
Abstract
Enhanced recovery after surgery (ERAS) has been successfully integrated into a diverse array of surgical fields to improve the quality and efficacy of treatment intervention. Nonetheless, the application of the ERAS protocol for patients with diabetic foot ulcer (DFU) subsequent to undergoing surgical procedures has not been previously explored. Therefore, this study aimed to investigate the effect of an enhanced recovery protocol on perioperative outcomes in patients with DFU following surgical procedures. A retrospective analysis was conducted on 112 patients with DFU who underwent surgery between January 2020 and December 2021 at a tertiary referral care center. In total, 57 patients received standard perioperative care (the non-ERAS group), and 55 patients received ERAS care (the ERAS group). The primary outcomes included the length of stay (LOS), wound healing time, patient satisfaction, and costs, serving as the basis for assessing the effectiveness of the two approaches. Secondary outcomes included preoperative anxiety (APAIS score), nutritional status (PG-SGA), pain (NRS score), the incidence of lower-extremity deep vein thrombosis (DVT), the reduction in lower-limb circumference, and the activity of daily living scale (Barthel Index). The ERAS group exhibited significantly shorter LOS (11.36 vs. 26.74 days; P < 0.001) and lower hospital costs (CNY 62,165.27 vs. CNY 118,326.84; P < 0.001), as well as a higher patient satisfaction score and Barthel Index score (P < 0.05). Additionally, we found a lower APAIS score, incidence of DVT, and circumference reduction in lower limbs in the ERAS group compared to the non-ERAS group (P < 0.05). In comparison, the wound healing time, nutritional status, and pain levels of participants in both groups showed no significant difference (P > 0.05). By reducing the LOS and hospital costs, and by minimizing perioperative complications, the ERAS protocol improves the quality and efficacy of treatment intervention in patients with DFU who underwent surgical procedures.
Trial registration number: ChiCTR 2200064223 (Registration Date: 30/09/2022).
Similar content being viewed by others

Introduction
Enhanced recovery after surgery (ERAS), also known as fast-track surgery (FTS), refers to a set of protocols that was first developed by Danish surgeon Kehlet1. ERAS aims to reduce surgical stress and postoperative complications and accelerate recovery without limiting the effectiveness of surgery. Operating based on evidence-based optimization measures during the perioperative period, the concept of ERAS initially achieved success in colorectal surgery2, resulting in early recovery without severe complications. This groundbreaking achievement advanced the revolutionary perspective that postoperative recovery may be more influenced by other factors than the specific choice of surgical technique (e.g., laparoscopic or open), such as effective pain management, early nutritional support, early mobilization, and the omission of recovery-inhibiting regimens (e.g., gastrointestinal tubes, prolonged urinary catheter drainage, and drains)3.
Recently, the ERAS program has been successfully applied in a variety of surgeries, including hepatobiliary surgery4, orthopedic surgery5, gynecological surgery6, and cardiothoracic surgery7, to accelerate recovery and decrease the length of stay (LOS) and hospital costs. As such, a specific consensus has formed in these surgical fields8. Nevertheless, a standardized set of ERAS procedures has not yet been established for diabetic foot ulcer (DFU) surgery, which may be attributed to the fact that DFU is a complication of diabetes mellitus, and endocrinology typically takes the lead in managing patients with DFU. Endocrinologists often tend to prioritize long-term dressing changes over surgery as the primary treatment for DFU on account of professional limitations.
As the understanding of the pathogenesis and progression of DFU has continued to grow, a multidisciplinary treatment (MDT) based on surgical debridement has gradually developed into the primary treatment of DFU. An increasing number of surgical departments are actively participating in the admission and treatment of patients with DFU, deploying techniques including vascular surgery, orthopedics, general surgery, treatment in the burn department, plastic surgery, etc.
However, the extended LOS9, multiple perioperative complications10, prolonged postoperative recovery11, and considerably elevated average hospital cost12 of patients with DFU have been reported to be associated with surgical interventions. These clinical issues have prompted us to use ERAS procedures to improve the quality and efficacy of treatment.
Thus, to cope with the above clinical problems, we have adapted some key elements of ERAS guidelines13 to patients with DFU following surgery in a tertiary referral hospital and evaluated their clinical outcomes. We conducted a retrospective cohort study on ERAS in patients with DFU. We hypothesized that the ERAS protocol would help to improve the treatment efficacy by shortening the LOS, reducing the hospital cost, and decreasing perioperative complications.
Methods
Study design
This study was a retrospective cohort study that included patients diagnosed with DFU after undergoing surgery between January 2020 and December 2021. The study was performed in accordance with the International Conference on Harmonization Good Clinical Practice Guidelines and the Declaration of Helsinki, and approved by the ethical review committee of Beijing Shijitan Hospital, Capital Medical University [(2022) Ethical approval number (23)]. Written informed consent was provided by all participants, and all identities were anonymized.
Participants
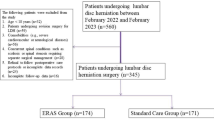
A total of 124 patients with DFU who underwent surgery in the Department of Orthopedic Surgery, Beijing Shijitan Hospital, Capital Medical University (CMU, China), from January 2020 to December 2021 were included in this study. Some 12 patients were excluded due to the following reasons: ① the condition was combined with multiple organ failure and required intensive care (n = 6); ② the patient was unable to cooperate with treatment and gave up midway (n = 3); ③ the follow-up was lost (n = 3). Finally, 112 patients were included in this study. Following January 2021, some key elements from the ERAS protocol released by the ERAS society13 were applied to DFU patients who underwent surgery in our department (Table 1). The 112 patients were divided by ERAS group (receiving ERAS protocol from January 2021 to December 2021), comprising 55 patients, and the non-ERAS group (receiving conventional perioperative care from January 2020 to December 2020) of 57 patients. All patients underwent standardized surgical procedures performed by the same operation team. Endovascular therapy was used to treat ischemic diabetic foot; radiofrequency thermocoagulation of lumbar sympathetic ganglia (LSG) or spinal cord stimulation (SCS) were used for painful diabetic peripheral neuropathy (PDPN)20,21; excisional debridement was used to treat infected ulcers with necrotic soft tissue or diabetic foot osteomyelitis14,15; amputation was performed for gangrene; skin grafting was carried out for delayed wounds after NPWT (negative-pressure wound therapy); and surgical off-loading was conducted for foot deformity16. All patients provided written informed consent prior to surgery. All patients remained anonymous prior to study analysis. The flow diagram illustrating participation selection is shown in Fig. 1.

Flow diagram illustrating participation selection.
Treatment protocol
(1) Non-ERAS group
After admission, a traditional perioperative management plan was implemented. This mainly comprised routine preoperative education, entailing a process of informing patients about the surgical procedure and corresponding precautions, potential risks during surgery, postoperative complications, and management measures. The patients underwent preoperative fasting, avoiding solid food for 8 h and water for 6 h. The indwelling catheter was placed before the operation, and routine spinal anesthesia was performed during the operation. Intraoperative fluid was administered to prevent volume-deficient hypotension. Patients continued fasting and drinking for 6 h after surgery. After surgery, the pillow was completely removed, and the patient was kept prone for 6 h to prevent headaches caused by low intracranial pressure. Subsequently, bed rest was the primary approach to preventing foot loads. A lower-limb pneumatic pump was used to passively activate lower-limb muscles to reduce the risk of deep vein thrombosis in these areas. Oral or intravenous painkillers were administered to manage perioperative pain. Routine nutritional support was administered, Oral Nutritional Supplements (ONS), as well as enteral and parenteral nutrition, were given as necessary to address malnutrition. Wound dressings were routinely changed until the wound stabilized at discharge.
(2) ERAS group: implementing perioperative ERAS care
Since January 2021, our department utilized some key elements from the ERAS protocol released by the ERAS society13, applying these aspects to patients with DFU who underwent surgery in our department (Table 1).
Preoperative measures
Patient information was acquired via direct communications with patients and their families. Patients’ psychological status, personality traits, and comprehension of the disease were assessed, with tailored psychological counseling provided as necessary. Patients who still exhibited tobacco or alcohol dependence were educated and assisted to quit smoking and alcohol during the perioperative and wound healing stages, with interventions performed based on their reported smoking and drinking history. The patients’ physical condition was comprehensively evaluated, and the patients and their families were informed about the current comorbidities that could be achieved through active interventions. The patients were encouraged to communicate with other patients who had successfully recovered, helping them to overcome psychological barriers and actively participate in surgical treatment and perioperative care. Detailed information on the significance of pre-surgery rehabilitation training was provided, and patients were guided to master the methods of postoperative rehabilitation training. There was no requirement to abstain from water consumption before surgery. Routine catheterization and indwelling catheters were not required before surgery. In cases of lower-limb ischemic pain caused by diabetic peripheral vascular disease, endovascular therapy including Percutaneous transluminal angioplasty (PTA) was performed to alleviate foot ischemic pain17. PTA is a minimally invasive vascular procedure performed to widen the lumen of a partially or fully occluded blood vessel that has narrowed or been blocked, typically by atherosclerotic plaque. This procedure involves passing a balloon catheter through the skin and into the blood vessel. This is to be guided to the site of obstruction, where the tip of the catheter is expanded via inflation to compress and flatten the plaque to restore blood flow. This is performed to ensure that the ischemic lower limb receives adequate blood supply, effectively relieving ischemic pain.
Preoperative nutritional support was provided, and we actively corrected cases of hypoproteinemia. A comprehensive nutritional risk assessment was conducted using the Nutritional Risk Screening 2002 (NRS2002)18 and the scored Patient-Generated Subjective Global Assessment (PG-SGA) as nutrition assessment tools before surgery. Enteral and intravenous nutrition were only preferred when oral intake failed to meet the nutritional needs, or when digestive ulcers or gastrointestinal dysfunctions were present. The nutritional intervention for each patient undergone dynamic adjustments, which was according to individual differences and disease conditions based on the following standardized nutritional interventions:
-
(1)
Protein intake: Many guidelines recommend 1.25–1.5 g/kg of body weight per day of protein for malnourished patients with pressure injuries19. The protein requirement of type 2 diabetes patients can be calculated as follows: ① For patients without risk of malnutrition, 0.8–1.0 g/kg/d of ABW (actual body weight). ② For patients who are at risk of malnutrition, 1.25–1.5 g/kg/d of ABW. ③ For obese patients, calculated based on IBW (ideal body weight): Ideal weight for males (kg) = [height (cm) -100] × 0.9; Ideal weight for women (kg) = [height (cm) -105] × 0.92. ④ Patients in a state of stress or illness: 2 g/kg/d of ABW, or use IBW if the patient is obese. ⑤ Critically ill with BMI 30–40 kg/m2: 2 g/kg/d of IBW. ⑥ Critically ill with BMI > 40 kg/m2: 2.5 g/kg/d of IBW. ⑦ In patients with chronic kidney disease who are not critically ill, it is advisable to prescribe a dietary protein intake of 0.6–0.8 g/kg/d of ABW per day under close clinical supervision to maintain a stable nutritional status and optimize glycemic control.
-
(2)
Carbohydrate: Carbohydrate daily recommendations will vary from patient to patient based on the progression of T2DM, daily glycemic control, and whether the patient is on insulin therapy or oral hypoglycemics. On average, women need approximately 45–60 g, while men may require 60–75 g per meal.
-
(3)
Fats: It is recommended to determine daily fat intake based on the patient’s specific condition. Compared to the quantity of intake, the quality of fat consumed is more important. The guidelines of the Chinese Nutrition Society recommend an intake ratio of long-chain saturated fatty acids, monounsaturated fatty acids, and polyunsaturated fatty acids of 1:1:120. Avoid consuming trans fatty acids. Important fats to consider are monounsaturated and polyunsaturated fatty acids, which play a major role in cell membranes. Eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and arachidonic acid are fatty acids that contribute to membrane fluidity, membrane and intracellular signaling, and the modulation of apoptotic pathways.
-
(4)
Micronutrients: Vitamins and minerals are essential for maintaining overall health and should be included in all nutritional assessments19,21. The intake and sources of micronutrients in the "Dietary Guidelines for Chinese Residents (2022)" compiled by the Chinese Nutrition Society22 are shown in Table 2.
Intraoperative management
The ERAS group underwent anesthesia via an ultrasound-guided lower-limb nerve block. This involved the sciatic and saphenous nerves and did not require patients to fast food and water before surgery. During the surgical procedure, the infusion speed was controlled, and the intake of venous fluid was reduced to prevent overloading of the heart and kidney. An infusion heater was used to warm the infusion liquid, and either an insulation blanket or a heater was used to maintain the patient's core temperature at approximately 37 ℃ during surgery23. Given the poor blood supply and microcirculation of diabetic foot wounds, the wound was not rapidly closed tightly; instead, it was gradually closed, with a local opening maintained for drainage. Unconventional placement of the drainage tube was used to ensure optimal drainage.
Postoperative management
In the ERAS group, patients were allowed to consume solid food and water immediately upon returning to the ward after surgery. On the same day as the surgical procedure, they were encouraged to sit up, move around their bed, and access the restroom for bowel movements with the assistance of a wheelchair or walking aid, gradually initiating foot movement after surgery. Medical staff regularly provided guidance and assisted patients to undertake active rehabilitation exercises during the early postoperative period. The training program was customized based on the individual differences between patients. Either on the day after surgery or the second day post-surgery, a foot offloading brace was placed on the affected limb to facilitate intermittent movement exercise on the ground. Weight-bearing activities were initiated after surgery as early as possible, and multiple short-term exercises were carried out to gradually extend the time of active movement on the ground and increase the level of lower-limb weight-bearing exercise.
Perioperative pain management
A comprehensive pain management plan was implemented, which included providing psychological counseling to patients, distracting their attention towards other activities, and reducing pain sensitization resulting from emotions such as anxiety and fear. Oral painkillers were administered before surgery to prevent the need for pain intervention during the surgical procedure. Before wound dressing, ropivacaine was locally inserted into the wound, extending the duration of the local nerve block and alleviating pain during surgery. A patient-controlled analgesia pump (PCA) was customized based on the patient's pain sensitivity and post-surgery tension level. In instances of neuropathic pain due to diabetes-related peripheral neuropathy, radiofrequency thermocoagulation of lumbar sympathetic ganglia (LSG)24 or spinal cord electrical stimulation (SCS)25 were used to relieve peripheral neuropathic pain. Radiofrequency thermocoagulation of lumbar sympathetic ganglia (LSG) applies nerve ablation on the lumbar sympathetic nerve to improve symptoms, such as chronic pain induced by nerve injury to lower limbs. Spinal cord electrical stimulation (SCS) is a safe and effective treatment for various types of chronic refractory pain. By implanting electrode wires into the epidural space of the spinal cord, the current generated by the neural stimulator is transmitted to the spinal cord, and low-voltage electrical stimulation is performed on the spinal nerves to block the transmission of pain to the brain center, relieving pain.
Discharge criteria for both groups remained consistent: (1) patient stability with satisfactory wound healing or evidence of healing progression, and the ability to perform dressing changes independently or with the assistance of family members; (2) patient and their family consent to discharge, along with receipt of relevant post-discharge precautions and follow-up time.
Outcomes
The primary outcomes involved the length of stay (LOS), wound healing time, patient satisfaction, and expenses associated with the two protocols. Secondary outcome parameters included preoperative anxiety (APAIS score26), nutritional status (PG-SGA27), pain (NRS score28), incidence of lower-extremity deep vein thrombosis (DVT), reduction in lower-limb circumference (The definition of “circumference” of lower limbs in our study is the thigh circumference which was measured by tape measure at 15 cm proximal to the patella), and the activity of the daily living scale (Barthel Index29). All outcomes were collected retrospectively from medical records in accordance with the methodology described in previous research30.
Statistical analysis
The continuous variables include age, duration of onset, ankle brachial index, the activity of daily living scale, preoperative leukocyte, preoperative CRP, preoperative hemoglobin, preoperative albumin, preoperative prealbumin, LOS, wound healing time, patient satisfaction, expenses, APAIS score, PG-SGA score, NRS score, the circumference of lower limbs, and Barthel Index. The categorical variables include gender, Wagner classification, and DVT occurrence. Normally distributed continuous variables were summarized using mean and standard deviation (SD). Categorical variables were expressed as frequency and percentage.
The distribution of data was evaluated using the Kolmogorov–Smirnov test. Student’s t-test or the Mann–Whitney U-test were used to evaluate differences of normally distributed continuous variables between ERAS group and non-ERAS group. A chi-square test was used to evaluate differences in nominal variables, including gender and the number of people with DVT across the ERAS group and non-ERAS group. The Wilcoxon test was used to evaluate differences in the proportion of Wagner’s grade between the ERAS group and non-ERAS group.
Subgroup analyses were used to further explore the improvement effect of ERAS on LOS and expenses between different genders, age groups, and Wagner’s grades, and results were displayed using a forest plot. In subgroup analysis, separate random-coefficient models were fitted to evaluate β changes in participants with and without the ERAS protocol.
All tests were two-sided, and a statistical significance level of 0.05 was used. All statistical analyses were performed using SPSS (Version 26.0, IBM, United States).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Approval was granted by the Ethics Committee of Beijing Shijitan Hospital Affiliated to Capital Medical University [(2022) Ethical approval number (23)].
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Results
General results
One hundred and twelve patients with DFU (82 males and 30 females; 65.72 ± 10.73 years old) who underwent surgery were grouped into the non-ERAS group (57; 65.16 ± 9.97 years old) and the ERAS group (55; 66.31 ± 11.52 years old) according to their management protocols. The numerical data all conformed to a normal distribution based on the Kolmogorov–Smirnov test. The difference in demographic characteristics (including gender, age, duration of onset, the proportion of patients in each Wagner’s grade,and preoperative comorbidities) and preoperative variables (including ABI, activity of daily living scale at admission, leukocyte, CRP, hemoglobin, albumin, prealbumin, and HbA1C) were compared between the ERAS group and the non-ERAS group (Table 3). No significant difference was observed in these parameters (P > 0.05).
Evaluation and comparison of primary and second outcomes
Compared with the non-ERAS group, the ERAS group had a significantly shorter LOS (11.36 vs. 26.74 days; P < 0.001), and the median total hospital expenses were significantly lower (CNY 62,165.27 vs. CNY 118,326.84; P < 0.001). Higher patient satisfaction could be noticed in the ERAS group (94.58 vs. 92.30; P = 0.008), but a comparable wound healing time was observed between the ERAS group and non-ERAS group (27.18 ± 10.25 days vs. 27.67 ± 9.67 days; P > 0.05).
The ERAS group also displayed a significantly lower score in APAIS score of preoperative anxiety (7.80 vs. 11.61; P < 0.001), a lower incidence of DVT (1.8% vs. 15.8%; P = 0.016), and circumference of the lower limbs (1.38 vs. 4.61 cm; P < 0.001). Moreover, it was also found that the ERAS group had a significantly higher score on the activity of daily living scale (85.36 vs. 73.51; P < 0.001). No significant differences were observed in terms of PG-SGA score (7.25 ± 3.47 vs. 7.89 ± 2.78; P > 0.05) and NRS score (4.80 ± 2.48 vs. 4.75 ± 2.28; P > 0.05) between the two groups. (Table 4).
Evaluation of the impact of interaction
Figures 2 and 3 show the treatment effects of interaction on subgroup analysis. The ERAS group had better clinical outcomes (shorter LOS and lower hospital expenses) in both men and women, as well as in those older than 65 years and those younger than 65 years. Patients with Wagner grade 4 and Wagner grade 5 were more likely to benefit from the ERAS protocol.

LOS of interaction for the subgroup analysis (overall and by gender, age, and Wagner classification).

Expenses of interaction for the subgroup analysis (overall and by gender, age, Wagner classification).
Discussion
Enhanced recovery after surgery is a multimodal approach to the perioperative care of patients undergoing surgical procedures, especially moderate-to-major surgeries31. The ERAS protocol represents a paradigm shift in surgical care delivery and the dissemination and implementation of practice changes32. The adoption of the ERAS protocol aims to facilitate rapid, uncomplicated postoperative recovery with both short-term and long-term benefits, improving patients' quality of life and saving expenses33.
In this retrospective study, the difference in the postoperative outcomes of patients with DFU between the ERAS group and the non-ERAS group were compared. The results showed that participants in the ERAS group experienced superior and more rapid recoveries than those in the non-ERAS group. Furthermore, the implementation of ERAS care resulted in reduced hospital costs and shortened LOS, ultimately enhancing the quality and effectiveness of surgical procedures and recovery.
Counseling plays an integral role in any surgical procedure, serving not only to obtain informed consent but also to alleviate the fears associated with both the disease and the surgery. It provides patients with an understanding of short-term perioperative and long-term rehabilitation outcomes34. Effective counseling and communication positively impact the perception of the surgical procedure and the overall expectations about recovery from surgery and the disease35. Providing detailed information on the planned surgical procedure might reduce fear and provide awareness about the anesthetic procedure and surgery-related pain36. Similarly, care and education on the severity of postoperative pain significantly alleviate postoperative pain, thus improving the postoperative course37. In this study, the ERAS group acquired a lower APAIS score by providing targeted psychological counseling and communication with participants. It helped participants to acquire a rational understanding of DFU, which is chronic and difficult to heal. It is crucial to emphasize holistic diagnosis and treatment because DFU is always accompanied by multiple organ dysfunctions. Further, it provided participants with a firm confidence in surviving DFU and long-term recovery.
Perioperative thermal management can effectively prevent the occurrence of hypothermia. The probability of wound infection can increase by 2–3 times on account of intraoperative hypothermia, leading to abnormal coagulation function, blood loss, and arrhythmia occurring at a significantly higher rate38. Hypothermia potentially promotes surgical site infections via three mechanisms. First, hypothermia triggers postoperative thermoregulatory arterio-venous shunt constriction39, which potentially reduces the delivery of immune cells to injured tissues. Second, hypothermia decreases tissue oxygenation40, which is required for the major oxidative killing of bacteria41. Third, mild core hypothermia directly impairs immune function, including the chemotaxis and phagocytosis of granulocytes, reduces macrophage mobility, and decreases antibody production. Hypothermia decreases platelet aggregation42 and impairs the functions of enzymes in the coagulation cascade43,44. The best-documented complication of perioperative hypothermia is coagulopathy, which requires transfusion. Meta-analyses in 2008 and 2020 both reported that active warming reduced the odds of transfusion by at least 22%45,46. As this was a retrospective study, the impact of intraoperative hypothermia on wound infection, abnormal coagulation function, blood loss, and arrhythmia were not studied. However, aggressive intraoperative warming reduced the occurrence of cold-induced shivering and increased patients’ satisfaction with the experience of the anesthetic–surgical procedure.
Regarding the selection of anesthesia for DFU surgery, the traditional approach generally chooses spinal anesthesia as this mode of treatment is more reliable in reducing pain and extending the duration of pain relief47. However, strict prohibition of food and drink is required to prevent the occurrence of central reactive nausea and vomiting, which lead to aspiration48. Postoperative fasting and drinking restriction are also required due to the paralyzing effect of spinal anesthesia on the gastrointestinal tract. Additionally, spinal anesthesia requires the removal of the pillow and for the patient to lie flat for at least 6 h after surgery to prevent adverse consequences, such as headaches caused by low intracranial pressure49, greatly limiting the patients' early active rehabilitation. This study confirmed that ultrasound-guided peripheral nerve blocks (PNBs) can be selected for most of the debridement, repairment, and even amputation surgeries to treat DFU. Since PNB is a local anesthesia, there is no requirement for fasting and drinking restriction before and after surgery. In our study, no statistically significant difference was found in the VAS score of pain between the two groups, proving the reliability of PNBs for DFU surgery. In addition to offering minimal side effects and a good patient experience, PNB anesthesia allows patients to get out of bed for early active rehabilitation50. This is greatly beneficial for the recovery of gastrointestinal function and cardiopulmonary function in DFU patients.
Nutritional status is crucial for wound healing. A chronic wound requires more nutrients to repair damaged tissue and address nutrient loss through wound inflammatory exudate. Malnutrition exists in patients with chronic diabetic foot wounds51, and specific micronutrient deficiencies are common and associated with impaired wound healing and an increased risk of amputation in people with DFU52,53. Therefore, nutritional supplements can improve DFU healing. Current Australian guidelines recommend the evaluation of nutritional status when progressing towards DFU closure54 and the use of oral nutritional supplements (ONS) when an oral diet is not sufficient to meet nutritional requirements. In our study, we implemented the following nutritional interventions for general DFU patients: (1) Dietary Modifications. Altering the diet is often the best initial step in nutritional interventions for DFU patients. Patients should reduce intake of unhealthy fats, such as trans fats, saturated fats, and cholesterol, and increase consumption of foods rich in unsaturated fatty acids and nutrients. Sodium intake should be limited to 3.4 g or less per day to help control blood pressure. Oral Nutritional Supplements (ONS) can be taken between meals, as needed, to provide additional protein and micronutrients. Patients should vary their food and supplement choices to avoid taste fatigue. When simple dietary changes are insufficient, high-calorie, high-protein fortified foods and supplements should be provided. (2) Oral Nutritional Supplements (ONS). Solely relying on an appropriate diet is often insufficient to achieve optimal wound healing. For patients at higher risk of malnutrition or already showing signs of malnutrition, initiating ONS as early as possible is crucial. ONS can be liquid, semi-solid, or powder, providing essential nutrients and micronutrients for wound healing. For many DFU patients, ONS is more effective than dietary changes alone. Adding specific supplements such as arginine, glutamine, and HMB to standard care can enhance DFU healing, especially in patients with poor limb perfusion or low albumin levels. Patients should be encouraged to take ONS between meals with appropriate fluids and a balanced diet. (3) Enteral and Parenteral Nutrition. If a patient cannot meet their estimated nutritional, calorie, protein, and hydration needs despite undergoing nutritional interventions, the benefits and risks of enteral or parenteral nutrition should be discussed to provide additional or alternative nutritional support. In this study, the ERAS group had a comparable nutritional score (PG-SGA) to the non-ERAS group after surgery because nutritional interventions for DFU were implemented before the ERAS program in our center. Nutritional intervention, as an important element of ERAS, can improve malnutrition status in patients and promote their recovery after surgery55.
Kobayashi M, et al.56 found that prolonged duration of postoperative bed rest was a significant independent risk factor for postoperative VTE. When lying still in bed, Venous stasis occurs when people are at bedrest, because of altered venous flow characteristics. This is commonly believed to be one etiology behind the development of deep venous thrombosis (DVT)57. In clinical practice, patients who are significantly injured or immobilized are at risk of perioperative thrombotic complications58. Patients with DFU who rely on bed rest acquire postoperative hypercoagulability and thrombophilia with higher risk in the perioperative period of surgery. In our study, a comparison was made between the ERAS group and the non-ERAS group in terms of early mobilization and bed rest after surgery. The incidence of postoperative DVT in both groups was statistically significant, and the low incidence of DVT in the ERAS group demonstrated that early postoperative mobilization of the lower limbs has a positive preventive effect on deep vein thrombosis in the lower limbs. This is consistent with the research results of previous lower limb surgeries, especially knee joint replacement surgeries—Early mobilization in the first 24 h after surgery is proved be a cheap and effective way to reduce the incidence of post-operative deep venous thrombosis59.
For early postoperative rehabilitation exercise (early mobilization), few clinical measures are presently undertaken in China for DFU patients. Furthermore, the DFU wound is located in the foot, and the foot must bear weight when getting out of bed, adversely affecting wound healing, aggravating wound pain, and causing bleeding. This can lead to wound dehiscence and other adverse consequences60. Moreover, the customized price of offloading for the diabetic foot is expensive and cannot be reimbursed by medical insurance61, greatly limiting the demand of patients for decompression treatment of diabetic feet. In our study, we customized a removable knee-high offloading device for participants, enabling early and active rehabilitation after diabetic foot surgery in the ERAS group. The removable knee-high offloading device is the second choice of offloading treatment for promoting ulcer healing recommended by the International Working Group on the Diabetic Foot (IWGDF)62. The first choice is either a total contact cast or nonremovable knee-high walker, the latter of which is always being contraindicated for dressing change or not be tolerated by participant, even it is very effective in the promotion of wound healing63. The removable knee-high offloading device is designed without weight bearing for feet with ulcers, and participants can walk on the ground with it in the early postoperative stage. Postoperative early ambulation can actively promote the recovery of cardiovascular and gastrointestinal functions64. It also psychologically enhances the patient's confidence to return to the self-care accompanying daily life65. The outcomes of this study indicate that wearing a removable knee-high offloading device for diabetic foot after surgery during early mobilization in the ERAS group prevented lower-limb muscle atrophy and lower-limb deep vein thrombosis and had significant benefits for the recovery of the postoperative life ability of patients without affecting wound healing time.
We found that integrating key elements from the ERAS program and adapting them to diabetic foot surgery were beneficial to the surgical treatment of chronic ulcers.
Limitations
Our study suffered from a number of limitations that should be addressed. Firstly, it was only a retrospective, single-center, observational study; thus, its results may display selection bias. Secondly, although we tried to unify the surgical methods, there were individual differences between patients with DFU, and we did not compare the impact of differences in surgical methods on outcomes. Last but not the least, in the future, it will be necessary to design a large-sample prospective randomized controlled trial to fully demonstrate the effectiveness of ERAS in patients with DFU.
Conclusions
According to the results of the comparison between the ERAS and non-ERAS groups, the ERAS protocol could help to improve the medical quality and efficacy by improving the patient satisfaction and activity of daily living scale scores, shortening the LOS, and reducing the hospital cost. Additionally, it reduced perioperative complications and improved clinical outcomes by reducing anxiety symptoms, the incidence of DVT, and the reduction in the circumference of the lower limbs. In brief, the ERAS protocol was feasibly and safely adopted in DFU patients after surgery.
Data availability
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Abbreviations
- ERAS:
-
Enhanced recovery after surgery
- DFU:
-
Diabetic foot ulcer
- LOS:
-
Length of stay
- DVT:
-
Deep vein thrombosis
- NRS:
-
Numerical rating scale
- NRS-2002:
-
Nutritional risk screening 2002
- PG-SGA:
-
Patient-generated subjective global assessment
- APAIS:
-
The Amsterdam preoperative anxiety and information scale
- FTS:
-
Fast-track surgery
- MDT:
-
Multidisciplinary treatment
- IWGDF:
-
International working group on the diabetic foot
- ABI:
-
Ankle brachial index
- CRP:
-
C-reactive protein
- ONS:
-
Oral nutritional supplements
- PNBs:
-
Peripheral nerve blocks
References
Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 78(5), 606–617 (1997).
Fearon, K. C. et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin. Nutr. 24(3), 466–477 (2005).
Wexner, S. D. Standardized perioperative care protocols and reduced lengths of stay after colon surgery. J. Am. Coll. Surg. 186(5), 589–593 (1998).
Lillemoe, H. A. & Aloia, T. A. Enhanced recovery after surgery: hepatobiliary. Surg. Clin. North. Am. 98(6), 1251–1264 (2018).
Kaye, A. D. et al. Enhanced recovery pathways in orthopedic surgery. J. Anaesthesiol. Clin. Pharmacol. 35(Suppl 1), S35–S39 (2019).
Bogani, G., Sarpietro, G., Ferrandina, G., Gallotta, V. & Donato, D. I. Enhanced recovery after surgery (ERAS) in gynecology oncology. Eur. J. Surg. Oncol. 47(5), 952–959 (2021).
Engelman, D. T. et al. Guidelines for perioperative care in cardiac surgery: enhanced recovery after surgery society recommendations. JAMA Surg. 154(8), 755–766 (2019).
Ljungqvist, O., Scott, M. & Fearon, K. C. Enhanced recovery after surgery: a review. JAMA Surg. 152(3), 292–298 (2017).
Choi, S. K. et al. Factors associated with a prolonged length of hospital stay in patients with diabetic foot: a single-center retrospective study. Arch. Plast. Surg. 44(6), 539–544 (2017).
Stancu, B. et al. Diabetic foot complications: a retrospective cohort study. Int. J. Environ. Res. Public Health 20(1), 187 (2022).
Armstrong, D. G., Tan, T. W., Boulton, A. J. M. & Bus, S. A. Diabetic foot ulcers: a review. JAMA 330(1), 62–75 (2023).
Rinkel, W. D. et al. In-hospital costs of diabetic foot disease treated by a multidisciplinary foot team. Diabetes Res. Clin. Pract. 132, 68–78 (2017).
Wainwright, T. W. et al. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: enhanced recovery after surgery (ERAS®) Society recommendations. Acta Orthop. 91(1), 3–19 (2020).
Ahluwalia, R., Lázaro-Martínez, J. L., Reichert, I. & Maffulli, N. Advances in pharmacotherapy for diabetic foot osteomyelitis. Expert Opin Pharmacother. 22(16), 2281–2291 (2021).
Aicale, R., Cipollaro, L., Esposito, S. & Maffulli, N. An evidence based narrative review on treatment of diabetic foot osteomyelitis. Surgeon 18(5), 311–320 (2020).
Ahluwalia, R., Maffulli, N., Lázaro-Martínez, J. L., Kirketerp-Møller, K. & Reichert, I. Diabetic foot off loading and ulcer remission: Exploring surgical off-loading. Surgeon 19(6), e526–e535 (2021).
Jiang, X. et al. Pain management in people with diabetes-related chronic limb-threatening ischemia. J. Diabetes Res. 2021, 6699292 (2021).
Hersberger, L. et al. Nutritional risk screening (NRS 2002) is a strong and modifiable predictor risk score for short-term and long-term clinical outcomes: secondary analysis of a prospective randomised trial. Clin. Nutr. 39(9), 2720–2729 (2020).
Armstrong DG, Mills JL, Molina M, et al. Nutrition interventions in adults with diabetic foot ulcers: expert consensus and guidance. https://www.guidelinecentral.com/guideline/502765/ pocket-guide/502768/, 2022–04–10.
Society for Prevention and Control of Tissue Inflammation and Injury of Chinese Preventive Medicine Association; Society of Parenteral and Enteral Nutrition of Chinese Medical Association; Diabetic Foot Group, Committee of Peripheral Vascular Disease, China Society of Integrated Traditional Chinese and Western Medicine. Medical nutrition treatment guideline for diabetic foot. Chin. J. Tissue Eng. Res., 2019, 23 (35): 5682–5689.
Kulprachakarn, K., Ounjaijean, S., Wungrath, J., Mani, R. & Rerkasem, K. Micronutrients and natural compounds status and their effects on wound healing in the diabetic foot ulcer. Int. J. Low Extrem Wounds 16(4), 244–250 (2017).
Chinese Nutrition Society. Dietary Guidelines for Chinese Residents (2022). People's Medical Publishing House.
Sessler, D. I. et al. Protect Investigators. Aggressive intraoperative warming versus routine thermal management during non-cardiac surgery (PROTECT): a multicentre, parallel group, superiority trial. Lancet 399(10337), 1799–1808 (2022).
Ding, Y., Yao, P., Li, H., Zhao, R. & Zhao, G. Evaluation of combined radiofrequency and chemical blockade of multi-segmental lumbar sympathetic ganglia in painful diabetic peripheral neuropathy. J. Pain Res. 11, 1375–1382 (2018).
Wood, H. High-frequency spinal cord stimulation alleviates painful diabetic neuropathy. Nat. Rev. Neurol. 17(5), 262 (2021).
Celik, F. & Edipoglu, I. S. Evaluation of preoperative anxiety and fear of anesthesia using APAIS score. Eur. J. Med. Res. 23(1), 41 (2018).
Clemente, G., Gallo, M. & Giorgini, M. AMD – Associazione Medici Diabetologi “Diabetes and Cancer” working group. Modalities for assessing the nutritional status in patients with diabetes and cancer. Diabetes Res. Clin. Pract. 142, 162–172 (2018).
Karcioglu, O., Topacoglu, H., Dikme, O. & Dikme, O. A systematic review of the pain scales in adults: Which to use?. Am. J. Emerg. Med. 36(4), 707–714 (2018).
Ocagli, H., Cella, N., Stivanello, L., Degan, M. & Canova, C. The Barthel index as an indicator of hospital outcomes: a retrospective cross-sectional study with healthcare data from older people. J. Adv. Nurs. 77(4), 1751–1761 (2021).
Noba, L. et al. Costs and clinical benefits of enhanced recovery after surgery (ERAS) in pancreaticoduodenectomy: an updated systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 149(9), 6639–6660 (2023).
Rollins, K. E., Lobo, D. N. & Joshi, G. P. Enhanced recovery after surgery: current status and future progress. Best Pract. Res. Clin. Anaesthesiol. 35(4), 479–489 (2021).
Sapin, A. et al. Enhanced recovery after surgery for sleeve gastrectomies: improved patient outcomes. Surg. Obes. Relat. Dis. 17(9), 1541–1547 (2021).
Ljungqvist, O. et al. Opportunities and challenges for the next phase of enhanced recovery after surgery: a review. JAMA Surg. 156(8), 775–784 (2021).
Bleasel, A. Pre-surgical counseling. Epilepsy Behav. 141, 109137 (2023).
Scheib, S. A., Thomassee, M. & Kenner, J. L. Enhanced recovery after surgery in gynecology: a review of the literature. J. Minim. Invasive Gynecol. 26(2), 327–343 (2019).
Refai, M. et al. Enhanced recovery after thoracic surgery: patient information and care-plans. J. Thorac. Dis. 10(Suppl 4), S512–S516 (2018).
Egbert, L. D., Battit, G. E., Welch, C. E. & Bartlett, M. K. Reduction of postoperative pain by encouragement and instruction of patients: a study of doctor–patient rapport. N Engl. J. Med. 270, 825–827 (1964).
Peiris, A. N., Jaroudi, S. & Gavin, M. Hypothermia. JAMA 319(12), 1290 (2018).
Carvalho, F., Magalhaes, C., Fernandez-Llimos, F., Mendes, J. & Gonçalves, J. Skin temperature response to thermal stimulus in patients with hyperhidrosis: a comparative study. J. Therm. Biol. 109, 103322 (2022).
Sheffield, C. W. et al. Centrally and locally mediated thermoregulatory responses alter subcutaneous oxygen tension. Wound Repair Regen 4(3), 339–345 (1996).
Allen, D. B. et al. Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch. Surg. 132(9), 991–996 (1997).
Michelson, A. D. et al. Reversible inhibition of human platelet activation by hypothermia in vivo and in vitro. Thromb. Haemost. 71(5), 633–640 (1994).
Felfernig, M. et al. Effects of temperature on partial thromboplastin time in heparinized plasma in vitro. Eur. J. Anaesthesiol. 18(7), 467–470 (2001).
Rohrer, M. J. & Natale, A. M. Effect of hypothermia on the coagulation cascade. Crit. Care Med. 20(10), 1402–1405 (1992).
Rajagopalan, S., Mascha, E., Na, J. & Sessler, D. I. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 108(1), 71–77 (2008).
Balki, I. et al. Effect of perioperative active body surface warming systems on analgesic and clinical outcomes: a systematic review and meta-analysis of randomized controlled trials. Anesth. Analg. 131(5), 1430–1443 (2020).
Zhang, X., JingWang, G. W., Li, L., LiangYu, L. K. & Li, N. Nursing methods and experience of local anesthesia patients under arthroscope. Scanning 2022, 3689344 (2022).
Huh, H. Postoperative nausea and vomiting in spinal anesthesia. Korean J. Anesthesiol. 76(2), 87–88 (2023).
Swyden S, Carter C, Shah SU. Intracranial Hypotension. 2023. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing
Restrepo-Holguin, M., Kopp, S. L. & Johnson, R. L. Motor-sparing peripheral nerve blocks for hip and knee surgery. Curr. Opin. Anaesthesiol. 36(5), 541–546 (2023).
Lauwers, P. et al. Malnutrition and its relation with diabetic foot ulcer severity and outcome: a review. Acta Clin. Belg. 77(1), 79–85 (2022).
Pena, G. et al. Micronutrient status in diabetic patients with foot ulcers. Adv. Wound Care (New Rochelle) 9(1), 9–15 (2020).
Brookes, J. D. L. et al. Broad-ranging nutritional deficiencies predict amputation in diabetic foot ulcers. Int. J. Low Extrem. Wounds 19(1), 27–33 (2020).
Chen, P. et al. Australian diabetes-related foot disease guidelines & pathways project. Australian guideline on wound healing interventions to enhance healing of foot ulcers: part of the 2021 Australian evidence-based guidelines for diabetes-related foot disease. J. Foot Ankle Res. 15(1), 40 (2022).
Basiri, R. et al. Nutritional supplementation concurrent with nutrition education accelerates the wound healing process in patients with diabetic foot ulcers. Biomedicines 8(8), 263 (2020).
Kobayashi, M. et al. Prevalence and risk factors for the development of venous thromboembolism after spinal tumor surgery. World Neurosurg. 164, e177–e182 (2022).
Rosenfeld, B. A., Faraday, N., Campbell, D., Sakima, N. & Bell, W. The effects of bedrest on circadian changes in hemostasis. Thromb. Haemost. 72(2), 281–284 (1994).
Nielsen, V. G. & Asmis, L. M. Hypercoagulability in the perioperative period. Best Pract. Res. Clin. Anaesthesiol. 24(1), 133–144 (2010).
Lei, Y. T., Xie, J. W., Huang, Q., Huang, W. & Pei, F. X. Benefits of early ambulation within 24 h after total knee arthroplasty: a multicenter retrospective cohort study in China. Mil. Med. Res. 8(1), 17 (2021).
Chen, P. et al. Guidelines on interventions to enhance healing of foot ulcers in people with diabetes (IWGDF 2023 update). Diabetes Metab. Res. Rev. 25, e3644 (2023).
Tran, K. & Spry, C. Custom-made foot orthoses versus prefabricated foot orthoses: a review of clinical effectiveness and cost-effectiveness [Internet] (Canadian Agency for Drugs and Technologies in Health, Ottawa (ON), 2019).
Bus, S. A. et al. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab. Res. Rev. 25, e3647 (2023).
Lazzarini, P. A. et al. Effectiveness of offloading interventions to heal foot ulcers in persons with diabetes: a systematic review. Diabetes Metab. Res. Rev. 36, e3275 (2020).
Tazreean, R., Nelson, G. & Twomey, R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J. Comp. Eff. Res. 11(2), 121–129 (2022).
Schrempf, M. C. et al. Immersive virtual reality fitness games to improve recovery after colorectal surgery: a randomized single blind controlled pilot trial. Games Health J. 12(6), 450–458 (2023).
Acknowledgements
The authors thank all subjects who participated in this study.
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Y.F.Y., L.L., L.G., S.Y.H., Y.J.D. and W.Y.R. The first draft of the manuscript was written by X.Y.Q. and J.N.W., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qin, X., Yin, Y., Liu, L. et al. A retrospective cohort study on enhanced recovery after surgery (ERAS) in patients with diabetic foot ulcer. Sci Rep 14, 18171 (2024). https://doi.org/10.1038/s41598-024-69150-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-69150-8
