
Abstract
Primary dysmenorrhea (PD) is a common global health concern. However, limited studies explored the association between soft drinks intake and PD among female undergraduates in China. To determine the association between soft drinks (carbonated soft drinks, etc.) as well coffee intake and the incidence/severity of PD among female undergraduates in China. We performed a cross-sectional study among 1809 female undergraduates in China from September 29, 2020 to October 22, 2020. The demographic information and menstrual information of the participants were collected by a self-administrated questionnaire. Chi-square test, ANOVA test, and logistic regression test were used to investigate the association between soft drinks intake and the incidence/severity of PD. We also conducted stratification analysis among different locations (rural or urban). The prevalence of PD was 47.1% (n = 852). There were 221 (25.9%) participants suffered from severe pain. In the participants with PD, the OR of carbonated soft drinks intake was 1.244 (95% CI 1.010–1.533). Among the participants with PD from rural areas, the OR of carbonated soft drinks intake was 1.402 (95% CI 1.045–1.881), compared with the non-carbonated soft drink group. In the participants with moderate and severe PD, the OR of coffee intake was 0.451 (95% CI 0.228–0.892), compared with the non-coffee-drinking group. There was a significant association between carbonated soft drinks intake frequency and the severity of PD (P < 0.05). Our study showed that carbonated soft drinks intake is a risk factor for PD, especially in participants from rural areas. Coffee intake is a protective factor for the severity of PD. Periodical awareness programs about adverse effects of excessive soft drink consumption should be introduced to reduce the prevalence and exacerbation of PD. Coffee intake might be helpful to relieve the severity of PD.
Similar content being viewed by others

Introduction
Primary dysmenorrhea (PD) is defined as painful menstruation in absence of pelvic pathological changes, characterized by recurrent, cramp-like lower abdominal pain during menstruation1,2. It doubles as the most common gynecologic condition and one of the most common causes of pelvic pain in pre-menopausal women1,3,4. The prevalence of PD among female university students varies widely, ranging from 45 to 95%5. Though not a life-threatening condition, PD can cause substantial burden on the quality of life2,6. In the United States, about 600 million work hours and 2 billion dollars annual economic loss has been attributed to PD7. In Japan, it has been reported that the total healthcare cost for patients with PD is 2.2 times higher than the healthcare cost for females without dysmenorrhea8. PD is highly prevalent among Chinese college girls, with a high burden of symptoms affecting productivity and assimilation into society9. With a prevalence rate of over 40% among Chinese College girls, there’s the need to understand why10.
Soft drinks include soda water, syrup, or other carbonated or non-carbonated beverages11. Also known sometimes as carbonated beverages or sodas, soft drinks are non-alcoholic beverages that are typically carbonated and flavored. Coffee is considered a beverage that is brewed from roasted coffee beans12. One of the primary ingredients in soft drinks is sugar, with an average content 100 g/L13. The global consumption of soft drinks has increased dramatically over the past several decades with the greatest increase among young people14. While the exact amount differs from study to study, they all indicate that soft drink consumption has been on the rise in China in recent years15, resulting in a remarkably increase in various health conditions and diseases.
Similarly, coffee consumption which was considered a western lifestyle, has significantly gained popularity in China, a country with long history of drinking green tea. The demand for coffee has also grown rapidly in recent years16. Statistical reports show that Chinese population consumed around 4.8 million 60-kg bags of coffee, as coffee production volume in China amounted to around 1.8 million bags in the same period. Although considered a beverage, coffee has a stimulant effect on the human nervous system due to it’s caffeine content17. Notable of these effects are caffeine in coffee possess an antagonistic effect on adenosine A1 and A2A receptors, causing hyperexcitability of the central nervous system18, also affects physical stamina, cognitive function and in some cases amplify symptoms of anxiety19.
A cross-sectional study conducted in Ethiopia in 2016 found that among students who consumed one or more servings of cola daily, the risk of PD was approximately seven times higher than those non-consumers, suggesting a potential link between sugary carbonated beverages and menstrual pain20. Additionally, a cross-sectional study conducted among 857 university students in Turkey in 2009 also found a positive association between excessive intake of sugary beverages, such as cola and the high prevalence of dysmenorrhea21. Our study buttresses the many previous studies examining the prevalence and characteristics of PD among female undergraduates in China. The relationship between soft drinks intake and the incidence and pain severity of PD is not well documented10,20,22,23. The association between coffee intaking and the incidence of dysmenorrhea are controversial. In a 2019 cross-sectional study conducted in Kuwait involving 763 12th-grade female students from public high schools aged between 16 and 21 years, found a significant association between coffee consumption frequency and increased risks of dysmenorrhea6; however, a cross-sectional study conducted in 2020 revealed no significant association between coffee intake and the prevalence of dysmenorrhea among university students in Zimbabwe24.
To bridge research gap, we conducted a cross-sectional study to analyze the association between soft drink and the incidence/severity of PD among Chinese female undergraduates. This is the first study to analyze the association between soft drinks consumption and PD incidence and severity among Chinese female undergraduates. We also did a stratification analysis according to the place of residence (urban or rural).
Methods
Study design and sample size considerations
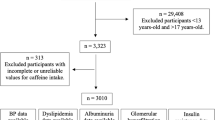
We performed a cross-sectional study to analyze the association between soft drinks intake and the incidence and severity of PD among female undergraduates in China from September 29, 2020 to October 22, 2020. The inclusion criteria of the study are: (1) Students from all across China enrolled in Binzhou Medical University in 2019; (2) Female; (3) No history of gyanecologic pathological changes. The distribution of participants is shown in Fig. 1. All participants had to provide informed consent before participation. This study was approved by Binzhou Medical University ethics committee. We estimated the sample size by

The distribution of the participants.
According to Iacovides’ study9, we conservatively determined that the prevalence (P) is 0.45, and we set permissible error (d) at 0.1p, α = 0.05, then the minimum sample size was calculated to be 489. Finally, we included 1809 samples from the Chinese Undergraduates Cohort (CUC).
Data collection
The participants’ information was collected by a self-administrated questionnaire. This self-administrated questionnaire included demographic information and menstrual information of the participants.
Covariates
Demographic information include age, residence, smoking, passive smoking, physical activity, carbonated soft drinks intake, carbonated soft drinks intake frequency, coffee intake, and coffee intake frequency. Participants were classified into urban and rural areas. In addition, anthropometric data including height and weight were self-reported. Each participant's Body Mass Index (BMI) was calculated as weight in kilograms divided by the height in meters squared. According to the Asian-Population Criteria of the World Health Organization: Underweight is defined as < 18.5 kg/m2, Normal weight ranges from 18.5 to 23.0 kg/m2, Overweight is from 23.0 to 27.5 kg/m2, and Obese is ≥ 27.5 kg/m225. The following demographic information variables were defined as categorical variables and the definitions used were: smoking—at least one cigarette per day in the past three months; passive smoking—at least 15 min of passive smoking per day for the past three months; physical activity—at least once a week for the past three months26. Data about soft drinks or coffee intake were collected by the question, “Do you often drink carbonated soft drinks/coffee?”. People who drank soft drinks or coffee had to report the intake frequency, and the frequency was classified as “ < 1 times/week”, “1–3 times/week”, “4–6 times/week”, “ ≥ 7 times/week”.
Menstrual information included menstrual cycle, menstrual duration and menstrual flow. Collecting menstrual information was based on those questions: “How often have you menstruated in the past three months?”, “What’s the duration of your menstruation in the past three months?”, “How is the menstrual flow in the past three months?”. PD was identified on the basis of the questions, “Have you experienced one or more of menstrual cramps or abdominal pain during your menstrual period in the past three months?”. Participants with PD had to report the level of their pain severity. The pain severity was categorized as mild, moderate, and severe, which are respectively defined as 1–3 points.
Statistical analysis
We divided participants into PD group and normal group according to their PD condition. The χ2 test was used to compare the distribution of PD characteristics across groups with different levels of pain severity. Logistic regression models were employed to assess the association between the intake of soft drinks and the incidence of PD, as well as the association between the intake of coffee and the severity of PD. In logistic regression analysis, PD was designated as the dependent variable, and the independent variables included: coffee, smoking, passive smoking, intake of soft drink, intake of milk tea, tea, physical exercise, BMI and urban versus rural status. A forward stepwise method was utilized for univariate regression to select independent variables, resulting in the most fitting model. Multivariate binary logistic regression was conducted to explore the relationship between the study variables and the incidence and severity of PD. The Kruskal–Wallis test was applied to determine the association between carbonated soft drinks intake frequency and the severity of PD, as well as the association between coffee intake frequency and the severity of PD. For categorical variables, χ2 test with a pre-set P(significance value) ≤ 0.05 was used to test for significant association between soft drinks intake and PD.
We also conducted a stratification analysis according to participants’ places of residence (urban or rural) to investigate the association between soft drinks intake and the incidence of PD among different populations in multiple logistic regression (Table S1). The data extracted from the questionnaires were statistically analyzed using the Statistical Package for Social Sciences (SPSS) 23.0 software after coding all answers. The level of statistically significance was set at P < 0.05.
Results
Characteristics of the study subjects
Table 1 shows the baseline demographic characteristics of participants. A total of 1809 participants were recruited in this study. The majority of the participants in this study were Han Chinese. Additionally, this study also included a small but diverse group of participants from different ethnic backgrounds. Three participants were from the Tujia ethnic group, three from the Yi ethnic group, two from the Buyi ethnic group, two from the Zhuang ethnic group, one from the Manchu ethnic group, one from the Miao ethnic group, one from the Mongolian ethnic group, one from the Bai ethnic group and one from other ethnic groups. The average age of participants was 19.7 ± 1.2 years. There were 852 (47.1%) participants experienced PD in the past three months. For PD group, 51.2% had consumed carbonated soft drinks compared with 48.8% in non-PD group. Moreover, 44.8% participants of the PD group drank coffee, whereas 55.2% in the non-PD group. There were 906 (50.1%) participants from rural areas. The distribution of the severity of PD cases was as follows: mild 24.4% (n = 208), moderate 49.6% (n = 423), and severe 26.0% (n = 221).
Table 2 reflects the baseline menstrual characteristics of participants in both non-PD and PD groups. Both non-PD and PD groups had a similarity in menstrual cycle. It can be noticed in the menstrual flow data of the participants that those in the PD group reported 62.3% having heavy flow as opposed to the 37.7% reported by the non-PD group.
Carbonated soft drinks intake and PD
Table 3 shows the association between carbonated soft drinks intake and the incidence of PD. The results showed that the risk of PD incidence in carbonated soft drink group was about 1.24 times higher (OR = 1.244, 95%CI 1.010–1.533) than non-carbonated soft drink group. Table 4 shows the association between carbonated soft drinks intake frequency and the severity of PD (x̅ ± s). The results found that there is a dose–response relationship between frequencies of carbonated soft drinks intake and the pain severity of PD. For example, when carbonated soft drinks intake frequency is less than once a week, the pain severity is mild. As the frequency of soft drink consumption increases, the pain severity gradually worsens.
Coffee intake and PD
Table 5 shows the association between the amount of coffee intake and the severity of PD. After analyzing the variables related to PD severity, we found that there is a significant association between coffee intake and PD severity. Specifically, participants with moderate to severe PD who consume coffee have lower odds of experiencing severe symptoms, with an odds ratio of 0.451 (95% CI 0.228–0.892) (P < 0.05).
Table 6 shows the association between coffee intake frequency and the severity of PD (x̅ ± s) using Kruskal–Wallis test. The results did not find significant associations between coffee drinking frequencies and severity of PD.
The associations between menstrual flow and the incidence and severity of PD are shown in Tables S2–S4. Menstrual flow and menstrual cycle were associated with the incidence of PD (P < 0.05).
Discussion
This is the first study to analyze the association between soft drinks consumption and PD incidence and severity among Chinese female undergraduates. Our findings revealed a high prevalence of PD, with 47.1% of participants experiencing it, and 26% of those experiencing severe pain. We found that women who consumed carbonated soft drinks had a higher risk of developing PD. However, those who drink more coffee had less chance of developing into sever PD pain.
Prevalence of PD among female undergraduates in China
According to our study, there were 46.1% of PD cases among female undergraduates in China, which is comparable to previous studies that reported rates ranging from 40 to 90%27. A previous study conducted in China indicated that the rate of PD among female university students was 41.7% 10. Our study used a self-administered questionnaire to assess the level of pain severity in the subjects, which showed that 24.4% of participants experienced mild pain, 49.6% had moderate pain, and 26.0% had severe pain. A study conducted in Saudi Arabia confirmed our findings, reporting that 23% of participants experienced mild dysmenorrhea, 50% suffered from moderate pain, and 27% reported severe pain28.
Although there were slight differences in the percentage distribution of pain severity in different studies, most of the results agree that approximately one-fourth of female undergraduates described their PD as severe21. Similarly, studies conducted in Turkey and other countries have reported the prevalence of severe dysmenorrhea to be between 10 and 27%29, indicating that PD is still a significant gynecological and public health issue among female undergraduates. These findings underscore the urgent need for better prevention protocols and intervention measures to address this condition.
Relationship between carbonated soft drinks consumption and PD
Our study further revealed that the intake of carbonated soft drinks had a statistically significant association with the incidence of PD. We also identified a significant relationship between carbonated soft drinks intake frequency and the severity of PD (P < 0.05). Our findings were backed up by several studies conducted in Turkish29, in Ethiopia20 and Indonesia30. These study found a positive correlation between carbonated soft drinks intake and PD incidence31. This could be due to the fact that the high sugar content in carbonated soft drinks can disrupt the absorption and processing of certain vitamins and minerals, leading to nutritional imbalances that can cause abnormal muscle contractions and ultimately muscle spasms29.
Besides, the cause of PD is likely related to the cyclooxygenase pathway producing higher levels of prostanoids, specifically prostaglandins (PGs), in the endometrium during ovulation cycles3,4. Some studies indicate that the concentration of prostaglandin F2α in menstrual fluid is twice as high in women who experience dysmenorrhea compared to those who don’t32. The elevated levels of PGs bring about contractions in the uterus, resulting in the production of anaerobic metabolites that activate pain receptors3. These metabolites may be derive from meals that contain sugar33. The heightened levels of PGs prompt the uterus to contract, which restricts blood flow and generates anaerobic metabolites that activate pain receptors. Prior study has suggested that consuming excessive sugar can impact the amount of steroids circulating in the body34. High-sugar beverages lead to increased cortisol (steroid) levels in young women. Cortisol is a hormone that is released in response to stress and is involved in regulating various physiological processes in the body. A study found that women with PD had higher levels of cortisol compared to women without menstrual pain, suggesting that the dysregulation of the stress response system, which includes cortisol secretion, may be involved in the development of primary dysmenorrhea35.
However, these findings are inconsistent with the results of several other researchers who reported there was no correlation between carbonated soft drinks consumption and PD36,37. The possible explanation may be there should be a threshold amount of carbonated drinks consumed to be able to cause PD. Normal consumption (not excessive) shows no evidence of a direct relationship with PD. Our study found a significant association between carbonated soft drinks intake frequency and the severity of PD (P < 0.05), which could better account for causal associations than ordinary cross-sectional study. However, additional studies are required to explore the connection between drinking carbonated soft drinks and PD.
The relationship between coffee consumption and PD
According to our study, drinking coffee has been shown to potentially decrease the risk of developing PD (P > 0.05). However, this finding contradicts some previous studies that have suggested otherwise23,38. Specifically, our research indicates that among individuals experiencing moderate to severe pain severity from PD, those who consumed coffee had a 0.451 lower risk compared to those who did not consume coffee. However, no significant correlation was found for participants experiencing only mild pain severity from PD.
Our study aligns with a Spanish study that reported a statistically significant association between dysmenorrhea or its severity and factors such as caffeine intake, supporting our results 31. Additionally, a study conducted in Saudi Arabia found a significant association between PD and caffeine consumption28.
The relationship between coffee intake and PD has been the subject of controversy in previous studies. While some studies have reported a positive association between coffee intake and the risk of PD21,39, others have found no correlation between PD and daily coffee consumption37,40. For instance, a study on medical sciences students at Babol University of Medical Sciences demonstrated that the risk of dysmenorrhea was twice as high in individuals who were high consumers of caffeine (≥ 300 mg/day) compared to those who were low/moderate consumers of caffeine (< 300 mg/day) (OR = 1.97, 95% CI 1.09–3.59)39. The conflicting results of these studies contribute to the controversy surrounding the association between coffee intake and PD. The variations in study designs, sample sizes, and populations may be factors influencing the divergent findings. A study conducted in medical students at Babol University of Medical Sciences found that moderate/moderate caffeine consumers (< 300 mg/day) showed a two-fold higher risk of dysmenorrhea (OR = 1.97 (95% CI 1.09–3.59))38. Another cross-sectional study of 1183 women, based on the Shanghai Birth Cohort Study, found that coffee consumption was positively associated with the severity of dysmenorrhea after considering potential confounding factors38.
In contrast, the prospective study of 428 women conducted in Saint Vincent and the Grenadines reported no statistically significant association between PD and caffeinated beverages41. Also, a cross-sectional study conducted in Surakarta on 274 female adolescents aged between 15 and 17 years old found that caffeine intake was not significantly associated with the severity of dysmenorrhea42. Additionally, other studies have shown a correlation between caffeine intake and dysmenorrhea21,41. Caffeine, the main component of coffee, is an adenosine analogue that blocks adenosine receptors (potent vasodilators)43. Blocking these receptors causes vasoconstriction, reducing blood flow to the uterus and making menstrual pain even worse44. Caffeine also has a strong vasoconstrictor effect and has been associated with pelvic pain. The mechanisms by which caffeine may induce crampy pain have not yet been identified and require further research28.
Potential pharmacodynamic effects have been shown for how inn helps in PD. Prostaglandin E1 (PGE1) increases cAMP, which essentially causes smooth muscle relaxation and vasodilation. PGE1 increases during menstruation along with PGE2 and other prostaglandins45. The effectiveness of individual PGs depends on concentration, potency, genetics, etc. Caffeine in coffee synergistically increases PGE1, causing uterine relaxation. Another study showed that a 1 mM concentration of caffeine stimulated cyclic AMP levels to 151% of control levels after 60 min. Higher concentrations of caffeine produced even greater stimulation of cyclic AMP levels46. We believe our findings further clarify the fact that coffee consumption is not always positively correlated with the severity of PD. More study on this topic is needed. Though there are various hypotheses on mechanism of action between PGE1 and cAMP. For example, PGE1 does at least not exclusively act by changing cAMP levels, but rather directly influences cell membrane functions47. We believe that our study result throws more light on the fact that coffee intake doesn’t always bear a positive correlation with severity of PD pains and that more research is required on the subject matter.
Implications for policy and practice
Our study has several public health implications. Our study examined the evidence of adverse effects of soft drinks consumption on Chinese female undergraduates, and found that frequent carbonated soft drinks intake is a risk factor for PD whereas coffee intake is a protective factor for PD. There are known non-modifiable risk factors such as menstrual flow and menstrual cycle, are also identified in our study, which increase the probability of suffering from PD. As modifiable risk factors, carbonated soft drinks intake and coffee intake had a significant association with PD. However, concerning lifestyle and eating habits, and based on our results and previous reports, further studies about soft drinks intake are necessary to provide recommendations on the most advisable diets or lifestyle habits for minimizing the consequences or reducing the risk of PD. Firstly, we should formulate corresponding policies to restrict the sale of soft drinks. In addition to strategies at country level, female undergraduates with PD could try to avoid the frequent intake of soft drinks, especially carbonated soft drinks and find other substitutes such as some type of tea (black tea, matcha green tea, etc.) or coffee.
Limitations and future directions
The advantages of our study are also worth noting. The large sample size made the results more precise. In addition, this study was based on a large cohort, which enables us to involve more potential confounders in the analyses. This study explored the association between soft drinks intake and the incidence as well as the severity of PD among female undergraduates. We have, in our discussion, highlighted a few issues that require further comprehensive research such as carbonated soft drinks intake (a risk factor) and coffee intake (a protective factor). We also divided the degree of PD pain severity into 3 levels of and further explored the impact of soft drinks intake on PD under the different levels of pain severity of PD. What’s more, we have also done the stratification analysis which enabled us explore the association between soft drink consumption and PD in different groups according to their places of residence (urban or rural). Our results indicated a significantly positive association between soft drinks intake and PD, which bear notable public health ramifications.
We are aware of some limitations. First, the study design is a cross-sectional study with no causal interpretation. Second, although the students in the sample are not only from Shandong, there are relatively many students from Shandong, so the sample may not be representative of all Chinese women. Further generalization of results in the future requires an expansion of the proportions of sample in different areas in China. Finally, pain and menstrual flow are measured by subjective assessment methods, which could lead to recall bias and over-reporting or under-reporting of certain variables. Despite these limitations, our study can be used to increase general perceptions of PD among Chinese female students.
Conclusion
Overall, a high portion of female undergraduates suffer from PD in China. We identified that carbonated soft drinks were a risk factor for the occurrence and severity of PD, while coffee consumption was a protective factor against PD. Furthermore, there maybe a dose–response relationship between carbonated soft drinks intake frequency and the severity of pain in PD. Being aware of this makes it possible for health professionals to organize better focused programs to reduce the adverse effects of PD. Our findings highlight the need for interventions to reduce undergraduates’ soft drinks consumption by educating them about the harmful effects of soft drinks.
Data availability
Data described in the manuscript, code book, and analytic code will be made available upon request pending application to and approval from the corresponding author Peng Lu.
References
Kho, K. A. & Shields, J. K. Diagnosis and management of primary dysmenorrhea. JAMA 323, 268–269 (2020).
Dawood, M. Y. Primary dysmenorrhea. Obstet. Gynecol. 108, 428–441 (2006).
Ferries-Rowe, E., Corey, E. & Archer, J. S. Primary dysmenorrhea: Diagnosis and therapy. Obstet. Gynecol. 136, 1047–1058 (2020).
Morales, C. R., Reguera, M., Vallejo, B. M., Ruiz, B. R. & Abuin, V. J. D. Ultrasound assessment of the abdominal wall muscles in women with and without primary dysmenorrhea: A cross-sectional study. Diagnostics 10, 166 (2020).
Iacovides, S., Avidon, I. & Baker, F. C. What we know about primary dysmenorrhea today: A critical review. Hum. Reprod. Update 21, 762–778 (2015).
Al-Matouq, S. et al. Dysmenorrhea among high-school students and its associated factors in Kuwait. BMC Pediatr. 19, 1–12 (2019).
Sultana, K., Fatma, S., Zaidi, S. S. & Khan, S. Primary dysmenorrhoea and its management in unani system of medicine. Eur. J. Pharm. Med. Res. 5, 243–248 (2018).
Sayako, A. et al. Evaluation of the treatment patterns and economic burden of dysmenorrhea in Japanese women, using a claims database. Clinicoecon Outcomes Res. 9, 295–306 (2017).
Chen, L., Tang, L., Guo, S., Kaminga, A. C. & Xu, H. J. B. O. Primary dysmenorrhea and self-care strategies among Chinese college girls: a cross-sectional study. BMJ Open 9, e026813 (2019).
Hu, Z. et al. Prevalence and risk factors associated with primary dysmenorrhea among Chinese female university students: A cross-sectional study. J. Pediatr. Adolesc. Gynecol. 33, 15–22 (2019).
Vartanian, L. R., Schwartz, M. B. & Brownell, K. D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 97, 667–675 (2007).
Malik, V. S. et al. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 33, 2477–2483 (2010).
Lien, L., Lien, N., Heyerdahl, S., Thoresen, M. & Bjertness, E. Consumption of soft drinks and hyperactivity, mental distress, and conduct problems among adolescents in Oslo, Norway. Am. J. Public Health 96, 1815–1820 (2006).
Tahmassebi, J. F. & Banihani, A. J. Impact of soft drinks to health and economy: A critical review. Eur. Arch. Paediatr. Dent. 21, 109–117 (2020).
Zhou, Y. et al. Prevalence of overweight and obesity in Chinese children and adolescents from 2015. Ann. Hum. Biol. 44, 642–643 (2017).
Ma, Z. & Hao, Mo. Longitudinal study of the relationship between coffee consumption and type 2 diabetes in Chinese adult residents: Data from China Health and Nutrition Survey. Plos One 16, e0251377 (2021).
Deshpande, S., Singh, S., Panneerselvam, A. & Rajeswari, V. D. Nutrients in caffeinated beverages—an overview. In Caffeinated and Cocoa Based Beverages 367–389 (Elsevier, 2019).
Fredholm, B. B., Bättig, K., Holmén, J., Nehlig, A. & Zvartau, E. E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 51, 83–133 (1999).
McLellan, T. M., Caldwell, J. A. & Lieberman, H. R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 71, 294–312 (2016).
Hailemeskel, S., Demissie, A. & Assefa, N. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: Evidence from female university students in Ethiopia. Int. J. Womens Health 8, 489–496 (2016).
Ozerdogan, N. et al. Prevalence and predictors of dysmenorrhea among students at a university in Turkey. Int. J. Gynaecol. Obstet. 107, 39–43 (2009).
Habibi, N., Huang, M. S., Gan, W. Y., Zulida, R. & Safavi, S. M. Prevalence of primary dysmenorrhea and factors associated with its intensity among undergraduate students: a cross-sectional study. Pain Manag Nurs. 16, 855–861 (2015).
Unsal, A., Ayranci, U., Tozun, M., Arslan, G. & Calik, E. Prevalence of dysmenorrhea and its effect on quality of life among a group of female university students. Ups. J. Med. Sci. 115, 138–145 (2010).
Nyirenda, T. et al. Prevalence of dysmenorrhea and associated risk factors among university students in Zimbabwe. Womens Health 19, 17455057231189548 (2023).
Tan, K. C. B. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363, 157–163 (2004).
Lu, P. et al. Mental health of new undergraduate students before and after COVID-19 in China. Sci. Rep. 11, 18783 (2021).
Dutra, L. R. D. V. et al. Modulating anxiety and functional capacity with anodal tDCS over the left dorsolateral prefrontal cortex in primary dysmenorrhea. Int. J. Womens Health 12, 243–251 (2020).
Hashim, R. T. et al. Prevalence of primary dysmenorrhea and its effect on the quality of life amongst female medical students at King Saud University, Riyadh, Saudi Arabia. A cross-sectional study. Saudi Med. J. 41, 283–289 (2020).
Cakir, M., Mungan, I., Karakas, T., Girisken, I. & Okten, A. Menstrual pattern and common menstrual disorders among university students in Turkey. Pediatr. Int. 49, 938–942 (2007).
Ramadhan, R., Putra, W. K. Y., Utari, D. M. & Anwar, K. Sugary food and beverages consumption, family history, and primary dysmenorrhea in undergraduate students, Faculty of Public Health, Universitas Indonesia. Indones. J. Public Health Nutr. https://doi.org/10.7454/ijphn.v4i1.7388 (2023).
Fernández-Martínez, E., Onieva-Zafra, M. D. & Parra-Fernández, M. L. Lifestyle and prevalence of dysmenorrhea among Spanish female university students. PLoS One 13, e0201894 (2018).
Bhat, A., Aquil, H. & Zaheer, M. Efficacy of hijamat bila shurt (Dry cupping) on pain relief in primary dysmenorrhea. Innov. J. Med. Health Sci. 3, 71–75 (2013).
Muluneh, A. A., Nigussie, T. S., Gebreslasie, K. Z., Anteneh, K. T. & Kassa, Z. Y. Prevalence and associated factors of dysmenorrhea among secondary and preparatory school students in Debremarkos town, North-West Ethiopia. BMC Womens Health 18, 57 (2018).
Gagua, T., Tkeshelashvili, B. & Gagua, D. Primary dysmenorrhea: Prevalence in adolescent population of Tbilisi, Georgia and risk factors. J. Turk. Ger. Gynecol. Assoc. 13, 162–168 (2012).
Stratton, P. & Berkley, K. J. Chronic pelvic pain and endometriosis: Translational evidence of the relationship and implications. Hum. Reprod. Update 17, 327–346 (2011).
Aykut, M. et al. The impact of some biological, socio-demographic and nutritional factors on the prevalence of Dysmenorrhoea. Erciyes tıp dergisi = Erciyes Med. J. 29, 393 (2007).
Unsal, A., Tozun, M., Aslan, G., Ayranci, U. & Alkan, G. Evaluation of dysmenorrhea among women and its impact on quality of life in a region of western Turkey. Pak. J. Med. Sci. 26, 142–147 (2010).
Zhang, X. et al. Association of tea drinking and dysmenorrhoea among reproductive-age women in Shanghai, China (2013–2015): A cross-sectional study. BMJ Open 9, e026643 (2019).
Faramarzi, M. & Salmalian, H. Association of psychologic and nonpsychologic factors with primary dysmenorrhea. Iran. Red Crescent Med. J. https://doi.org/10.5812/ircmj.16307 (2014).
Alia, S., Shamssain, M. & Shahwan, M. Prevalence and impact of premenstrual syndrome in adolescent schoolgirls in the United Arab Emirates. Eur. J. Pharm. Med. Res. 3, 77–86 (2016).
Monday, I. et al. Prevalence and correlation between diet and Dysmenorrhea among high school and college students in Saint Vincent and Grenadines. Open Access Maced. J. Med. Sci. 7, 920–924 (2019).
Wrisnijati, D., Wiboworini, B. & Sugiarto, S. Prevalence and factor associated with severity of dysmenorrhea among female adolescent in Surakarta. J. Gizi Pangan Soedirman 3, 76–89 (2019).
Ribeiro, J. A. & Sebastiao, A. M. Caffeine and adenosine. J. Alzheimers Dis. 20(Suppl 1), S3–S15 (2010).
Åkerlund, M. Pathophysiology of dysmenorrhea. Acta Obstet. Gynecol. Scand. 58(sup87), 27–32 (1979).
Ninagawa, T., Matsukawa, R., Yoshio, T., Kan, S. & Ito, K. Prostaglandins and dysmenorrhea effect of naproxen on prostaglandin concentrations in menstrual blood (author’s transl). Acta Obstet. Gynaecol. Jpn. 33, 449–454 (1981).
Schreiner, C. M., Zimmerman, E. F., Wee, E. L. & Scott, W. J. Jr. Caffeine effects on cyclic AMP levels in the mouse embryonic limb and palate in vitro. Teratology 34, 21–27 (1986).
Oropeza-Rendon, R. L., Bauer, H. C. & Fischer, H. Effect of prostaglandin E1 on the level of cAMP in bone marrow macrophages. Inhibition of phagocytosis and cell shape changes. J Immunopharmacol. 2, 133–147 (1980).
Acknowledgements
The authors wish to thank all undergraduates who participated in the study for their collaboration in the study.
Funding
The study was supported by Taishan Scholar Program. PL was sponsored by Taishan Scholar Foundation (tsqn202211228), National Natural Science Foundation of China (42307549) Natural Science Foundation of Shandong Province (ZR202103050697) and Shandong Province Environmental Health Innovative Team. Guanghe Wang was supported by the Foundation of Shanghai Municipal Health Commission (202140204). Qiang Guo is supported by National Natural Science Foundation of China (62407040).
Author information
Authors and Affiliations
Contributions
L.W.: Methodology, Formal analysis, Software, Writing—original draft, Writing—review & editing. S.W.: Methodology, Formal analysis, Software, Resources, Writing—review & editing. X.L.: Methodology, Software, Formal analysis, Resources, Writing—review & editing. A.M.: Resources, Writing—review & editing. H.C.: Resources, Writing—review & editing. S.F.: Resources, Writing—review & editing. G.W.: Resources, Writing—review & editing. Q.G.: Supervision, Methodology, Resources, Writing—review & editing, Funding acquisition. P.L.: Conceptualization, Supervision, Methodology, Project administration, Resources, Writing—review & editing, Funding acquisition.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by Binzhou Medical University ethics committee (NO. 2019075). Written informed consent was obtained from all subjects.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, L., Wen, S., Li, X. et al. Associations between soft drinks intake and primary dysmenorrhea among Chinese undergraduate female students. Sci Rep 14, 21210 (2024). https://doi.org/10.1038/s41598-024-71802-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71802-8
