
Abstract
It is unclear which factors are associated with progressive sinus node dysfunction after cavotricuspid isthmus (CTI)-dependent atrial flutter (AFL) ablation. We sought to evaluate the incidence and predictors for permanent pacemaker (PPM) implantation after CTI-dependent AFL ablation. Between January 2011 and June 2021, 353 patients underwent CTI-dependent AFL ablation were studied. During a median follow-up of 31.6 months, 30 patients (8.5%) received PPM implantation, 24 for sick sinus syndrome and 6 for atrioventricular block. In multivariable model, prior atrial fibrillation (AF) (HR 3.570; 95% CI 1.034–12.325; P = 0.044), lowest previous sinus heart rate (HR 0.942; 95% CI 0.898–0.988; P = 0.015), and left atrial volume index (LAVI) (HR 1.067; 95% CI 1.024–1.112; P = 0.002) were independently associated with PPM implantation after CTI-dependent AFL ablation. The best cut-off points for predicting PPM implantation were 60.1 ml/m2 for LAVI and 46 beats per minute for lowest previous sinus heart rate. Among the patients discharged without PPM implantation after ablation, sinus pause over three seconds at AFL termination during ablation was an independent predictor of PPM implantation (HR 17.841; 95% CI 4.626–68.807; P < 0.001). Physicians should be aware of the possibility of PPM implantation during follow-up after AFL ablation, especially in patients with the relevant risk factors.
Similar content being viewed by others

Introduction
Previous studies have shown the clinical association between atrial tachyarrhythmia and sinus node dysfunction (SND)1,2,3. Both diseases are associated with structural and electrical atrial remodeling and stretched atria4. Patients with atrial fibrillation (AF) or atrial flutter (AFL) showed atrial remodeling, characterized by low voltage areas, slow conduction, and a reduction in atrial refractoriness5,6,7. Similarly, diffuse atrial and sinus node remodeling with structural changes and conduction abnormalities were also observed in patients with SND8. Furthermore, atrial tachyarrhythmia may directly impair sinus node function9,10. Importantly, previous studies demonstrated that SND might be recovered after catheter ablation for atrial tachyarrhythmia in patients with AF or AFL5,11. Considering reverse remodeling, the current guidelines recommended AF catheter ablation in patients with AF-related bradycardia to avoid permanent pacemaker (PPM) implantation12. However, even after AF catheter ablation, 8–11% of patients with AF and SND required PPM implantation during follow-up, and several studies have reported long sinus pause at the termination of AF, anterior line ablation, and high E/e’ as risk factors for progressive SND13,14,15.
The possibility of PPM implantation after AFL ablation may be commonly underestimated, unlike that of AF, since AFL is effectively treated by cavotricuspid isthmus (CTI) ablation, and CTI ablation can be performed at less equipped electrophysiology laboratories. However, some reported that patients that underwent AFL ablation were more likely to receive PPM implantations during follow-up compared with those who underwent AF ablation. Moreover, the predictors associated with irreversible or progressive SND after AFL ablation have not been reported16,17. Therefore, we sought to evaluate the incidence of and predictors for PPM implantation after CTI-dependent AFL catheter ablation.
Methods
Study population
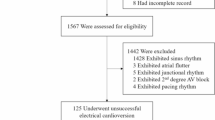
We enrolled 515 consecutive patients who underwent AFL catheter ablation at the Samsung Medical Center (Seoul, Korea) between January 2011 and June 2021. All enrolled patients had symptomatic or drug-refractory AFL documented on electrocardiogram (ECG). Patients under the age of 18 (n = 2) and those with atypical AFL (n = 39), a previous history of AF catheter ablation (n = 37), a previous history of thoracoscopic AF ablation or Maze operation (n = 45), previous PPM implantation (n = 23), and follow-up loss (n = 16) were excluded. Finally, a total of 353 patients were selected for the current study. Among them, 30 patients underwent PPM implantation during the follow-up period (Fig. 1). The Institutional Review Board of Samsung Medical Center approved this study and waived the requirement for written informed consent. The study protocol complied with the Declaration of Helsinki.

Study flow. AF atrial fibrillation, CTI cavotricuspid isthmus, PPM permanent pacemaker, RFCA radiofrequency catheter ablation.
AFL catheter ablation procedure
All antiarrhythmic medications were withheld for at least 5 half-lives prior to the ablation procedure. The procedure was performed under conscious sedation. A duodecapolar catheter was placed into the right atrium and coronary sinus, and a His-RV catheter was placed into the His area and right ventricle apex. All catheters were inserted through the femoral vein. The surface ECG and bipolar intracardiac electrogram were simultaneously monitored and recorded. Regarding CTI ablation, an 8 Fr long sheath (RAMP or SL1, St. Jude Medical, Minneapolis, MN, USA) and a 3.5 mm tip open irrigated ablation catheter (Thermo-Cool, Bidirectional catheter, Biosense Webster, Irvine, CA, USA) were used. While radiofrequency energy was applied for 60 s with 30 watts by point, the ablation catheter was continuously pulled back along the CTI line from the side of the right ventricle to the right atrium and inferior vena cava junction. The endpoint of ablation was bidirectional electrical block confirmed by the presence of parallel and widely split (> 110 ms) double potentials along the CTI as well as activation sequence reversal when pacing from the opposite site across the CTI. If a bidirectional block was not achieved, conduction gaps were ablated, or additional line ablation was performed.
Data collection, follow-up, and study outcomes
Baseline characteristics, 12-lead ECG, Holter ECG, echocardiography, intracardiac electrogram during the index ablation, and clinical outcome data were prospectively collected in our ablation registry by trained research coordinators using a standardized case report form and protocol. Previous 12-lead and Holter ECG findings were analyzed based on the ECGs performed within 1 year before the index ablation. AFL was considered persistent if it sustained for at least 1 week. Prior AF was defined by the presence of documented 12-lead ECG or AF > 30 s on Holter ECG. Previous echocardiographic findings were assessed based on the most recently performed echocardiography within a year prior to the index ablation. Most of the echocardiography (70.0%) included in the current study were performed one month prior to the index ablation. Left atrial (LA) volume was measured using the biplane area-length method, and the LA volume index (LAVI) was then derived by dividing LA volume by body surface area18. Left ventricular ejection fraction (LVEF) was assessed using the biplane Simpson’s method. Patients were routinely followed up at 1, 3, 6, and 12 months after the index procedure and biannually thereafter. Further information was collected by telephone contact or medical records if necessary. During follow-up, PPM implantation was performed when clinically indicated, based on the current guidelines19. The primary outcome was PPM implantation after CTI-dependent AFL catheter ablation. The secondary outcome was future PPM implantation among the patients discharged without PPM implantation after CTI-dependent AFL catheter ablation.
Statistical analysis
Continuous variables were analyzed using the unpaired t-test or Mann–Whitney rank-sum test and were presented as means and standard deviations or medians with interquartile ranges according to their distributions, which were checked using the Kolmogorov–Smirnov test and visual inspection of Q-Q plots. All discrete and categorical variables were presented as numbers and relative frequencies (percentages) and compared using the chi-square test or Fisher’s exact test. Cox proportional hazards regression analysis was used to calculate hazard ratios (HRs) with 95% confidence intervals (CIs) to find independent predictors for PPM implantation. Multivariable Cox proportional hazard regression models were constructed using variables with a P value < 0.10 in univariable analyses. The receiver operating characteristic curve was constructed to determine the best cut-off values of LAVI and the previous lowest sinus heart rate for predicting PPM implantation after ablation. The cumulative incidence of PPM implantation was presented as a Kaplan–Meier estimate and compared using a log-rank test or Breslow test. As a sensitivity analysis, we also assessed the independent predictors for PPM implantation for sick sinus syndrome (SSS) or atrioventricular block and for PPM implantation within 1 year of CTI-dependent AFL catheter ablation using multivariable Cox regression analysis. All analyses were two-tailed, and statistical significance was defined as P < 0.05. Statistical analyses were performed using SPSS 25.0 for Windows (SPSS-PC, Chicago, IL, USA) and R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline patient and procedural characteristics
Among a total of 353 patients, 30 patients (8.5%) received PPM implantation during follow-up. The median follow-up duration was 31.6 months (interquartile range: 11.8–63.0 months). The baseline patient and procedural characteristics are presented in Table 1. Patients who underwent PPM implantation were more likely to be women and had a higher prevalence of previous stroke and AF compared to those without PPM implantation. Moreover, CHA2DS2-VASc scores were significantly higher in the patients who underwent PPM implantation. The type of AFL was not significantly different between the patients who underwent PPM and those that did not. In ECG findings prior to the index ablation, compared to patients without PPM implantation, those who received PPM implantation showed significantly lower heart rates at both sinus and AFL rhythms and higher PR intervals. The prevalence of prior sinus pauses longer than 3 seconds was higher in the patients who received PPM implantation. In echocardiographic findings before the index ablation, LAVI was significantly greater in the PPM group compared to the no PPM group. Other parameters, including LVEF, E/e’, and right ventricular systolic pressure were not significantly different depending on PPM implantation. Acute ablation success rates and HV interval were comparable between the patients who underwent PPM and those that did not. Among the cases in which AFL was terminated during CTI ablation, sinus pauses over three seconds at AFL termination were frequently observed in the PPM group. Type of antiarrhythmic agent used after ablation were similar between the two groups. During follow-up, CTI-dependent AFL recurrence rates were not significantly different between the two groups (10.0% vs. 7.4%, P = 0.883). However, patients who underwent PPM implantation showed significantly higher AF occurrence rates after AFL ablation compared to those without PPM implantation (56.7% vs. 31.6%, P = 0.010).
PPM implantation
The median time to PPM implantation from AFL ablation was 57 days (interquartile range: 1–854 days). Among 30 patients who received PPM implantation, 24 patients (80%) underwent PPM for SSS, and six patients (20%) underwent PPM for atrioventricular block (Table 2). 18 patients (60%) received PPM implantation within a year of ablation. The time until PPM implantation after AFL ablation is presented in Supplemental Figure. Most patients received dual-chamber PPM, but only one patient underwent leadless pacemaker implantation due to arteriovenous fistula for hemodialysis.
Independent predictors for PPM implantation
According to multivariable Cox regression analysis, prior AF (HR 3.570; 95% CI 1.034–12.325; P = 0.044), lowest previous sinus heart rate (HR 0.942; 95% CI 0.898–0.988; P = 0.015), and LAVI (HR 1.067; 95% CI 1.024–1.112; P = 0.002) were independently associated with PPM implantation after CTI-dependent AFL ablation (Table 3). The best cut-off points for predicting PPM implantation were 60.1 ml/m2 for LAVI and 46 beats per minute for the lowest previous sinus heart rate (Fig. 2). The patients with prior AF had significantly higher risk of PPM implantation after AFL ablation compared to those without prior AF (P = 0.031) (Fig. 3). The incidence of PPM implantation after AFL ablation was significantly higher in patients had LAVI > 60.1 ml/m2 than in patients had LAVI ≤ 60.1 ml/m2 (P < 0.001). The patients with the lowest previous sinus heart rate < 46 beats per minute had significantly higher risk of PPM implantation after AFL ablation compared to those with the lowest previous sinus heart rate ≥ 46 beats per minute (P < 0.001). Female sex (HR 4.310; 95% CI 1.248–14.882; P = 0.021) was an independent predictor of PPM implantation for sick sinus syndrome (Supplemental Table 1), but was not significantly associated with overall PPM implantation. Prior AF, lowest previous sinus heart rate, and LAVI were also independently associated with PPM implantation for SSS (Supplemental Table 1). However, there were no significant predictors regarding PPM implantation for atrioventricular block (Supplemental Table 2). In the sensitivity analysis, the lowest previous sinus heart rate and LAVI emerged as independent predictors of PPM implantation within a year of AFL ablation, but female sex and prior AF did not (Supplemental Table 3).

Best cut-off value of LAVI and the lowest previous sinus heart rate for the prediction of PPM implantation after CTI-dependent AFL ablation. Best cut-off value of LAVI and the lowest previous sinus heart rate to predict the risk of PPM implantation after CTI-dependent AFL ablation which was evaluated by the maximally selected log-rank statistics method. (A) The best cut-off value of LAVI was > 60.1 ml/m2 (B) The best cut-off value of the lowest previous sinus heart rate was < 46 beats per minute. AFL atrial flutter, CTI cavotricuspid isthmus, LAVI left atrial volume index, PPM permanent pacemaker.

Kaplan–Meier Estimates of the Incidence of PPM Implantation after CTI-dependent AFL ablation. (A) Kaplan–Meier curves for PPM implantation after AFL ablation in overall population. (B) Kaplan–Meier curves for PPM implantation after AFL ablation according to the presence of prior AF. (C) Kaplan–Meier curves for PPM implantation after AFL ablation according to LAVI (cut-off value: 60.1 ml/m2). (D) Kaplan–Meier curves for PPM implantation after AFL ablation according to the lowest previous sinus heart rate (cut-off value: 46 beats per minute). AF atrial fibrillation, AFL atrial flutter, CTI cavotricuspid isthmus, LAVI left atrial volume index, PPM permanent pacemaker.
Among the patients discharged without PPM implantation after AFL ablation, a sinus pause over three seconds at AFL termination during ablation was significantly associated with a higher risk of future PPM implantation (multivariable HR 17.841; 95% CI 4.626–68.807; P < 0.001) (Table 4).
Discussion
The present study evaluated the incidence of and predictors for PPM implantation after CTI-dependent AFL ablation. The major findings are as follows. First, after CTI ablation, 8.5% of patients received PPM implantation (6.8% for SSS and 1.7% for atrioventricular block) during a median follow-up period of 31.6 months. Second, prior AF, lowest previous sinus heart rate, and LAVI were independently associated with the risk of future PPM implantation after CTI ablation. Female sex was an independent predictor of PPM implantation for SSS. Third, the best cut-off values for prediction of PPM implantation were 60.1 ml/m2 for LAVI and 46 beats per minute for the lowest previous sinus heart rate. Fourth, among the patients discharged without PPM implantation after ablation, sinus pause over three seconds at AFL termination during ablation was an independent predictor of PPM implantation.
Atrial remodeling is considered a common mechanism for the development of atrial tachyarrhythmia and SND4. Importantly, atrial tachyarrhythmia (especially AF and AFL) itself may worsen sinus node function by atrial structural fibrosis, electrical remodeling, and molecular changes5,9,10,20. In patients with AF, atrial fibrosis with low voltage near the sinus node area was associated with SND9. AFL patients showed significant depression of sinus node automaticity and sinoatrial conduction5. In dogs that underwent atrial tachypacing, ion channel expression in sinoatrial node cells was significantly downregulated with alteration in the funny current10. Fortunately, atrial remodeling and SND can be reversed by ablation for AF and AFL5,11. In this regard, AF catheter ablation for patients with AF-related bradycardia has been incorporated into clinical practice and the current guidelines12. However, 8–11% of patients with AF and SND underwent PPM implantation during follow-up even after successful AF catheter ablation13,14,15. Some studies have reported long sinus pause on the termination of AF, anterior line ablation, and E/e’ to be independent predictors for PPM implantation after AF ablation in patients with AF and SND14,15. Contrary to AF catheter ablation, limited data are available regarding the incidence and risk factors for PPM implantation after CTI-dependent AFL ablation.
In the present study, 8.5% of patients received PPM implantation after CTI-dependent AFL ablation, and the main indication was SSS. Interestingly, this rate was comparable to the PPM implantation rate after AF catheter ablation in patients with AF and SND from previous studies (8–11%)13,14,15. Considering most patients in the present study did not have significant SND prior to AFL ablation, we assumed that patients who underwent CTI-dependent AFL ablation received more PPM implantation during follow-up compared with those who underwent AF catheter ablation. This finding is in line with a prior nationwide population-based study which showed that 8.4% of patients underwent PPM implantation during long-term follow-up after CTI-dependent AFL ablation, and PPM implantations were more frequent following AFL ablation than AF ablation16. However, since the follow-up period of the present study was shorter (median 31.6 months) that that of the previous nationwide study (mean 5.5 years), the incidence of PPM implantation after CTI ablation in the present study was higher than expected. Because the hospital where the present study was conducted is a tertiary referral hospital, it is likely that patients with longer duration of AFL and who had advanced atrial remodeling were included in this study. Medi et al. reported that patients with AFL showed more advanced remodeling in the posterior right atrium than patients with AF, and this finding might be associated with a higher rate of PPM implantation in patients who underwent AFL ablation than those who underwent AF ablation7. Complete atrioventricular block (CAVB) occurred in 1.1% (4/353) of all enrolled patients. Among them, three patients were diagnosed with CAVB shortly after CTI ablation and underwent PPM implantation during the index hospitalization. These patients showed AFL with regular slow ventricular rate (35–45 beats per minute) on 12-lead ECG just before the CTI ablation, and it was finally confirmed that the patients' rhythm was CAVB during electrophysiology study for CTI ablation. In other words, there was no case where CTI ablation directly affected atrioventricular node conduction.
The identification of risk factors for irreversible and progressive SND after AFL ablation is of great importance to the prevention of adverse events like syncope and sudden cardiac death. The present study demonstrated that prior AF, slow intrinsic sinus heart rate, and large left atrial volume significantly increased the risk of PPM implantation after AFL ablation. In this study, AF occurrence after CTI ablation was significantly higher in the patient with prior AF than without prior AF (46.4% vs. 25.4%, P < 0.001). Seara et al. also showed that prior AF was an independent predictor of transition to AF after CTI-dependent AFL ablation (HR 2.55; 95% CI 1.85–3.52, P < 0.001)21. Previous studies showed that enlarged LA volume was associated with a significantly increased risk of incident AF after CTI-dependent AFL ablation22,23. Based on these findings, the higher occurrence of AF after AFL ablation in patients with prior AF or enlarged LA volume might exacerbate SND, which results in PPM implantation during follow-up. Actually, the PPM group showed significantly higher AF occurrence rate after CTI ablation than the no PPM group. In this context, more intensive monitoring of AF occurrence after AFL ablation in patients with prior AF or enlarged LA volume may help avoid PPM implantation by providing an opportunity for early AF catheter ablation. While 39.7% of enrolled patients had documented AF before CTI ablation, CTI-dependent AFL was dominant and AF was rarely documented (less than 3 times of paroxysmal AF event) in these patients. Since CTI ablation is relatively simple procedure than AF ablation and AF ablation is generally recommended as a second-line therapy after failure of antiarrhythmic agents12, in the patients with typical AFL with rarely documented paroxysmal AF, we performed CTI ablation first, and then, if symptomatic AF occurred during follow-up even with antiarrhythmic agent use, we proceed AF ablation. However, considering higher AF occurrence in patients with prior AF, AF ablation at the time of CTI ablation might reduce sinus node dysfunction. Further research is warranted to confirm whether catheter ablation for AF and AFL together in the patients with typical AFL with rarely documented paroxysmal AF reduces the risk of future PPM implantation.
Additionally, the lowest previous sinus heart rate and LAVI emerged as independent predictors of relatively early PPM implantation within a year of AFL ablation in the present study. This finding suggests that patients with lower intrinsic sinus heart rate (less than 46 per minute) or greater LAVI (over 60.1 ml/m2) might have extensive and irreversible atrial remodeling24. A gender difference in the indications for PPM implantation has been shown in previous large registry studies consistently reporting female patients to have more SSS and fewer atrioventricular blocks compared to male patients25,26,27. This finding is line with the result of the present study. The mechanism of this gender disparity remains unclear, but differences in electrophysiological properties and the effects of sex hormones on ion channels might be associated with this finding28. Interestingly, there was a large difference in the incidence of sinus pause between before and at the time of CTI ablation. This could be explained in two ways. First, since the majority of enrolled patients had persistent AFL, sinus pause could not be detected before the CTI ablation. Thus, sinus pause was revealed after AFL termination by CTI ablation in patients with persistent AFL. Second, since the patients' rhythm was assessed intermittently with 12-lead ECG or holter at the outpatient clinic, the detection rate of sinus pause might have been low.
CTI ablation for AFL is commonly considered an effective and safe procedure. However, physicians should be aware of the possibility of PPM implantation during follow-up after AFL ablation, especially in patients with the relevant risk factors.
Study limitations
Some limitations of the present study should be acknowledged. First, the study was a small-numbered, observational, single-center study. Potential selection bias could have influenced the study outcome. Second, the timing of echocardiography analyzed in the study was different for each patient because previous echocardiographic findings were assessed based on the most recently performed echocardiography during a year prior to the index ablation. However, most of the echocardiography (70.0%) included in the current study were performed 1 month prior to the index ablation. Third, there could be inter-operator variability in the measurement of echocardiographic parameters, including LAVI. Fourth, we did not have direct information regarding AFL or AF duration.
Conclusion
In patients who underwent CTI-dependent AFL ablation, prior AF, slow intrinsic sinus heart rate, and large left atrial volume were independent predictors for future PPM implantation. Patients with predisposing factors for irreversible and progressive SND should be carefully monitored after AFL ablation.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Ferrer, M. I. The sick sinus syndrome in atrial disease. JAMA 206, 645–646 (1968).
Lamas, G. A. et al. The mode selection trial (MOST) in sinus node dysfunction: Design, rationale, and baseline characteristics of the first 1000 patients. Am. Heart J. 140, 541–551. https://doi.org/10.1067/mhj.2000.109652 (2000).
Yang, P. S. et al. Risk of sick sinus syndrome in patients diagnosed with atrial fibrillation: A population-based cohort. J. Cardiovasc. Electrophysiol. 32, 2704–2714. https://doi.org/10.1111/jce.15202 (2021).
Lee, J. M. & Kalman, J. M. Sinus node dysfunction and atrial fibrillation: Two sides of the same coin?. Europace 15, 161–162. https://doi.org/10.1093/europace/eus223 (2013).
Sparks, P. B., Jayaprakash, S., Vohra, J. K. & Kalman, J. M. Electrical remodeling of the atria associated with paroxysmal and chronic atrial flutter. Circulation 102, 1807–1813. https://doi.org/10.1161/01.cir.102.15.1807 (2000).
Teh, A. W. et al. Electroanatomic remodeling of the left atrium in paroxysmal and persistent atrial fibrillation patients without structural heart disease. J. Cardiovasc. Electrophysiol. 23, 232–238. https://doi.org/10.1111/j.1540-8167.2011.02178.x (2012).
Medi, C. et al. Right atrial remodeling is more advanced in patients with atrial flutter than with atrial fibrillation. J. Cardiovasc. Electrophysiol. 23, 1067–1072. https://doi.org/10.1111/j.1540-8167.2012.02364.x (2012).
Sanders, P. et al. Electrophysiological and electroanatomic characterization of the atria in sinus node disease: Evidence of diffuse atrial remodeling. Circulation 109, 1514–1522. https://doi.org/10.1161/01.CIR.0000121734.47409.AA (2004).
Chang, H. Y. et al. Sinus node dysfunction in atrial fibrillation patients: The evidence of regional atrial substrate remodelling. Europace 15, 205–211. https://doi.org/10.1093/europace/eus219 (2013).
Yeh, Y. H. et al. Funny current downregulation and sinus node dysfunction associated with atrial tachyarrhythmia: A molecular basis for tachycardia-bradycardia syndrome. Circulation 119, 1576–1585. https://doi.org/10.1161/CIRCULATIONAHA.108.789677 (2009).
Hocini, M. et al. Reverse remodeling of sinus node function after catheter ablation of atrial fibrillation in patients with prolonged sinus pauses. Circulation 108, 1172–1175. https://doi.org/10.1161/01.CIR.0000090685.13169.07 (2003).
Hindricks, G. et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 42, 373–498. https://doi.org/10.1093/eurheartj/ehaa612 (2021).
Inada, K. et al. The role of successful catheter ablation in patients with paroxysmal atrial fibrillation and prolonged sinus pauses: outcome during a 5-year follow-up. Europace 16, 208–213. https://doi.org/10.1093/europace/eut159 (2014).
Hwang, T. H. et al. Permanent pacemaker implantations after catheter ablation in patients with atrial fibrillation associated with underlying sinus node dysfunction. Korean Circ. J. 50, 346–357. https://doi.org/10.4070/kcj.2019.0268 (2020).
Kim, D. H. et al. Long-term clinical outcomes of catheter ablation in patients with atrial fibrillation predisposing to tachycardia-bradycardia syndrome: a long pause predicts implantation of a permanent pacemaker. BMC Cardiovasc. Disord. 18, 106. https://doi.org/10.1186/s12872-018-0834-0 (2018).
Skjoth, F. et al. Disease progression after ablation for atrial flutter compared with atrial fibrillation: A nationwide cohort study. Int. J. Clin. Pract. 72, e13258. https://doi.org/10.1111/ijcp.13258 (2018).
Takahira, H. et al. Pathophysiological background and prognosis of common atrial flutter in non-elderly patients: Comparison to atrial fibrillation. J. Cardiol. 78, 362–367. https://doi.org/10.1016/j.jjcc.2021.05.008 (2021).
Lang, R. M. et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 28, 1–39. https://doi.org/10.1016/j.echo.2014.10.003 (2015).
Glikson, M. et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 42, 3427–3520. https://doi.org/10.1093/eurheartj/ehab364 (2021).
Burstein, B. & Nattel, S. Atrial fibrosis: Mechanisms and clinical relevance in atrial fibrillation. J. Am. Coll. Cardiol. 51, 802–809. https://doi.org/10.1016/j.jacc.2007.09.064 (2008).
Seara, J. G. et al. Risk of atrial fibrillation, stroke, and death after radiofrequency catheter ablation of typical atrial flutter. Clin. Res. Cardiol. 103, 543–552. https://doi.org/10.1007/s00392-014-0682-6 (2014).
Li, J. H. et al. Risk of new-onset atrial fibrillation post-cavotricuspid isthmus ablation in typical atrial flutter without history of atrial fibrillation. Front. Physiol. 12, 763478. https://doi.org/10.3389/fphys.2021.763478 (2021).
Rzucidlo, J. et al. Elevated left atrial volume index predicts incident atrial fibrillation after typical right atrial flutter ablation. J. Atr. Fibrillation 14, 20200485. https://doi.org/10.4022/jafib.20200485 (2021).
John, R. M. & Kumar, S. Sinus node and atrial arrhythmias. Circulation 133, 1892–1900. https://doi.org/10.1161/CIRCULATIONAHA.116.018011 (2016).
Chen, R. H. et al. The gender difference of utilization of cardiac implantable electronic device in China: Data from Arrhythmia Interventional Therapy Data Registry. J. Geriatr. Cardiol. 15, 310–314. https://doi.org/10.11909/j.issn.1671-5411.2018.04.010 (2018).
Eccleston, D. et al. Sex differences in Cardiac electronic device implantation: Outcomes from an Australian multi-centre clinical quality registry. Int. J. Cardiol. Heart Vasc. 35, 100828. https://doi.org/10.1016/j.ijcha.2021.100828 (2021).
Nowak, B. et al. Do gender differences exist in pacemaker implantation?–results of an obligatory external quality control program. Europace 12, 210–215. https://doi.org/10.1093/europace/eup312 (2010).
Linde, C. et al. Sex differences in cardiac arrhythmia: a consensus document of the European Heart Rhythm Association, endorsed by the Heart Rhythm Society and Asia Pacific Heart Rhythm Society. Europace 20, 1565. https://doi.org/10.1093/europace/euy067 (2018).
Author information
Authors and Affiliations
Contributions
The study was designed by J.K., S.H.L., H.R.K., and K.-M.P., Data collection were made by J.K., S.H.L., T.-W.C., J.-H.C., J.Y.K., S.-J.P., Y.K.O., J.S.K. and K.-M.P., Statistical analysis was performed by J.K., S.H.L., H.R.K., T.-W.C., and K.-M.P., The manuscript was drafted by J.K., S.H.L., and K.-M.P., Critical revision of the manuscript for key intellectual content was made by J.K., S.H.L., J.-H.C., J.Y.K., S.-J.P., Y.K.O., J.S.K. and K.-M.P., All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, J., Lee, S.H., Kim, H.R. et al. Predictors of permanent pacemaker implantation after sinus conversion of cavotricuspid isthmus-dependent atrial flutter. Sci Rep 12, 5336 (2022). https://doi.org/10.1038/s41598-022-09439-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-022-09439-8
