
Abstract
This study was aimed to compare the clinical and radiographic outcomes of patients with intercondylar fractures of the humerus treated with orthogonal and parallel plating methods via precontoured plates. This was a retrospective comparative study conducted on 50 adult patients with intercondylar humerus fractures that were surgically treated over an eleven-year period. The patients were divided into two groups: Group A underwent internal fixation via parallel plating, whereas Group B received orthogonal plating. Clinical outcomes were evaluated via the Mayo Elbow Performance Score (MEPS), and the radiographic assessments included time to consolidation, pseudoarthrosis, malunion and hardware removal. Both groups presented similar demographic and preoperative characteristics. The functional outcomes assessed by the MEPS were not significantly different between the groups. Radiographically, comparable healing times and rates of complications, including pseudoarthrosis, malunion and hardware removal, were observed. The study findings suggest that both orthogonal and parallel plating methods yield comparable clinical and radiographic outcomes in the treatment of intercondylar humerus fractures. These results underscore the effectiveness of both techniques and emphasize the importance of further research to elucidate the optimal plating method for specific fracture patterns.
Similar content being viewed by others


Introduction
Intercondylar fractures of the humerus are defined as fractures located between the distal insertion of the anterior brachialis muscle and the elbow joint space and are classified as fractures of the lower end of the humerus1. Because of the comminution and/or porotic state of the bone, these fractures can be complex.
Intercondylar fractures are the most common type of fracture of the distal humerus in adults, accounting for 1 to 2% of elbow fractures2.
The success of surgery, which is widely considered difficult, requires an understanding of the fracture types, mastery of the approach and good intraoperative assessment of the quality of synthesis to guide rehabilitation3.
The primary goal of surgery is to achieve stable and accurate bone and articular reconstruction that permits early range of motion (ROM) activities. Previous biomechanical studies on internal fixation methods for distal humerus fractures have indicated that double-plate fixation provides adequate stability4.
The standard method used by most surgeons is the application of 2 perpendicular plates, one on the medial supracondylar ridge and the other placed posterolaterally3. However, a parallel plating method, whereby plates are placed along each supracondylar ridge at approximately 180° to each other, also provides stable internal fixation. The optimal position of the plating remains controversial.
The purpose of the present study was to compare the clinical and radiographic outcomes of patients with intercondylar humerus fractures treated with orthogonal and parallel plating methods via precontoured plates for distal humerus fractures.
Materials and methods
Study design
This is a retrospective comparative study of two series of intercondylar humerus fractures surgically treated over a period of eleven years from 2010 to 2020 in our orthopedics and traumatology department at Kassab Hospital in Tunis via two different methods.
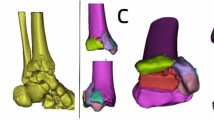
For our inclusion criteria, we used the AO/OTA classification of distal humerus fractures5. (Fig. 1) All adult patients treated surgically for type C fractures of the distal humerus via open reduction and internal fixation (ORIF) with perpendicular or parallel plates were included.

AO/OTA classification of distal humerus fractures.5.
The minimum follow-up recommended was 18 months. The exclusion criteria were patients younger than 18 years, patients who had an extra-articular or pathological fractures, other fixation procedures, incomplete records or a follow-up period of less than 18 months.
In total, 50 patients met our criteria; these participants were divided into two groups:
Group A: Internal fixation via the parallel plating method (29 patients). (Fig. 2)
Group B: Internal fixation via the orthogonal plating method (21 patients). (Fig. 3)

A 47-year-old female patient with a distal humerus fracture.
The patient underwent surgery with the parallel plating method.
-
a.
Anteroposterior and lateral initial plain radiographs.
-
b.
Anteroposterior and lateral postoperative plain radiographs taken 2 weeks postoperatively.

A 31-year-old male patient with a distal humerus fracture.
The patient underwent an operation via the orthogonal plating method.
-
a.
Anteroposterior and lateral initial plain radiographs.
-
b.
Anteroposterior and lateral postoperative plain radiographs at 2 weeks.
postoperatively.
Patients
A total of 50 patients (19 women and 31 men) with a mean age of 44.4 ± 11.5 years (range: 21–70 years) were included in this study.
All 50 patients were followed for a minimum of 18 months (range: 2.0–3.7 years).
Demographic information from both groups is presented in Table 1.
Five patients had open fractures: 4 were grade I, and one was grade II, according to the criteria defined by Gustilo and Anderson6.
For open fractures, debridement, irrigation, and plate fixation were performed on the date of admission. All other patients were stabilized within 4 days of injury.
Two patients had additional fractures of the forearm bones, two others had additional olecranon fractures, and one patient had an ipsilateral tibia shaft fracture.
One patient had neurologic symptoms.
Surgical technique
All patients were placed in the supine position on the operating table, with the arm supported on the arm board table. A tourniquet was applied as far proximally as possible.
Chevron olecranon osteotomy was performed for all patients.
In the orthogonal group, the fracture was exposed, and Kirschner wires (K-wires) were employed for temporary fixation of the reduction. After initial stabilization, 1 or 2 lag screws were used to stabilize the lower portion of the distal humerus. The extraarticular fracture component was subsequently reduced and stabilized with either K-wires or reduction forceps. The two plates were then strategically positioned in posterolateral and medial orientations in an orthogonal manner. The surgeon prioritized initially performing plate fixation on the column to increase the ease of anatomical reconstruction and mitigate the risk of significant bone loss.
In the parallel plating group, we initially achieved temporary fixation via K-wires positioned near the subchondral level to prevent interference with screw passage from the plates to the distal fragments. However, in instances of significant comminution in the distal fragment, fixation was accomplished via a 2.7- or 3.5-mm interfragmentary screw. Two precontoured plates were subsequently positioned along the medial and lateral supracondylar ridges, approximately 180 degrees apart. Once the plates were preliminarily applied, distal introduction of medial or lateral screws became necessary, which necessitated additional distal fragments to ensure stable fixation of the intraarticular fragments and secure anchoring of the plates. The screws for distal fragments traversed the plate, thereby contributing to stability at the supracondylar level and engaging as many articular fragments as possible.
In both groups, an olecranon osteotomy site was fixed by placement of a tension-band wire.
Functional and clinical evaluation
At the final follow-up, our patients were assessed for functional impairment via the Mayo Elbow Performance Scale (MEPS)7.
This scoring system consisted of the assessment of pain, arc of motion, and stability and a patient rating of daily function, as shown in Fig. 4.
A MEPS of 75 or more is considered satisfactory.

Clinical scores within each group.
Radiological evaluation
All patients were monitored by frontal and lateral radiographs of the elbow.
The radiological evaluation criteria were as follows:
● Time to consolidation: the disappearance of the line in the medial and lateral abutment.
● Pseudarthrosis: the persistence of the fracture line between one or more bone fragments six months after surgery8.
● Malunion: divided into articular and extra-articular malunion.
● Hardware removal.
Ethics approval
This was an observational study. The Ethics Committee of Kassab Hospital confirmed that no ethical approval was needed.
Results
Descriptive results
A total of 50 patients were enrolled in our study. The average patient age was 44.4 years (ranging from 21 to 70 years). Men were more affected than women were, with a sex ratio of 2/1 (31 males and 19 females).
Domestic accidents were the most common etiology, accounting for more than 64% of the cases. Direct trauma was the main mechanism (82%).
The mean time to surgical management was 20.9 ± 24.5 h. Postoperatively, all the patients were immobilized in an elbow splint for an average of 2.4 weeks (ranging from 2 to 4 weeks). The start of rehabilitation varied depending on the stability of the fracture fixation (ranging from one to 21 days).
Group A included 29 patients. The average age was 43.7 years (ranging from 21 to 65 years), with a male predominance (65.5%). Compound fractures were present in 10.34% of the cases. The fractures were AO/OTA Type C2 in 34.5% of the cases. ULN injury was noted in 3.44% of the patients.
Group B included 21 patients. The average age of the participants was 45.3 years (ranging from 24 to 76 years), with a male predominance (57.14%). Compound fractures were present in 9.52% of the cases. The fractures were AO/OTA Type C2 in 52.4% of the cases.
Neither of the two groups required bone grafting. The two groups were comparable in terms of epidemiology and preoperative data (Table 1).
Complications
There was no significant difference in terms of complications between the two groups, as shown in Table 2.
Functional and clinical results
For Group A, the mean follow-up time was 62 months (ranging from 40 to 95 months).
For Group B, the average follow-up time was 68 months (ranging from 45 to 117 months).
42% of Group A and 32% of Group B patients had an MEPS ≥ 75 (Fig. 4). There was no statistically significant difference in the MEPS between the two groups (P = 0.67).
Radiological results
There was no difference in the radiological results between the two groups (Table 3).
Discussion
The primary finding of this study is that both surgical techniques (osteosynthesis via perpendicular plates versus parallel plates) resulted in comparable Mayo Clinic scores. However, there are notable limitations. First, the retrospective design introduced potential biases in patient selection and data collection, as the treatment methods were not assigned randomly. Second, the relatively small sample size of 50 patients, divided between the two groups, may have limited the statistical power to identify minor differences in outcomes between the orthogonal and parallel plating methods.
Fixation of comminuted distal intra-articular humeral fractures via double plates has been considered by several authors to be more stable than the use of a single plate9,10,11.
In the literature, the results comparing the two operative techniques have been divergent.
Our results were similar to those of the studies by Proust et al. and Tian et al., who concluded that when comparing the different placements of the two plates (orthogonal and parallel), there was no significant difference according to the Mayo Clinic score (Mayo Clinic score = 74 versus 77, respectively)4,12,13.
Schwartz et al. tested perpendicular and parallel plate fixation in compression, torsion and flexion in varus and valgus and reported no significant difference in stability between the two systems11.
Similarly, Atalar et al. reported that the two fixation systems had similar biomechanical stabilities when anatomical plates with distal locking screws were used14. Indeed, the stiffness values in all directions did not significantly differ between the orthogonal and parallel groups. There was no significant difference between the two groups regarding plastic deformation values (0.31 vs. 0.29 mm) or posterior bending failure load tests (372.4 vs. 379.7 N). In the perpendicular fixation system, most failures were caused by fracture of the proximal stem, whereas in the parallel fixation system, failure resulted from displacement of the most distal screw in the proximal fragment14.
Sang et al. reported no significant differences between perpendicular and parallel fixation methods in terms of clinical outcomes and complication rates. However, the perpendicular fixation method might be preferred in cases of coronal shear fractures (where posterior‒anterior fixation can provide additional stability to intra-articular fractures), whereas the parallel fixation method might be the preferred technique for fractures that occur at the more distal end of the humerus, as greater stability can be achieved by providing additional screws in the distal fragments8.
In another study, the parallel plate group presented significantly greater values in stiffness and cyclic load tests under axial loading, whereas the perpendicular plate group presented higher stiffness values under posterior bending loading in composite humerus models15. The greatest displacement under an axial load of 300 N was observed for perpendicular plating. However, under posterior bending loading, the parallel veneer presented the largest displacement values. The authors of that study reported that both fixation systems could be used for distal humerus fractures but that the parallel fixation system was superior in axial loading15. This superiority could be explained by the difference in the number of transchondylar screws in each group. The parallel fixation system involves transchyle screws, whereas the orthogonal fixation system involves a single screw.
Several other studies have suggested that supra- and intercondylar fractures of the humerus would be better stabilized via parallel plates than via traditional perpendicular fixation techniques, as the implants would interdigitate with the distal fragments (extending into the fragment adjacent to the opposing plate) and form the equivalent of a compression arch10,11,12.
Stoffel et al.12 compared the biomechanical stability of perpendicular and parallel locking plate systems for internal fixation of AO C2 distal humerus fractures in osteoporotic bone. They reported that both locking plate systems enabled early elbow mobilization in osteoporotic patients after fixation of a comminuted distal humerus fracture. However, the parallel locking system showed better stability than the perpendicular locking system. Indeed, the parallel plate system offered significantly greater stability during compression (p = 0.005) and external rotation (p = 0.006), as well as a greater ability (p = 0.005) to resist axial plastic deformation. The stability of both constructs appeared to depend on the bone quality; however, the stability of the perpendicular system was generally more sensitive to bone mineral density, indicating the possible need for additional independent interfragmentary screws. However, wear debris produced by the taping system is a disadvantage of the parallel locking plate system. Furthermore, one of the negative aspects of this study was the difference in material properties. The parallel plates were made of titanium alloy, and the orthogonal plates were made of stainless steel. Varus/valgus and flexion/extension loads were not evaluated in this study.
Similarly, Schemitsch et al.4 compared the biomechanics of various constructions, concluding that plates applied parallel to each other offered the greatest stability. Tian et al. tested various double-plate methods in axial compression and flexion (simulated by extension of the whole elbow joint), and despite some methodological differences, the results revealed greater compressive stiffness with the parallel plate system13.
O’Driscoll et al. noted that perpendicular plates cannot withstand varus loads and maintain compression between the diaphysis and metaphysis16. They also reported that compression of the supracondylar region could be achieved with a parallel plate system16. However, it is not possible to achieve this structure in all fractures, particularly in fractures with posterolateral bone defects. Placement of the lateral plate may be difficult because muscles and ligaments adhere to the lateral column. The placement of the posterolateral plate would be much easier. In addition, removal of the implant due to skin irritation is much more common with lateral plates13.
Kumar et al. concluded that parallel plate placement is an excellent method of fixation, with results similar to those obtained with orthogonal placement17.
In contrast, Jacobson et al. conducted a biomechanical study of the torsional and flexural stiffness of perpendicular and parallel braces, but in contrast to our results, the perpendicular brace had greater flexural and varus stiffness18.
Similarly, the Association for the Study of Internal Fixation (AO) group also recommended the use of perpendicular plates for distal humeral fractures12.
Nevertheless, a comparison of these studies would not be possible because of differences in implant types, fracture patterns, mechanical tests, screw types and the number of screws used in these studies. In most of the studies that demonstrated the superiority of parallel fixation systems, 3.5 mm nonlocking plates were used for posterolateral fixation. It could be difficult to achieve adequate fixation of the distal fragment with these plates, and the number of screws that could be applied to the distal fragment would be limited. With the new precontoured locking plates, it would be possible to fix the distal fragment with four 2.7 mm locking screws14.
This study greatly contributes to the field of orthopedic surgery by directly comparing two well-established double-plate fixation techniques (orthogonal and parallel plating) for the treatment of intercondylar humeral fractures via precontoured plates. It is noteworthy that there are few clinical comparative studies in this domain ; most comparative studies available are mechanical in nature4,10,11,14,15,18. Unlike many prior investigations1,3,5that examined these techniques in isolation or employed various methodologies, our research provides a head-to-head comparison of both clinical and radiographic outcomes.
Our findings reveal that both orthogonal and parallel plating methods result in comparable clinical outcomes, as evidenced by the Mayo elbow performance score (MEPS) and similar radiographic parameters, including healing times and complication rates.
By employing a rigorous retrospective design and evaluating a substantial number of cases with an extended follow-up period, this study contributes to the ongoing debate regarding the optimal plating method for distal humeral fractures.
In summary, this comparative analysis provides a solid foundation for future prospective studies. Further research is needed to explore the relationship between plating methods and specific fracture patterns, which will help tailor treatment strategies and improve patient outcomes.
Data availability
The database analyzed during the current study is available from the corresponding author on reasonable request.
References
Hani, R. et al. 2017 Surgical treatment of the humeral pallet fractures in adults. Pan Afr. Med. J. 26 79. https://doi.org/10.11604/pamj.2017.26.79.10781
Kamineni, S. & Morrey, B. F. Distal humeral fractures treated with noncustom total elbow replacement. J. Bone Joint Surg. Am. 86(5), 940–947. https://doi.org/10.2106/00004623-200405000-00009 (2004).
Saragaglia, D., Rouchy, R. C. & Mercier, N. Fractures of the distal humerus operated on using the Lambda plate: report of 75 cases at 9.5 years follow-up. Orthop. Traumatol. Surg. Res. 99(6), 707–712. https://doi.org/10.1016/j.otsr.2013.04.007 (2013).
Schemitsch, E. H., Tencer, A. F. & Henley, M. B. Biomechanical evaluation of methods of internal fixation of the distal humerus. J. Orthop. Trauma. 8(6), 468–475 (1994).
Bégué, T. Articular fractures of the distal humerus. Orthop. Traumatol. Surg. Res. 100 (Suppl 1), 55–63. https://doi.org/10.1016/j.otsr.2013.11.002 (2014).
Paul, H. & Kim, M. D. Seth S. Leopold Gustilo-Anderson Classif. Clin. Orthop. Relat. Res. 470(11) 3270–3274. https://doi.org/10.1007/s11999-012-2376-6 (2012).
Cusick 1, M. C., Nicolas, S., Bonnaig 1, Frederick, M. & Azar 1, B. M. Mauck 1, Richard A Smith 1, Thomas W Throckmorton. 2014 Accuracy and reliability of the Mayo Elbow performance score. 39(6) 1146–1150. https://doi.org/10.1016/j.jhsa.2014.01.041
Lee, S. K., Kim, K. J., Park, K. H. & Choy, W. S. 2014 a comparison between orthogonal and parallel plating methods for distal humerus fractures: a prospective randomized trial. Eur. J. Orthop. Surg. Traumatol. 24(7) 1123–1131. https://doi.org/10.1007/s00590-013-1286-y
Jupiter, J. B., Neff, U., Holzach, P. & Allgöwer, M. Intercondylar fractures of the humerus: an operative approach. J. Bone Joint Surg. Am. 67 (2), 226–239 (1985).
Helfet, D. L. & Hotchkiss, R. N. Internal fixation of the distal humerus: a biomechanical comparison of methods. J. Orthop. Trauma. 4 (3), 260–264. https://doi.org/10.1097/00005131-199004030-00004 (1990).
Schwartz, A., Oka, R., Odell, T. & Mahar, A. Biomechanical comparison of two different periarticular plating systems for stabilization of complex distal humerus fractures. Clin. Biomech. 21 (9), 950–955. https://doi.org/10.1016/j.clinbiomech.2006.04.018 (2006).
Stoffel, K., Cunneen, S., Morgan, R., Nicholls, R. & Stachowiak, G. Comparative stability of perpendicular versus parallel double-locking plating systems in osteoporotic comminuted distal humerus fractures. J. Orthop. Res. 26 (6), 778–784. https://doi.org/10.1002/jor.20528 (2008).
Tian, D., Jing, J., Qian, J. & Li, J. Comparison of two different double-plate fixation methods with olecranon osteotomy for intercondylar fractures of the distal humeri of young adults. Exp. Ther. Med. 6 (1), 147–151. https://doi.org/10.3892/etm.2013.1102 (2013).
Atalar, A. C. et al. Biomechanical comparison of orthogonal versus parallel double plating systems in intraarticular distal humerus fractures. Acta Orthop. Traumatol. Turc. 51 (1), 23–28. https://doi.org/10.1016/j.aott.2016.11.001 (2017).
Penzkofer, R., Hungerer, S., Wipf, F., von Oldenburg, G. & Augat, P. Anatomical plate configuration affects mechanical performance in distal humerus fractures. Clin. Biomech. 25 (10), 972–978. https://doi.org/10.1016/j.clinbiomech.2010.07.005 (2010).
DriscollSW Optimizing stability in distal humeral fracture fixation. J. Shoulder Elb. Surg. 14, 186–194. https://doi.org/10.1016/j.jse.2004.09.033 (2005).
Kumar, S., Singh, S., Kumar, D., Kumar, N. & Verma, R. Intercondylar humerus fracture: parallel plating and its results. J. Clin. Diagn. Res. 9 (1), 1–4. https://doi.org/10.7860/JCDR/2014/12137.5479 (2015).
Jacobson, S. R., Glisson, R. R. & Urbaniak, J. R. Comparison of distal humerus fracture fixation: a biomechanical study. J. South. Orthop. Assoc. 6 (4), 241–249 (1997).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Sami Bahroun, Hamdi Grami, Mohamed Samih Kacem, Alaa Aloui, Zied Jlalia and Mohamed Samir Daghfous. The first draft of the manuscript was written by Sami Bahroun and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
The authors affirm that the human research participants provided informed consent for the publication of the radiographs in Figures 1 and 2
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bahroun, S., Grami, H., Kacem, M. et al. Comparative analysis of two double-plate fixation techniques for intercondylar fractures of the distal humerus. Sci Rep 14, 23913 (2024). https://doi.org/10.1038/s41598-024-73299-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-73299-7
Keywords
This article is cited by
-
Parallel vs. Orthogonal dual plating for distal humerus fractures: a systematic review and pooled analysis of functional outcomes and union times
Journal of Orthopaedic Surgery and Research (2026)
-
Evaluation of internal fixation stability of distal humerus C-type fractures based on musculoskeletal dynamics: finite element analysis under dynamic loading
Journal of Orthopaedic Surgery and Research (2025)
-
Factors influencing elbow function after internal fixation of complex distal humeral fractures in adults
Scientific Reports (2025)
