
Abstract
There is increasing awareness of radiotherapy’s potential side effects, such as lymphopenia. Therefore, this study aimed to establish the association between WBRT and the development of lymphopenia in patients with brain metastases undergoing brain radiotherapy (RT), along with evaluating the corresponding clinical outcomes. Including 116 patients with brain metastases undergoing brain radiotherapy, the study collected the absolute lymphocyte counts (ALC) within 2 weeks before brain radiotherapy (pre-radiotherapy, pre-RT), as well as ones at 1 and 2 months after completing RT (post-RT). Univariate and multivariate analyses were performed to identify associations between radiation modality and post-RT ALC. The relationships between post-RT ALC and overall survival were evaluated with Kaplan–Meier analysis and a multivariate Cox regression model. The median ALC definitely decreased at 1 month post-RT, but at 2 months post-RT, gradually rose but not to the pre-RT ALC. The multivariate analysis identified WBRT and lower pre-RT ALC as independent risk factors associated with the decrease in post-RT ALC at 1 month. It also revealed more than 4 brain metastases, G3-4 lymphopenia at 1 month and lower post-RT ALC at 2 months exhibited significantly worse prognosis regardless of the radiation modality. However, there was indeed an independent correlation between radiation modality and the outcome of intracranial progression-free survival (PFS). To approach the feasibility and reasonableness of treatment, clinicians should carefully consider various factors to achieve long-term survival of patients.
Similar content being viewed by others

Introduction
The overall survival of solid cancer has been significantly improved with the advancement of systemic treatments and the development of modern imaging technology, leading to an inevitable increase in the incidence of brain metastases. Brain metastases occur in approximately 20% of patients with extracranial tumors, primarily due to changes in microvascular anatomy that trap cancer emboli1. Depending on the location of intracranial mass lesions, metastatic encephalomata often present with various symptoms, including edema, hemorrhage, headache, projectile vomiting, and dysfunction in eloquent brain areas. Once brain metastases occur, the prognosis of these patients continues extremely poor.
In the era of immunotherapy, the regulation of immune function plays an increasingly crucial role in the treatment of solid cancers. Immunotherapy, with its unique mechanism compared to traditional chemotherapy, holds a promising prospect in various cancers, including melanoma and HER-2 positive breast cancer2,3. However, the central nervous system, historically regarded as an immune-privileged organ4, poses challenges for the effectiveness of immunotherapy in treating brain metastases.
Radiotherapy, as an effective and prompt treatment, exerts a profound impact on both primary and metastatic brain tumors, due to the promotion of immune system as well as the suppression of immunologic surveillance. Currently, local therapies, such as whole-brain radiotherapy (WBRT) and focal radiotherapy including stereotactic radiosurgery (SRS), are the primary treatments for patients with brain metastases5. However, WBRT and focal radiotherapy differ in radiation time, fractionated dose, and fractionations. Focal radiotherapy is primarily used for oligo-brain metastasis, allowing for hypofractionation and smaller radioactive dose, while WBRT is the standard treatment for patients with multiple brain metastases due to its effectiveness in palliation, widespread availability, and ease of delivery6,7. Both of radiation modalities can achieve local control and prevent the recurrence of brain metastases.
Lymphocytes in the circulating blood are of vital importance in mediating cellular immunity against tumor cells. They have also recently been identified as an essential biomarker for predicting the response to immunotherapy8. Unfortunately, lymphocytes are the most sensitive cells in the hematopoietic system when they come to radiation. Radiotherapy with a dose of 1–2 Gy can significantly reduce the number of lymphocytes9, and even a dose of 3 Gy can cause a 90% reduction10. The resulting lymphopenia induced by radiotherapy exacerbates the risk of disease progression and death, including opportunistic infections that can interrupt the radiotherapy regimen and reduce the anti-tumor immune response11. Multiple studies have shown a reduction in the ALC after radiation therapy in various extracranial and intracranial malignancies12,13,14,15.
However, the dynamic changes in ALC and the underlying mechanisms in WBRT have not been thoroughly elucidated. It is believed that the larger radiation field in WBRT exposes more circulating cells to incidental radiation doses within the treatment area, leading to lymphopenia16. Previous studies have demonstrated that lymphopenia is correlated with clinical features such as gross tumor volume and age17,18. Dosimetric parameters have also been used to investigate radiation-induced lymphopenia. Higher mean lung dose and longer treatment duration are significantly associated with lower post-SBRT ALC19. In glioma, whole-brain V20 is correlated with radiation-induced lymphopenia20. However, whether WBRT, which irradiates the entire brain tissue, is associated with radiation-induced lymphopenia in patients with brain metastases remains unknown. Despite increasing evidence regarding the impact of radiation-induced lymphopenia on poor survival in patients receiving extracranial radiotherapy13,18,21, the prognosis of brain metastases patients developing into radiation-induced lymphopenia through brain radiotherapy is still unclear.
This study aimed to investigate the influence of different radiation modalities on the changes in ALC among patients with brain metastases undergoing brain radiotherapy and evaluate its ultimate impact on survival.
Materials and methods
Patient selection
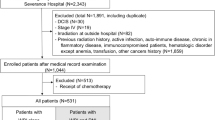
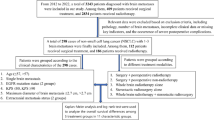
A total of 116 patients with brain metastases who received brain radiotherapy at our institution between September 1st 2019 to April 30th 2022 were included in this study. The inclusion criteria were as follows (1) biopsy-confirmed diagnosis of extracranial solid tumor (including lung, breast, colon cancer, etc.) at either the primary site or metastatic lesion; (2) diagnosis of brain metastasis confirmed by enhanced magnetic resonance imaging (MRI); (3) no history of brain radiotherapy; (4) available detailed individual information (clinical features and radiotherapy regimens); (5) expected survival time of more than 3 months. To evaluate expected lifespan of patients, detailed individual characteristics, including ages, ECOG scores, nutritional status, tumor type, clinical stage, time from the diagnosis of primary tumor to the occurrence of brain metastases, and the numbers of brain metastases, were took into consideration by two of the same oncologists with senior title.
Treatments
After evaluating brain metastases by enhanced MRI, the radiation modality, either WBRT with or without local boost or focal radiotherapy, was selected by clinicians based on individual difference. Available methods for brain radiotherapy included focal radiotherapy for limited metastases (≤ 4) and WBRT for multiple lesions (> 10). In most cases of metastatic brain tumors, the extracranial disease state and Eastern Cooperative Oncology Group (ECOG) score of patients with 4–10 metastatic lesions would influence the choice of radiation modality, except for small cell lung cancer (SCLC), for which WBRT was recommended regardless of the numbers of brain metastases. Radiotherapy was delivered by intensity-modulated radiotherapy (IMRT) technique. The gross tumor volume of metastasis (GTVm) was defined as specific lesion on T1 sequence of enhanced MRI, which was the referential safety margin by expanding 0.3 cm to generate planning target volume of metastasis (PTVm). Common organs at risk might include brainstem, hippocampus, bilateral lens of eyes, optical nerves and chiasma, if necessary. The standard prescription doses of WBRT were 25 Gy in 10 fractions, 30 Gy in 10 fractions, and 37.5 Gy in 15 fractions. In some cases, an additional radiation boost was delivered for WBRT at a dose of 10–20 Gy in 5–10 fractions. And the doses of focal radiotherapy for intracranial lesions ranged from 54–60 Gy in 15–18 fractions. Of note, clinicians determined when it was appropriate to administer concurrent therapies (including molecular targeted therapy (epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs), anaplastic lymphoma-tyrosine kinase inhibitors (ALK-TKIs) and etc.), and anti-vascular endothelial factor receptor (VEGFR) targeted therapy) or subsequent systemic therapies, including conventional cytotoxic chemotherapy with or without immunotherapy and support treatment, based on the tumor type and physical condition of the patient. As for steroid use, for patients with mild secondary intracranial hypertension and brain edema, the initial dose of dexamethasone is 5 mg/d for 3–5 days. For moderate to severe symptoms, an increased dose of dexamethasone, such as 10 mg/ day or more, is recommended. The application is continued until the symptoms are alleviated. However, the use of herbal medications was prohibited.
Assessment of lymphopenia
Peripheral venous blood samples were collected to measure ALC at three time points: within 2 weeks before the treatment (pre-RT), 1 month after completing brain radiotherapy (post-RT), and 2 months post-RT. The classic threshold for lymphopenia was defined as the absolute lymphocyte count < 1000 cells/µL. Lymphopenia was categorized according to Common Terminology Criteria for Adverse Events criteria (CTCAE) , version 5.0, as Grade 1 (800–1000 cells/µL) , Grade 2 (500–800 cells/µL), Grade 3 (200–500 cells/µL), and Grade 4 (< 200 cells/µL).
Statistical analysis
The statistical analysis was conducted using with the Statistical Package for Social Sciences, version 23.0 (IBM SPSS Statistics, Chicago, IL, USA). A significance level of p ≤ 0.05 was used to determine statistical significance. The clinical and treatment characteristics were summarized using descriptive statistics. Univariate and multivariate linear regression analyses were performed to identify variables associated with post-RT ALC. Covariates with p ≤ 0.05 in the univariate analysis were incorporated in the multivariate model. Overall survival (OS) was determined as the time from the start of brain radiotherapy to the date of death from any cause or the last follow-up visit. The Kaplan–Meier estimator with a log-rank test was used to calculate and compare OS based on different covariates. Multivariate Cox regression was used to assess the impact of clinical factors and radiation modality on OS and intracranial PFS.
Results
Patient characteristics
The study included 116 patients with brain metastases who met the criteria and had available laboratory values for review. The median age was 62 years (range, 19–80 years). 77 (66.4%) patients were over 60 years old. The median follow-up was 8.3 months (range, 2–29.3 months). Among the patients, 37 (31.9%) received WBRT with or without local boost, while 79 (68.1%) received focal radiotherapy. Detailed characteristics of all the patients can be found in Table 1.
Changes of ALC following brain radiotherapy
Figure 1 illustrated the changes in peripheral lymphocyte counts following brain radiotherapy. The median pre-RT ALC was 1100 cells/µL (range, 290–3500 cells/µL). At baseline, 53 patients (45.7%) had lymphopenia, and 8 patients (6.9%) had severe lymphopenia (G3-4 lymphopenia, ALC < 500 cells/µL). At 1 month post-RT, the median ALC of all patients was 830 cells/µL (range, 120–2970 cells/µL). Additionally, 77 (66.4%) patients developed into lymphopenia at this time point, with 24 (20.6%) patients developing into new lymphopenia, and the proportion of patients with G3-4 lymphopenia was 16.4%. At 2 months post-RT, available data on ALC for analysis was only in 77 patients due to death or out-of-hospital follow-up. The median ALC was 950 cells/µL (range, 190–3520 cells/µL). Among these patients, 48 (62.3%) patients evolved into lymphopenia, with 9 (11.6%) patients into new lymphopenia. 13 (16.9%) patients developed into G3-4 lymphopenia. Both the proportion of patients with G3-4 lymphopenia at 1 month and 2 months post-RT were higher compared to baseline (p = 0.016, p = 0.015, respectively) (Fig. 1A–C). The median decrease in ALC was 160 cells/µL at 1 month post-RT and 130 cells/µL at 2 months post-RT, respectively. The evaluation of whether chemotherapy induced lymphopenia showed no significant difference in the change of ALC at 1 month post-RT (p = 0.09) (Fig. 1D). However, it was worth noting that WBRT resulted in a significant decrease at 1 month post-RT in ALC while focal RT did not (p ≤ 0.01) (Fig. 1E).

Kinetics of ALC before brain radiotherapy (pre-RT) and at 1, 2 months after completing brain radiotherapy. (A) ALC at pre-RT, 1 and 2 months after brain radiotherapy. (B,C) Relative proportions of patients with lymphopenia classification. (D) Changes of ALC after brain radiotherapy at 1 month between chemotherapy group and non-chemotherapy group. (E) ALC of both radiation modalities at pre-RT and post-RT. pre-RT, before brain radiotherapy; post-RT, after completing RT; ns, p ≥ 0.05; **, p ≤ 0.01; ***, p ≤ 0.001.
Association of post-RT ALC with clinical factors
Initially, there was no significant difference in pre-RT ALC based on sex, age, history of extracranial radiotherapy, or primary tumor site (all p > 0.05). In the univariate analysis, it was found that lower pre-RT ALC, WBRT, more than 4 brain metastases, and a history of previous extracranial radiotherapy were significantly associated with lower post-RT ALC at 1 month. After performing stepwise multivariate linear regression, which incorporated all significant parameters from the univariate analysis, it showed that lower pre-RT ALC (p < 0.001) and WBRT (p = 0.006) were independent risk factors for the decrease in ALC at 1-month post-RT. At 2 months post-RT, the univariate analysis revealed that lower post-RT ALC was significantly associated with WBRT, history of extracranial radiotherapy and lower pre-RT ALC. The numbers of brain metastases, however, did not show a significant association. In the multivariate analysis, only pre-RT ALC (p < 0.001) was the independent risk factor for ALC at 2 months post-RT. Notably, the effects of chemotherapy and steroid use during RT did not show statistical significance of ALC at 1 and 2 months post-RT. The results of univariate and multivariate linear regression analyses between clinical factors and post-RT ALC were shown in Table 2.
Prognostic value of post-RT ALC
Survival analysis was conducted to assess the prognostic value of post-RT ALC for clinical outcome. Among the patients included in the study, 69 were alive at the end of the follow-up period. The median OS was 14.5 months, with a 1-year OS rate of 56.2% and a 2-year OS rate of 35.5%. As shown in Fig. 2A,B, there was no significant difference in survival between patients with ALC ≥ 1000 cells/µL and ALC < 1000 cells/µL (G1-4 lymphopenia) at either 1 month or 2 months after completing brain radiotherapy (p = 0.1 and p = 0.4, respectively). However, when comparing patients with ALC ≥ 500 cells/µL and ones with ALC < 500 cells/µL, obvious differences in OS were observed at both 1 month and 2 months post-RT (p = 0.006 and p = 0.001, respectively) (Fig. 2C,D). Univariate analysis of clinical factors revealed that having more than 4 brain metastases (HR: 0.29; p < 0.001), pre-RT ALC (HR: 0.397; p = 0.009), ALC at 1-month and 2-month post-RT (HR: 0.417; p = 0.026; HR: 0.342; p = 0.031, respectively), and G3-4 lymphopenia at 1 month post-RT (HR: 0.408, p = 0.008) were associated with OS. In the multivariate analysis, after controlling for confounding variables including radiation modality, it was found that having more than 4 brain metastases (HR: 0.216; p < 0.001), G3-4 lymphopenia at 1-month post-RT (HR: 0.187; p = 0.008) and ALC at 2-month post-RT (HR: 0.049; p < 0.001) were significantly associated with shorter OS (Table 3). Additionally, Table 4 demonstrated that WBRT was an independent and significant predictor for intracranial PFS (p = 0.034).

Kaplan‒Meier curves showing OS in patients stratified by different degrees of radiation-induced lymphopenia. (A,B) Patients with ALC ≥ 1000cells/µL had longer OS compared to those with ALC < 1000 cells/µL at 1 month and 2 months post-RT. (C,D) Patients with ALC ≥ 500 cells/µL had longer OS than patients with ALC < 500 cells/µL at 1 month and 2 months post-RT.
Discussion
In this study of patients with brain metastases receiving RT, we observed a significant decrease in ALC at 1 month after RT, followed by a gradual rebound at 2 months post-RT, but not reaching the pre-RT levels. Furthermore, WBRT and lower pre-RT ALC were significantly correlated with decreased post-RT ALC at 1 month post-RT. However, only pre-RT ALC remained as an independent risk factor at 2 months post-RT. Moreover, this study confirmed that Grade 3–4 lymphopenia at 1 month post-RT and ALC at 2 months post-RT were independently associated with worse survival outcomes in a multivariate Cox model, while WBRT was independently associated with intracranial PFS.
Lymphocytes in the bone marrow may remain stationary during each fraction of RT, but they can move between fractions22. Despite the fact that the proliferating bone marrow in the skull accounts for only 6% of the total body marrow23 and there is minimal lymphoid tissue in the brain and skull, there was a significant decrease in ALC at 1 and 2 months post-RT. And the actual amount of actively proliferating bone marrow within radioactive field predicted treatment-related lymphopenia23. Perhaps the exposure of circulating lymphocytes to radiation should be considered as a significant factor of inducing lymphopenia24. These indicated that WBRT is more likely to induce lymphopenia compared to focal radiotherapy in the treatment of brain metastases. Previous studies have confirmed that WBRT leads to a significant morbidity in terms of neurocognitive dysfunction and reduces quality of life1. And the influence on cognitive function of hippocampus sparing was inferior to conventional WBRT, which might need memantine to relieve its side effect1. However, WBRT-related lymphopenia had rarely been reported. Potential mechanisms may involve the following aspects. WBRT has larger radiation field than focal radiotherapy and brain tissue has rich blood flow, which contribute to the exposure and depletion of peripheral lymphocytes within radiation field. In contrast, focal radiotherapy specifically targets localized intracranial lesions. Due to variations in techniques and beam arrangements, different levels of low and moderate radiation doses may be delivered to the vasculature outside the radiation field of the brain, which also contributes to the exposure of circulating lymphocytes to radiation25. Furthermore, previous studies have demonstrated that dosimetric parameters, including gross tumor volume, lung V5, heart V5, integral body dose, and mean spleen dose, etc.11,12,15, are associated with radiation-induced lymphopenia in extracranial radiotherapy26. Thus, it is imperative to further investigate the relationships between dosimetric parameters and the decrease in ALC after brain radiotherapy in future studies. Presently, WBRT is regarded as the standard treatment for patients with more than 10 brain metastases. However, there is some controversy regarding the use of WBRT for 4–10 brain metastases27. Therefore, considering its effects on PFS and lymphopenia, a comprehensive evaluation should be conducted when deciding whether to use WBRT for controlling brain metastases.
The dynamics of lymphocytes after extracranial radiotherapy had been extensively investigated. In one aspect, the white blood cell and platelet counts increased following a decline during RT, while ALC continuously decreased28. In another aspect, ALC gradually normalized over a period of 2 months after completing concurrent chemoradiotherapy in locally advanced pancreatic cancer29. According to Cho et al., the majority of patients experienced recovery from treatment-related lymphopenia in 3 month after radiotherapy30. Pike et al. found that lymphopenia after radiotherapy lasted for at least 6 months in cases of metastatic cancer31. It might take 1 year for the complete white cell series to reach a recovery plateau, while lymphocytes might require 6 years24. Further analysis revealed that the duration of radiation, age, and baseline ALC were associated with the recovery of lymphopenia32. Our study suggested that only pre-RT ALC was associated with ALC at 2 months post-RT, indicating the recovery process of lymphocytes uncorrelated to clinical factors but to the baseline of ALC before RT. However, further confirmation is required by expanding the sample size. Regarding symptomatic metastases and the mitigation of brain edema, steroid use often lasted for several days. Dexamethasone was lymphotoxic25 and increased the incidence of lymphopenia11. However, our study demonstrated that steroid use during radiotherapy was not associated with ALC post-RT when considering other clinical factors, which was consistent with prior data33. The main reason for the diverse results may be the short duration and low dosage. Moreover, numerous studies had demonstrated the effects of systemic therapy on the lymphocyte counts, including chemotherapy-induced decline in circulating lymphocytes, in addition to the evident inhibition of neutrophils. Sanchez-Pere et al. found that fist-line chemotherapy for glioblastoma often resulted in lymphopenia34. Chen et al. showed that patients with breast cancer might experience lymphopenia as a result of previous chemotherapy35. It is well known that myelosuppression is the most common adverse reaction of chemotherapy, leading to a decrease in white blood cells and neutrophils, which, to some extent, affects lymphocyte count. However, chemotherapy did not impact lymphocyte counts at 1 month in our study, possibly due to the small number of patients receiving chemotherapy (24 in WBRT and 29 in focal RT, respectively) and the poor ECOG scores of patients undergoing WBRT. With the prolonged duration of chemotherapy and the associated increase in concomitant drug toxicity, outcomes may vary significantly over a period of 2 months or longer. Subsequent studies with larger sample sizes are necessary to provide further validation of these findings. Therefore, when selecting chemotherapy regimens, oncologists should likewise be as considerate as possible in order to improve patients’ tolerance, particularly when combined with brain radiotherapy. Furthermore, targeted therapy and immunotherapy are less likely to impact lymphocyte counts. The reasons for the discrepancy between our research and previous studies may be attributed to the relatively small sample size and other factors.
Prognostic factors in patients with brain metastases had been gradually identified. Performance status and evidence of systemic disease might be the strongest factors for prognosis36. Graded Prognostic Assessment was an important prognostic factor for lung cancer patients with brain metastases37. Currently, the relationship between ALC and clinical outcomes has been widely studied. Lymphopenia after treatment was associated with decreased survival in patients with limited-stage small cell lung cancer38. Shiraishi et al. reported lymphopenia in 480 patients receiving neoadjuvant chemoradiotherapy and found that Grade 4 ALC was significantly associated with reduced distant metastasis-free survival39. Our results showed that patients with G3-4 (lymphocyte count < 500 cells/µL) lymphopenia had worse survival compared with G0-2 lymphopenia at 1 month and 2 months post-RT, respectively. In the multivariate Cox model, including confounders such as the history of extracranial radiotherapy, radiotherapy modality, chemotherapy and steroid use, poor OS were related not only to G3-4 lymphopenia at 1 month post-RT but also to a lower ALC at 2 months post-RT. To the best of our knowledge, this is the first study to demonstrate an association between radiation-induced lymphopenia and prognosis in patients with brain metastases receiving radiotherapy. Previous reports had shown that radiation-induced lymphopenia affected the effectiveness of immunotherapy. Studies had demonstrated that lower lymphocyte counts could indicate diminished performance status and worse systemic immunity40,41. Additionally, it had been observed that immune cells homed to cancer and changed its microenvironment through calreticulin and high-mobility group box 1 (HMGB 1)11. Finally, a worse effect of comprehensive treatment resulted in shorter intracranial PFS and poor OS. However, neither radiation modality nor the numbers of brain metastases showed a prominent relation with survival in either univariate or multivariate analysis. However, WBRT was associated with intracranial PFS (i. e. short-term efficacy). This might be attributed to the fact that most of the enrolled patients had received multi-line systemic treatments. Broadly speaking, the final survival of patients mainly depends on the efficacy of comprehensive treatments, tumor characteristics and patients’ condition. Reserving lymphocytes could potentially boost the response to systemic therapy42. For instance, keeping low dose of organs at risk could reduce the incidence of lymphopenia22. Clinicians should strive to strike a balance between better cancer control and the risk of lymphopenia. By avoiding or alleviating adverse effects as much as possible, therapeutic effectiveness can be enhanced and survival can be extended.
This study had some limitations. First, it was a retrospective study conducted at a single center with a limited number of cases, so selection bias was inevitable. Second, there was a need for further analysis of the dosimetric parameters related to radiation-induced lymphopenia. Third, for cases of limited brain metastases, focal radiotherapy was performed in our institution, but the prescribed doses of radiation and the number of fractionations varied considerably from individual to individual, which might yield different results if replaced with standard radiation regimens. Therefore, further validation is required in the future studies.
Conclusion
We demonstrated that the reasonable selection of radiation modality can indirectly impact clinical outcomes by attenuating lymphopenia in patients undergoing brain radiotherapy. This finding suggests that in the era of precise treatments, taking into account individual differences, prognostic stratification is important for guiding clinicians in offering prudent and appropriate treatments to patients with risk factors, particularly those with 4–10 metastases of brain. Needless to say, completing radiotherapy of metastatic lesion without severe toxicities and complications, marks a profound impact on comprehensive therapy of solid tumors. Clinicians still have a long way to go to reach the final goal, but achieving some milestones remains well within the realm of possibility.
Data availability
The original data presented in the study are included in the article. Further inquiries can be directed to the corresponding authors. All methods were carried out in accordance with relevant guidelines and regulations.
Abbreviations
- RT:
-
Radiotherapy
- ALC:
-
Absolute lymphocyte counts
- Pre-RT:
-
Before brain radiotherapy
- Post-RT:
-
After completing RT
- ECOG:
-
Eastern Cooperative Oncology Group
- WBRT:
-
Whole-brain radiotherapy
- PFS:
-
Progression-free survival
- SRS:
-
Stereotactic radiosurgery
- GTVm:
-
Gross tumor volume of metastasis
- PTVm:
-
Planning target volume of metastasis
- CTCAE:
-
Common terminology criteria for adverse events criteria
- OS:
-
Overall survival
References
Brenner, A. W. & Patel, A. J. Review of current principles of the diagnosis and management of brain metastases. Front. Oncol. 12, 857622 (2022).
Liu, L. et al. Radiotherapy in combination with systemic therapies for brain metastases: Current status and progress. Cancer Biol. Med. 17(4), 910–922 (2020).
Schlam, I. & Gatti-Mays, M. E. Immune checkpoint inhibitors in the treatment of breast cancer brain metastases. Oncologist 27(7), 538–547 (2022).
Nguyen, T. T. et al. Reshaping the tumor microenvironment with oncolytic viruses, positive regulation of the immune synapse, and blockade of the immunosuppressive oncometabolic circuitry. J. Immunother. Cancer 10(7) (2022).
Soffietti, R. et al. Diagnosis and treatment of brain metastases from solid tumors: Guidelines from the European Association of Neuro-Oncology (EANO). Neuro-oncology 19(2), 162–174 (2017).
Tonse, R., Tom, M. C., Mehta, M. P., Ahluwalia, M. S. & Kotecha, R. Integration of systemic therapy and stereotactic radiosurgery for brain metastases. Cancers 13(15), 3682 (2021).
Singh, R. et al. Repeat stereotactic radiosurgery for locally recurrent brain metastases previously treated with stereotactic radiosurgery: A systematic review and meta-analysis of efficacy and safety. J. Radiosurgery SBRT 8(1), 1–10 (2022).
Cho, Y. et al. Impact of treatment-related lymphopenia on immunotherapy for advanced non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 105(5), 1065–1073 (2019).
Nakamura, N., Kusunoki, Y. & Akiyama, M. Radiosensitivity of CD4 or CD8 positive human T-lymphocytes by an in vitro colony formation assay. Radiat. Res. 123(2), 224–227 (1990).
Joseph, N. et al. Post-treatment lymphocytopaenia, integral body dose and overall survival in lung cancer patients treated with radical radiotherapy. Radiother. Oncol. 135, 115–119 (2019).
Upadhyay, R. et al. Risk and impact of radiation related lymphopenia in lung cancer: A systematic review and meta-analysis. Radiother. Oncol. 157, 225–233 (2021).
Tang, C. et al. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 89(5), 1084–1091 (2014).
Rudra, S. et al. Effect of radiation treatment volume reduction on lymphopenia in patients receiving chemoradiotherapy for glioblastoma. Int. J. Radiat. Oncol. Biol. Phys. 101(1), 217–225 (2018).
Kroese, T. E. et al. Severe lymphopenia acquired during chemoradiotherapy for esophageal cancer: Incidence and external validation of a prediction model. Radiother. Oncol. 163, 192–198 (2021).
Liu, J. et al. Radiation-related lymphopenia is associated with spleen irradiation dose during radiotherapy in patients with hepatocellular carcinoma. Radiat. Oncol. 12(1), 90 (2017).
Xie, X. et al. Radiation-induced lymphopenia correlates with survival in nasopharyngeal carcinoma: Impact of treatment modality and the baseline lymphocyte count. Radiat. Oncol. 15(1), 65 (2020).
Xie, X. et al. Radiation-induced lymphopenia during chemoradiation therapy for non-small cell lung cancer is linked with age, lung V5, and XRCC1 rs25487 genotypes in lymphocytes. Radiother. Oncol. 154, 187–193 (2021).
Taguchi, A. et al. Postradiotherapy persistent lymphopenia as a poor prognostic factor in patients with cervical cancer receiving radiotherapy: A single-center, retrospective study. Int. J. Clin. Oncol. 25(5), 955–962 (2020).
Zhao, Q., Li, T., Chen, G., Zeng, Z. & He, J. Prognosis and risk factors of radiation-induced lymphopenia in early-stage lung cancer treated with stereotactic body radiation therapy. Front. Oncol. 9, 1488 (2019).
Byun, H. K. et al. Clinical predictors of radiation-induced lymphopenia in patients receiving chemoradiation for glioblastoma: Clinical usefulness of intensity-modulated radiotherapy in the immuno-oncology era. Radiat. Oncol. 14(1), 51 (2019).
Yu, H. et al. Potential determinants for radiation-induced lymphopenia in patients with breast cancer using interpretable machine learning approach. Front. Immunol. 13, 768811 (2022).
Abravan, A., Faivre-Finn, C., Kennedy, J., McWilliam, A. & van Herk, M. Radiotherapy-related lymphopenia affects overall survival in patients with lung cancer. J. Thorac. Oncol. 15(10), 1624–1635 (2020).
Park, S., Byun, H. K. & Seong, J. Irradiation-related lymphopenia for bone metastasis from hepatocellular carcinoma. Liver Cancer 8(6), 468–479 (2019).
Harisiadis, L., Kopelson, G. & Chang, C. H. Lymphopenia caused by cranial irradiation in children receiving craniospinal radiotherapy. Cancer 40(3), 1102–1108 (1977).
Huang, J. et al. Clinical and dosimetric predictors of acute severe lymphopenia during radiation therapy and concurrent temozolomide for high-grade glioma. Int. J. Radiat. Oncol. Biol. Phys. 92(5), 1000–1007 (2015).
Chen, F. et al. Radiation induced lymphopenia is associated with the effective dose to the circulating immune cells in breast cancer. Front. Oncol. 12, 768956 (2022).
Loo, M., Clavier, J. B., Attal Khalifa, J., Moyal, E. & Khalifa, J. Dose-response effect and dose-toxicity in stereotactic radiotherapy for brain metastases: A review. Cancers 13(23), 6086 (2021).
Yang, T. J. et al. Clinical and dosimetric predictors of acute hematologic toxicity in rectal cancer patients undergoing chemoradiotherapy. Radiother. Oncol. 113(1), 29–34 (2014).
Lee, B. M., Byun, H. K. & Seong, J. Significance of lymphocyte recovery from treatment-related lymphopenia in locally advanced pancreatic cancer. Radiother. Oncol. 151, 82–87 (2020).
Cho, Y. et al. Lymphocyte dynamics during and after chemo-radiation correlate to dose and outcome in stage III NSCLC patients undergoing maintenance immunotherapy. Radiother. Oncol. 168, 1–7 (2022).
Pike, L. R. G. et al. The impact of radiation therapy on lymphocyte count and survival in metastatic cancer patients receiving PD-1 immune checkpoint inhibitors. Int. J. Radiat. Oncol. Biol. Phys. 103(1), 142–151 (2019).
Zhao, Q., Li, T., Du, S., He, J. & Zeng, Z. Shortened radiation time promotes recovery from radiation-induced lymphopenia in early-stage non-small cell lung cancer patients treated with stereotactic body radiation therapy. Technol. Cancer Res. Treat. 21, 15330338221112288 (2022).
Grossman, S. A. et al. Immunosuppression in patients with high-grade gliomas treated with radiation and temozolomide. Clin. Cancer Res. 17(16), 5473–5480 (2011).
Sanchez-Perez, L., Suryadevara, C. M., Choi, B. D., Reap, E. A. & Sampson, J. H. Leveraging chemotherapy-induced lymphopenia to potentiate cancer immunotherapy. Oncoimmunology 3(7), e944054 (2014).
Chen, F. et al. Chemotherapy is a risk factor of lymphopenia before adjuvant radiotherapy in breast cancer. Cancer Rep. 5(7), e1525 (2022).
Lagerwaard, F. J. et al. Identification of prognostic factors in patients with brain metastases: A review of 1292 patients. Int. J. Radiat. Oncol. Biol. Phys. 43(4), 795–803 (1999).
Gaspar, L. et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 37(4), 745–751 (1997).
Wang, X., Lu, J., Teng, F. & Yu, J. Lymphopenia association with accelerated hyperfractionation and its effects on limited-stage small cell lung cancer patients’ clinical outcomes. Ann. Transl. Med. 7(16), 385 (2019).
Wang, X. et al. A review of radiation-induced lymphopenia in patients with esophageal cancer: An immunological perspective for radiotherapy. Ther. Adv. Med. Oncol. 12, 1758835920926822 (2020).
Raghu, D., Xue, H. H. & Mielke, L. A. Control of lymphocyte fate, infection, and tumor immunity by TCF-1. Trends Immunol. 40(12), 1149–1162 (2019).
Uzhachenko, R. V. & Shanker, A. CD8+ T lymphocyte and NK cell network: Circuitry in the cytotoxic domain of immunity. Front. Immunol. 2019, 10 (1906).
Chen, D. et al. Interaction between lymphopenia, radiotherapy technique, dosimetry, and survival outcomes in lung cancer patients receiving combined immunotherapy and radiotherapy. Radiother. Oncol. 150, 114–120 (2020).
Acknowledgements
The study was supported by Chongqing Medical Scientific Research Project (No. 2020FYYX143) and the Natural Science Foundation of Chongqing, China (No. CSTB2023NSCQ-MSX020).
Author information
Authors and Affiliations
Contributions
Y Wang, WW Zeng collected data and wrote the manuscript. WY Xie and W Zhao designed the project and implemented the research. GP Yang collected and analysed data. YH Chen were responsible for patient follow-up. All authors contributed to the article and approved the submitted version. Y Wang and WW Zeng contributed equally to the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the ethics committee of the second affiliated hospital of Chongqing medical university. The written informed consent was obtained from all the patients. All methods were carried out in accordance with relevant guidelines and regulations.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Y., Zeng, W., Xie, W. et al. Lymphopenia associated with whole-brain radiotherapy and its effects on clinical outcomes of patients with brain metastases. Sci Rep 14, 21315 (2024). https://doi.org/10.1038/s41598-024-71943-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71943-w
