
Abstract
Individuals living in rural areas have a higher incidence rate of stroke than their urban counterparts in China. However, few studies have investigated the association between blood malondialdehyde (MDA), an end product of lipid oxidation caused by reactive oxygen species (ROS), and stroke risk in rural populations. We aimed to investigate whether blood MDA levels contribute to a higher stroke risk in a Chinese elderly population from rural areas. Data from 2011 to 2012 from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), a national cohort of older adults in China, were analyzed. Smooth curve and multivariable correction analyses were used to evaluate the association between blood MDA levels and stroke risk in elderly populations from rural and urban areas, respectively. The median age of all included participants (N = 1598) was 84.04 years. The results of the smooth curve model revealed a gradual upward trend in the association of blood MDA levels with stroke risk in rural participants but not in urban participants. Similarly, the conditional logistic regression analysis suggested a significant association between MDA levels and stroke risk in rural participants but not in urban participants after adjustments for related confounding factors (age, sex, current smoker, current drinker, regular exercise, BMI and cardiovascular diseases (hypertension, heart disease, atrial fibrillation and diabetes)) were made. In brief, among the elderly population in China, elevated blood MDA levels were associated with increased stroke risk in rural participants but not in urban participants.
Similar content being viewed by others

Introduction
The urban‒rural disparity in life expectancy has gradually expanded in recent decades, especially in developing countries1,2. An important factor that widens the gap is an imbalance in the morbidity and mortality of cardiovascular diseases (CVDs), particularly stroke, in urban and rural areas3. A prior study reported that 7.1% of a gap in urban‒rural disparities in life expectancy resulted from stroke, and rural areas had a significantly higher rate of stroke mortality than urban areas4. However, the mechanisms underlying urban‒rural differences in the incidence rate of stroke are incompletely known. Some previous data might partly explain the difference. For example, individuals who lived in rural areas tended to have more and worse risk factor profiles, including hypertension, diabetes and dyslipidemia for stroke, compared with those who lived in urban areas5,6,7,8,9. Other evidence also suggested that populations in rural areas had less access to medical services than populations in urban areas, which may lead to an increase in the incidence rate of stroke10,11. Much of this literature, however, has mainly focused on the relationship between risk factors for urban‒rural differences and stroke, such as demographic characteristics and risk factors related to lifestyle. Few studies have investigated the association of biochemical indices in the human body with stroke risk in rural and urban populations.
Oxidative damage can arise from an imbalance between increased production of reactive oxygen species (ROS) and/or a reduction in antioxidant defenses12,13. Malondialdehyde (MDA), the main end product of lipid oxidation, can cause cross-linking polymerization of proteins, nucleic acids and other living macromolecules and cause great damage to the activities of the mitochondrial respiratory chain complex and key enzymes in mitochondria14,15. The present evidence has demonstrated that rapid ROS overexpression can immediately overwhelm antioxidant defenses after acute ischemic stroke, further causing tissue or cell damage. Furthermore, a second burst of ROS generation caused by increased blood flow contributes to reperfusion injury in brain tissue16. As an important indicator of the degree of oxidative damage, MDA has also been found to be associated with a series of complications after stroke17,18. However, it is not yet known whether there is an urban‒rural difference in the association between blood MDA and stroke risk.
Considering the present research background, we aimed to determine the association between blood MDA levels and stroke risk in a Chinese elderly population from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). Our first aim was to investigate whether a higher blood MDA level contributed to elevated stroke risk in the elderly population, independent of confounding factors such as demographic characteristics, lifestyle risks and concomitant CVDs. Then, we further investigated whether there was an urban‒rural disparity in the relationship between blood MDA levels and stroke in the present study.
Methods
Study population
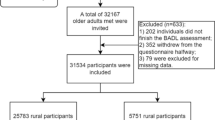
Study data were from the CLHLS study (https://www.icpsr.umich.edu/web/pages/ICPSR/), which is a prospective, longitudinal, community-based study19. Twenty-two provinces in China were initially selected, and then half of the cities or counties in these provinces were randomly selected to include the study population. A detailed description of the CLHLS has been published elsewhere20. Further details on the study design, study procedures and data quality assessment were also performed elsewhere21,22,23. In the present study, we used data from the 2011–2012 wave of the cohort. Our study had a sufficient analysis among adults aged 65 and older in the wave with complete information on stroke, MDA and other covariates. In all, 9765 elderly individuals were initially included in the 2011–2012 CLHLS. For the purpose of this study, 1598 elderly participants met the inclusion criteria in our study after excluding incorrect and missing data. All participants or their relatives were informed of the data for research in the CLHLS study. Written informed consent was obtained from all participants or their proxies, according to the Declaration of Helsinki guidelines.
Assessment of covariates
A structured questionnaire was conducted to obtain covariates. Sociodemographic characteristics included age, gender and residence. The other health characteristics included smoking, drinking, activities of daily living (regular exercise), body mass index (BMI) and self-reported diseases, such as heart disease, stroke, diabetes mellitus and other CVDs. Residence was categorized as “urban (city residence or town)” or “rural (countryside residence)”. Current smokers and current drinkers were evaluated by the self-reports “Do you currently smoker?” and “Do you currently drink alcohol?” Current smokers were categorized as “current smokers” and “not current smokers”. Current drinker was categorized as “current drinker” and “not current drinker”. Activity of daily living was classified as “regular exercise” and “not regular exercise”, according to “Do you do exercise regularly at present (yes or not)?” Self-reported diseases were classified as “yes” and “not”. The definition of all suffered diseases has been clarified in previous studies19,20,21,22,23.
Statistical analysis
All of the analyses were performed by using EmpowerStats 3.0. A P value ≤ 0.05 was considered to be statistically significant. We first implemented a smooth curve to estimate the association between blood MDA levels and stroke risk. Then, stratification analysis using a smooth curve was further performed to evaluate the association between blood MDA levels and the risk of stroke in the elderly population from rural and urban areas. Furthermore, in the stratification analysis, multiple logistic regression analysis was used to analyze the association of blood MDA with stroke risk in rural and urban areas respectively. From the Crude model to Model 4, variables including age, gender, current smoker, current drinker, regular exercise, BMI and CVDs (hypertension, heart disease, atrial fibrillation and diabetes) were controlled. Crude: Not adjusted. Model 1: Adjusted for age and gender; Model 2: Adjusted for age, gender, current smoker, current drinker and regular exercise; Model 3: Adjusted for age, gender, current smoker, current drinker, regular exercise and BMI; Model 4: Adjusted for age, gender, current smoker, current drinker, regular exercise, BMI and CVDs.
Additionally, stratification analysis for the association between blood MDA level and stroke risk was also performed by using “age”, “gender”, “current smoker”, “current drinker”, “regular exercise” and “BMI” as the hierarchical variables.
Ethics approval and consent to participate
Our study methods were also carried out in accordance with relevant guidelines and regulations. Our data were freely obtained from 2011 to 2012 of the CLHLS study, a national cohort of older adults in China. All participants or their relatives were informed of the data for research in the CLHLS study. Written informed consent was obtained from all participants or their proxies, according to the Declaration of Helsinki guidelines.
Results
Characteristics of participants
As shown in Table 1, the mean age of the participants was 84.04 years. A total of 818 of them (51.19%) were male. The mean MDA levels of both urban and rural participants were 4.73 mmol/mL and 5.25 mmol/mL, respectively. All participants were divided into two groups according to urban and rural areas. Compared with urban participants [stroke rate for 16 (6.69%)], rural participants [stroke rate for 105 (7.73%)] were more likely to be current drinkers and tended to have significantly higher serum MDA levels, a higher rate of atrial fibrillation and a lower heart rate. The blood biomarkers are also described in detail in Table 1.
Smooth curve analysis of the association between blood MDA level and stroke risk
The results analyzed by a smooth curve revealed a gradual upward trend in the association between serum MDA levels and the risk of stroke (Fig. 1A, P < 0.05), which suggested that elevated levels of serum MDA might be closely related to a higher risk of stroke. Furthermore, a gradual upward trend in the association was observed only in rural participants (P < 0.05) and not in urban participants (P > 0.05), as shown in Fig. 1B.

(A) The association between blood malondialdehyde (MDA) levels and risk of stroke in all included participants (urban and rural areas). (B) The associations between blood malondialdehyde (MDA) levels and risk of stroke in participants from urban and rural areas.
Elevated blood MDA levels contributed to higher stroke risk in rural participants
Consistent with the above, similar results were analyzed in the multiple logistic regression analysis: elevated blood MDA levels were associated with an increased risk of stroke in Model 4 (OR = 1.13, 95% CI 1.05–1.22, P = 0.002) after adjustments for age, gender, current smoker, current drinker, regular exercise, BMI and CVDs (hypertension, heart disease, atrial fibrillation and diabetes) were made (Table 2). Then, we further investigated whether there was an urban‒rural disparity in the association. Conditional logistic regression analysis suggested that after adjustment for confounding factors, there was a significant association between MDA level and stroke risk only in rural participants (OR = 1.14, 95% CI 1.05–1.24, P = 0.001, Model 4) but not in urban participants (OR = 0.94, 95% CI 0.68–1.29, P = 0.694, Model 4), as shown in Table 3. These results demonstrated an urban‒rural difference in the association between blood MDA levels and stroke in the Chinese elderly population.
Additionally, the association between blood MDA level and stroke risk was further performed by stratified analysis using “age”, “gender”, “current smoker”, “current drinker”, “regular exercise” and “BMI” as the hierarchical variables. Our results showed that age, current drinker, regular exercise and BMI had significant effects on the association between blood MDA levels and stroke risk in rural participants (Table 4). However, in participants from City & Town, we did not observe that any variable had a significant effect on the association between MDA level and stroke risk (Table 5).
Discussion
In this cross-sectional and community-based study, after adjustment for important identified confounders, blood MDA levels presented a positive association with stroke risk among adults in the Chinese elderly population. Specifically, higher values of serum MDA predicted an elevated risk of stroke. After we explored this association in the urban‒rural stratification analysis of these participants, the results further supported an urban‒rural difference in the association. Elevated blood MDA levels were independently associated with increased stroke risk only in rural individuals but not in urban individuals.
Oxidative damage caused by ROS can result in cell death and tissue destruction, such as protein denaturation, lipid peroxidation, DNA damage, inactivation of enzymes, release of Ca2+ from intracellular stores, and destruction of the cytoskeletal structure. The condition of ischemia and reperfusion after stroke has been found to be associated with overproduction of ROS, potentially leading to neuronal death24,25,26,27,28. MDA is commonly used as a marker of oxidative status and is related to the excessive formation of ROS25. Considering the adverse effect of oxidative stress on stroke, we analyzed the relationship between serum MDA and the risk of stroke. As we expected, our results showed that serum MDA levels were significantly and positively associated with the risk of stroke, which is consistent with previous conclusions that excessive oxidative damage increases the risk of stroke25,28. Interestingly, we found an urban‒rural difference in the association that elevated blood MDA levels were independently associated with an increased risk of stroke in rural individuals but not in urban individuals. Some previous evidence may partly explain this discrepancy. For instance, there is evidence to report that rural individuals are likely to have worse risk factor profiles of stroke, such as unhealthy lifestyles (high mental pressure, staying up late to work and less exercise) and eating habits (high fat and high sugar diet), related to higher levels of oxidative stress, which might contribute to a higher stroke risk, compared with urban individuals1,2,3,4. Because of improved living standards in China, a high-fat diet and unhealthy lifestyle associated with oxidative stress and its related diseases are more common in rural populations. It is also known that individuals from rural areas tend to have more risk factors for stroke, including hypertension, diabetes and dyslipidemia, than those from urban areas5,6,7,8,9. In addition, early prevention and treatment of stroke are not well performed in rural populations, which leads to a high risk of apoplectic attack due to a lack of health awareness. These reasons may partly explain why elevated MDA levels can be associated with higher stroke risk in rural participants than in urban participants. Certainly, if we would like to elucidate this urban‒rural difference from the perspective of molecular mechanisms, it is still quite difficult due to numerous complex mechanisms concerning stroke and its related risk factors, and further research may be needed in the future.
Additionally, to analyze the impact of other variables, such as sociodemographic characteristics and lifestyle, stratification analyses were used to further evaluate the independent association between blood MDA levels and stroke risk. Importantly, we observed that age, current drinking status, regular exercise and BMI in rural participants had significant influences on the association of blood MDA with stroke risk. The results further support our view that excessive production of MDA caused by oxidative stress in rural populations contributed to the higher stroke risk. However, the effect of these factors in the urban participants was not significant, which may be because the urban population is likely to have better lifestyle habits, a healthier diet and more medical resources, leading to a relatively lower incidence rate of stroke.
In this cross-sectional study, we first found an independent association between increased blood MDA levels and the risk of stroke among old adults. Specifically, the independent association only existed in rural individuals but not in urban individuals, which extends few previous studies on urban‒rural differences related to stroke in the elderly population. However, several limitations should be noted in the present study. First, blood indicators were tested only once. In the process of stroke, different levels of oxidative stress lead to different levels of blood MDA, which may further make our analysis biased. Second, more than 9000 individuals were included in the CLHLS study. Only 2439 individuals participated in blood biochemical tests, and 1598 individuals were included in our study because approximately 800 individuals were excluded due to the absence of important variables. Our study did not significantly analyze data on these excluded populations. Finally, we cannot define the type of stroke (hemorrhagic or ischemic stroke, acute or chronic stroke), which might produce a heterogeneous association between serum MDA and the risk of different stroke types.
Conclusions
Our results indicated that elevated blood MDA levels were related to increased stroke risk in rural individuals but not in urban individuals. This may provide new information that excessive oxidative stress contributes to increased stroke risk in rural populations.
Data availability
Study data were from the CLHLS study (https://www.icpsr.umich.edu/web/pages/ICPSR/), which is a prospective, longitudinal, community-based study. Twenty-two provinces in China were initially selected, and then half of the cities or counties in these provinces were randomly selected to include the study population. A detailed description of the CLHLS has also been published elsewhere20. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Koh, H. K., Graham, G. & Glied, S. A. Reducing racial and ethnic disparities: The action plan from the department of health and human services. Health Aff. (Millwood) 30(10), 1822–1829 (2011).
Zimmerman, F. J. & Anderson, N. W. Trends in health equity in the United States by race/ethnicity, sex, and income, 1993–2017. JAMA Netw. Open 2(6), e196386 (2019).
Irani, S. S. et al. Heart disease and stroke statistics-2020 update: A report from the american heart association. Circulation 141(9), e139–e596 (2020).
Singh, G. K. & Siahpush, M. Widening rural-urban disparities in all-cause mortality and mortality from major causes of death in the USA, 1969–2009. J. Urban Health 91(2), 272–292 (2014).
Kapral, M. K. et al. Rural-urban differences in stroke risk factors, incidence, and mortality in people with and without prior stroke. Circ. Cardiovasc. Qual. Outcomes 12(2), e004973 (2019).
Howard, G. et al. Contributors to the excess stroke mortality in rural areas in the United States. Stroke 48(7), 1773–1778 (2017).
Eberhardt, M. S. & Pamuk, E. R. The importance of place of residence: Examining health in rural and nonrural areas. Am. J. Public Health 94(10), 1682–1686 (2004).
Gillum, R. F. & Ingram, D. D. Relation between residence in the southeast region of the United States and stroke incidence. The NHANES I Epidemiologic Followup Study. Am. J. Epidemiol. 144(7), 665–673 (1996).
Correia, M. et al. Prospective community-based study of stroke in Northern Portugal: Incidence and case fatality in rural and urban populations. Stroke 35(9), 2048–2053 (2004).
Joynt, K. E., Harris, Y., Orav, E. J. & Jha, A. K. Quality of care and patient outcomes in critical access rural hospitals. JAMA 306(1), 45–52 (2011).
Joubert, J. et al. Stroke in rural areas and small communities. Stroke 39(6), 1920–1928 (2008).
Sagar, S. et al. Oxygen free radicals in essential hypertension. Mol. Cell. Biochem. 111(1–2), 103–108 (1992).
Teesalu, R., Allikmets, K. & Zimer, M. Oxidative stress and hyperinsulinaemia in essential hypertension: Different facets of increased risk. J. Hypertens. 14(3), 407 (1996).
Adams, A., Kimpe, N. D. & Boekel, M. V. Modification of casein by the lipid oxidation product malondialdehyde. J. Agric. Food Chem. 56(5), 1713 (2008).
Emelyanova, L. et al. Detrimental effect of lard-based diet on mitochondrial respiratory chain complexes and oxidative stress. J. Am. Coll. Cardiol. 59, 13 (2012).
Su, X. T. et al. Mechanisms of acupuncture in the regulation of oxidative stress in treating ischemic stroke. Oxid. Med. Cell Longev. 24(2020), 7875396 (2020).
Jouyban, A. & Khoubnasabjafari, M. Comments on “Malondialdehyde: A novel predictive biomarker for post-stroke depression”. J. Affect. Disord. 1(225), 52–53 (2018).
Mueangson, O. et al. Malondialdehyde as a useful biomarker of low hand grip strength in community-dwelling stroke patients. Int. J. Environ. Res. Public Health 17(21), 7918 (2020).
Yi, Z. Introduction to the Chinese Longitudinal Healthy Longevity Survey (CLHLS). Healthy longevity in China 23–38 (Springer, 2008).
Zeng, Y., Feng, Q., Hesketh, T., Christensen, K. & Vaupel, J. W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 389, 1619–1629 (2017).
Lv, Y. B. et al. Revisiting the association of blood pressure with mortality in oldest old people in China: Community based, longitudinal prospective study. BMJ 5(361), k2158. https://doi.org/10.1136/bmj.k2158 (2018).
Zeng, Y. et al. Sociodemographic and Health Profiles of the Oldest Old In China. Popul. Dev. Rev. 2002, 28 (2002).
Zeng, Y. & Vaupel, J. W. Chinese Longitudinal Healthy Longevity Survey (CLHLS), Biomarkers Datasets, 2009, 2012, 2014. Inter-university Consortium for Political and Social Research [distributor], 2019-01-15. https://doi.org/10.3886/ICPSR37226.v1.
Kadowaki, H. et al. Amyloid beta induces neuronal cell death through ROS-mediated ASK1 activation. Cell Death Differ. 12(1), 19–24 (2005).
Adibhatla, R. M. et al. Retraction: CDP-choline significantly restores phosphatidylcholine levels by differentially affecting phospholipase A2 and CTP: Phosphocholine cytidylyltransferase after stroke. J. Biol. Chem. 288(11), 7549 (2013).
McCracken, E. et al. The lipid peroxidation by-product 4-hydroxynonenal is toxic to axons and oligodendrocytes. J. Cereb. Blood Flow Metab. 20(11), 1529–1536 (2000).
Szabó, C. Role of poly(ADP-ribose)synthetase in inflammation. Eur. J. Pharmacol. 350(1), 1–19 (1998).
Love, S., Barber, R. & Wilcock, G. K. Neuronal death in brain infarcts in man. Neuropathol. Appl. Neurobiol. 26(1), 55–66 (2000).
Funding
The work was supported by the Jiangxi Provincial Natural Science Foundation [20224BAB216019], National Natural Science Foundation Incubation Program of the Second Affiliated Hospital of Nanchang University [2022YNFY12010] and National Natural Science Foundation of China [82060059].
Author information
Authors and Affiliations
Contributions
R.W. and Y.S. completed the main manuscript text; M.Z. completed data collation and validation; Y.H. revised the final draft and supervised it. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wan, R., Su, Y., Zhu, M. et al. Elevated blood malondialdehyde level contributed to a high stroke risk in a Chinese elderly population from rural areas: a cross-sectional study. Sci Rep 14, 4325 (2024). https://doi.org/10.1038/s41598-024-54419-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-54419-9
