
Abstract
This case–control study aimed to assess the effect of drinking water nitrate on serum nitric oxide concentration and the risk of metabolic syndrome (MetS) in the population in the Middle East. The study included 50 control and 50 thyroid disorder cases who were referred to two medical centers in 2021. In this study, serum nitric oxide concentration, drinking water nitrate, and metabolic syndrome components were measured in the two groups. The results showed there was a statistically significant difference between serum NO in the case and control groups (p-value < 0.001). There was a positive correlation between the concentration of nitrate in drinking water and serum nitric oxide in the case and control groups; however, this relationship was not significant statistically. A statistically significant difference was found between serum nitric oxide and systolic blood pressure in the cases (p-value < 0.05), but there was no significant difference between MetS and nitric oxide. Therefore, we concluded that the relationship between nitric oxide and nitrate in consuming water should be determined in thyroid patients. In addition to their water consumption, it is better to study the nitrate of foods, especially vegetables.
Similar content being viewed by others

Introduction
Nitrate and nitrite levels are currently increasing due to the excessive use of fertilizers and industrial development1. Nitrate is a common contaminant in drinking water, especially in agricultural areas where the use of nitrogen fertilizers has increased its concentration in drinking water sources since the 1950s2,3,4. In addition to agriculture, leachate from the waste accumulation and pollution due to human and animal wastes cause a considerable increase in nitrate concentration in the surface and groundwater5.
Nitrate is unstable in the human body and metabolized by human enzymes. Nitrate reduction activities by bacteria may convert nitrate to nitrite and other nitrogen compounds, which affects the physiological state and human health. After consumption, nitrate absorbed by the upper gastrointestinal tract easily. More than 25% of it is excreted into the saliva, and 20% is transformed to nitrite by oral bacteria6. Under acidic conditions in the stomach, nitrite is altered to nitrogen trioxide (N2O3), nitric oxide (NO), and nitrogen dioxide (NO2) as the nucleus of nitric acid (HNO2)7. Nitric oxide is a lipophilic molecule that is involved in various physiological and pathophysiological processes8,9 and is also the first gas molecule to be described as a mediator in signaling pathways10. Recent evidence suggests that NO is involved in the adjustment of thyroid function11 and perhaps in the thyroid arteries and blood flow adjustment12. Nitric oxide (NO), hydroxyl radical (OH), superoxide anion (O2−), and hydrogen peroxide (H2O2) are free radicals that are considered oxidative stress13. Oxidative stress is a general term used to describe the state of damage caused by ROS (reactive oxygen species)14. ROS has a high reaction potential and will be toxic and lead to oxidative damage to cellular macromolecules such as proteins, lipids, and DNA15. Recently, the possible association between thyroid dysfunction and reactive oxygen species has been increasingly considered16. High doses of nitrate can also inhibit iodine uptake and cause hypertrophic changes in the thyroid gland13. Decreased iodine intake can lead to lower production of thyroid hormones T3 and T4 and thus increase the production of thyroid-stimulating hormone (TSH)14. The association of thyroid disease with the risk of metabolic syndrome (hypertension, glucose, HDL, triglyceride, and waist circumference) has been reported in several studies15,16,17,18,19,20,21,22,23,24. Diet quality is also a factor influencing the development of MetS due to diet-related inflammatory processes associated with metabolically unhealthy obesity (MUO) and metabolic syndrome (MetS)25.
Various studies have shown that the prevalence of MetS is about 15/5% in China and 35% in the United States26. The corresponding value in Iran has been reported in about 25% of the adult population27,28.
Mets is a chronic disease that, in addition to thyroid disease, increases the risk of many diseases, including cardiovascular disease, stroke, and type 2 diabetes. Mets can be diagnosed based on at least three of the following five conditions: High blood sugar (glucose levels ˃100 mg/dL), hypertension (systolic blood pressure (SBP) ≥ 130 mm Hg), and diastolic blood pressure (DBP) ≥ 85 mmHg abdominal obesity (waist circumference (WC) ˃ 102 and 88 cm in men and women, respectively), high serum triglycerides (TG levels ˃ 150 mg/dL), and lipoprotein cholesterol with High density (HDL-C < 50 and 40 mg/dL for men and women, respectively)29.
This case–control study aimed to assess the effect of drinking water nitrate on the serum nitric oxide concentration and the risk of metabolic syndrome (MetS) in the general population.
In recent years, diseases related to the thyroid gland in Shiraz have increased, and Fars province is a leader in agriculture. According to the research, the relationship between drinking water nitrate and serum nitric oxide has not been studied in Iran; therefore, we aimed to carry out this study due to the importance of drinking water for human health and its possible effect on thyroid.
Materials and methods
Study population, design, and sampling
This case–control study was performed on the population in Shiraz in 2021. Shiraz is the capital of Fars province (29° 36′ 37′′ North and 52° 31′ 52′′ East; 1486 m above sea level) and the fifth metropolis. Shiraz has a population of 1,869,000 people according to the 2016 census and is about 17,889 ha.
In recent years, the concentration of nitrate in Shiraz water has increased over the years due to various factors such as human processes, lack of proper hygiene, and placement of wells in groundwater; in some wells, it causes more nitrate than the standard (50 mg/L)30,31. Therefore, due to the relationship between nitrate and this disease38 and the increasing prevalence of thyroid disorders in this city32, this study was performed. Thyroid disorders include generalized goiter, thyroid nodules, hyperthyroidism or clinical hypothyroidism, and abnormal thyroid function in thyroid individuals33.
In this study, we looked at people with hypothyroidism, hyperthyroidism, and benign thyroid cancer as patients with thyroid disorders. In recent years, the amount of iodine has been sufficient in the study area, and the increase in the prevalence of hypothyroidism is due to increasing age34. T4 and TSH tests were also taken to determine if the control group had hormonal problems. 150 national codes of Shiraz residents were randomly selected, and their contact numbers were provided to us. The selected individuals were then contacted and 100 of them (including 50 controls and 50 cases) were referred to the medical diagnostic laboratory for the relevant tests on a specific day.
Inclusion criteria for the cases were: (a) fasting time (12–14 h), (b) people with thyroid disorders for at least one year, (c) consumption of piped municipal water as drinking water, and (d) residents of Shiraz.
Inclusion criteria for the controls were: (a) fasting time (12–14 h), (b) consumption of piped municipal water as drinking water, (c) residents of Shiraz, and (d) lack of a disease with Thyroid disorders. Informed consent was signed by the participants before taking the samples. Additionally, this study was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1400.137), and The study followed the guidelines of the Declaration of Helsinki along with relevant guidelines35.
Blood sampling to measure serum nitric oxide
In this study, to measure serum nitric oxide, after sampling the blood of case and control groups with a thyroid disorder, we left the gelled tubes containing their blood for at least 15 min and at most 30 min at ambient temperature (15–25 °C).
Then, they were centrifuged at 2500–3000 rpm for 10–15 min. The serum was separated from the tubes and stored at −20 °C for testing with each identification code. Nitric oxide was measured using a nitric oxide measuring kit (Kiazist Company, Iran).
In this experiment, Griess39 reagent was used as a reactant with nitric oxide. Nitric oxide was then bonded with a reagent and read at 540–560 nm36.
Water nitrate assessment
After contacting the people to go to the laboratory, they were asked to bring a sample of drinking water in a bottle. Labeled samples in plastic bottles were transferred to the laboratory of the Department of Environmental Health of Shiraz University of Medical Sciences for chemical analysis.
In the first 24 h, the nitrate concentration of the samples was measured by the standard method using a spectrophotometer (UV (DR 6000) model) (hack company in Germany) at a wavelength of 220 nm for the samples37. Mean and standard deviation (SD) were calculated by SPSS Statistics 26.
Assessment of metabolic syndromes
Concurrent with the measurement of blood samples, the participants' metabolic syndrome (blood pressure, waist circumference, glucose, HDL, and triglyceride) was measured. Also, age, sex, and amount of vegetables and fruits consumed in the samples (case and control groups) were asked daily and weekly. Anthropometric measurements including weight, height, and WC were also performed on the day of sampling.
Weight and height were measured according to the National Health and Nutrition Survey (NHANES) with minimal clothing and no shoes38. Blood pressure in the right hand was measured after ten minutes of rest (OMRON, M2 Japan). It was measured twice with an interval of ten minutes; then, the mean final blood pressure was considered. Blood biochemical parameters, including TG, HDL-C, and fasting blood sugar (FBS), were measured by an automated biochemical analyzer (Poch-100i, Sysmex, Kobe, Japan) in the clinical laboratory. Finally, Mets of risk were assessed based on NCEP-ATP III criteria29. The use of this criteria is preferred in Asia because they can be easily applied to primary care settings in many of those regions39.
Statistical analysis
SPSS version 26 was used for all analyses. Mean and standard deviation were used to describe the quantitative variable. Pearson correlation coefficient was used to measure the correlation between variables if the data distribution was normal and the Spearman correlation coefficient was used if it was not normal. Linear regression was used to compare the correlation coefficients between the two groups.
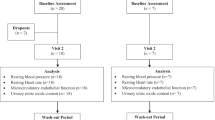
Logistic regression was used to compare the metabolic syndrome between the two groups. To determine the relationship between normal variables of the body mass index, we used triglyceride from the independent t-test, and for the rest of the table data due to abnormality, Mann–Whitney test was used. Also, a duplicate test was used to the accuracy of the device and random error to measure serum nitric oxide and nitrate. To do this, we tested the samples twice in a row without a time interval. The process of conducting the study is shown in Fig. 1.

Study execution process.
Discussion and results
Characteristics of the participants
According to Table 1, the mean age of the control group was 37.88 years; of them, 12 (24%) were male and 38 (76%) were female; also, for the cases, the mean age was 46.06 and among them 6 (12%) were male and 44 (88%) were female According to NCEP-ATP III criteria, the prevalence of MetS was 34% in the control group and 46% in the patient group with a thyroid disorder, which did not show a significant difference between the two groups (p value > 0.05) (Table 2).
Distribution of serum NO and nitrate levels in drinking water in the case and control groups
Table 3 shows the distribution of serum NO levels separately in the case and control groups.
As can be seen, the mean serum NO concentration in the case and control groups was 7.26 ± 0.14 and 7.14 ± 0.12, respectively; there was a statistically significant difference between the case and control groups. Figure 2 shows the distribution of serum NO levels in the case and control groups as a box plot.

Box plot of serum NO level distribution in the case and control groups with thyroid disorders.
Bagheri et al. concluded that serum NOx levels were associated with free T4 in men and anti-TPO in women. In this study, no significant relationship was observed between NOx and TSH40. Zoran et al.'s study, which was performed on 88 women (including 44 hypothyroid patients and 38 healthy women), found that serum NO levels in both groups could change and could also be a good predictor of the severity of hypothyroidism36.
Verma et al. estimated the nitric oxide of level on the 50 hypothyroid, 50 hyperthyroid, and 50 healthy individuals with a grease reaction. Nitric oxide concentrations were significantly lower in hyperthyroid patients compared with the controls, while this rate was significantly increased in hypothyroid patients. They also suggested that estimating nitric oxide levels in thyroid disorders may help understand the pathogenesis of thyroid disorders41. Abhinav Kumar al. revealed that NO levels were significantly reduced in hypothyroidism patients42. Mohammed et al. and Kumari et al. also reported a significant association between NO and thyroid disorders43,44. On the other hand, Ghazi Saidi et al.'s study,evaluated the correlation between serum nitric oxide concentration and thyroid hormones, and the amount of serum NOx was 30.71 ± 22.17 μmol/L. In this study, like our study, factors affecting serum levels such as BMI, FBS, etc. asked. They concluded that there is no relationship between serum nitric oxide and thyroid hormones45.
As shown in Table 2, the mean NO3 concentration of drinking water in the case and control groups was 21.43 ± 13.92 and 20.46 ± 14, respectively. Figure 3 shows a box plot of the distribution of nitrate levels in drinking water in the control group and patients with thyroid disorders.

Box plot of serum NO3 level distribution in the case and control groups with thyroid disorders.
According to Table 4, the maximum nitrate concentration was 47.5 in the case group and 45.5 mg/L in the control group, which is lower than the nitrate concentration set by the World Health Organization50 mg/L46. Although the amount of nitrate consumed in all points was less than the standard, there was a big difference between the minimum nitrate (in the patient and control groups equal to 3 mg/L) and the maximum. The supply of distribution systems from different surfaces and groundwater sources can cause differences in nitrate concentration in various places47. Examination of water supply showed that areas with higher nitrate concentrations are supplied than groundwater.
Ajdarpour et al. determined the nitrate concentration in 31 sampling points of the distribution system in the Shiraz and observed that the lowest and highest two-year mean concentrations were 2.1 and 58.35; they also stated that nitrate concentration in moment concentration in some places in Shiraz water distribution system was more than the standard level48. Another issue with nitrate entering the human body is the nitrate in food, which is shown in Table 1. Typically, about 85% of dietary nitrate (mineral nitrate anion, NO3−) is obtained from vegetables, and the rest from drinking water49. Vegetables can be a significant source of nitrate entering the body of the study participants, and it may be possible that the fertilizer1 and water used in vegetables are high in nitrate.
In a study conducted in 2006 by Maria Tajtakova et al., which examined the students in an area with nitrate-contaminated well water sources, thyroid volume and symptoms of thyroid disorders were assessed. Excessive consumption of nitrate in water and their home meals led to an increase in thyroid volume and an increase in the frequency of symptoms of subclinical thyroid disorders50.
In the study, Arianna et al. obtained nitrate concentrations in drinking water wells from the California Water Website (GAMA2020). The date of nitrate readings was from 1907 to 2019. They concluded that there was a statistically significant correlation between thyroid cancer registration data and California Water Board data (p < 0.05). They also stated that the rate of thyroid cancer in deprived areas was twice that in non-deprived ones. The number of wells and nitrate-contaminated sites was higher than the state average there51.
The relationship between drinking water nitrate concentration and serum nitric oxide in patients with thyroid disorders, (P-value = 0.062) (r = 0.266) and also in the control group, (P-value = 0.756) (r = 0.045) showed a positive correlation although this relationship was not statistically significant.
Comparison of serum NO correlation and components of metabolic syndrome in the case and control groups
According to Table 3, the results of metabolic syndrome components using clinical examinations for the case and control groups showed a significant difference in BMI, waist size, and triglyceride between the case and control groups (p-value < 0.05).
In a study carried out by Fontenelle et al. on the mechanism of thyroid function in human obesity, it was concluded that the thyroid function of obese individuals could contribute the worsening of metabolic complications and disease progression in the thyroid gland18.
Aleksander Kuś et al. in a study on the effect of changes in normal thyroid function on cholesterol levels, blood pressure, and the risk of type 2 diabetes found some changes in normal thyroid function on the serum cholesterol levels, blood pressure, and risk of type 2 diabetes17. A study was done by Rizos et al. in 2011 on the effects of thyroid dysfunction on lipid profile; it was concluded that thyroid dysfunction should be considered when evaluating and treating patients with hyperlipidemia52. As in our study, the mean triglyceride in patients was higher than that in the case group. According to NCEP-ATP III criteria, TG ˃ 150 can be one of the components of metabolic syndrome.
Table 4 shows the correlation between the serum NO level and metabolic syndrome components in the case and control groups. As shown, there was a correlation between the serum nitric oxide concentration and systolic blood pressure in the case group (P-value = 0.031, r = −0.30) and the control group (P-value = 0.38, r = −0.12). This correlation was statistically significant (p-value < 0.05).
The relationship between serum nitric oxide concentration and waist circumference in the case group (P-value = 0.34, r = 0.13) and control group (P-value = 0.32, r = 0.14) showed a positive correlation, which was not statistically significant. Also, a positive correlation was shown between the serum nitric oxide concentration and HDL level in patients (P-value = 0.12, r = 0.21). This correlation was not statistically significant. There was a negative correlation between serum nitric oxide concentration and HDL level in the control group (r = −0.12, P-value = 0.3) which was not statistically significant.
Correlation between the serum nitric oxide concentration and metabolic syndrome (according to NCEP-ATP III criteria) in patients (P-value = 0.16, r = −0.19) and in the control group (P-value = 0.52, r = −0.09) was negative; this relationship was not statistically significant.
Ashok Kumar et al.'s study included 50 Mets and 50 control. The Mets group was divided into two groups based on the presence or absence of SCH. In this study, a statistically significant correlation was shown in the BMI, systolic and diastolic blood BP, Glucose, HDL, and NO. They also stated that Met S cases should be screened for SCH and treated appropriately53.
In our study, the prevalence of Mets was higher in the patient group, but it showed a significant relationship with NO only in patient's diastolic blood pressure.
Hashemi et al. measured the levels of fasting blood glucose (FPG), lipid profile components, and nitric oxide by spectrophotometry on 50 women (25 healthy groups and 25 hypothyroid patients). They found that nitric oxide was significantly different from LDL in the two groups, but it was not significantly different for other components54.
In general, the limitation of this study was the small sample size that could not show a cause-and- effect relationship. Therefore, it is recommended that further studies should be done with large sample size. Then, in addition to measuring the water nitrate consumption of the samples, the nitrate of food, especially the vegetables, should be examined.
Conclusion
The results showed that serum NO was significantly different between the control and case groups (p-value < 0.001). The mean NO3 concentration of drinking water in the cases and controls was 21.43 ± 13.92 and 20.46 ± 14, respectively. There was a positive correlation between the concentration of nitrate in drinking water and serum nitric oxide in cases and controls; however, this relationship was not statistically significant. There was a statistically significant relationship between serum nitric oxide and systolic blood pressure in cases (p-value < 0.05). According to NCEP-ATP III criteria, the prevalence of MetS was 34% in the control group and 46% in the case group with a thyroid disorder, which did not show a significant difference between the two groups (p value > 0.05).
Data availability
All the data produced and analyzed is available with the Mansooreh Dehghani corresponding author “Email: mandehghani@yahoo.com” and shall be provided on a reasonable request.
References
Jordao, C., Pereira, M., Bellato, C., Pereira, J. & Matos, A. Assessment of water systems for contaminants from domestic and industrial sewages. Environ. Monit. Assess. 79(1), 75–100 (2002).
Nolan, B. T. & Hitt, K. J. Vulnerability of shallow groundwater and drinking-water wells to nitrate in the United States. Environ. Sci. Technol. 40(24), 7834–7840 (2006).
Kross, B. & Johnson, C. Continuing importance of nitrate contamination of groundwater and wells in rural areas. Am. J. Ind. Med. AJIMD 18(4), 449 (1990).
Nolan, B. T., Hitt, K. J. & Ruddy, B. C. Probability of nitrate contamination of recently recharged groundwaters in the conterminous United States. Environ. Sci. Technol. 36(10), 2138–2145 (2002).
Egboka, B. Nitrate contamination of shallow groundwaters in Ontario, Canada. Sci. Tot. Environ. 35(1), 53–70 (1984).
Spiegelhalder, B., Eisenbrand, G. & Preussmann, R. Influence of dietary nitrate on nitrite content of human saliva: Possible relevance to in vivo formation of N-nitroso compounds. Food Cosmet. Toxicol. 14(6), 545–548 (1976).
Leaf, C. D., Wishnok, J. S. & Tannenbaum, S. R. L-arginine is a precursor for nitrate biosynthesis in humans. Biochem. Biophys. Res. Commun. 163(2), 1032–1037 (1989).
Sudar, E. et al. Regulation of inducible nitric oxide synthase activity/expression in rat hearts from ghrelin-treated rats. J. Physiol. Biochem. 67(2), 195–204 (2011).
Zhang, P. et al. Inducible nitric oxide synthase deficiency protects the heart from systolic overload–induced ventricular hypertrophy and congestive heart failure. Circ. Res. 100(7), 1089–1098 (2007).
SoRelle, R. Nobel prize awarded to scientists for nitric oxide discoveries. Circulation 98(22), 2365–2366 (1998).
Fellet, A. L., Arza, P., Arreche, N., Arranz, C. & Balaszczuk, A. M. A. Nitric oxide and thyroid gland: modulation of cardiovascular function in autonomic-blocked anaesthetized rats. Experim. Physiol. 89(3), 303–312 (2004).
Colin, I. M. et al. Expression of nitric oxide synthase isoforms in the thyroid gland: Evidence for a role of nitric oxide in vascular control during goiter formation. Endocrinology 136(12), 5283–5290 (1995).
Ward, M. H. Too much of a good thing? Nitrate from nitrogen fertilizers and cancer. Rev. Environ. Health 24(4), 357–363 (2009).
Zaki, A. et al. Impact of nitrate intake in drinking water on the thyroid gland activity in male rat. Toxicol. Lett. 147(1), 27–33 (2004).
Buscemi, S. et al. Association of obesity and diabetes with thyroid nodules. Endocrine 60(2), 339–347 (2018).
Matrone, A., Ferrari, F., Santini, F. & Elisei, R. Obesity as a risk factor for thyroid cancer. Curr. Opin. Endocrinol. Diabetes Obes. 27(5), 358–363 (2020).
Kuś, A. et al. Variation in normal range thyroid function affects serum cholesterol levels, blood pressure, and type 2 diabetes risk: A mendelian randomization study. Thyroid 31(5), 721–731 (2021).
Fontenelle, L. et al. Thyroid function in human obesity: Underlying mechanisms. Horm. Metab. Res. 48(12), 787–794 (2016).
Chen, R.-H. et al. Thyroid diseases increased the risk of type 2 diabetes mellitus: A nation-wide cohort study. Medicine 98(20), 1 (2019).
Wang, C. The relationship between type 2 diabetes mellitus and related thyroid diseases. J. Diabetes Res. 2013, 1 (2013).
Mouradian, M. & Abourizk, N. Diabetes mellitus and thyroid disease. Diabetes Care 6(5), 512–520 (1983).
Danzi, S. & Klein, I. Thyroid hormone and blood pressure regulation. Curr. Hypertens. Rep. 5(6), 513–520 (2003).
Prisant, L. M., Gujral, J. S. & Mulloy, A. L. Hyperthyroidism: A secondary cause of isolated systolic hypertension. J. Clin. Hypertens. 8(8), 596–599 (2006).
Gumieniak, O. et al. Thyroid function and blood pressure homeostasis in euthyroid subjects. J. Clin. Endocrinol. Metab. 89(7), 3455–3461 (2004).
Bohn, T., Samouda, H. & Alkerwi, A. A. Dietary patterns and type 2 diabetes—Relationship to metabolic syndrome and inflammation. Diet, Inflammation, and Health 261–366 (Elsevier, 2022).
Saklayen, M. G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 20(2), 1–8 (2018).
Delavari, A., Forouzanfar, M. H., Alikhani, S., Sharifian, A. & Kelishadi, R. First nationwide study of the prevalence of the metabolic syndrome and optimal cutoff points of waist circumference in the Middle East: The national survey of risk factors for noncommunicable diseases of Iran. Diabetes Care 32(6), 1092–1097 (2009).
Sharifi, F., Mousavinasab, S., Saeini, M. & Dinmohammadi, M. Prevalence of metabolic syndrome in an adult urban population of the west of Iran. Experim. Diabetes Res. 2009, 1 (2009).
Expert Panel on Detection E. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 285(19), 2486–2497 (2001).
Darvishmotevalli, M. et al. Evaluation of carcinogenic risks related to nitrate exposure in drinking water in Iran. MethodsX 6, 1716–1727 (2019).
Nezhad, A. B. et al. Nitrite and nitrate concentrations in the drinking groundwater of Shiraz City, South-central Iran by statistical models. Iran. J. Public Health 46(9), 1275 (2017).
Karimi, F., Kalantarhormozi, M. R., Dabbaghmanesh, M. H. & Omrani, G. R. Thyroid disorders and the prevalence of antithyroid antibodies in Shiraz population. Arch. Iran. Med. 17(5), 1 (2014).
Bryer-Ash, M. Evaluation of the patient with a suspected thyroid disorder. Obstet. Gynecol. Clin. North Am. 28(2), 421–438 (2001).
Mirahmadizadeh, A., Bahadori, R., Ranjbar Omrani, G., Saki, F. & Sayadi, M. Prevalence of hypothyroidism in children and adolescents of Fars Province (Southern Iran): A nationwide prescription study, 2018–2019. Arch. Iran. Med. (AIM) 25(7), 1 (2022).
Inc, W. M. A. Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Indian Med. Assoc. 107(6), 403–405 (2009).
Gluvic, Z. M. et al. Serum nitric oxide levels correlate with quality of life questionnaires scores of hypothyroid females. Med. Hypotheses 131, 109299 (2019).
Federation, W. E. & Association, A. Standard Methods for the Examination of Water and Wastewater 21 (American Public Health Association (APHA), Washington, 2005).
Vidot, D. C. et al. Metabolic syndrome among marijuana users in the United States: An analysis of national health and nutrition examination survey data. Am. J. Med. 129(2), 173–179 (2016).
Tan, C.-E., Ma, S., Wai, D., Chew, S.-K. & Tai, E.-S. Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians?. Diabetes Care 27(5), 1182–1186 (2004).
Bagheripuor, F. et al. Association between serum nitric oxide metabolites and thyroid hormones in a general population: Tehran Thyroid Study. Endocr. Res. 41(3), 193–199 (2016).
Verma, M., Dahiya, K., Ghalaut, V., Seth, S., Saha, P. R., & Basu, A. editors. Thyroid Disorders And Nitric Oxide Levels (2015).
Kumar, A., Suresh, D., Annam, V. & Srikrishna, R. Significance of early biochemical markers of atherosclerosis in subclinical hypothyroidism patients with normal lipid profile. Int. J. Biol. Med. Res. 3(4), 2483–2486 (2012).
Kumari, S., Sandhya, G. K. & Gowda, K. Oxidative stress in hypo and hyperthyroidism. Al Ameen J. Med. Sci. 4(1), 49–53 (2011).
Atta, M. N., Elessawy, R., Deghedy, A., Hafez, A. & Elsherbiny, T. M. Hashimoto thyroiditis is an independent cardiovascular risk factor in clinically hypothyroid patients. Alexandria J. Med. 47(4), 1 (2011).
Ghazisaeidi, B. et al. Association between serum nitric oxide level and changes in thyroid function test in a population-based study: Tehran thyroid study participants (TTS). Int. J. Endocrinol. Metab. 19(3), 1 (2021).
Eskiocak, S., Dundar, C., Basoglu, T. & Altaner, S. The effects of taking chronic nitrate by drinking water on thyroid functions and morphology. Clin. Exp. Med. 5(2), 66–71 (2005).
Chen, J., Wu, H., Qian, H. & Gao, Y. Assessing nitrate and fluoride contaminants in drinking water and their health risk of rural residents living in a semiarid region of Northwest China. Exposure and Health. 9(3), 183–195 (2017).
Moeini, Z. & Azhdarpoor, A. Health risk assessment of nitrate in drinking water in Shiraz using probabilistic and deterministic approaches and impact of water supply. Environ. Chall. 5, 100326 (2021).
Lidder, S. & Webb, A. J. Vascular effects of dietary nitrate (as found in green leafy vegetables and beetroot) via the nitrate-nitrite-nitric oxide pathway. Br. J. Clin. Pharmacol. 75(3), 677–696 (2013).
Tajtáková, M. et al. Increased thyroid volume and frequency of thyroid disorders signs in schoolchildren from nitrate polluted area. Chemosphere 62(4), 559–564 (2006).
Tariqi, A. Q. & Naughton, C. C. Water, health, and environmental justice in California: Geospatial analysis of nitrate contamination and thyroid cancer. Environ. Eng. Sci. 38(5), 377–388 (2021).
Rizos, C., Elisaf, M. & Liberopoulos, E. Effects of thyroid dysfunction on lipid profile. Open Cardiovasc. Med. J. 5, 76 (2011).
Ahirwar, A. K. et al. Raised TSH is associated with endothelial dysfunction in metabolic syndrome: A case control study. Rom. J. Intern. Med. 55(4), 212–221 (2017).
Hashemi, M. M., Kosari, E., Mansourian, A. R. & Marjani, A. Serum levels of nitrite/nitrate, lipid profile, and Fasting Plasma Glucose and their associations in subclinical hypothyroid women before and after a two month treatment by levothyroxine. Rom. J. Intern. Med. 55(4), 205–211 (2017).
Acknowledgements
This article was extracted from the thesis written by Mrs. Shaghayegh Jafari, Master's student of Environmental Health Engineering. Hereby, the authors would like to acknowledge the Research Vice chancellor of Shiraz University of Medical Sciences for financially supporting the research (Proposal No. 22743).
Author information
Authors and Affiliations
Contributions
S.H.J. Methodology, Investigation, Writing—original draft. M.D. Writing—review & editing, Supervision. H.G.H. carried out the analyses. M.S. and H.H. provided advice.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jafari, S., Dehghani, M., Ghaem, H. et al. Relationship between serum nitric oxide of patients with thyroid disorders and metabolic syndrome indices and nitrate concentration of water. Sci Rep 13, 692 (2023). https://doi.org/10.1038/s41598-023-27560-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-023-27560-0
This article is cited by
-
Assessment of groundwater salinization and nitrate pollution in a sub-humid to semi-arid agricultural area: a case study of the Sidi Smail plain in northwestern Tunisia
Modeling Earth Systems and Environment (2026)
-
Synthesis and characterization of a polyionic liquid based on modified gum tragacanth for the removal of nitrates and investigation of its antimicrobial properties
Macromolecular Research (2025)
