
Abstract
The COVID-19 pandemic has increased germ aversion, an aversive affective response to a high likelihood of pathogen transmission. While psychological factors are associated with chronic pain, the relationship between germ aversion and chronic pain remains unexplored. This study aimed to examine the relationship between germ aversion and new-onset and prognosis of chronic pain using longitudinal data collected during the COVID-19 pandemic. We conducted web-based surveys of full-time workers at baseline and after three months. Data were collected on demographic characteristics, psychological factors, and chronic pain. Germ aversion was assessed using a modified Perceived Vulnerability to Disease scale. We analyzed responses from 1265 panelists who completed the survey twice. The prevalence of chronic low back pain (CLBP) and chronic neck and shoulder pain (CNSP) was associated with sex, short sleep duration, psychological distress, loneliness, and germ aversion. Stratified analyses showed that germ aversion was a risk factor for CLBP at three months in both individuals with and without CLBP at baseline, and for CNSP at three months in those with CNSP at baseline, even after adjustment for confounders. In conclusion, this preliminary study suggests that high germ aversion is a risk factor for CLBP and CNSP in young and middle-aged workers.
Similar content being viewed by others


Introduction
Coronavirus disease 2019 (COVID-19) is a serious infectious disease that has spread worldwide. The COVID-19 pandemic has created an enormous fear of infection and restricted social activities to an unprecedented degree. Although the situation is waning, there is always the possibility of a new infectious disease epidemic.
The behavioral immune system, which evolved separately from the physiological immune system, is a psychological mechanism that detects cues of infectious agents in the immediate environment, triggers disease-relevant responses, and facilitates behavioral avoidance or escape1. Germ aversion, a major component of the behavioral immune system, is defined as an aversive affective response to situations that imply a relatively high likelihood of pathogen transmission2. An Australian study found that germ aversion among university students during the lockdown in the spring of 2020 was higher than that before the COVID-19 pandemic3.
Psychological factors, such as depression, anxiety, and negative beliefs, are associated with noncommunicable diseases and chronic pain. Chronic pain, defined as pain that persists or recurs for more than three months, is a common health problem affecting over 30% of the global population according to previous studies4,5. A Japanese national survey conducted in 2019 reported that low back pain, neck and shoulder pain, joint pain, and headaches were the most common subjective symptoms6. Chronic pain has been shown to reduce quality of life and cause significant economic losses7,8. Therefore, understanding the pathophysiology of chronic pain and developing treatments for it are important. Psychological factors are associated not only with the development of chronic pain but also with a worse prognosis of chronic pain, including chronic musculoskeletal pain9,10,11,12. Negative psychological factors increase pain sensitivity and the tendency to limit activities, further exacerbating pain and creating a vicious cycle of chronic musculoskeletal pain13.
During the COVID-19 pandemic, germ aversion has the potential to cause activity limitations and negative psychological factors, such as feelings of loneliness14, suggesting that germ aversion may be associated with chronic pain. However, no study has investigated the relationship between germ aversion and chronic pain, including chronic musculoskeletal pain. In this study, we investigated the relationship between germ aversion, the onset of new chronic musculoskeletal pain, and its prognosis using longitudinal data collected during the COVID-19 pandemic.
Methods
This study was conducted as part of a multi-wave longitudinal research project organized by the Shimazu Laboratory (Faculty of Policy Management, Keio University, https://hp3.jp/project/study-on-covid-19-and-worker-well-being) using web-based, self-reported questionnaire surveys. All surveys were supported by a large Internet research agency (Rakuten Insight, Inc.), which had approximately 2.2 million qualified panelists in 2019. The questionnaires were distributed to 1600 full-time workers aged 20–59 years who were stratified by sex (male and female) and age (20–29, 30–39, 40–49, and 50–59 years) to control for selection bias15. The panelists were selected for each sex and age category using simple random sampling, consented to participate in the survey through the designated website, and responded to the questionnaires with the option of not responding to or withdrawing at any point.
We used data from the third survey (baseline), conducted from December 8 to December 17, 2020, and the fourth survey, conducted from March 8 to March 12, 2021 (three months later), because we began to include the germ aversion questionnaire from the third survey.
We collected data including age, sex, height, weight, highest educational level achieved, marital status, sleep duration, smoking status (current smoker or not), teleworking opportunity, frequency of low back, neck, and shoulder pain (rarely, sometimes, often, and always), and psychological status (germ aversion, loneliness, and psychological distress). Chronic pain is generally defined as pain that persists for more than three months. However, due to the absence of specific items assessing the duration of pain in the questionnaire, chronic pain was defined as “always” in the pain frequency category.
Ethics
This study was approved by the Institutional Ethics Committee of the SFC Research Ethics Committee of the Keio University School (approval number: 336). The protocol was registered in the UMIN Clinical Trials Registry (UMIN-CTR ID: UMIN000040683). This study was performed in accordance with the relevant guidelines/regulations and the Declaration of Helsinki, and informed consent was obtained from all participants.
Germ aversion
Germ aversion refers to beliefs about personal susceptibility to infectious diseases and the emotional discomfort associated with potential disease transmission2. The Perceived Vulnerability to Disease (PVD) scale, consisting of 15 items, measures vulnerability to infectious diseases from two aspects: perceived infectiousness, which pertains to susceptibility to colds and flu, and germ aversion, which is the discomfort experienced when pathogens are likely to be present, such as when touching unhygienic objects2. The two-factor structure and internal consistency of the scale have been confirmed by analyzing survey data from college students of various ethnic backgrounds16.
We modified the germ aversion portion of the PVD to fit the current context of our society. The original version included items about situations that are rare today, such as “I do not like to write with a pencil someone else has obviously chewed on’ and “I avoid using public telephones because of the risk that I may catch something from the previous user.” These items were excluded from the questionnaire used in this study. Additionally, an item with the lowest factor loading (0.38)16 in the original scale, “It does not make me anxious to be around sick people,” was rephrased to “It makes me anxious to be around people without masks.”
The germ aversion questionnaire in this study consisted of six items scored on a 7-point Likert scale, ranging from 0 (“strongly disagree”) to 6 (“strongly agree”), with two items scored in reverse for a total of 36 points (Table 1). We calculated factor loadings for validity using a confirmatory factor analysis and assessed internal consistency using Cronbach’s alpha to evaluate the reliability of the modified germ aversion questionnaire.
Assessment of loneliness
Loneliness was assessed using the Japanese version of the University of California, Los Angeles Loneliness Scale (Version 3) and the Short Form 3-item scale (UCLA-LS3-SF3) to assess loneliness. Although this scale was originally developed in English, both the English and Japanese versions have been previously found to be valid and reliable17,18. The items were as follows: (1) “How often do you feel that you lack companionship?”, (2) “How often do you feel left out?”, and (3) “How often do you feel isolated from others?”. Participants rated the frequency with which they experienced these feelings on a 3-point scale [1 (hardly ever), 2 (some of the time), 3 (often)] of 1 to 3. The Cronbach’s alpha for the internal consistency of the loneliness scale was 0.93.
Assessment of psychological distress
Psychological distress was assessed using the Japanese version of the Kessler Psychological Distress Scale (K6), which was well validated in the previous study (Cronbach’s α = 0.85)19,20,21. Participants rated their psychological distress over the past 30 days on a 5-point scale, with frequencies ranging from 0 (never) to 4 (always) for the six K6 items (e.g., nervousness, worthlessness). Higher scores indicate greater psychological distress. Consistent with previous studies, participants who scored 13 or more points were classified as having severe psychological distress21,22.
Statistical analysis
First, we compared the demographic characteristics at baseline between people with and without chronic low back pain (CLBP) three months later. The t-test was used for continuous data, and the chi-square test was used for categorical data. Second, multivariable logistic regression analyses including age, sex, body mass index (BMI), highest educational level achieved, marital status, sleep duration, smoking status, teleworking opportunities, loneliness, and psychological distress as confounding factors, were performed to identify the relationship between germ aversion and the prevalence of CLBP at baseline.
Finally, we stratified people based on the presence of CLBP at baseline and performed the same regression analysis to identify the associations of germ aversion with new-onset CLBP and recovery from CLBP at three months.
Furthermore, similar analyses were performed for people with chronic neck and shoulder pain (CNSP).
All statistical analyses were performed by the JMP® Version 16.0.0 (SAS Institute) software package. Statistical significance was determined using two-tailed p-values < 0.05.
Results
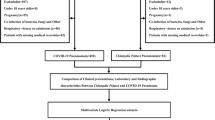
Of the 1600 people who received the questionnaire, 1386 panelists (86.6%) responded at baseline and 1345 panelists (84.1%) responded three months later; 1265 panelists (79.1%) completed the survey twice (Fig. 1).

Flowchart of study participants and prevalence of chronic musculoskeletal pain. CLBP Chronic low back pain, CNSP chronic neck and shoulder pain.
In the reliability analysis, Cronbach’s alpha of the modified germ aversion questionnaire was 0.67. Table 1 presents the factor loadings of the items.
Table 2 shows demographic characteristics at baseline between people with and without CLBP, and between those with and without CNSP. People with CLBP or CNSP had a significantly higher prevalence among females, people with short sleep duration (< 5 h), and people with psychological distress (K6 ≥ 13), as well as greater feelings of loneliness and the germ aversion.
Multivariable logistic regression analyses for people with CLBP and CNSP after three months (Table 3) showed significant associations of the germ aversion with prevalence of the CLBP (odds ratio [OR] = 1.34; 95% confidence interval [CI] 1.14–1.57; p < 0.001) and the CNSP (OR = 1.35; 95% CI 1.17–1.54; p < 0.001), even under adjustment of confounding factors. Sex, short sleep duration, and psychological distress were significantly associated with CLBP and CNSP.
In the stratified analyses of people without CLBP at baseline, the odds ratio of germ aversion with the prevalence of CLBP three months later was significantly high (OR = 1.35; 95% CI 1.03–1.76; p = 0.031, Table 4). Similarly, the stratified logistic regression analysis among people with the CLBP at baseline identified a significantly high odds ratio of the germ aversion with the prevalence of the CLBP at three months (OR = 1.50; 95% CI 1.09–2.07; p = 0.010, Table 4).
According to another stratified analysis by the prevalence of the CNSP at baseline (Table 5), there was no statistical significance of association between the germ aversion and the prevalence of the CNSP at three months alter among people without the CNSP at baseline (OR 1.16; 95% CI 0.92–1.47; p = 0.206). On the other hand, the odds ratio of the germ aversion with the prevalence of the CNSP at three months was significantly high in people with the CNSP at baseline (O = 1.36; 95% CI 1.05–1.77; p = 0.020).
Discussion
This longitudinal study conducted during the COVID-19 pandemic suggests that germ aversion is a risk factor for new-onset CLBP and inhibits recovery from CLBP and CNSP in young and middle-aged workers.
We assessed the internal consistency of the modified germ aversion questionnaire using Cronbach’s alpha, a measure of reliability. Typically, values in the range of 0.7 to 0.9 indicate good reliability. However, Cronbach’s alpha of the Japanese version of the PVD (15 items) was 0.73, and that of the Japanese germ aversion (8 items) was 0.6716. The result of this study (Cronbach’s alpha = 0.67) was less than 0.7, which is not ideal, but not less than that of the previous validation study, indicating that the modified germ aversion scale has reasonable internal consistency. The low loading of the items “I feel comfortable sharing a water bottle with a friend” and “My hands do not feel dirty after touching money” in the germ aversion questionnaire may be because the custom of sharing a bottle with a friend is not common, and cashless payment is becoming more common, and touching money is decreasing.
The results of the demographic characteristics at baseline suggested that females, people with germ aversion, people with psychological distress, and people with less sleep were more likely to have CLBP and CNSP. The finding that CLBP is more common in females is consistent with the results of a previous study that examined the global prevalence of CLBP23. Previous systematic reviews have concluded that psychological distress prolongs CLBP24. A prospective study reported that short sleep duration is a risk factor for chronic musculoskeletal pain, similar to the findings of this study25. Thus, the population in this study had shown a general trend toward chronic musculoskeletal pain.
In the multivariable logistic regression analyses, germ aversion was associated with the prevalence of CLBP and CNSP, even after adjusting for confounding factors, including psychological distress. General mechanisms of psychological factors working for chronic musculoskeletal pain includes both biological processes such as neuromechanisms26,27 and behavioral processes such as sedentary behavior resulting from fear of movement13,28,29. Given that germ aversion is associated with COVID-19 concern as shown in a previous study30, we can consider a similar mechanism to general psychological factors in the effect of germ aversion on musculoskeletal pain. In the COVID-19 pandemic, it has been reported that higher levels of germ aversion are associated with greater disease-avoidance behaviors31,32 and social distancing adherence33. Similarly, sedentary behavior associated with germ aversion may have led to CLBP and CNSP in this study. Although most people during the COVID-19 pandemic lived at a low activity level, those with high germ aversion may have had more sedentary behavior, which may have led to CLBP and CNSP. On the other hand, telework opportunity was not associated with CLBP and CNSP in this study. Although telework drives staying at home, sedentary behaviors other than work-related aspects may have contributed to our findings.
Stratified analyses showed that germ aversion was a risk factor for new-onset CLBP. Even among people without pain at baseline, chronicity is likely to occur after acute low back pain if germ aversion is high. Since higher germ aversion is also associated with a higher prevalence of CLBP at three months among individuals with CLBP at baseline, recovery from CLBP is likely to be difficult under conditions of high germ aversion. These longitudinal results suggest that germ aversion is a risk factor for CLBP, implying the aforementioned biological and behavioral mechanisms. In individuals with CNSP, germ aversion contributes to delayed recovery, with similar mechanisms thought to be responsible. Although there was no significant association with new-onset CNSP, a similar trend was observed. The lack of statistical significance may be due to the small sample size and observation period, which, if increased, may have revealed significant differences.
The behavioral immune system is likely to be more activated in individuals with higher germ aversion when the threat of an infectious disease arises1. The association between germ aversion and chronic musculoskeletal pain may involve excessive behavioral restriction due to activation of the behavioral immune system. Indeed, behavioral restriction increases the likelihood of protection from infection; however, the results of this study suggest that noninfectious diseases such as chronic musculoskeletal pain may increase. Overall, we need to avoid excessive behavioral restrictions and provide psychological reassurance against infections and epidemics. To achieve this, we need to provide accurate information about infectious diseases and encourage appropriate behaviors from multiple perspectives, including both communicable and noncommunicable diseases.
The present study had several limitations. First, the target population was limited to those aged 20 to 59 years who were employed full-time; therefore, it is unclear whether the same conclusions can be applied to the rest of the population. Second, we did not assess the external validity or reliability of the modified germ aversion questionnaire, so our results are preliminary, and further studies are needed to confirm its scientific usefulness. Third, as we did not adhere to the common definition of chronic pain, which is pain persisting for three months or more, there is a possibility that the chronic pain identified in this study cannot be generalized. Additionally, we could not clarify the relationship between germ aversion and pain intensity, as the intensity of chronic musculoskeletal pain was not assessed in this survey. Fourth, pain-specific psychological factors, such as pain catastrophizing, were not assessed. Therefore, further studies are needed to identify the actual psychological mechanisms underlying the development of chronic musculoskeletal pain due to germ aversion. Fifth, the individuals’ history of COVID-19 infection or vaccination was unknown, although these experiences should be associated with the intensity of germ aversion. Moreover, the relationship between chronic musculoskeletal pain and these experiences remains unclear. Sixth, the results of the present study may be specific to a situation in which COVID-19 was prevalent, and it is not clear whether our findings would be replicated in other situations.
In conclusion, this preliminary study suggested that high germ aversion is a risk factor for the new onset of CLBP and delayed recovery from CLBP and CNSP in young and middle-aged workers. Our findings provide important evidence for making clinical suggestions to prevent the development of chronic musculoskeletal pain in people with low back pain or neck and shoulder pain. Additionally, given that chronic musculoskeletal pain corresponding to greater germ aversion is also a socioeconomic burden, our findings suggest that there will be a greater social cost–benefit in managing physical and psychological safety against emerging infectious diseases. Even after the COVID-19 pandemic subsides, the present study will be helpful for our lives and activities during the next pandemic situation of a new infectious disease.
Data availability
The data are available upon request. The data analyzed in this study are available with permission from the Shimazu Laboratory (Faculty of Policy Management, Keio University, https://hp3.jp/project/study-on-covid-19-and-worker-well-being) and the Institutional Review Board of Keio University School of Medicine corresponding to each request (https://www.ctr.med.keio.ac.jp/rinri/).
References
Schaller, M. & Park, J. H. The behavioral immune system (and why it matters). Curr. Dir. Psychol. Sci. 20, 99–103 (2011).
Duncan, L. A., Schaller, M. & Park, J. H. Perceived vulnerability to disease: Development and validation of a 15-item self-report instrument. Pers. Individ. Dif. 47, 541–546 (2009).
Stevenson, R. J., Saluja, S. & Case, T. I. The impact of the Covid-19 pandemic on disgust sensitivity. Front. Psychol. 11, 600761 (2020).
Treede, R.-D. et al. A classification of chronic pain for ICD-11. Pain 156, 1003–1007 (2015).
Cohen, S. P., Vase, L. & Hooten, W. M. Chronic pain: An update on burden, best practices, and new advances. Lancet 397, 2082–2097 (2021).
Ministry of Health Labor and Welfare. Summary Report of Comprehensive Survey of Living Conditions 2019. https://www.mhlw.go.jp/english/database/db-hss/cslc-report2019.html (2020).
Leadley, R. M. et al. Healthy aging in relation to chronic pain and quality of life in Europe. Pain Pract. 14, 547–558 (2014).
Gatchel, R. J., McGeary, D. D., McGeary, C. A. & Lippe, B. Interdisciplinary chronic pain management: past, present, and future. Am. Psychol. 69, 119–130 (2014).
Boersma, K. & Linton, S. J. Expectancy, fear and pain in the prediction of chronic pain and disability: A prospective analysis. Eur. J. Pain 10, 551–557 (2006).
van der Windt, D., Croft, P. & Penninx, B. Neck and upper limb pain: more pain is associated with psychological distress and consultation rate in primary care. J. Rheumatol. 29, 564–569 (2002).
van der Windt, D. A. W. M., Kuijpers, T., Jellema, P., van der Heijden, G. J. M. G. & Bouter, L. M. Do psychological factors predict outcome in both low-back pain and shoulder pain?. Ann. Rheum. Dis. 66, 313–319 (2007).
Nijrolder, I., van der Windt, D. & van der Horst, H. Prediction of outcome in patients presenting with fatigue in primary care. Br. J. Gen. Pract. 59, e101–e109 (2009).
Vlaeyen, J. W. S. & Linton, S. J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 85, 317–332 (2000).
Yamada, K., Wakaizumi, K., Kubota, Y., Murayama, H. & Tabuchi, T. Loneliness, social isolation, and pain following the COVID-19 outbreak: Data from a nationwide internet survey in Japan. Sci. Rep. 11, 18643 (2021).
Shimazu, A. et al. Frequency of laughter and work engagement among Japanese employees: A cross-sectional study during COVID-19. Ind. Health https://doi.org/10.2486/indhealth.2023-0085 (2023).
Fukukawa, Y., Oda, R., Usami, H. & Kawahito, J. Development of a Japanese version of the perceived vulnerability to disease scale. Shinrigaku Kenkyu 85, 188–195 (2014).
Arimoto, A. & Tadaka, E. Reliability and validity of Japanese versions of the UCLA loneliness scale version 3 for use among mothers with infants and toddlers: A cross-sectional study. BMC Womens. Health 19, 105 (2019).
Hughes, M. E., Waite, L. J., Hawkley, L. C. & Cacioppo, J. T. A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 26, 655–672 (2004).
Kessler, R. C. et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 32, 959–976 (2002).
Furukawa, T. A. et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 17, 152–158 (2008).
Sakurai, K., Nishi, A., Kondo, K., Yanagida, K. & Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 65, 434–441 (2011).
Kessler, R. C. et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 60, 184–189 (2003).
Meucci, R. D., Fassa, A. G. & Faria, N. M. X. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 49, 1 (2015).
Pincus, T., Burton, A. K., Vogel, S. & Field, A. P. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine 27, E109–E120 (2002).
Skarpsno, E. S. et al. The interplay between sleeplessness and high-sensitivity C-reactive protein on risk of chronic musculoskeletal pain: Longitudinal data from the Tromsø Study. Sleep 42, zsz127 (2019).
Petrelis, M., Soultanis, K., Michopoulos, I. & Nikolaou, V. Associations of somatic symptom disorder with pain, disability and quality of life in patients with chronic low back pain. Psychiatrike 34, 221–230 (2023).
Knardahl, S. Psychological and social factors at work: Contribution to musculoskeletal disorders and disabilities. G. Ital. Med. Lav. Ergon. 27, 65–73 (2005).
Baradaran Mahdavi, S., Riahi, R., Vahdatpour, B. & Kelishadi, R. Association between sedentary behavior and low back pain: A systematic review and meta-analysis. Health Promot. Perspect. 11, 393–410 (2021).
Mazaheri-Tehrani, S. et al. Sedentary behavior and neck pain in adults: A systematic review and meta-analysis. Prev. Med. 175, 107711 (2023).
Shook, N. J., Sevi, B., Lee, J., Oosterhoff, B. & Fitzgerald, H. N. Disease avoidance in the time of COVID-19: The behavioral immune system is associated with concern and preventative health behaviors. PLoS One 15, e0238015 (2020).
Safra, L., Sijilmassi, A. & Chevallier, C. Disease, perceived infectability and threat reactivity: A COVID-19 study. Pers. Individ. Dif. 180, 110945 (2021).
Church, L. D., Bounoua, N., Rodriguez, S. N., Bredemeier, K. & Spielberg, J. M. Longitudinal relationships between COVID-19 preventative behaviors and perceived vulnerability to disease. J. Anxiety Disord. 88, 102561 (2022).
Gerretsen, P. et al. Determinants of social distancing adherence. Front. Public Health 10, 977857 (2022).
Acknowledgements
The authors thank all the respondents of this study. We would also like to thank Editage (www.editage.jp) for English language editing.
Funding
This work was supported by Grant-in-Aid for Scientific Research (B), JSPS KAKENHI Grant Number 24K02541 and 24K00498.
Author information
Authors and Affiliations
Contributions
Yuki Mashima contributed to interpretation and drafting of the manuscript. Morihiko Kawate, Yihuan Wu, Yuta Shinohara, Reiko Hoshino, Saki Takaoka, and Chisato Tanaka contributed to study conception and manuscript editing. Masahito Tokita and Akihito Shimazu collected the data. Kenta Wakaizumi designed the study, analyzed the data, edited the first draft, and supervised the study. Morihiko Kawate, Yihuan Wu, Chisato Tanaka, Masahito Tokita, Akihito Shimazu and Kenta Wakaizumi critically revised the manuscript for important intellectual content. All the authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mashima, Y., Kawate, M., Wu, Y. et al. Germ aversion is a risk factor for chronic low back pain and shoulder pain under the COVID-19 pandemic: an internet-based panel study. Sci Rep 14, 19196 (2024). https://doi.org/10.1038/s41598-024-70452-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-70452-0
