
Abstract
Non-steroidal anti-inflammatory drugs (NSAIDs) are widely used for their antipyretic, analgesic, and anti-inflammatory properties. However, various aspects of NSAID-induced lower gastrointestinal tract injury remain unclear, and effective prophylaxis has not been established. Based on its pharmacological effect and clinical trials, rebamipide may prevent lower gastrointestinal tract injury, although this evidence is limited by the small scale of trials. The present study used the FDA Adverse Event Reporting System (FAERS) and the Japanese Adverse Event Reporting Database (JADER) to assess the efficacy of rebamipide in combination with loxoprofen and diclofenac in preventing NSAID-induced lower gastrointestinal tract injury. The calculated reporting odds ratio and 95% confidence interval (CI) for rebamipide in combination with loxoprofen and diclofenac were 1.15 (95% CI 0.88–1.51) and 1.28 (95% CI 0.82–2.01) for FAERS, and 0.50 (95% CI 0.35–0.71) and 0.43 (95% CI 0.27–0.67) for JADER, respectively. No signal was detected when combining drugs. These results suggest a prophylactic effect of rebamipide on NSAID-induced lower gastrointestinal tract injury.
Similar content being viewed by others

Introduction
Non-steroidal anti-inflammatory drugs (NSAIDs) are widely applied for their antipyretic, analgesic, and anti-inflammatory properties1. They have been known to cause upper gastrointestinal tract injury; however, advances in capsule endoscopy have revealed that NSAIDs can also elicit lower gastrointestinal tract injury2,3. The latter has been linked to fewer mucosal protective factors caused by decreased prostaglandin production, oxidative stress due to mitochondrial dysfunction, and an abundance of gram-negative bacteria following disruption of intestinal microflora homeostasis4,5,6. Nevertheless, several aspects of NSAID-induced lower gastrointestinal tract injury remain unclear, and an effective prophylaxis has not been established.
Rebamipide has antioxidant effects by protecting mucous membranes through increased production of prostaglandins and by inhibiting the production of superoxide as a free radical scavenger7,8,9. In this way, rebamipide counteracts some of the causes of NSAID-induced lower gastrointestinal tract injury. Rebamipide has been shown to be effective in preventing lower gastrointestinal tract injury when used in combination with diclofenac, a common NSAID10,11,12. Such pharmacological evidence and the findings from clinical trials suggest that rebamipide may have a beneficial protective function; however, this evidence is limited by the small size and unreliability of trial reports. There are various approaches for analyzing prophylaxis against adverse drug reactions. Although randomized controlled trials (RCTs) provide the best evidence, it is sometimes difficult from an ethical perspective to conduct large-scale clinical studies on prophylaxis13,14. Moreover, it is not possible to comprehensively analyze all types of patients, as children, pregnant women, and individuals with underlying conditions are generally excluded from clinical trials13,14.
In recent years, large real-world adverse drug reaction databases, such as the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) and the Japanese Adverse Drug Event Report (JADER) of the Pharmaceuticals and Medical Devices Agency (PMDA), have come to include an increasing amount of data15,16,17,18. Spontaneous adverse event reports include data on patients normally excluded from clinical trials, making them more likely to reflect clinical practice. Such databases are now regarded as a suitable alternative to RCTs for preventive drug discovery19,20,21,22. FAERS is the world's largest database of spontaneous adverse event reports, with 13 million cases currently registered. Comparatively, JADER has fewer entries, but it is useful for drugs, such as rebamipide, which are frequently prescribed in Japan. Although there are some differences in the nature of data published by FAERS and JADER, they can serve as complementary sources of information23.
In the present study, we employed these two databases of adverse drug reactions to analyze NSAID-induced lower gastrointestinal tract injury in relation to concomitant use of rebamipide and evaluated the possible protective effect of this agent.
Results
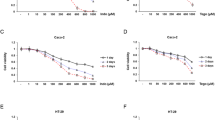
The flow chart illustrating the use of the FAERS database to analyze the reporting odds ratio (ROR) of NSAID-induced lower gastrointestinal tract injury is shown in Fig. 1. The ROR (95% confidence interval [CI]) for loxoprofen and diclofenac was 4.23 (95% CI 3.75–4.78) and 4.70 (95% CI 4.40–5.02), respectively. The lower limit of the 95% CI of ROR for both drugs was > 1 and, hence, the adverse event signal was detected (Table 1, [I] [III]). Assessing the combined effect of rebamipide and loxoprofen or diclofenac on NSAID-induced lower gastrointestinal tract injury yielded a ROR (95% CI) of 1.15 (95% CI 0.88–1.51) and 1.28 (95% CI 0.82–2.01). The lower limit of the 95% CI was < 1, and no signal was detected (Table 1, [II] [IV]).

Flow chart summarizing the determination of RORs for lower gastrointestinal tract injury categorized according to drug usage in FAERS. Numbers in parentheses indicate the number of adverse drug reactions reported. [I] ROR shows the odds ratio of lower gastrointestinal tract injury for loxoprofen alone and for drugs excluding loxoprofen. [II] ROR shows the odds ratios for loxoprofen with and without rebamipide. [III] ROR shows the odds ratio of lower gastrointestinal tract injury for diclofenac alone and for drugs excluding diclofenac. [IV] ROR shows the odds ratios for diclofenac with and without rebamipide.
The same analysis was performed using the JADER database and the corresponding flow chart is shown in Fig. 2. The ROR (95% CI) for loxoprofen and diclofenac was 1.61 (95% CI 1.40–1.84) and 4.84 (95% CI 4.26–5.50), respectively. The lower limit of the 95% CI for both loxoprofen and diclofenac was > 1, and the signal was detected (Table 2, [I] [III]).

Flow chart summarizing the determination of RORs for lower gastrointestinal tract injury categorized according to drug usage in JADER. Numbers in parentheses indicate the number of adverse drug reactions reported. [I] ROR shows the odds ratio of lower gastrointestinal tract injury for loxoprofen alone and for drugs excluding loxoprofen. [II] ROR shows the odds ratios for loxoprofen with and without rebamipide. [III] ROR shows the odds ratio of lower gastrointestinal tract injury for diclofenac alone and for drugs excluding diclofenac. [IV] ROR shows the odds ratios for diclofenac with and without rebamipide.
The ROR (95% CI) for lower gastrointestinal tract injury with loxoprofen and diclofenac in combination with rebamipide was 0.50 (95% CI 0.35–0.71) and 0.43 (95% CI 0.27–0.67). The lower limit of the 95% CI was < 1, and no signal was detected (Table 2, [II] [IV]).
Discussion
Reports about the clinical significance and frequency of adverse events with NSAIDs resulting in lower gastrointestinal tract injury are increasing24, and they present a higher mortality rate than upper gastrointestinal events, suggesting the need for early prophylaxis25. At present, there is no prophylaxis for NSAID-induced lower gastrointestinal tract injury because acid secretion inhibitors are not expected to be effective. In this study, we analyzed the preventive effect of the combination of NSAIDs and rebamipide on NSAID-induced lower gastrointestinal tract injury using the FAERS and JADER databases. The results showed that the risk of lower gastrointestinal tract injury was reduced when rebamipide was combined with loxoprofen and diclofenac, confirming a potential preventive effect.
NSAID-induced lower gastrointestinal tract injury has been reported in 40‒53% of patients taking diclofenac for 2 weeks3,26, and in 71% of patients taking multiple NSAIDs for more than 3 months27. These values indicate that NSAIDs cause frequent lower gastrointestinal tract injuries, regardless of treatment duration. In the present study, the RORs of loxoprofen and diclofenac were consistent with the findings from previous reports, and an adverse event signal was obtained with both drugs. Hence, this study can be considered a good reflection of actual clinical practice.
In recent years, data mining using large-scale databases has been attracting attention as an exploratory study method for the prevention of adverse drug reactions21,22. Zhao et al. investigated the preventive effect of exenatide combination on the side effects of rosiglitazone, such as myocardial infarction and stroke, using FAERS21. The results showed that the combination of rosiglitazone and exenatide eliminated the signals of myocardial infarction and stroke. Furthermore, validation using a mouse model proved that exenatide inhibits the increase in blood coagulation caused by rosiglitazone and has a preventive effect on myocardial infarction and stroke. Nagashima et al. also conducted an analysis using FAERS to search for prophylactic drugs that can reduce the risk of hyperglycemia caused by atypical antipsychotics22. The results showed that the diabetes-related signal of quetiapine disappeared when combined with vitamin D. Furthermore, the results of validation using a mouse model established that vitamin D improves insulin resistance to quetiapine. As shown in these reports, the results of basic research correlated with the disappearance of side effect signals when certain drugs were used in combination, so database analysis may play a complementary role. Pharmacological evidence suggests a protective effect of rebamipide against NSAID-induced lower gastrointestinal tract injury28,29. Clinical trials have also shown the prophylactic effects of rebamipide, but they were carried out only in Japan, and the number of cases was reduced10,11,12. To date, no large-scale clinical trials have been conducted. In this study, the analysis was conducted using FAERS and JADER with reference to basic research and small clinical trials of rebamipide. The results suggest that rebamipide may be effective as a prophylactic agent according to FAERS and JADER data, as the combination of NSAIDs and rebamipide abolished the signals associated with lower gastrointestinal tract injury (Tables 1, 2).
Data from FAERS and JADER may differ with respect to race, social background, and medical circumstances30. Analyzing interstitial pneumonia using FAERS and JADER, Matsui et al. found very different rates of gefitinib-induced injury (7.4% and 45.6%, respectively)31, indicating strong regional variations between the two databases. In JADER, most reports are from Japan, whereas in FAERS, 70% are from the U.S.A. Rebamipide was developed in Japan and was launched there in 1990, while in other countries it entered the market only after the year 2000, explaining the limited number of cases in FAERS (Figs. 1 and 2). FAERS entries on adverse reaction associated with rebamipide are insufficient; however, the incidence can be estimated more accurately if analytical results from JADER are also taken into account15. In fact, complementing information from one database with the other will provide a better understanding of the discrepancy in adverse events between Japan and other countries, and thus ensure a more targeted approach in clinical practice16,31. Supporting the use of both databases and confirming the reliability of this study, it should be noted that the present results are similar in spite of different patient backgrounds. Thus, pharmaco-epidemiological studies using databases, such as JADER and FAERS, offer excellent tools for detecting trends on adverse drug reactions and preventive medications. However, the present study has some limitations that need to be considered. It should be kept in mind that these data are derived from an observational study, not an analysis using RCTs, and the possibility of bias in reporting rates should be recognized. In addition, because the adverse event spontaneous reporting database is voluntary, it is not possible to capture all adverse events that occur. Furthermore, the lack of comprehensive medical records and medication histories limits the scope of the analysis, as the dosage and duration of use of NSAIDs and rebamipide are unknown.
Nevertheless, FAERS and JADER databases represent a rich and invaluable post-market resource for drug safety research. The huge number of cases obtained by using these databases is solid information and has been reported to be useful19,20,21,22. In this study, the combined use of NSAIDs and rebamipide eliminated the signals associated with lower gastrointestinal tract injury. This was consistent with the results of previous clinical studies, and we believe that it contains important findings. We believe that these findings can stimulate future research on rebamipide, ultimately helping to prevent or control serious complications, such as ulceration, bleeding, or perforation, caused by NSAID-induced lower gastrointestinal tract injury.
Methods
Data acquisition and preprocessing
FAERS data were downloaded from the FDA website (http://www.fda.gov/). The FAERS database contains data tables named 'DEMO', 'DRUG', 'REAC', 'OUTC', 'RPSR', 'THER', and 'INDI'. In this study, we used the DEMO, DRUG, and REAC files. The DEMO file contains basic patient information such as age, date of adverse event, and country of adverse event; the DRUG file contains the name of the drug, route of administration, and dose; and the REAC file contains the name of the adverse event. Microsoft Office Access 2016 was used to create the FAERS dataset used in this study. In the case of duplicate reports from the same patient, only the most recent adverse event was analyzed, in line with FDA recommendations. The JADER database was downloaded from the PMDA website (https://www.pmda.go.jp/index.html). It consists of four files: 'DEMO', 'DRUG', 'REAC', and 'HIST'; and data tables are divided by ID number. We included reports labeled as "suspicious drug" in the drug involvement section based on Hosomi et al.32. Multiple reports that were registered in the database in duplicate were deleted based on case information, and each case was regarded as one report.
Database search
All reports added to the FAERS and JADER databases between April 1, 2004 and March 31, 2016 were accessed and downloaded. The adverse event entries used for extraction were selected from the 39 terms corresponding to "lower gastrointestinal tract injury" in the Preferred Term (PT) of the ICH International Medical Dictionary for Regulatory Activities (MedDRA ver. 22.1): Rectal haemorrhage (PT 10038063), Anal haemorrhage (PT 10049555), Lower gastrointestinal haemorrhage (PT 10050953), Large intestinal haemorrhage (PT 10052534), Small intestinal haemorrhage (PT 10052535), Intestinal haemorrhage (PT 10059175), Mesenteric haemorrhage (PT 10060717), Anal ulcer (PT 10002180), Anorectal ulcer (PT 10002582), Rectal perforation (PT 10038073), Rectal ulcer (PT 10038080), Rectal ulcer haemorrhage (PT 10038081), Anal ulcer haemorrhage (PT 10063896) Anal erosion (PT 10067272), Duodenal perforation (PT 10013832), Duodenal ulcer (PT 10013836), Duodenal ulcer haemorrhage (PT 10013839), Duodenal ulcer perforation (PT 10013849), Erosive duodenitis (PT 10062532), Ulcerative duodenitis (PT 10080994), Ileal perforation (PT 10021305), Ileal ulcer (PT 10021309), Ileal ulcer perforation (PT 10021310), Intestinal perforation (PT 10022694), Intestinal ulcer (PT 10022714), Jejunal perforation (PT 10023174), Jejunal ulcer (PT 10023177), Jejunal ulcer perforation (PT 10023178), Large intestinal ulcer (PT 10023799), Large intestine perforation (PT 10023804), Small intestinal perforation (PT 10041103), Small intestine ulcer (PT 10041133), Large intestinal ulcer perforation (PT 10052497), Small intestinal ulcer perforation (PT 10052498), Intestinal ulcer perforation (PT 10061248), Large intestinal ulcer haemorrhage (PT 10061262), Small intestinal ulcer haemorrhage (PT 10061550), Large intestine erosion (PT 10076369), and Lower gastrointestinal perforation (PT 10078414).
Statistical analyses
The ROR is a widely used method in adverse drug event signal detection. It has been employed extensively in studies based on FAERS and JADER data15,16,17,18. When the lower limit of the 95% CI for the adjusted ROR was > 1, the adverse event was considered to be significantly more reported following use of the drug of interest compared to all other drugs. The ROR score is defined as \(\frac{A/B}{C/D}\), where ‘‘A’’ is the number of safety reports in patients who received rebamipide and manifested the NSAID-induced lower gastrointestinal tract injury adverse event; ‘‘B’’ is the number of safety reports, in which patients received rebamipide but did not present the NSAID-induced lower gastrointestinal tract injury adverse event; ‘‘C’’ is the number of safety reports, in which patients did not receive rebamipide and had the NSAID-induced lower gastrointestinal tract injury event; and ‘‘D’’ is the number of safety reports, in which patients did not receive rebamipide and did not present the NSAID-induced lower gastrointestinal tract injury adverse event.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Cryer, B. NSAID-associated deaths: The rise and fall of NSAID-associated GI mortality. Am. J. Gastroenterol. 100, 1694–1695 (2005).
Chan, F. K. L. NSAID-associated lower gastrointestinal bleeding: Where do we stand?. Clin. Gastroenterol. Hepatol. 10, 1060–1061 (2012).
Maiden, L., Thjodleifsson, B., Theodors, A., Gonzalez, J. & Bjarnason, I. A quantitative analysis of NSAID-induced small bowel pathology by capsule enteroscopy. Gastroenterology 128, 1172–1178 (2005).
Somasundaram, S. et al. Mitochondrial damage: A possible mechanism of the “topical” phase of NSAID induced injury to the rat intestine. Gut 41, 344–353 (1997).
Wallace, J. L. Mechanisms, prevention and clinical implications of nonsteroidal anti-inflammatory drug-enteropathy. World J. Gastroenterol. 19, 1861–1876 (2013).
Utzeri, E. & Usai, P. Role of non-steroidal anti-inflammatory drugs on intestinal permeability and nonalcoholic fatty liver disease. World J. Gastroenterol. 23, 3954–3963 (2017).
Arakawa, T., Watanabe, T., Fukuda, T., Yamasaki, K. & Kobayashi, K. Rebamipide, novel prostaglandin-inducer accelerates healing and reduces relapse of acetic acid-induced rat gastric ulcer. Comparison with cimetidine. Dig. Dis. Sci. 40, 2469–2472 (1995).
Park, S. C., Chun, H. J., Kang, C. D. & Sul, D. Prevention and management of non-steroidal anti-inflammatory drugs-induced small intestinal injury. World J. Gastroenterol. 17, 4647–4653 (2011).
Naito, Y. et al. Hydroxyl radical scavenging by rebamipide and related compounds: Electron paramagnetic resonance study. Free Radic. Biol. Med. 18, 117–123 (1995).
Niwa, Y. et al. Efficacy of rebamipide for diclofenac-induced small-intestinal mucosal injuries in healthy subjects: A prospective, randomized, double-blinded, placebo-controlled, cross-over study. J. Gastroenterol. 43, 270–276 (2008).
Ito, Y. et al. Nonsteroidal anti-inflammatory drug-induced visible and invisible small intestinal injury. J. Clin. Biochem. Nutr. 53, 55–59 (2013).
Fujimori, S. et al. Rebamipide has the potential to reduce the intensity of NSAID-induced small intestinal injury: A double-blind, randomized, controlled trial evaluated by capsule endoscopy. J. Gastroenterol. 46, 57–64 (2011).
Beaulieu-Jones, B. K. et al. Examining the use of real-world evidence in the regulatory process. Clin. Pharmacol. Ther. 107, 843–852 (2020).
Roberts, M. H. & Ferguson, G. T. Real-world evidence: Bridging gaps in evidence to guide payer decisions. Pharmacoecon. Open. 5, 3–11 (2021).
Ando, G. et al. Evaluation of the expression time of ganciclovir-induced adverse events using JADER and FAERS. Biol. Pharm. Bull. 42, 1799–1804 (2019).
Sasaoka, S. et al. Evaluation of the association of hand-foot syndrome with anticancer drugs using the US Food and Drug Administration Adverse Event Reporting System (FAERS) and Japanese Adverse Drug Event Report (JADER) Databases. Yakugaku Zasshi 136, 507–515 (2016).
Hatahira, H. et al. Drug-induced gingival hyperplasia: A retrospective study using spontaneous reporting system databases. J. Pharm. Health Care Sci. 19, 3–19 (2017).
Shimada, K. et al. Adverse reaction profiles of hemorrhagic adverse reactions caused by direct oral anticoagulants analyzed using the Food and Drug Administration Adverse Event Reporting System (FAERS) database and the Japanese Adverse Drug Event Report (JADER) database. Int. J. Med. Sci. 16, 1295–1303 (2019).
Franklin, J. M. & Schneeweiss, S. When and how can real world data analyses substitute for randomized controlled trials?. Clin. Pharmacol. Ther. 102, 924–933 (2017).
Xu, D. et al. MSBIS: A multi-step biomedical informatics screening approach for identifying medications that mitigate the risks of metoclopramide-induced tardive dyskinesia. EBioMedicine 26, 132–137 (2017).
Zhao, S. et al. Systems pharmacology of adverse event mitigation by drug combinations. Sci. Transl. Med. 5, 140–206 (2013).
Nagashima, T., Shirakawa, H., Nakagawa, T. & Kaneko, S. Prevention of antipsychotic-induced hyperglycaemia by vitamin D: A data mining prediction followed by experimental exploration of the molecular mechanism. Sci. Rep. 6, 26375 (2016).
Manabu, A. & Kaori, N. Impact of database differences on drug safety considerations: Data mining of the FDA Adverse Event Reporting System and Japanese Adverse Drug Event Report Database. Jpn. J. Drug Inform. 18, N6–N11 (2016).
Sostres, C., Gargallo, C. J. & Lanas, A. Nonsteroidal anti-inflammatory drugs and upper and lower gastrointestinal mucosal damage. Arthritis. Res. Ther. 15(Suppl 3), S3 (2013).
Lanas, A. et al. Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. Am. J. Gastroenterol. 104, 1633–1641 (2009).
Fujimori, S. et al. Prevention of nonsteroidal anti-inflammatory drug-induced small-intestinal injury by prostaglandin: A pilot randomized controlled trial evaluated by capsule endoscopy. Gastrointest. Endosc. 69, 1339–1346 (2009).
Graham, D. Y., Opekun, A. R., Willingham, F. F. & Qureshi, W. A. Visible small-intestinal mucosal injury in chronic NSAID users. Clin. Gastroenterol. Hepatol. 3, 55–59 (2005).
Tanigawa, T. et al. Rebamipide inhibits indomethacin-induced small intestinal injury: Possible involvement of intestinal microbiota modulation by upregulation of α-defensin 5. Eur. J. Pharmacol. 704, 64–69 (2013).
Diao, L. et al. Rebamipide suppresses diclofenac-induced intestinal permeability via mitochondrial protection in mice. World J. Gastroenterol. 18, 1059–1066 (2012).
Hosomi, K., Arai, M., Fujimoto, M. & Takada, M. Applied data mining of the FDA adverse event reporting system, FAERS, and the Japanese Adverse Drug Event Report Database, JADER: Signal detection of adverse events by new quinolones. Jpn. J. Drug Inform. 17, 15–20 (2015).
Matsui, T. et al. Adverse event signals of interstitial lung disease in the FDA adverse event reporting system (FAERS) database and the Japanese adverse drug event report (JADER) database. Jpn. J. Drug Inform. 17, 145–154 (2015).
Hosomi, K., Park, B., Inose, R., Fujimoto, M. & Takada, M. Association between antipsychotic use and extrapyramidal symptoms: Data mining of the FDA adverse event reporting system and japanese adverse drug event report database. Jpn. J. Drug Inform. 17, 125–132 (2015).
Acknowledgements
We thank Shinsaku Washinosu for contributions to processing the FAERS and JADER data files and supporting the computer environment.
Author information
Authors and Affiliations
Contributions
T.I. and K.H. designed the research. T.I. and K.H. wrote the article. T.I., K.H. and S.S. collected the data. T.I. and K.H. performed data analysis. T.I., K.H., Y.K., S.S. and S.O. contributed to data interpretation and intellectual content. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Imai, T., Hazama, K., Kosuge, Y. et al. Preventive effect of rebamipide on NSAID-induced lower gastrointestinal tract injury using FAERS and JADER. Sci Rep 12, 2631 (2022). https://doi.org/10.1038/s41598-022-06611-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-022-06611-y
This article is cited by
-
A multidimensional assessment of adverse events associated with paliperidone palmitate: a real-world pharmacovigilance study using the FAERS and JADER databases
BMC Psychiatry (2025)
-
Association Between Melatonin Receptor Agonists and Cardiac Arrhythmia; Disproportionality Analysis Studies Using Pharmacovigilance Databases
Cardiovascular Toxicology (2025)
-
Evaluation of tolvaptan-associated hepatic disorder using different national pharmacovigilance databases
Scientific Reports (2024)
-
Berberine mitigates diclofenac-induced intestinal mucosal mechanical barrier dysfunction through the restoration of autophagy by inhibiting exosome-mediated lncRNA H19
Inflammopharmacology (2024)
-
Chrysin mitigates diclofenac-induced hepatotoxicity by modulating oxidative stress, apoptosis, autophagy and endoplasmic reticulum stress in rats
Molecular Biology Reports (2023)
