
Abstract
Injury recurrence in young children is a significant public health concern, as it may indicate an unfavorable home environment. This study evaluates whether infantile injuries increase recurrence during preschool years, contributing to more effective prevention strategies for vulnerable families. The study included 20,191 children from “The Longitudinal Survey of Babies in the 21st Century,” a representative sample of infants born in Japan between May 10 and 24, 2010. We conducted a logistic regression analysis to compare injury recurrence risk between children aged 18 months to seven years with and without infantile injury histories. The study revealed that infants with a history of injuries had a higher risk of subsequent hospital visits for injuries during preschool years (crude Odds Ratio (cOR) 1.52, 95% CI, 1.41–1.64, adjusted OR (aOR) 1.48, 95% CI 1.37–1.60). Specific injuries, such as falls (aOR 1.34, 95% CI, 1.26–1.43), pinches (aOR 1.22, 95% CI, 1.15–1.29), drowning (aOR 1.29, 95% CI, 1.19–1.40), ingestion (aOR 1.35, 95% CI, 1.17–1.55), and burns (aOR 1.47, 95% CI, 1.31–1.65), independently increased the risk of future injuries. Our findings highlight the necessity of universal safety measures in the home environment and targeted interventions for families with a history of high-risk injuries.
Similar content being viewed by others

Introduction
Pediatric injuries have always been a worldwide public health concern. The World Health Organization reported 18,000 injury-related deaths in children under 15 years old1. Although the burden of pediatric injuries in disability-adjusted life years dropped from 1990 to 20152, approximately 10% of preschool-aged children still require emergency room treatment each year3.
Infants, toddlers, and preschool-aged children are often injured at home4,5. Burns, choking, and drowning are the leading causes of fatal home injuries, whereas falls and cuts are nonfatal, but very common6,7,8. Injury recurrence is a significant issue that needs to be addressed because potential hazards in the living environment can persist. For example, children less than three years old with burns were more likely to be hospitalized by the age of six9. Forensic evidence revealed that 15.6% of autopsied infants had one or more bruises10 and the rate of recurrent head trauma rose to 55%, with previous episodes of ecchymoses and bone fractures in abusive head trauma cases11. However, previous studies have some limitations. Many reports focused on a single type of injury, and the effects brought by multiple injuries are not well-described. Additionally, surveys used in most of the literature started retrospectively from the onset of the injury, which varied from case to case, making the optimal intervention time unclear. Extracted data from hospitals or child welfare services may only capture occurrences of injuries in charts or documents. Therefore, a comprehensive study on injury recurrence in this age group is warranted.
The objectives of this study are to confirm whether experiences of injuries at 18 months of age can predict subsequent serious events, and to elucidate the impact of injury types and developmental characteristics on recurrent injuries. To achieve these objectives, we conducted a survey as part of a large cohort study, “The Longitudinal Survey of Babies in the 21st Century,” and analyzed the resulting dataset.
Methods
Study participants
The Japanese Ministry of Health, Labor, and Welfare (MHLW) implemented a large cohort study, “The Longitudinal Survey of Babies in the 21st Century,” which focuses on family circumstances, child-rearing, and children’s health and developmental status. A description of the study methods has been previously published12,13,14. The MHLW possesses two data sets on children born in 2001 and 2010. For this study, we utilized the latter, an ongoing survey that targeted 43,767 families with infants born between May 10 and 24 in 2010. After the first questionnaires were mailed when the infants were six months old, 38,554 answers were received, resulting in an 88.1% response rate. Follow-up questionnaires were sent annually when children reached 18, 30, 42, and 54 months old and at 1.5-year intervals between 66 months and seven years old.
This study was approved by the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Science Institutional Review Board (K1506-073). The study results adhere to the principles outlined in the Declaration of Helsinki and the STROBE guidelines15. Since this research is a retrospective study and the records do not contain personally identifiable information, the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Science Institutional Review Board waived the need for informed consent.
Injuries in infants and preschool-aged children
We defined “injuries in infants” as injuries experienced by children between six to 18 months of age (one year prior to the second survey at 18 months). These injuries included falls, pinches, cuts, bites, drowning, ingestion, choking, burns, traumatic accidents, and other conditions (as indicated in Supplement Fig. 1). Children aged 18 months to seven years old who visited a doctor due to bone fracture, burn, or other injury within each year from the third to the seventh survey were categorized as “injuries in preschool-aged children” in this study (as shown in Supplemental Fig. 2 to 6).

Patient flow diagram with numbers of eligible children.
Inclusion
A total of 32,407 children responded to the question regarding their experience of injuries in the second survey. From this group of eligible children, 20,191 were included based on their responses: they either answered “no” to injuries in all the required questionnaires or “yes” to at least one of them between the third and seventh surveys. Meanwhile, 12,216 children were categorized as “lost to follow-up” due to missing responses.
The “injury” and “no injury” groups comprised children with or without hospital visits from 18 months to seven years old, with 7,179 and 13,012 children included in each group, respectively (Fig. 1).
Statistical analysis
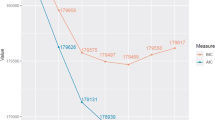
The primary outcome was hospital visits for injuries occurring between 18 months and seven years old. In the logistic regression analysis, we examined the association between injury types in the second survey and the outcome, using both the crude and adjusted odds ratios (cOR and aOR). We also performed a stratified analysis on children according to the presence or absence of problematic behavior at 66 months old. Children were categorized as having problematic behavior if families recognized children’s difficulties with any of these actions: listening to others, holding attention, patience, expressing feelings, acting in groups, and keeping promises (as shown in Supplemental Fig. 7).
To adjust for confounding factors, socioeconomic status and biological characteristics were collected from the first or the second survey as well as birth records linked to each child’s survey data. Variables include children’s sex (dichotomous), term or preterm birth (dichotomous; <37 weeks of gestation), singleton or not (dichotomous), birth order (categorical; one, two, ≥three), daycare attendance at 18 months old (dichotomous), maternal age at delivery (categorical; <25, 25–29, 30–34, ≥ 35 years old), maternal educational attainment (categorical; ≤high school, junior college, ≥university), parents’ smoking status (dichotomous), and residential area (categorical; wards or districts, cities, towns, or villages). We first conducted a comparison between eligible children and children lost to follow-up to evaluate the impact of the lost cases. We also compared the baseline characteristics of the “injury” and “no injury” groups. All confidence intervals (CI) were calculated at the 95% level. All statistical analyses were performed with Stata version 17 statistical software (StataCorp LP, College Station, TX, USA).
Results
Table 1 shows the baseline characteristics of the enrolled children and the children lost to follow-up. Children in the lost cases were less likely to encounter injuries at the age of 18 months. They also demonstrated a greater tendency to be girls, have more than two siblings, have a younger and lower-educated mother, attend a nursery facility, be nurtured by parents with smoking habits, and live in more rural areas. The characteristics of the “injury” and “no injury” groups are summarized in Table 2, revealing no significant differences except for variables of sex, singleton, and daycare attendance. The relationship between the experience of injuries in infants and hospital visits due to trauma in preschool-age children is shown in Fig. 2 and the Supplemental Table. Overall, 6,067 out of 16,239 (37.4%) infants with a positive history of injuries saw a doctor due to trauma before seven years old. Univariable and multivariable logistic regression analysis showed that children with infantile injuries have an increased risk of hospital visits for injuries during preschool age (cOR 1.52, 95% CI 1.41–1.64, and aOR 1.48, 95% CI 1.37–1.60, respectively). Among all types of injuries, falls, pinches, drowning, ingestion, burns, and others were independent risks for later injuries (falls: aOR 1.34, 95% CI 1.26–1.43, pinches: aOR 1.22, 95% CI 1.15–1.29, drowning: aOR 1.29, 95% CI 1.19–1.40, ingestion: aOR 1.35, 95% CI 1.17–1.55, burns: aOR 1.47, 95% CI 1.31–1.65, and others: aOR 1.57, 95% CI 1.35–1.83). The occurrence of injuries was similar in preschool-aged children with or without problematic behaviors at the age of 66 months (aOR 1.72, 95% CI 1.42–2.08, and aOR 1.44, 95% CI 1.32–1.57), as shown in Table 3.

The association between infantile injuries and preschool-aged trauma.
Discussion
This study examined the association between infantile injuries and preschool-aged trauma in a nationwide cohort study. Our results suggest that there should be required interventions for potential persistent harm in children’s living environments. This conclusion is supported by the large amount of data collected through a long-term follow-up of the same population group, which is a unique and advantageous aspect of this study. Additionally, our study’s high response rate to questionnaires increases the reliability of our results.
The cause of pediatric injury is multifactorial, including familial societal status, a lack of safety conditions, and children’s developmental characteristics1,16. The comparison of our “injury” and “no injury” groups showed that only the sex of boys was a significant risk factor, as shown in previous studies17, indicating that these two groups have similar familial backgrounds. The first point to note is that 80.4% of eligible children had encountered some kind of injuries before 18 months of age in Japan. Moreover, this study suggests that children who experienced injuries during infancy were at a higher risk of recurrent injuries during preschool years due to potentially continued or frequent exposure to unsafe environments or situations, where even less mobile infants were prone to injury. Injury prevention is facilitated by a combination of environmental and behavioral modification18. Patient education, for example, plays an essential role in reducing the incidence of home accidents7,19. The perception of household risks for injuries helps caregivers enforce guidance to avoid exposing children to danger20. Counseling has brought positive changes in knowledge or behaviors related to the injuries of falls, poisoning, burns, traumatic accidents, and drowning21,22,23. These universal efforts for injury prevention must be reinforced to reduce tragedies at home.
Logistic regression analysis revealed that falls, pinches, drowning, ingestion, and burns were independently related to injury recurrence. Although “others” was also related to later injuries, injury types were miscellaneous and not standardized due to free description. Considering the typical developmental course, some of these hazardous situations can be related to not only equipment safety matters but also improper parenting, such as inadequate adult supervision or inappropriate baby handling, potentially associated with child maltreatment (CM). This finding is basically consistent with findings from previous literature24,25. Burns and drowning are known to be associated with CM, especially neglect, with a high fatality rate26,27,28,29. As for injury persistence, increased later hospitalization in burn cases and repetition of head trauma were reported9,30. However, our finding is notable in that the recurrence was not limited to the original injury type but generalized to various injuries, such as burns and bone fractures, which required hospital visits. Namely, infants who suffer from certain injury types may be at risk of experiencing subsequent severe traumas caused by unfavorable nurturing environments during preschool age. This chronicity can lead to future negative outcomes, including deficit in educational achievement, mental health problems, and substance use24,31,32,33. Children with behavioral or attention problems are vulnerable to accidental injuries34,35, and our data showed a similar trend in children with problematic behaviors at 66 months. However, the recurrence risk was comparable to children with or without personality issues, possibly meaning that factors other than children’s developmental characteristics might play a significant role in injury recurrence during preschool age.
Eighteen months old is the time when key developmental milestones occur36. In Japan, a well-child care visit at this age is one of the mandatory health examinations as defined by the Japanese Maternal and Child Health Act, with over 95% of children undergoing this checkup annually37. Regular checkups provide excellent opportunities for identifying and intervening in various problems through health and developmental screenings. However, Hammig et al. reported that only 15% of pediatric injury cases received counseling about prevention before their occurrence38. Given this situation, a thorough introduction of general education for household injury is prioritized as we mentioned above. Furthermore, if children have experienced high-risk types of injuries at 18 months of age, intensive observation should be considered. Globally, programs like the Injury Prevention Program (TIPP) in the U.S., which integrates tailored safety advice into pediatric well-child visits, have significantly decreased injury rates among young children by improving parental awareness and preventive action39. Similarly, Sweden’s Safe Communities Model and Australia’s Kidsafe Program have demonstrated substantial reductions in child injuries through community-based approaches focusing on safer home, school, and public environments40. These examples underscore the importance of integrating data-driven, multi-faceted prevention strategies into public health policies to mitigate the recurrence of childhood injuries, especially in high-risk families.
Our study has several limitations. Injury severity is not addressed in this study, as only “yes” or “no” answers regarding injuries were obtained. However, a minor injury is sometimes recognized as a herald of escalating abuse41. The intervention should be initiated regardless of severity if a family answers “yes” to an injury experience at 18 months old. While approximately 10% of families with children born during the study period declined to participate, the response rate was high enough to ensure the generalizability of the results. Another important point about the sampling is that the children included were all born within a specific period of the year, which may underrepresent certain types of injury, such as those related to seasonal activity. The group lost to follow-up might be more likely to be victimized by an unfavorable nurturing environment because it demonstrated some common societal contributors to injuries, such as young maternal age, limited education level, or rural residential area3,42, which leads to underestimation of the results. There are various biases inherent in self-reporting studies. Recall bias can occur to some extent, although the duration of recall was not so long. Social desirability bias may lead to underreporting of injury. Additionally, the way parents understand the questions and recognize the onset of injuries may vary based on their subjective perspectives, which could also affect the results. Lastly, although the data is somewhat dated, the study is ongoing, and combining this dataset with more recent data in future analyses will provide further insights.
Conclusion
Our findings indicated that the experience of injury at the age of 18 months presented an increased risk for recurrent injury before seven years old, even if they don’t have problematic behaviors. To reduce the likelihood of recurring injuries, it’s essential to implement safety measures in the home environment for children under 18 months old who have a history of injuries, especially injuries related to falls, pinches, drownings, ingestions, and burns, as they showed independent relations to recurrence.
Data availability
Data derived from a source in the public domain, but the access to the data analyzed in this study is restricted under the license for the current study from MHLW. To obtain data from this study, you must apply directly to the MHLW. For further details, please contact the corresponding author.
References
Organization, W. H. Preventing Injuries and Violence: An Overview13 (p. (World Health Organization, 2022).
Kassebaum, N. et al. Child and adolescent Health from 1990 to 2015: findings from the Global Burden of diseases, injuries, and risk factors 2015 study. JAMA Pediatr. 171, 573–592 (2017).
Azar, S. T., Miller, E. A., Stevenson, M. T. & Johnson, D. R. Social Cognition, Child Neglect, and child Injury Risk: the contribution of Maternal Social Information Processing To Maladaptive Injury Prevention Beliefs within a high-risk sample. J. Pediatr. Psychol. 42, 759–767 (2017).
Morrongiello, B. A., Midgett, C. & Shields, R. Don’t run with scissors: young children’s knowledge of home safety rules. J. Pediatr. Psychol. 26, 105–115 (2001).
Powell, E. C. & Tanz, R. R. Adjusting our view of injury risk: the burden of nonfatal injuries in infancy. Pediatrics. 110, 792–796 (2002).
Gielen, A. C., McDonald, E. M. & Shields, W. Unintentional home injuries across the life span: problems and solutions. Annu. Rev. Public. Health. 36, 231–253 (2015).
Altundağ, S. & Körükçü, Ö. Risk reduction education to prevent Preschool Children’s Home accidents: a pilot study. Disaster Med. Public. Health Prep. 17, e115 (2022).
DeGeorge, K. C., Neltner, C. E. & Neltner, B. T. Prevention of Unintentional Childhood Injury. Am. Fam Physician. 102, 411–417 (2020).
Hutchings, H., Barnes, P. M., Maddocks, A., Lyons, R. & James-Ellison, M. Y. Burns in young children: a retrospective matched cohort study of health and developmental outcomes. Child. Care Health Dev. 36, 787–794 (2010).
Ingham, A. I., Langlois, N. E. & Byard, R. W. The significance of bruising in infants–a forensic postmortem study. Arch. Dis. Child. 96, 218–220 (2011).
Adamsbaum, C., Grabar, S. & Mejean, N. Rey-Salmon, C. Abusive Head Trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 126, 546–555 (2010).
Obara, T. et al. Short or irregular sleep duration in early childhood increases risk of Injury for Primary School-Age children: a Nationwide Longitudinal Birth Cohort in Japan. Int. J. Environ. Res. Public. Health 18, 9512 (2021).
Yamakawa, M., Yorifuji, T., Inoue, S., Kato, T. & Doi, H. Breastfeeding and obesity among schoolchildren: a nationwide longitudinal survey in Japan. JAMA Pediatr. 167, 919–925 (2013).
Kikkawa, T. et al. Birth order and paediatric allergic disease: a nationwide longitudinal survey. Clin. Exp. Allergy. 48, 577–585 (2018).
Vandenbroucke, J. P. et al. Strengthening the reporting of Observational studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 4, e297 (2007).
Hyder, A. A., Wali, S., Fishman, S. & Schenk, E. The burden of unintentional injuries among the under-five population in South Asia. Acta Paediatr. 97, 267–275 (2008).
Morrongiello, B. A., Corbett, M., Colwell, S., Bryant, L. & Cox, A. A longitudinal study of boys’ and girls’ injury-risk behaviors and parent supervision during infancy. Infant Behav. Dev. 68, 101729 (2022).
Jullien, S. Prevention of unintentional injuries in children under five years. BMC Pediatr. 21, 311 (2021).
Gaw, C. E. et al. Pediatric Health Care Provider Perspectives on Injury Prevention Counseling in Acute and Primary Care settings. Clin. Pediatr. (Phila). 59, 1150–1160 (2020).
Lagziel, T. et al. Public perception of household risks for pediatric burn injuries and assessment of management readiness. Burns. 49, 1305–1310 (2023).
Zonfrillo, M. R., Gittelman, M. A., Quinlan, K. P. & Pomerantz, W. J. Outcomes after injury prevention counselling in a paediatric office setting: a 25-year review. BMJ Paediatr. Open. 2, e000300 (2018).
Tupetz, A. et al. Prevention of childhood unintentional injuries in low- and middle-income countries: a systematic review. PLoS One. 15, e0243464 (2020).
Yusuf, S., Jones, J. L., Camp, E. A. & McCallin, T. E. Drowning prevention counselling by paediatricians to educate caregivers on water safety. J. Paediatr. Child. Health. 58, 1584–1593 (2022).
Gilbert, R. et al. Burden and consequences of child maltreatment in high-income countries. Lancet. 373, 68–81 (2009).
Coohey, C. Defining and classifying supervisory neglect. Child. Maltreat. 8, 145–156 (2003).
Hollen, L., Bennett, V., Nuttall, D., Emond, A. M. & Kemp, A. Evaluation of the efficacy and impact of a clinical prediction tool to identify maltreatment associated with children’s burns. BMJ Paediatr. Open. 5, e000796 (2021).
Feldman, K. W., Monastersky, C. & Feldman, G. K. When is childhood drowning neglect? Child. Abuse Negl. 17, 329–336 (1993).
Harpole, B. G., Wibbenmeyer, L. A. & Erickson, B. A. Genital burns in the national burn repository: incidence, etiology, and impact on morbidity and mortality. Urology. 83, 298–302 (2014).
Kennedy, J. M., Lazoritz, S. & Palusci, V. J. Risk factors for child maltreatment fatalities in a National Pediatric Inpatient database. Hosp. Pediatr. 10, 230–237 (2020).
Jenny, C., Hymel, K. P., Ritzen, A., Reinert, S. E. & Hay, T. C. Analysis of missed cases of abusive head trauma. Jama. 281, 621–626 (1999).
Green, J. G. et al. Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: associations with first onset of DSM-IV disorders. Arch. Gen. Psychiatry. 67, 113–123 (2010).
Jonson-Reid, M., Kohl, P. L. & Drake, B. Child and adult outcomes of chronic child maltreatment. Pediatrics. 129, 839–845 (2012).
Beveridge, J. K. et al. Examining parent adverse childhood experiences as a distal risk factor in Pediatric Chronic Pain. Clin. J. Pain. 38, 95–107 (2021).
İz, M. & Çeri, V. Prevalence of Attention Deficit Hyperactivity Disorder Symptoms in Children Who Were Treated at Emergency Service due to Unintentional Injury. Emerg Med Int. 7814910 (2018). (2018).
Garzon, D. L., Huang, H. & Todd, R. D. Do attention deficit/hyperactivity disorder and oppositional defiant disorder influence preschool unintentional injury risk? Arch. Psychiatr Nurs. 22, 288–296 (2008).
Mousmanis, P. & Watson, W. J. The 18-month well-child visit in primary care: clinical strategies for early intervention. Paediatr. Child. Health. 13, 845–849 (2008).
Report of Vital Statistics: Occupational and Industrial Aspects General mortality Fiscal yearly 2022 (written in Japanese)https://www.e-stat.go.jp/stat-search/database?statdisp_id=0003411661 (Accessed 2023, June 25).
Hammig, B. & Jozkowski, K. Prevention counseling among pediatric patients presenting with unintentional injuries to physicians’ offices’ in the United States. Prev. Med. 74, 9–13 (2015).
Perrin, E. M. et al. The Injury Prevention Program to Reduce Early Childhood injuries: a Cluster Randomized Trial. Pediatrics.153, e2023062966 (2024).
Spinks, A., Turner, C., McClure, R. & Nixon, J. Community based prevention programs targeting all injuries for children. Inj Prev. 10, 180–185 (2004).
Pierce, M. C. et al. History, injury, and psychosocial risk factor commonalities among cases of fatal and near-fatal physical child abuse. Child. Abuse Negl. 69, 263–277 (2017).
Putnam-Hornstein, E. Report of maltreatment as a risk factor for injury death: a prospective birth cohort study. Child. Maltreat. 16, 163–174 (2011).
Author information
Authors and Affiliations
Contributions
T.H. and T.O. conceptualized and designed the study, carried out the initial analyses, drafted the initial manuscript, and critically reviewed and revised the manuscript. N.M. and T.Y. designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript. K.T., T.H., T.N., M.H., T.Y., A.N. and H.N. coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hiraoka, T., Obara, T., Matsumoto, N. et al. A nationwide longitudinal survey of infantile injury and its recurrence in Japan. Sci Rep 14, 24716 (2024). https://doi.org/10.1038/s41598-024-76403-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76403-z
