration rate (GFR) is independently associated with a more rapid decline in renal function of patients with type 1 diabetes. J. Diabetes Complications. 30(2), 256–261 (2016).
Melsom, T. et al. Correlation between baseline GFR and subsequent change in GFR in Norwegian adults without diabetes and in pima Indians. Am. J. Kidney Dis. 73(6), 777–785 (2019).
Moriya, T. et al. Patients with type 2 diabetes having higher glomerular filtration rate showed rapid renal function decline followed by impaired glomerular filtration rate: Japan Diabetes Complications Study. J. Diabetes Complicat. 31(2), 473–478 (2017).
Magee, G. M. et al. Is hyperfiltration associated with the future risk of developing diabetic nephropathy? A meta-analysis. Diabetologia 52(4), 691–697 (2009).
Melsom, T. et al. Impaired fasting glucose is associated with renal hyperfiltration in the general population. Diabetes Care 34(7), 1546–1551 (2011).
Sasson, A. N. & Cherney, D. Z. Renal hyperfiltration related to diabetes mellitus and obesity in human disease. World J. Diabetes. 3(1), 1–6 (2012).
Stefansson, V. T., Schei, J., Jenssen, T. G., Melsom, T. & Eriksen, B. O. Central obesity associates with renal hyperfiltration in the non-diabetic general population: a cross-sectional study. BMC Nephrol. 17(1), 172 (2016).
Blance, A., Tu, Y. K. & Gilthorpe, M. S. A multilevel modelling solution to mathematical coupling. Stat. Methods Med. Res. 14(6), 553–565 (2005).
Yu, H., Jiang, S. & Land, K. C. Multicollinearity in hierarchical linear models. Soc. Sci. Res. 53, 118–136 (2015).
Tu, Y. K. & Gilthorpe, M. S. Revisiting the relation between change and initial value: A review and evaluation. Stat. Med. 26(2), 443–457 (2007).
Vatcheva, K. P., Lee, M., McCormick, J. B. & Rahbar, M. H. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiology 6, 2 (2016).
Levey, A. S. & Coresh, J. Chronic kidney disease. Lancet 379(9811), 165–180 (2012).
K/DOQI clinical practice guidelines for chronic kidney disease. evaluation, classification, and stratification. Am. J. Kidney Dis. 39(2 Suppl 1), S1-266 (2002).
Wu, M. Y. & Wu, M. S. Taiwan renal care system: A learning health-care system. Nephrology (Carlton). 23(Suppl 4), 112–115 (2018).
Chen, L. I. et al. Modification of diet in renal disease (MDRD) study and CKD epidemiology collaboration (CKD-EPI) equations for Taiwanese adults. PLoS ONE 9(6), e99645 (2014).
Beggs, L., Briscoe, R., Griffiths, C., Ellison, G. T. H. & Gilthorpe, M. S. Intervention differential effects and regression to the mean in studies where sample selection is based on the initial value of the outcome variable: An evaluation of methods illustrated in weight-management studies. Biostat. Epidemiol. 2, 1–17 (2020).
Fountoulakis, K. N. The misleading concept of initial severity in depression clinical trials: Development and results from a mathematical model. Australas. Psychiatry 25(1), 18–20 (2016).
Snider, S. E., Quisenberry, A. J. & Bickel, W. K. Order in the absence of an effect: Identifying rate-dependent relationships. Behav. Processes. 127, 18–24 (2016).
Bjornstad, P. et al. Rapid GFR decline is associated with renal hyperfiltration and impaired GFR in adults with Type 1 diabetes. Nephrol. Dial. Transplant. 30(10), 1706–1711 (2015).
Lovshin, J. A. et al. Hyperfiltration, urinary albumin excretion, and ambulatory blood pressure in adolescents with Type 1 diabetes mellitus. Am. J. Physiol. Renal Physiol. 314(4), F667-f674 (2018).
Low, S. et al. Long-term prospective observation suggests that glomerular hyperfiltration is associated with rapid decline in renal filtration function: A multiethnic study. Diab. Vasc. Dis. Res. 15(5), 417–423 (2018).
Molitch, M. E. et al. Early glomerular hyperfiltration and long-term kidney outcomes in type 1 diabetes: The DCCT/EDIC experience. Clin. J. Am. Soc. Nephrol. 14(6), 854–861 (2019).
Yip, J. W., Jones, S. L., Wiseman, M. J., Hill, C. & Viberti, G. Glomerular hyperfiltration in the prediction of nephropathy in IDDM: A 10-year follow-up study. Diabetes 45(12), 1729–1733 (1996).
Denic, A. et al. The substantial loss of nephrons in healthy human kidneys with aging. J. Am. Soc. Nephrol. 28(1), 313–320 (2017).
Gaspari, F. et al. The GFR and GFR decline cannot be accurately estimated in type 2 diabetics. Kidney Int. 84(1), 164–173 (2013).
Stevens, L. A. & Levey, A. S. Measured GFR as a confirmatory test for estimated GFR. J. Am. Soc. Nephrol. 20(11), 2305–2313 (2009).
Levey, A. S. et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 130(6), 461–470 (1999).
Imai, E. et al. Estimation of glomerular filtration rate by the MDRD study equation modified for Japanese patients with chronic kidney disease. Clin. Exp. Nephrol. 11(1), 41–50 (2007).
Chapter 2: Definition, identification, and prediction of CKD progression. Kidney Int Suppl (2011). 3(1), 63–72 (2013).
Paccagnella, O. Centering or not centering in multilevel models? The role of the group mean and the assessment of group effects. Eval. Rev. 30(1), 66–85 (2006).
Wen, C. P. et al. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462 293 adults in Taiwan. Lancet 371(9631), 2173–2182 (2008).
Denic, A. et al. Single-nephron glomerular filtration rate in healthy adults. N. Engl. J. Med. 376(24), 2349–2357 (2017).
Acknowledgements
The authors thank Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan and Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital and College of Medicine, Taipei, Taiwan, for their analytic support in this study.
Author information
Authors and Affiliations
Contributions
Y.-C.L., T.-S.L., and Y.-K.T. designed the research. Y.-C.L., T.-S.L., S.-L.L., Y.-M.C., T.-S.C. collected the data and performed the research. Y.-C.L., T.-S.L., and Y.-K.T. analyzed the data. Y.-C.L., T.-S.L., and Y.-K.T. made the tables and figures. Y.-C.L., T.-S.L., and Y.-K.T. drafted and revised the paper. All authors approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, YC., Lai, TS., Lin, SL. et al. The impact of baseline glomerular filtration rate on subsequent changes of glomerular filtration rate in patients with chronic kidney disease. Sci Rep 11, 7894 (2021). https://doi.org/10.1038/s41598-021-86955-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-021-86955-z
This article is cited by
-
Androgen deprivation therapy and kidney function in patients with prostate cancer: an analysis of the RADICAL-PC cohort
International Urology and Nephrology (2026)
