
Abstract
The current study aimed to explore the effect of daily caffeine supplementation (100 mg/day) and 12-week of Zumba training on functional performances in middle-aged women. Eighty-five middle-aged women were randomized into 4 groups including control, Zumba training (ZT), caffeine supplementation (Ca) or caffeine-Zumba training (Ca + ZT) groups. Functional performances were assessed using 10 m Walk, Timed Up and Go, Functional Reach, and 30-Second Chair Stand tests. As results, ZT, Ca and Ca + ZT intervention programs showed a significant (p < 0.05) functional performances improvement. However, Ca + ZT group showed significant (p < 0.001) better scores in terms of mobility (95%CI [0.71, 1.43]), gait speed (95%CI [0.52, 1.71]) and lower body endurance strength (95%CI [-6.93, -1.92]), except for dynamic balance (95%CI [-9.41, -3.44]). In conclusion, 12-week of Zumba training improves functional performances in middle-aged women, and daily caffeine intake is an effective alternative for improving such performances. Supplementing caffeine (100 mg/day) to Zumba training was effective in boosting Zumba benefits on these functional performances.
Similar content being viewed by others
Introduction
Middle-aged period is an important event in women life corresponding to the menopausal stage, in which they often suffer from multiple emotional instability, sexual dysfunction, vasomotor symptoms, musculoskeletal pain and mood alterations1,2, altering health-related fitness3. Most of these changes alter health-related fitness in term of muscle strength, endurance and mass, flexibility and cardiovascular endurance3,4, which increase dependence in performing daily activities, significantly raising healthcare costs5. Disability issues and limitations in physical functioning (i.e. reduced strength, flexibility, walking speed, mobility and postural instability) are common in middle-aged6, inducing a higher risk of falls mainly for middle-aged women7,8.
Physical fitness is vital for maintaining health and ensuring well-being at every stage of life. It refers to the ability to perform daily life activities safely and independently without experiencing fatigue, involving biomotor abilities like strength, endurance, flexibility, agility, balance, and coordination9. The literature revealed that physical fitness can be assessed through multiple test batteries, such as the Groningen Fitness Test10, Senior Fitness Test11, and Alpha Fit Test Battery12. Particularly, the Senior Fitness Test battery was commonly used to assess the functional capacities among women aged over 50 years old8,13.
Importantly, physical activity has been stated as a crucial element in preventing and managing aging-related problems (i.e. chronic diseases, functional limitations, and dependency), notably for middle-aged women, to maintain their physical functioning14, enhancing overall quality of life15,16. Nevertheless, these women are usually inactive17, with approximately 57.84% reporting low levels of physical activity18. In fact, during the menopausal transition, previous studies found a significant reduction in daily energy expenditure and a shift toward a more sedentary19,20, which could lead to serious health problems21. Therefore, enjoyable and convenient exercise programs should be designed in order to encourage these women to adhere to the recommended exercise regimes.
Importantly, Zumba dance is one of the most successful dance-fitness program and popular high-impact physical activities especially for women22,23. It’s a dance class that features Latin rhythms (merengue, salsa, bachata, hip hop) engaging whole-body movements and creating a kind of choreography24. It is a potential type of exercise for inducing improvements in functional capacity (cardiorespiratory fitness, walking speed, muscle strength and endurance, and dynamic balance) in women with or without clinical conditions25,26,27,28. Recently, 12 weeks of a Zumba training program was reported to have positive effects on static balance, muscle strength, mood and quality of life in postmenopausal women29. These authors called for further exploration of the implications of these findings to better understand the impact and applicability of Zumba training in similar contexts29.
In combination, it has been reported in the literature that one potential way to enhance exercise performance in older adults is to provide adjunctive ergogenic aids like caffeine30. Dietary caffeine intake is common across society, and as a central nervous stimulant, it works by blocking central and peripheral adenosine receptors31. This blockade leads to greater recruitment of motor units32,33. Several studies have been published, culminating in a recent meta-analysis, demonstrating caffeine’s ergogenic effects across various exercise modes, including aerobic endurance, anaerobic power, muscular strength, muscle endurance, exercise speed, and vertical jump height34. Caffeine has been frequently used to boost performance both before and during exercise. Notably, it has been shown to markedly improve the physical and cognitive states of both athletes (i.e. young recreational runners35) and elderly8. Epidemiological data reported that caffeine consumption peaks during the fifties and sixties, likely to alleviate sleepiness due to ongoing social and professional responsibilities36, and has been shown to functional performances in terms of postural balance, muscle strength and endurance, and aerobic endurance in middle-aged women8,37. In particular a low-dose caffeine (i.e. 100 mg) has been recommended as a sufficient dose to significantly improve static and dynamic balance, dual-talk performance and walking speed in middle-aged women37,38. Despite this extensive research, to our best knowledge, no study has examined the simultaneous effects of exercise training and caffeine consumption on functional abilities or daily living activities in middle-aged women.
Based on all of these considerations and the need to provide nutritional strategies along with exercise activities to expedite conclusion and motivate physical activity, this study aimed to explore the effect of 12-week caffeine supplementation (100 mg/day) combined with Zumba training on functional performances, compared to Zumba training alone, in middle-aged women. We hypothesized that (i) both training modalities would have beneficial effects on functional performances; and that (ii) supplementing caffeine with Zumba training would boost these effects in middle-aged women.
Materials and methods
Study design
All aspects of the Declaration of Helsinki were adhered to except preregistration. The study was registered retrospectively at the Ethics Committee of the VASILE ALECSANDRI UNIVERSITY of BACĂU (NR#23219/2/14.12.2023).
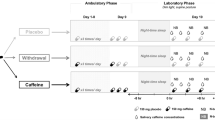
The current study was designed as a randomized single-blind, controlled training intervention, employing a parallel-group design with four groups (a caffeine + Zumba training group (Ca + ZT), Zumba training group (ZT), caffeine supplementation group (Ca) and control group (CG)). The allocation ratio was 1:1:1:1, ensuring equal distribution of participants across the groups. Each participant was randomly allocated by an independent researcher to either a caffeine + Zumba training group (Ca + ZT), Zumba training group (ZT), caffeine supplementation group (Ca) or control group (CG), using a computer-generated simple randomization (Fig. 1). The participant randomization allocation was blinded to the assessment staff using a computer-generated random number sequence for assignment to each group. A code for each participant and group randomization was kept in securely sealed opaque envelopes by a researcher unaware of intervention sequences and not involved in assessments or interventions. Another independent researcher opened the envelopes when all the data had been collected and analyzed.

Study design illustration.
The Ca + ZT group underwent a 12-week Zumba training program combined to daily caffeine supplementation (100 mg/day). The ZT group undertook a 12-week of the same Zumba training program alone, while, the Ca group took part in a 12-week caffeine (100 mg/day) treatment intervention alone. However, the participants in the CG were not engaged to any type of intervention (no training program or caffeine intake) and continued their normal daily activities for the 12-week-period, which were monitored every week using the IPAQ (IPAQ-SF) (Fig. 1). During this period, all participants were asked not to consume any drink and/or food containing caffeine, and they were provided with supplies of decaffeinated coffee or tea in order to facilitate adherence to this requirement.
The evaluation protocol consisted of three test sessions; a familiarization session, a pre-intervention test session and a post-intervention test session (two days before and after 12-week) (Fig. 1). When conducting all pre- and post-intervention evaluations, the experimenters were blinded to group allocation.
Participants
The G*power software (version 3.1.9.2; Kiel University, Kiel, Germany)39was used to calculate the required sample size. Parameters such as effect size, alpha, power, correlation among repeated measures, and non-sphericity correction (ε) were set at 0.4, 0.05, 0.80, 0.50, and 1, respectively. According to the estimated sample size suggested by Ben Waer et al., 2023 using the same G*Power software, a sample size of 10 participants per group, for combined effects of caffeine and Zumba training on postural balance, was initially calculated40. Based on its findings, Cohen f effect size established at 0.48. The analysis was conducted with a significance level of 0.05, and a power of 0.8 was examined, incorporating considerations for four groups, two measurements and an assumed correlation of 0.5 between repeated measurements. Consequently, the resulting sample size for the current study was computed as a minimum of 12 participants per group.
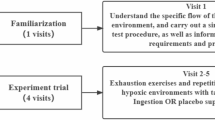
Considering an estimated drop out of 30%, 107 voluntary middle-aged women, aged between 50 and 60 years, were recruited to participate in this study. To ensure that they met al.l inclusion criteria, all the participants completed the Medical Health History (MHQ41), , the Caffeine Consumption Questionnaire-Revised (CCQ-R42), , the International Physical Activity (IPAQ43), , the Self-Rated Fall Risk (FRQ44), , the Women’s Health (WHQ45), and the Mini Mental State Examination (MMSE46), questionnaires. Only eighty-five women, who were healthy (MHQ, WHQ and MMSE), non-habitual caffeine consumers (CCQ-R), inactive (IPAQ), with a mild risk for falling (FRQ), not engaged in a structured physical activity in the prior 6-month and no previous experience of Zumba and non-users of any medical substances or nicotine or treatments that could mask the effects of caffeine, included in this study (Table 1). Women how had a history of cardiovascular, neurological, metabolic disorders or any other medical conditions that interact with caffeine (MHQ) were excluded from this study. The protocol distribution demonstrated in Fig. 2.

The flowchart of participant enrollment.
Data were collected at a fitness center where supervised Zumba training sessions took place, and in the homes of participants for daily caffeine consumption. Monitoring was done through questionnaires and functional performance tests administered at the same location.
Intervention programs
Zumba training
Zumba exercises were applied to the participants for 12-week at a rate of three 1-h sessions/week on non-consecutive days at a fitness center and supervised by professional Zumba trainers. The Zumba training program consisted of continuous dance movements to Latin music, there are 8–10 different dance choreographies for each session with varying intensity level throughout the sessions (Supplementary Table S1).
Each training session was initiated with a 10 min warm-up (easy Zumba elements, dynamic stretching and fast music to elevate HR from 50 to 60% of HRmax), followed by a 45 min Zumba main part (Its intensity was set between 60 and 75% of HRmax) and a 5 min cool down section (with an intensity of around 40% of HRmax to eliminate fatigue) (Supplementary Table S1). Intensity was gradually increased every two weeks with increasing the combination and complexity of the tasks in order to maintain motivation and exercise efficiency11,28.
A combination of individual monitoring and group management techniques was used to control exercise intensity by percentage HRmax for each participant. On the first visit, we measured the participants’ HRmax using the Tanaka et al. formula (HRmax = 208 − (0.7 × age))47. Next, the percentage of HR was estimated through the reserve HR (HRR method: Target HR (THR) = [(HRmax − HRrest) × % Intensity] − HRrest). The HR was collected from the start to the end of each section (pre-exercise, warm-up, main workout part, and cool-down) during each training session. Relative exercise intensity during each exercise section was calculated by devising the HRmax value by the HR measured during exercise, and this calculated number was then multiplied by 10048.
Besides, participants were considered as having completed the training program if they attended to a minimum of 90% of the training sessions that were a minimum of 33 sessions.
Caffeine supplementation protocol
All participants of both Ca + ZT and ZT groups were given their capsule supply (100 mg of pure caffeine or placebo (0 mg of caffeine)) that should be consumed every day (60 min prior each training session in the training days and in the morning, morning, at a constant time “09:00am”, prior to breakfast in the non-training days) with a cup of water. Participants were contacted, by telephone, every day during the intervention period to remind them of the time to take the capsule. Each capsule was intake by the double-blind method. An independent researcher prepared the treatment capsules for both groups (with caffeine or placebo) and put them into envelopes according to the allocation orders. These capsules contained the same color and volume and were not distinguished. Both participants and experimenters were blinded to capsules-allocated.
Concerning the Ca group, each participant consumed every day a caffeine capsule contains 100 mg/day of pure caffeine in the morning at a constant time with a cup of water during the 12-week intervention period.
Functional performance measurements
As previously described by Ben Waer et al., 202413, , functional performance was assessed by the Senior Fitness Test battery49. This battery included standard tests valid for multiple aging populations, including women over 50 years old, such as Functional Reach Test (FRT)50, Timed Up and Go (TUG) test51, 10-Meter Walk Test (10MWT)52and the 30 S Chair Stand Test (CS-30 test)49.
Lower body endurance strength
The lower body endurance strength was measured using the CS-30 test53. The participant, arms crossed the chest in a seated position on an armless chair, was instructed to complete as many full sit to stand movements at a maximal speed for 30s. The number of stand-to-sit repetitions was considered as the final score. This test provided results with high reliability in healthy women aged 18–59 years (r= 0.71, 95% CI = 0.53-0.84)54,55.
Walking speed
The 10 m Walk Test (10MWT) was used to evaluate walking speed performance. During this test, participants were instructed to walk at their ‘usual walking speed’ for 10 m and no verbal encouragement during the test was provided56. The time (s) to complete the walk was recorded by a digital stopwatch, and considered as the final score. This test exhibited high test-retest reliability: Intraclass correlation coefficient (ICC) = 0.940, CI 95% = (0.904–0.961) for middle-aged women57.
Functional mobility
The functional mobility was assessed by the Timed Up and Go test, where participants were asked to stood from the chair, walk 3 m, turn and return to a seated position as quickly as possible with the duration to complete the test, was taken as a result. The test exhibited high test-retest reliability (ICC = 0.99)58in middle-aged women59.
Dynamic balance
The dynamic balance was evaluated using the Functional Reach Test (FRT). Functional Reach is the maximum forward-reaching distance (cm) that individuals can reach in the forward direction from a comfortable standing posture while fixing their base of support on the floor, without balance loss60. The distance between the first marked position of their third metacarpal bone and the position of the bone was recorded when participants reached maximally. This test has a high inter-rater reliability (ICC = 0.98)60in middle-aged women59.
Statistical analyses
Statistical tests were processed and analyzed using STATISTICA Software (StatSoft, version 12, Paris, France). All data were expressed as means ± standard deviations (SD).
Since data normality distribution and sphericity were confirmed by the Shapiro-Wilk W test and the Mauchly test, respectively, parametric tests were applied. The functional performances (TUGT, CS-30, 10MWT and FRT) were analyzed using a two-way ANOVA [4 groups (CG/ZT/Ca/Ca + ZT) × 2 sessions (pre-/post-intervention)]. Statistical differences were reported by their level of significance. When significant differences were observed, a post-hoc analysis was then performed with the Bonferroni test. Besides, the 95% confidence interval (CI) were also performed61. Effect size was calculated using partial eta squared η2p formula to determine whether a statistically significant difference is a difference of practical concern (small effect: 0.01 < η2p < 0.06; medium effect: 0.06 < η2p < 0.14; and large effect: η2p > 0.14). The alpha level of statistical significance was set as p < 0.05.
Results
Lower body endurance strength
The two-way repeated measures ANOVA revealed a significant main effect of the session (F(1,13) = 30.61, p < 0.001, η2p = 0.7) factor and a significant group × session interaction (F(3,39) = 5.25, p < 0.01, η2p = 0.28) on the lower body endurance strength scores. However, no significant effect of group factor was found. Concerning the session effect, the post-hoc analysis showed that the CS-30 test scores increased significantly during the post- in comparison to the pre-intervention for the Ca + ZT (p < 0.001, 95% CI -6.93 to -1.92), ZT (p < 0.01, 95% CI -5.43 to -0.42) and Ca (p < 0.05, 95% CI -5.36 to -0.34) groups, but not for the CG (Table 2).
Walking speed
The two-way repeated measures ANOVA revealed significant main effects of the group (F(3,36) = 4, p < 0.01, η2p = 0.25) and session (F(1,12) = 65.43, p < 0.001, η2p = 0.84) factors and a significant group × session interaction (F(3,36) = 6.95, p < 0.001, η2p = 0.36) on the 10MWT scores. The post-hoc analysis showed that these scores increased significantly during the post- in comparison to the pre-intervention for Ca + ZT (p < 0.001, 95%CI 0.52 to 1.71), ZT (p < 0.001, 95%CI 0.19 to 1.39) and Ca (p < 0.05, 95%CI 0.04 to 1.23) groups but not for the CG. Moreover, the walking velocity scores were significantly lower in the CZG compared to both Ca (p < 0.05, 95%CI -1.17 to 0.02) and ZT (p < 0.01; 95%CI -1.27 to -0.07) groups (Table 2).
Functional mobility
The two-way repeated measures ANOVA revealed significant main effects of session (F(1,12) = 46.52, p < 0.001, η2p = 0.79) factors and a significant group × session interaction (F(3,36) = 17.68, p < 0.001, η2p = 0.59) on the functional mobility scores. The post-hoc analysis showed that the TUGT scores decreased significantly during the post- in comparison to the pre-intervention for Ca + ZT (p < 0.001, 95%CI 0.71 to 1.43), ZT (p < 0.01, 95%CI 0.07 to 0.79) and Ca (p < 0.05, 95%CI 0.11 to 0.83) groups but not for the CG (Table 2). Moreover, these scores were significantly lower (p < 0.0001) in the Ca + ZT group compared to both Ca (p < 0.001, 95%CI -1.08 to -0.35) and ZT (p < 0.001, 95%CI -1.13 to -0.4) groups (Table 2).
Dynamic balance
The two-way repeated measures ANOVA revealed a significant main effect of the session factor (F(1,12) = 34.95, p < 0.001, η2p = 0.74) and a significant group × session interaction (F(3,36) = 7.57, p < 0.001, η2p = 0.38) on the FRT scores. The post-hoc analysis showed that the reached distance increased significantly during the post- in comparison to the pre-intervention for both Ca + ZT (p < 0.001, 95% CI -9.41 to -3.44) and ZT (p < 0.001, 95% CI -7.91 to -1.94) groups but not for Ca nor CG (Table 2).
Discussion
The results of the current study revealed that the three intervention programs (Ca, ZT, Ca + Zt) were effective to improve functional performances (in term of mobility, endurance strength and walking speed) in these women with more greater effects observed in the Ca + ZT group.
Several authors reported Zumba training benefits, in healthy populations, on muscle strength, autonomy and daily life activities. In this context, previous studies documented the beneficial effect of Zumba training on lower body strength27,28and functional mobility25in young and older women13. Indeed, Zumba fitness has been shown to significantly enhance individuals’ functional and motor abilities62. It incorporates aerobic interval training and strengthening exercises, which significantly improved cardiovascular system and strength of the whole body63. It has been also suggested to meet fitness goals such as achieving body harmony, improving posture, and strengthening the bone-joint segments of the locomotor system64.
Besides, Zumba is a rhythmic aerobic training65with a mixed of Latin dance styles (salsa, reggaeton, cumbia, etc.…)24, based on turning, twisting, stepping and jumping elements, which may lead to a high muscle activity26. This training modality was proved to enhance muscle power and protein mass in young women65. In general, dance-based exercise, as a progressive step marching exercise program, enhances muscle strength by increasing motor unit recruitment and muscle firing rate66,67. This was assumed to increase neural feedback from the cutaneous receptors to the central nervous system and contribute to better postural balance performance68,69. Additionally, the increase in lean mass and strength may improve the functional capacity performance65. With this in mind, the improvements found in lower body strength, walking speed and functional mobility in both Ca + ZT and ZT groups extended the existing knowledge in the literature about Zumba training efficacy on these performances.
The main results of our study indicated that daily caffeine intake promotes Zumba benefits on these functional performances in middle-aged women. In fact, enhancements in these performances were greater in the Ca + ZT group compared to the ZT group. In accordance, a previous study revealed that providing adjunctive ergogenic aids with a range of substances like caffeine is an effective way to enhance exercise performance in older adults30. The optimal performance found in the CZG could be explained by the impact of caffeine on the center nervous system through adenosine inhibition70. Indeed, adenosine increases in muscle and plasma during muscular activity and in the brain during stress, negatively affecting neuron excitability and synapse transmission70. Thus, increased antagonism of adenosine related to caffeine intake may enhance exercise performance71. Furthermore, previous studies investigated the effects of caffeine intake on muscle performance suggested that its ergogenic effect could also be explained by increased sarcoplasmic reticulum calcium ion release and muscle contractility72.
Caffeine intake was also proved to ameliorate cognitive capacities such as attention, memory and executive function73, which are extremely important to execute adequate motor functions74. All these considerations mentioned above may explain additional benefits of caffeine supplementation on functional performances following 12 weeks of Zumba training found in our study on functional performances.
In accordance, our findings indicates that 12-week of daily caffeine consumption was suffusion to also improve functional performances in terms of lower body endurance strength, walking speed and functional mobility. Caffeine may, therefore, considered as seems to be a good alternative or/and complementary component that could be easily recommended for middle-aged women to enhance their functional performances. Caffeine ingestion is widely used within sports and exercise settings for its benefits with evidence suggesting induced increases in endurance, mobility, postural balance, strength, and power activities75,76. Although the efficacy of caffeine ingestion for enhanced exercise performance is well established, most evidence demonstrating caffeine’s ergogenic properties is derived from studies using young or well-trained participants. Thus, our findings are of particular interest because such performance-enhancing benefits in our Ca group indicate that caffeine intake might be one means by which to enhance functional capacities and the ability to undertake activities of daily living.
Nevertheless, the beneficial combined effect compared to solely Zumba training program was not observed in dynamic balance outcomes. According to our results, 12-week of daily caffeine supplementation was not suffusion to significantly improve on dynamic balance in middle-aged women. To our best knowledge, no data revealed such caffeine treatment effects on dynamic balance in middle-aged women. However, it has been reported that 6 mg/kg of caffeine ingestion improved dynamic balance in young adults77. When compared to the present study, beyond differences in gender, age and caffeine dose, these authors measured dynamic postural balance on a moving platform in a unipedal stance. The reasons for the present outcomes with regard to dynamic balance are less clear. Probably, the FRT used in our study, may have more technical components (i.e. ankle motion-range and trunk functions)78,79, that seem to be more difficult to get ameliorated via 100 mg-caffeine supplementation combined with Zumba training. In agreement, it has been proved that, in active men, a high (5 mg/kg) dose of caffeine improve knee function while low dose (2 mg/kg) did not80.
The present study findings are likely to have important practical implications. Indeed, our findings highlight the beneficial effect of Zumba training with or without caffeine supplementation on functional performances including mobility, endurance strength and walking speed in middle-aged women. Given that functional performances are important for preventing falls in middle-aged women81, leading to independence, and therefore good quality of life82, it seems important to consider combining caffeine supplementation with Zumba training while designing intervention strategies for middle-aged women to achieve optimal results. Thus, these women are recommended to daily consume 100 mg of caffeine (equivalent to one cup of instant coffee) and to practice Zumba at a rate of 3 sessions per week during 12-week in order to improve their functional performances during performing daily physical activities, and therefore to achieve healthy aging that promotes enhanced quality of life.
Limits
The present study is not without limitations. First, it would be important to evaluate others functional (fatigue, endurance, static balance…), cognitive (alertness level and vigilance), and psychological (mood, anxiety and depression) parameters in order to have more generative results. Second, further FRT components evaluation (as ankle motion-range and trunk muscles functions) could be included to explain more clearly the results and confirm the hypothesis raised to explain the lake of additional effect of caffeine supplementation on this performance. Finally, since detraining effect may occur a few months after the intervention, it would be interesting to evaluate the protective effect of exercise (3–6 months after the intervention).
Conclusion
The current study showed that 12-week of Zumba training improved functional performances in terms of mobility, lower body endurance strength, dynamic balance and walking speed in middle-aged women, and daily caffeine intake was a good alternative for improving such functional performances, except for dynamic balance. Besides, combining the Zumba training modality and daily caffeine supplementation (100 mg/day) boosts these effects in these women. This highlights the importance of considering such a combination while designing intervention programs as a useful strategy to achieve optimal functional performance and reduce falls risk in middle-aged women.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Monteleone, P. et al. Symptoms of menopause—Global prevalence, physiology and implications. Nat. Rev. Endocrinol. 14 (4), 199–215 (2018).
Aqeel, M., Arbab, K. B. & Akhtar, T. Psychological problems and its association to other symptoms in menopausal transition. Pak. J. Psychol. Res. 33 (2), 507–519 (2018).
Nitz, J., Low, N. & Choy Changes in activity level in women aged 40–80 years. Climacteric. 10 (5), 408–415 (2007).
Nitz, J. C. & Choy, N. L. The relationship between ankle dorsiflexion range, falls and activity level in women aged 40 to 80 years. N. Z. J. Physiother. 32(3). (2004).
Martien, S. et al. Is knee extension strength a better predictor of functional performance than handgrip strength among older adults in three different settings? Arch. Gerontol. Geriatr. 60 (2), 252–258 (2015).
Murray, E. T. et al. Gender and life course occupational social class differences in trajectories of functional limitations in midlife: Findings from the 1946 British birth cohort. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 66 (12), 1350–1359 (2011).
Li, W. et al. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am. J. Public Health. 96 (7), 1192–1200 (2006).
Waer, F. B. et al. Functional and cognitive responses to caffeine intake in middle-aged women are dose depending. Behav. Brain Res. 397, 112956 (2021).
Han, Y. O. & Lee, B. S. Development of physical activity competence test battery and evaluation standards for Korean Children. Children. 9 (1), 79 (2022).
Lemmink, K. A. et al. Reliability of the Groningen fitness test for the elderly. J. Aging Phys. Act. 9 (2), 194–212 (2001).
Jones, C. J. & Rikli, R. E. Measuring functional. J. Act. Aging. 1, 24–30 (2002).
Ruiz, J. R. et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 45 (6), 518–524 (2011).
Ben Waer, F. et al. The effects of Pilates vs. Zumba dancing on functional performance, mood and health-related quality of life in Postmenopausal women. Appl. Sci. 14 (7), 2886 (2024).
Straight, C. R., Ward-Ritacco, C. L. & Evans, E. M. Association between accelerometer-measured physical activity and muscle capacity in middle-aged postmenopausal women. Menopause. 22 (11), 1204–1211 (2015).
Kaushal, N. et al. Investigating dose–response effects of multimodal exercise programs on health-related quality of life in older adults. Clin. Interv. Aging, 209–217. (2019).
Nelson, M. E., King, A. C., Castaneda-Sceppa, C. et al. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 39(8), 1435–1445. (2007).
Manaf, H. Barriers to participation in physical activity and exercise among middle-aged and elderly individuals. Singap. Med. J. 54 (10), 581–586 (2013).
Kim, M. J. et al. Association between physical activity and menopausal symptoms in perimenopausal women. BMC Women’s Health. 14, 1–8 (2014).
Karine, D. et al. Effects of the menopausal transition on factors related to energy balance. A MONET group study: I. Energy expenditure. Eur. J. Clin. Nutr. 67 (4), 407 (2013).
Lovejoy, J. C. et al. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int. J. Obes. 32 (6), 949–958 (2008).
Scheers, T., Philippaerts, R. & Lefevre, J. Compliance with different physical activity recommendations and its association with socio-demographic characteristics using an objective measure. BMC Public Health. 13, 1–10 (2013).
Thompson, W. R. Now trending: Worldwide survey of fitness trends for 2014. ACSM’s Health Fit. J. 17 (6), 10–20 (2013).
Blackler, A. et al. Using technology to enhance and encourage dance-based exercise. Heliyon, 5(3). (2019).
Luettgen, M. et al. ZUMBA®: Is the fitness-party a good workout? J. Sports Sci. Med. 11 (2), 357 (2012).
Arol, P. The effect of Zumba exercises on body composition, dynamic balance and functional fitness parameters in 15–17 years old women with high body mass index. Pedagogy Phys. Cult. Sports 24(3). (2020).
Donath, L. et al. The effects of Zumba training on cardiovascular and neuromuscular function in female college students. Eur. J. Sport Sci. 14 (6), 569–577 (2014).
Oktay, G. Investigation of effects of 8 weeks zumba exercise of women on health related physical fitness factors. Eur. J. Phys. Educ. Sport Sci. (2018).
Barene, S. et al. Effects on muscle strength, maximal jump height, flexibility and postural sway after soccer and Zumba exercise among female hospital employees: A 9-month randomised controlled trial. J. Sports Sci. 34 (19), 1849–1858 (2016).
Lahiani, M. et al. Effect of 12-week-zumba training on postural balance, lower limb strength, mood and quality of life in postmenopausal women. Exp. Aging Res. 1–19 (2023).
Cherniack, E. P. Ergogenic dietary aids for the elderly. Nutrition. 28 (3), 225–229 (2012).
Davis, J. M. et al. Central nervous system effects of caffeine and adenosine on fatigue Am. J. Physiol. Regul. Integr. Comp. Physiol., 2003).
Bazzucchi, I. et al. Caffeine improves neuromuscular function during maximal dynamic exercise. Muscle Nerve. 43 (6), 839–844 (2011).
Souza, D. B. et al. Acute effects of caffeine-containing energy drinks on physical performance: A systematic review and meta-analysis. Eur. J. Nutr. 56, 13–27 (2017).
Grgic, J. et al. Wake up and smell the coffee: Caffeine supplementation and exercise performance—An umbrella review of 21 published meta-analyses. Br. J. Sports Med. 54 (11), 681–688 (2020).
Khcharem, A., Masmoudi, L. & Sahnoun, Z. A single dose of Caffeine Ingestion improves physical and cognitive performance during a 1500-M Run Competition. Health Nexus. 2 (1), 29–34 (2024).
Robillard, R. et al. Sleep is more sensitive to high doses of caffeine in the middle years of life. J. Psychopharmacol. 29 (6), 688–697 (2015).
Ben Waer, F. et al. Acute effects of low versus high caffeine dose consumption on postural balance in middle-aged women. J. Women Aging, 1–15 (2020).
Laatar, R. et al. Caffeine consumption improves motor and cognitive performances during dual tasking in middle-aged women. Behav. Brain Res. 412, 113437 (2021).
Faul, F. et al. G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods. 39 (2), 175–191 (2007).
Ben Waer, F. et al. Effects of 12 weeks of caffeine supplementation and Zumba training on postural balance and cognitive performances in middle-aged women. Health Care Women Int.. 1–21 (2023).
Stokes, J. Medical history questionnaire. (1997).
Irons, J. G. et al. Development and initial validation of the caffeine consumption questionnaire-revised. J. Caffeine Res. 6 (1), 20–25 (2016).
Craig, C. et al. International physical activity questionnaire-short form. J. Am. Coll. Health. 65 (7), 492–501 (2017).
Rubenstein, L. Z. et al. Validating an evidence-based, self-rated fall risk questionnaire (FRQ) for older adults. J. Saf. Res. 42 (6), 493–499 (2011).
Hunter, M. The women’s Health Questionnaire (WHQ): The development, standardization and application of a measure of mid-aged women’s emotional and physical health. Qual. Life Res. 9, 733–738 (2000).
Grigoletto, F. et al. Norms for the Mini-mental State examination in a healthy population. Neurology. 53 (2), 315–315 (1999).
Tanaka, H., Monahan, K. D. & Seals, D. R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 37 (1), 153–156 (2001).
Garber, C. E. et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports. Exerc. 43 (7), 1334–1359 (2011).
Ritchie, C. et al. Reliability and validity of physical fitness field tests for adults aged 55 to 70 years. J. Sci. Med. Sport. 8 (1), 61–70 (2005).
Kostic, R. et al. Effects of dance training programme on postural stability of middle aged women. Cent. Eur. J. Public Health. 23, S67 (2015).
Chen, H. Y. & Tang, P. F. Factors contributing to single-and dual-task timed up & go test performance in middle-aged and older adults who are active and dwell in the community. Phys. Ther. 96 (3), 284–292 (2016).
Koley, A. & Bandyopadhyay, N. Construction of a physical fitness test battery for middle-aged women. Int. J. Disabil. Sports Health Sci. 7 (1), 51–65 .
Jones, C. J., Rikli, R. E. & Beam, W. C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport. 70 (2), 113–119 (1999).
Cuenca-Garcia, M. et al. Reliability of field-based fitness tests in adults: A systematic review. Sports Med. 52 (8), 1961–1979 (2022).
Kahraman, T. et al. Assessment of sit-to-stand movement in nonspecific low back pain: A comparison study for psychometric properties of field-based and laboratory-based methods. Int. J. Rehabil. Res. 39 (2), 165–170 (2016).
McGinn, A. P. et al. Walking speed and risk of incident ischemic stroke among postmenopausal women. Stroke. 39 (4), 1233–1239 (2008).
de Oliveira Júnior, G. N. et al. Prime: Evidence-based proposal for a New Predictor of Gait Speed in Older Women. Muscles. 2 (3), 286–298 (2023).
Isles, R. C. et al. Normal values of balance tests in women aged 20–80. J. Am. Geriatr. Soc. 52 (8), 1367–1372 (2004).
Wu, F. et al. Cut-points for associations between vitamin D status and multiple musculoskeletal outcomes in middle-aged women. Osteoporos. Int. 28, 505–515 (2017).
Duncan, P. W. et al. Functional reach: A new clinical measure of balance. J. Gerontol. 45 (6), M192–M197 (1990).
Steiger, J. H. Beyond the F test: Effect size confidence intervals and tests of close fit in the analysis of variance and contrast analysis. Psychol. Methods. 9 (2), 164 (2004).
ÇAĞLAR, E. Ç. An investigation of dance based aquatic and Zumba exercise in sedentary women according to motoric and physiological parameters. Educ. Youth Res. 2 (2), 48–58 (2022).
Perez, B. & Greenwood-Robinson, M. Zumba: Ditch the Workout, join the Party! The Zumba Weight loss Program (Grand Central Life & Style, 2014).
Furjan-Mandić, G., Kosalec, V. & Vlašić, J. The effects of aerobic exercise on the increase of repetitive strength in women. In 3th International aspects of Sports, Physical education and Recreation, 75–83 (2011).
Najafnia, Y. et al. Effects of 8-week step aerobic exercise on women’s physiological characteristics, body fat percentage, and quality of life. Int. J. Sport Stud. 3 (12), 1335–1341 (2013).
Suchomel, T. J. et al. The importance of muscular strength: Training considerations. Sports Med. 48 (4), 765–785 (2018).
Mayer, F. et al. The intensity and effects of strength training in the elderly. Deutsches Ärzteblatt International 108 (21), 359 (2011).
Horak, F. B., Henry, S. M. & Shumway-Cook, A. Postural perturbations: New insights for treatment of balance disorders. Phys. Ther. 77 (5), 517–533 (1997).
Qiu, F. et al. Enhanced somatosensory information decreases postural sway in older people. Gait Posture. 35 (4), 630–635 (2012).
Keisler, B. D. & Armsey, T. D. Caffeine as an ergogenic aid. Curr. Sports Med. Rep. 5 (4), 215–219 (2006).
Duncan, M. et al. The effect of acute caffeine ingestion on coincidence anticipation timing in younger and older adults. Nutr. Neurosci. 17 (5), 234–238 (2014).
Giráldez-Costas, V. et al. The long way to establish the ergogenic effect of caffeine on strength performance: An overview review. Nutrients. 15 (5), 1178 (2023).
Smit, H. & Rogers, P. Effects of low doses of caffeine on cognitive performance, mood and thirst in low and higher caffeine consumers. Psychopharmacology. 152 (2), 167–173 (2000).
Yogev-Seligmann, G., Hausdorff, J. M. & Giladi, N. The role of executive function and attention in gait. Mov. Disord. Off. J. Mov. Disord. Soc. 23 (3), 329–342 (2008).
Graham, T. E. Caffeine and exercise: Metabolism, endurance and performance. Sports Med. 31, 785–807 (2001).
Duncan, M. J. et al. The effect of caffeine ingestion on functional performance in older adults. J. Nutr. Health Aging. 18, 883–887 (2014).
Kara, M. et al. Effect of caffeine on standing balance during perceptual-cognitive tasks. MoHE. 7, 167–175 (2018).
Jorrakate, C. et al. Effect of yoga training on one leg standing and functional reach tests in obese individuals with poor postural control. J. Phys. Ther. Sci. 27 (1), 59–62 (2015).
Demura, S. & Yamada, T. Simple and easy assessment of falling risk in the elderly by functional reach test using elastic stick. Tohoku J. Exp. Med. 213 (2), 105–111 (2007).
Astorino, T. A. et al. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med. Sci. Sports. Exerc. 42 (12), 2205–2210 (2010).
Ferguson, B. ACSM’s guidelines for exercise testing and prescription 9th Ed. 2014. J. Can. Chiropr. Assoc. 58 (3), 328 (2014).
Roe, B. et al. Older people’s experience of falls: Understanding, interpretation and autonomy. J. Adv. Nurs. 63 (6), 586–596 (2008).
Acknowledgements
A great thank for all collaborating and volunteers for their availability and contribution in this study. Cristina Ioana Alexe and Dan Iulian Alexe thanks for the support and assistance provided by the “Vasile Alecsandri” University of Bacău, Romania.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
FW, DIA and CIA: conceptualization. FW, CIA and RL: methodology. FW, DB, AMA and CIA: software. FW, DIA, FC, CIA, RL, DB, AMA, AL, and SS: validation. FW and FC formal analysis. FW, DIA and HR: investigation. FW, AL, CIA, DB and DIA: resources. FW: data curation. FW, DIA, and FC: writing—original draft preparation. FW, DIA, RL, CIA, FC, AMA, SS, HR, DB and AL: writing—review and editing. FW, AMA, AL and RL: visualization. FW, SS, CIA, HR and DIA: supervision. FW, HR, SS, and DIA: project administration. DIA, CIA, AMA, DB, and AL: funding acquisition. All authors contributed to the article, all authors reviewed the manuscript and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the VASILE ALECSANDRI UNIVERSITY of BACĂU (NR#23219/2/14.12.2023). The participants provided their written informed consent to participate in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Waer, F.B., Alexe, D.I., Chaari, F. et al. Caffeine optimizes Zumba training benefits on functional performances in middle-aged women: a randomized trial study. Sci Rep 14, 25657 (2024). https://doi.org/10.1038/s41598-024-76650-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76650-0
