
Abstract
In PDAC patients, ctDNA detection’s prognostic significance needs validation especially in resected patients. This study investigated ctDNA kinetics in portal and peripheral blood before and after resection, and whether tissue mobilization during surgery influences ctDNA detection. In this single-center prospective cohort, portal and peripheral blood were drawn during pancreaticoduodenectomy before and after tissue mobilization, during 12 postoperative months and were associated with overall survival (OS), recurrence-free survival (RFS) and CA19-9 (secondary endpoints). Tumor mutations were identified using next-generation-sequencing and ctDNA detected by digital droplet PCR. From 2018 to 2022, 34 patients were included. The 2-year RFS and OS were 47.6%(95%CI[29.5; 63.6]) and 65.7%(95%CI[46.5; 79.4]) respectively. Intraoperatively, ctDNA detection in portal or peripheral blood was associated with worse RFS (HR[95%CI]3.26[1.26; 8.45],p = 0.010) and OS (HR[95%CI]5.46[1.65;18.01],p = 0.002). Portal vein sampling did not improve ctDNA detection. CtDNA levels were increased by 2.5-fold (p = 0.031) in peripheral blood after tissue mobilization but not significantly linked to RFS or OS. Detecting ctDNA intraoperatively was correlated with poorer RFS (HR [95% CI] 3.26 [1.26;8.45], p = 0.010) and 0S (HR [95% CI] 5.46 [1.65;18.01], p = 0.002). Portal vein sampling did not improve ctDNA detection. Tissue mobilization increases ctDNA levels. Intraoperative detection of ctDNA is associated with a worse prognosis.
Similar content being viewed by others

Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a major public health challenge due to its rising incidence and mortality rates. With an annual increase of approximately 1% in incidence, PDAC has become the third leading cause of cancer death in Western countries. The overall 5-year survival rate for all stages combined is a mere 12%, and PDAC is projected to become the second leading cause of cancer-related deaths by 20301,2. Surgical resection remains the only curative treatment for PDAC, but it is feasible in only 10 to 20% of cases due to the often late presentation of symptoms3. Despite recent advancements in onco-surgical approaches, which integrate systemic therapies with various chemotherapeutic protocols, including neoadjuvant treatments, survival rates remain low. The median 5-year survival rate for resected patients is only 20 to 30%, and the 3-year recurrence-free survival rate is less than 40% for those treated with adjuvant mFOLFIRINOX4. The high incidence of occult metastases in patients considered resectable at diagnosis underscores the need for more accurate detection of minimal residual disease and the development of clinically relevant biomarkers to improve early diagnosis, prognosis assessment, tumor progression monitoring, and treatment response evaluation5.
Currently, CA 19–9 (Carbohydrate Antigen 19.9) is the only recommended routine biomarker for PDAC patients. Upon diagnosis, CA 19–9 demonstrates a sensitivity of 79% and a specificity of 82%, though its specificity can be compromised by false positives, particularly in the presence of obstructive jaundice, where can range from 10 to 60%6,7. Current guidelines suggest that patients with elevated CA 19–9 levels above 500 U/L at diagnosis should receive neoadjuvant treatment8. However, CA19-9 has significant limitations, including its limited ability to predict tumor progression or recurrence, and a high rate of false positives, particularly in patients with benign pancreaticobiliary conditions9,10and those with Lewis antigen deficiencies11. These limitations highlight the urgent need for more robust and reliable biomarkers. Consequently, further research is essential to identify and validate alternative biomarkers and diagnostic tools that can provide a more precise and comprehensive assessment of PDAC, ultimately improving patient outcomes and treatment strategies.
One promising approach for non-invasive biomarker discovery is liquid biopsy, particularly the analysis of circulating tumor DNA (ctDNA)12. This approach offers potential applications in early diagnosis, disease prognosis, and treatment monitoring12,13,14. First described in 194815, cell-free DNA is shed into the bloodstream from apoptotic or necrotic tumor cells16. ctDNA can be distinguished from normal circulating DNA by detecting specific oncogenic mutations indicative of the originating tumor, using highly sensitive and specific techniques such as digital droplet PCR (ddPCR)17,18,19. KRAS mutations are the most common alterations found in PDAC, present in approximately 90% of patients, particularly in codons 12 and 6120,21, which are associated with poorer prognosis22. Previous studies from our group have shown that combining KRAS mutation analysis with endoscopic ultrasonography-guided cytopathology improves diagnostic accuracy compared to cytopathology alone22,23. Additionally, recent research has demonstrated the prognostic significance of detecting KRAS mutations from ctDNA, especially in metastatic PDAC24,25,26,27. However, further validation is needed to establish the clinical relevance of ctDNA detection in both initial diagnosis and follow-up, particularly in resectable patients with lower tumor burdens28,29. Additionally, the impact of tumor manipulation during surgery, such as the “no-touch” technique used in other cancers to prevent tumor cell dissemination30,31, on ctDNA detection has not been thoroughly investigated in PDAC surgeries.
This study aims to explore, in a prospective cohort of patients receiving surgery for PDAC, the prognostic impact of ctDNA detection in both peripheral and portal blood before and after PDAC resection. We also assess whether tissue mobilization during surgery affects ctDNA levels in these blood compartments.
Results
Patient characteristics
A total of 57 patients underwent pancreaticoduodenectomy due to suspicion of resectable PDAC from February 2018 to June 2022 at Toulouse University Hospital and were screened for enrolment in this study. Ten patients were excluded because resection surgery could not be performed (exploratory laparotomy), 1 patient was excluded because their surgery was changed to distal pancreatectomy, 11 patients were removed as the histopathological analysis revealed a different type of tumor than PDAC and 1 patient died within the first month after surgery and had incomplete post-operative serum samples. Finally, the remaining 34 patients were enrolled in the study. The study flow-chart is presented in Fig. 1.

Study flow chart. PDAC: Pancreatic Ductal Adenocarcinoma.
Preoperative and intraoperative characteristics of the study population are detailed in Table 1. Discovery of the tumor occurred in 50.0% (n = 17) of patients following the onset of jaundice. Most patients (76.5%, n = 26) underwent a preoperative endoscopic ultrasound and diagnosis of pancreatic adenocarcinoma was made preoperatively in 35.3% (n = 12) of patients.
Post-operative characteristics of the population are listed in Table 2. On histopathological analysis, most of patients had lymph node metastasis (73.5%, n = 25), perineural infiltration (69.7%, n = 23) and R0 resection (85.3%, n = 29). The majority of patients had POD 90 medical (67.6%, n = 23) and surgical (58.8%, n = 20) complications, with a POD 90 median CCI of 29.0 (0.0; 92.6). A total of 20.6% (n = 7) of patients experienced major post-operative complications (Clavien-Dindo score ≥ 3).
Mutational status of the primary tumor
Analysis of the primary tumor mutations performed on the surgical specimen using NGS is set out in Fig. 2. KRAS and TP53 mutations were identified in 88.2% (30/34) and 79.4% (27/34) of the patients respectively. Five patients (14.7%) exhibited 4 or more mutations in the primary tumor. Primary tumor KRAS status was G12V in 26.5% (9/34), G12D in 35.3% (12/34) G12R in 20.6% (7/34), Q61H in 5.9% (2/34) and Q16R in 2.9% (1/34) patients. One patient (2.9%) had two KRAS mutations within their primary tumor: G12R and G12D.

Primary tumor mutations performed on the surgical specimen using next-generation-sequencing. KRAS mutations and codons are in red and other mutations are in black.
Recurrence-free survival and overall survival
After a median follow-up of 32.7 months (95% CI [23.4; 38.9]), disease recurrence was observed in 20 (58.8%) patients and 13 (38.2%) patients had died (Table 3). The median survival after recurrence (among the 20 patients who experienced a recurrence) is 7.5 months (95% CI = [2.0; 10.4]). All deceased patients in the study had PDAC recurrence. The median RFS was 20.7 months (95% CI [8.4; 37.5]) although median OS was not reached. The 2-year RFS and OS were 47.6% (95% CI [29.5; 63.6]) and 65.7% (95% CI [46.5; 79.4]) respectively.
PreoperativeCA 19–9
CA 19–9 rates were measured at each timepoint and are listed in Supplementary data - Table 1. The level of CA 19–9 before surgery was significantly associated with poorer RFS (HR [95% CI] 1.01 [1.00; 1.02], p = 0.007) and OS (HR [95% CI] 1.02 [1.01; 1.03], p = 0.002).
Analysis of intraoperative levels of cfDNA and ctDNA
Intraoperative mobilization of the tumor led to a significant increase in mean cfDNA levels by 2.74-fold in peripheral blood before mobilization (2864 ± 2600 copies/mL) versus after mobilization (7866 ± 5148 copies/ml, p < 0.0001, Fig. 3A).

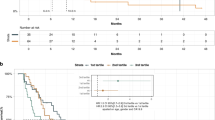
Intraoperative data. Comparison of (A) peripheral and (B) portal cfDNA (copies/mL, mean, SD) and ctDNA (copies/mL, mean, SD) levels before and after tissue mobilization. (C) KRAS mutation detection in tumor specimen (“Tumor”) and in peripheral and/or portal vein, before and/or after tissue mobilization during surgery (“Peroperative ctDNA”). Recurrence-free survival (D) and Overall survival (E) according to evolution of ctDNA after mobilization comparing to before tissue mobilization. **** p < 0.0001, ** p < 0.01, * p < 0.05. ctDNA: Circulating tumor DNA, cfDNA: Circulating-Free DNA, NS: not significant, SD: Standard deviation.
We measured a similar increase (1.66-fold) in the level of mean cfDNA in portal blood after mobilization of the tumor (8060 ± 5650 copies/mL) versus pre-mobilization (4864 ± 3728 copies/mL, p = 0.005, Fig. 3B). Additionally, we measured a significant difference in mean cfDNA levels in blood from the portal vein as compared to peripheral blood before tissue mobilization (1.64-fold increase, p = 0.03).
Statistical analysis was conducted to study the effect of cfDNA levels on survival rates. The univariate analysis did not reveal that the perioperative cfDNA rate had any significant impact on RFS or OS (Supplementary data—Table 1).
We also analyzed KRAS mutations to address the presence of ctDNA in these samples. Fourteen patients out of 34 (41.2%) showed positivity for intraoperative ctDNA, regardless of the sampling site before or after mobilization. Four patients (11.8%) and 11 patients (32.4%) tested positive on peripheral blood samples before and after tissue mobilization respectively. Four patients (12.1%, one missing data) and 6 patients (17.6%) tested positive on portal blood before and after tissue mobilization respectively.
Among the 14 patients who showed positivity for intraoperative ctDNA, we found no increase in ctDNA levels in the portal blood following tissue mobilization. On the contrary, ctDNA levels were significantly increased by 2.5-fold (1.4 ± 2.5 vs 3.4 ± 2.1, p = 0.031, Fig. 3A) in peripheral blood after mobilization.
Furthermore, 13 patients out 14 (92.9%) with positive intraoperative ctDNA exhibited KRAS mutation in the tumor specimen (Fig. 3C). One patient whose tumor was negative for KRAS mutation in their tumor specimen revealed positivity of ctDNA in peripheral blood after mobilization.
Statistical analysis was performed to study the impact of ctDNA levels on survival rates. The univariate analysis (Table 3) revealed that intraoperative detection of ctDNA in portal or peripheral blood was significantly correlated with worse RFS (HR [95% CI] 3.26 [1.26; 8.45], p = 0.010) and OS (HR [95% CI] 5.46 [1.65; 18.01], p = 0.002) even if the presence of ctDNA was only detected in portal or peripheral blood after mobilization of the tumor: RFS (HR [95% CI] 2.77 [1.07; 7.14], p = 0.028) and OS (HR [95% CI] 4.24 [1.37; 13.16], p = 0.007).

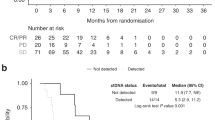
Postoperative data. (A) CtDNA detection and levels and recurrence. (B) Ca 19–9 levels and recurrence. (C) Examples of ctDNA detection and recurrence. BS: Before surgery, BEFORE-P: Peripheral blood before tissue mobilization, AFTER-P: Peripheral blood after tissue mobilization, BEFORE-PV: Portal blood before tissue mobilization, AFTER-PV: Portal blood after tissue mobilization, POD: Postoperative day, POM: Postoperative month. Arrows indicate clinical recurrence.
The increase in ctDNA detection after tissue mobilization was not significantly correlated with RFS (HR [95% CI] 1.79 [0.69; 4.68], p = 0.225) (Fig. 3D) or OS (HR [95% CI] 2.43 [0.81; 7.28], p = 0.101) (Fig. 3E).
Analysis of Ca-19.9, cfDNA and ctDNA during post-operative follow-up
Samples of peripheral venous blood were collected post-operatively at POD 1, 10, POM 1, 3, 6 and 12. In case of recurrence within the 12 post-operative months, a consultation was conducted, and a final peripheral venous blood sample was taken.
Detection of CA 19–9 during the immediate post-operative period was predictive of recurrence at POD 1 (HR [95% CI] 1.02 [1.01; 1.04], p = 0.010) and OS at POD 1 (HR [95% CI] 1.03 [1.01; 1.05], p = 0.002) and POD 10 (HR [95% CI] 1.07 [1.01; 1.13], p = 0.012) (Supplementary data—Table 1).
The univariate analysis did not reveal that cfDNA level had any significant impact on RFS or OS during the post-operative period (Supplementary data—Table 1).
Patient follow-up with ctDNA detection and levels, if applicable, is detailed for each patient in Fig. 4A. Ca 19–9 levels are detailed for each patient in Fig. 4B. Detection of ctDNA during the immediate post-operative period (POD 1 and/or POD 10) almost corresponded to significant correlation with worse RFS (HR [95% CI] 2.39 [0.96; 5.98], p = 0.054) but not to OS (HR [95% CI] 1.21 [0.37; 3.95], p = 0.752) (Table 3).
As an example, patient 18 had positive ctDNA detected in their intraoperative samples (peripheral and portal blood) and 4 post-operative positive samples during the follow-up period: POD 1, POM 3, POM 6 and POM 12 which was the date of recurrence detection (POM 12). All the samples for patient 29 were positive for ctDNA detection except for POD 1, with recurrence diagnosed at POM 6. In both patients, CA-19.9 levels showed a similar trend (Fig. 4C).
Discussion
The presence of ctDNA in advanced PDAC patients with high tumor burden is widely acknowledged thanks to KRAS mutation detection in peripheral blood and exhibits clinical value24,29,32,33,35,36,36. Moreover, the dynamic changes of ctDNA levels in response to treatment have an even stronger impact28,37,38. However, the use of KRAS mutation detection for the management of localized PDAC is still debated, even though it is most needed for early diagnosis or recurrence detection. This study investigated the use of ctDNA as a non-invasive biomarker in resectable PDAC patients, specifically focusing on its prognostic impact after sampling both peripheral and portal venous blood. Various authors have investigated ctDNA in patients with resectable PDAC although the populations were predominantly heterogeneous: some patients received neoadjuvant treatment before surgery, some authors included PDAC from all stages and in some studies, patient follow-up was limited to the immediate post-operative period9,19,24,28,39,40,41,42,42.
To overcome these limitations, we have presented a cohort which included a homogeneous and representative population of resectable PDAC patients with long-term follow-up in order to increase the clinical importance of the study. This work aims to explore whether sampling from the portal vein improves the detection of ctDNA compared to peripheral blood sampling and whether tissue mobilization during surgery influences ctDNA levels.
When we examined the profile of mutations found in the surgery specimens using NGS detection, we identified the same mutational profile as reported in the literature for larger cohorts. Indeed, KRAS mutation was identified in more than 90% of PDAC and loss of tumor suppressor genes such as TP53, SMAD4 and CDKN2A is also frequently observed43,44.
We faced a discordance in one patient whose tumor was negative for KRAS mutation but who showed positivity in ctDNA sampled from peripheral blood after mobilization. This finding may be due to differences in sensitivity for KRASmutation detection between ddPCR (down to 0.001%) and NGS (2 to 3%)45,46. Furthermore, PDAC has the particularity of being a highly heterogeneous tumor, either between patients or even within the same tumor sample47. Heterogeneity can manifest at various levels, whether at the genetic, epigenetic or cellular and tumor microenvironment levels47. As the NGS analysis of the surgical specimen was only performed on an area of the tumor, KRAS mutation could have been “missed” during the process due to tumor heterogeneity.
We confirmed that Ca 19–9 detection has no prognostic value during follow-up for early prediction of recurrence, in accordance with the literature48,49. In addition, we further demonstrate that perioperative elevation of CA 19–9 is prognostic of recurrence, as described before28. Collectively, these molecular investigations validate the clinical representativity of the cohort.
This study illustrates that detection of cfDNA is improved when sampling is performed in the portal vein compared to the peripheral vein which is consistent with findings from the study by Nitschke et al., the only study to date in the literature to evaluate peripheral and portal cfDNA and ctDNA detection19. Some authors have described that the carcinogenic process can be impacted by cfDNA-induced inflammation which is attributable to the ability of cfDNA to cause inflammatory responses50. In our study, cfDNA increases had no impact on RFS or OS. However, despite increased detection of cfDNA in the portal vein, such a sampling strategy does not appear to improve the sensitivity of ctDNA detection. Our research does therefore not support findings that hepatic filtration plays a major role in decreasing accessibility of ctDNA and shows no apparent benefit in performing EUS-guided sampling of the portal vein for ctDNA detection as suggested by some authors19.
The results of this study show that when ctDNA is detected in the portal or peripheral vein before or after tissue mobilization, the prognosis for RFS and OS is worse. Furthermore, tissue mobilization significantly increases the level of ctDNA in peripheral blood and its detection is correlated with poorer RFS and OS. Considering these results, it would be of interest to address ctDNA levels in a “no-touch” technique such as a pancreaticoduodenectomy with resection performed “from back to front” using superior mesenteric artery first approach. This approach allows for the vessels to be sectioned off before the pancreatic section51.
In the literature, ctDNA detection during the immediate postoperative period has been associated with a high rate of recurrence and poor median RFS28. However, this study did not reveal such associations (neither considering POD1 nor POD10), likely due to the limited statistical power resulting from the small sample size. CtDNA persistence or detection during the immediate post-operative period has the potential to help clinicians identify high-risk patients and initiate early intervention for recurrence19,24,28,29,38. However, clinical relevance regarding the presence of ctDNA after tumor resection is limited since there is presently no different treatment based on the prognosis of patients after surgery: the current standard treatment is adjuvant mFOLFIRINOX for all resected PDAC patients4 but it may help in future with the development of novel therapeutic strategies.
Previous studies have shown that detection of preoperative ctDNA or during follow-up is related to poor prognosis19,24,28,29,38,41,52,53,54,54. In our study, the presence of ctDNA pre-surgery (before tissue mobilization) could not be analyzed due to limited numbers of events. However, when the results of ctDNA detection before and after tissue mobilization were pooled, regardless of the sampling method, a significant impact on RFS and OS was notably observed. We did not identify an effect on survival from preoperative ctDNA detection or during long-term follow-up (after POM 1); this again, would be likely due to the small sample size.
Moreover, detecting ctDNA in resectable patients is believed to be challenging as a result of low tumor burden and an early cancer stage12,13,14, both factors which must have affected ctDNA detection in this study. Nevertheless, ctDNA was detected before recurrence in two patients highlighted as examples, indicating that this biomarker could be useful during follow-up.
This study presents us with a prospective cohort of resectable patients, but biases should be noted since it is monocentric and because of limited statistical power due to the small sample size. Even so, the statistically significant outcomes from our pilot study are supported by recent works where intraoperative ctDNA was correlated with poor prognosis19,24,28,29,38. Moreover, the recruitment of these patients who underwent upfront pancreaticoduodenectomy took a long time (4 years). This extended inclusion period was due, on the one hand, to the strict selection of patients who had a resectable pancreatic head adenocarcinoma from the outset, and on the other hand, to the changes in the management of these patients, with an increase in the administration of neoadjuvant chemotherapy during this period when the CA 19–9 level was high or when there was venous tumor contact8,55,56,57,57. Also, the detection rate in our study might have been higher if cfDNA had been extracted from a larger quantity of blood, and if the inclusion time had been shorter, which would have reduced the storage time of the samples28. However, this study is the first, to our knowledge, to address the impact of tissue mobilization on ctDNA detection.
This study proposes the need for multicenter clinical trials to validate the relevance of liquid biopsy in the management of resectable PDAC. The development of alternative tools and detection methods is widely discussed in the literature. KRASmutations, identified in more than 90% of PDAC, are a prime target for liquid biopsy in pancreatic cancer. However, it may also require to develop more sensitive assays or increase the amount of cfDNA input, particularly in localized PDAC. Authors have developed multi-analyte approaches which show promise58,59,60,60. Exploring other markers on circulating DNA (i.e., methylation61or fragmentation62 is progressive for ctDNA detection. In addition, recent studies have identified exosomes (small extracellular vesicles produced by cancer calls) as a significant source of mutant KRAS DNA in the plasma of PDAC patients. They have also demonstrated the potential of exosome detection in the blood which could be a promising alternative to detect ctDNA and KRASmutation by ddPCR63,64,65,65. However, the cost and clinical feasibility of these alternative strategies must also be considered.
In conclusion, this prospective study provides valuable insights into the prognostic significance of ctDNA in PDAC patients undergoing surgical resection, especially when ctDNA is detected during the intraoperative period. We found that portal vein sampling has no effect on ctDNA detection compared to peripheral blood collection. Furthermore, this study raises important considerations for the first time about the impact of surgical manipulation on ctDNA release. As detection of ctDNA in resectable patients is still challenging due to the presumably low tumor burden, it is therefore necessary to develop new assays addressing multiple biomarkers to further explore the clinical role of liquid biopsy-guided diagnosis and management of PDAC patients.
Material and methods
Study design and population
This was a single-center prospective explorative cohort study carried out from February 2018 to June 2022 at Toulouse University Hospital. The Nord-Ouest I (Northwest I) Ethics Committee approved the study on January 2018 (No. 006/2018) which complied with Good Clinical Practices and the Declaration of Helsinki. Informed consent was obtained for all included patients. This study was supported by a grant from the Toulouse University Hospital, local grant 2017, no. RC31/17/0327 and was registered on 19/02/2018 on the ClinicalTrials.gov website under the reference NCT03435536.
The eligibility criteria are summarized in Table 4.
During the surgery, the first portal blood sample was taken before any tissue mobilization took place and a second sample portal blood was drawn at the end of the pancreaticoduodenectomy. These two portal blood specimens were accompanied by two peripheral blood samples at the same stage of the procedure. Six samples of peripheral venous blood were subsequently collected post-operatively at post-operative day (POD) 1, 10, post-operative month (POM) 1, 3, 6 and 12. In case of recurrence within the 12 post-operative months detected outside of the scheduled follow-up consultations (POM 1, POM 3, POM 6 and POM 12), a consultation was conducted to confirm the recurrence and a final peripheral venous blood sample was gathered.
Pancreaticoduodenectomy (PD)
All patients underwent PD with dissection which removed the head of the pancreas in one piece, the duodenal frame with the antropyloric region and the distal main bile duct. Pancreatic anastomosis included pancreatico-jejunal (PJ) anastomoses with Child’s type reconstruction and pancreatic-gastric anastomoses with or without a trans-anastomotic stent. The resection was performed “from front to back” which is the most commonly used method since it allows for improved exposure as anatomical structures are sectioned, leaving the more delicate part, the segment of the retroportal lamina at the right edge of the superior mesenteric artery (SMA), to be completed last.
Study endpoints
The ctDNA levels were compared in both portal and peripheral blood before and after resection of PDAC (primary endpoint) and associated with overall survival (OS), recurrence-free survival (RFS) and CA 19–9 (secondary endpoints). RFS was defined as the time between the date of surgery and the date of recurrence or death from any cause. Patients alive and recurrence-free were censored at last follow-up. Recurrence was diagnosed for each patient based on a combination of biological, radiological and clinical criteria during a multidisciplinary meeting involving at least three experts from four specialties: radiology, gastroenterology, digestive surgery and digestive oncology. The experts were blinded for ctDNA levels. OS was defined as the time between the date of surgery and the date of death from any cause. Patients alive were censored at last follow-up.
Definitions
CtDNA was defined as cell-free DNA with KRASalterations. Post-operative pancreatic fistula (POPF) and its severity stages were defined by the 2016 ISGPS grading system66. Post-operative morbidity was staged according to the Clavien-Dindo score67and the Comprehensive Complication Index (CCI)68 at post-operative day 90 (POD 90). The POD 90 CCI was performed for each patient using an online calculator (https://www.cci-calculator.com/cciCalculator). Major post-operative complications were defined by a Clavien-Dindo score ≥ 3.
Blood collection and processing
At each timepoint, 16 mL of portal or peripheral blood was collected in 8 mL PAXgene tubes (PreAnalitiX™ A QIAGEN/BD Company, Hombrechtikon, Switzerland) and were processed immediately 24 h after blood collection. To separate plasma from peripheral blood cells, samples were centrifuged for 10 min at 1,200 g at 4 °C. A second centrifugation was performed for 10 min at 16,000 g at 4 °C. All isolated plasmas were aliquoted and stored at − 80 °C for later use.
Cell-free DNA (cfDNA) extraction
DNA extraction and analysis for ctDNA detection were conducted as a whole batch at the end of the study. CfDNA was purified from 2 mL of plasma. The extraction was performed manually with QIAamp Circulating Nucleic Acid kit (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. Circulating-free circulating DNA was stored at − 20 °C.
Next-generation sequencing (NGS) of primary tumor
Analysis of the primary tumor mutations (including KRAS mutational status) was conducted on the surgical specimen using NGS. Tumor DNA was extracted from a 10 µm-thick section of FFPE samples using the Maxwell® 16 FFPE Plus LEV DNA Purification Kit (Promega) according to the manufacturer’s instructions. Extracted DNA was quantified using the Qubit dsDNA broad-range assay kit in combination with a Qubit Fluorometer (Thermo Scientific). A qPCR-based assay was also carried out to qualify the extracted genomic DNA. Targeted sequencing of a panel of 48 genes frequently involved in solid tumors (ACVR1, AKT1, ALK, BRAF, BRCA1, BRCA2, CKDKN2A, CTNNB1, DDR2, DICER1, EGFR, ARBB2, ARBB4, FGFR1, FGFR2, FGFR3, FGFR4, FOXL2, GNA11, GNAQ, GNAS, H3F3A, H3F3B, HIST1H3B, HIST1H3C, HRAS, IDH1, IDH2, JAK2, KIT, KRAS, MAP2K1, MET, MYOD1, NRAS, PDGFRA, PIK3CA, POLD1, POLE, PRKD1, PTEN, PTPN11, RAC1, RET, SMAD4, STK11, TERT, TP53) including KRAS (exons 2, 3 and 4) was executed using capture-based target enrichment. DNA libraries were prepared using Twist Biosciences instruction with mechanical fragmentation (Covaris ME220 system). Samples were sequenced on an Illumina MiseqDX or NextSeq 550 in paired-end sequencing (2 × 150 cycles) using a minimum of 5 ng, with up to 100 ng of DNA input. We targeted a minimum depth of 150X with a limit of detection of 3%.
Digital droplet PCR and analysis
CfDNA was tested for the presence of KRAS mutation by digital droplet PCR. All plasma samples were screened for the three most frequent KRAS mutations in pancreatic adenocarcinoma (i.e., codons 12 and 13) by ddPCR on the QX200 system (Bio-Rad, France) using ddPCR™ KRAS G12/G13 Screening Kit (1,863,506) or ddPCR™ KRAS Q61 Screening Kit (12,001,626) (Bio-Rad, France) when KRAS mutation was detected in codon 61 on the surgical specimen using NGS. For each sample, a triplicate of 8 μL cfcDNA was tested. Negative controls with no DNA or KRAS wild-type DNA as well as positive controls for G12V, G12D, G12R or Q61 mutation at 0.5% mutant allele frequency (MAF) were included in each run. ddPCR was performed according to the manufacturer’s protocol and analyzed using Quantasoft software v1.5.38.1118 (Bio-Rad, France). A minimum of 10,000 accepted droplets per well was required for valid quantification and the sample was considered positive for KRAS mutation when at least three positive droplets were detected. Results were expressed as the number of KRAS mutations copies detected per mL of plasma.
Statistical analysis
Data were summarized using descriptive statistics. Categorical variables were presented as frequency and percentage and continuous variables as median and range. Survival rates were estimated using the Kaplan–Meier method with 95% confidence interval (95% CI). Univariate analyses were performed using the Logrank test and the Cox proportional hazards model. Hazards ratios (HR) were estimated with 95% CI. To prevent immortal-time bias, landmark analyses were carried out to study the association between parameters measured post-surgery and RFS and OS. All statistical tests were two-sided and a p-value less than 0.05 was considered statistically significant. Statistical analyses were performed using STATA v16 (StataCorp, College Station, TX, USA) software.
Data Availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at Toulouse University Hospital. This study was registered on 19/02/2018 on the ClinicalTrials.gov website under the reference NCT03435536.
Abbreviations
- 95% CI:
-
95% Confidence Interval
- CA 19–9:
-
Carbohydrate Antigen 19.9
- CCI:
-
Comprehensive Complication Index
- cfDNA:
-
Cell-Free DNA
- ctDNA:
-
Circulating Tumor DNA
- IPMN:
-
Intraductal Papillary Mucinous Tumor of the Pancreas
- MD:
-
Missing Data
- NGS:
-
Next-Generation Sequencing
- OS:
-
Overall Survival
- PDAC:
-
Pancreatic Ductal Adenocarcinoma
- POD:
-
Post-Operative Day
- POM:
-
Post-Operative Month
- POPF:
-
Post-Operative Pancreatic Fistula
- RFS:
-
Recurrence-Free Survival
- SMA:
-
Superior Mesenteric Artery
- TNM:
-
Tumor Node Metastasis
References
Siegel, R. L., Miller, K. D., Wagle, N. S. & Jemal, A. Cancer statistics, 2023. CA. Cancer J. Clin. 73, 17–48 (2023).
Rahib, L. et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 74, 2913–2921 (2014).
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2020. CA. Cancer J. Clin. 70, 7–30 (2020).
Conroy, T. et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 379, 2395–2406 (2018).
Riva, F. et al. Clinical applications of circulating tumor DNA and circulating tumor cells in pancreatic cancer. Mol. Oncol. https://doi.org/10.1016/j.molonc.2016.01.006 (2016).
Ballehaninna, U. K. & Chamberlain, R. S. The clinical utility of serum CA 19–9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 3, 105–119 (2012).
Coppola, A. et al. Role of CA 19.9 in the Management of Resectable Pancreatic Cancer: State of the Art and Future Perspectives. Biomedicines 10, 2091 (2022).
Isaji, S. et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 18, 2–11 (2018).
Earl, J. et al. Circulating tumor cells (Ctc) and kras mutant circulating free Dna (cfdna) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer 15, 797 (2015).
Poruk, K. E. et al. The Clinical Utility of CA 19–9 in Pancreatic Adenocarcinoma: Diagnostic and Prognostic Updates. Curr. Mol. Med. 13, 340–351 (2013).
Goggins, M. Markers of pancreatic cancer: working toward early detection. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 17, 635–637 (2011).
Pappas, L., Adalsteinsson, V. A. & Parikh, A. R. The emerging promise of liquid biopsies in solid tumors. Nat. Cancer 3, 1420–1422 (2022).
Bettegowda, C. et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 6, 224ra24 (2014).
Fleischhacker, M. & Schmidt, B. Circulating nucleic acids (CNAs) and cancer—A survey. Biochim. Biophys. Acta BBA - Rev. Cancer 1775, 181–232 (2007).
Mandel, P. & Metais, P. Nuclear Acids In Human Blood Plasma. C. R. Seances Soc. Biol. Fil. 142, 241–243 (1948).
Holdenrieder, S. & Stieber, P. Circulating apoptotic markers in the management of non-small cell lung cancer. Cancer Biomark. Sect. Dis. Markers 6, 197–210 (2010).
Olmedillas-López, S., Olivera-Salazar, R., García-Arranz, M. & García-Olmo, D. Current and Emerging Applications of Droplet Digital PCR in Oncology: An Updated Review. Mol. Diagn. Ther. https://doi.org/10.1007/s40291-021-00562-2 (2021).
Palacín-Aliana, I. et al. Clinical Utility of Liquid Biopsy-Based Actionable Mutations Detected via ddPCR. Biomedicines 9, 906 (2021).
Nitschke, C. et al. Peripheral and Portal Venous KRAS ctDNA Detection as Independent Prognostic Markers of Early Tumor Recurrence in Pancreatic Ductal Adenocarcinoma. Clin. Chem. hvac214 (2023) https://doi.org/10.1093/clinchem/hvac214.
Qian, Z. R. et al. Association of alterations in main driver genes with outcomes of patients with resected pancreatic ductal adenocarcinoma. JAMA Oncol. 4, e173420 (2018).
Cancer Genome Atlas Research Network. Electronic address: andrew_aguirre@dfci.harvard.edu & Cancer Genome Atlas Research Network. Integrated Genomic Characterization of Pancreatic Ductal Adenocarcinoma. Cancer Cell 32, 185–203.e13 (2017).
Buscail, L., Bournet, B. & Cordelier, P. Role of oncogenic KRAS in the diagnosis, prognosis and treatment of pancreatic cancer. Nat. Rev. Gastroenterol. Hepatol. 17, 153–168 (2020).
Bournet, B. et al. Endoscopic ultrasound-guided fine-needle aspiration biopsy coupled with KRAS mutation assay to distinguish pancreatic cancer from pseudotumoral chronic pancreatitis. Endoscopy 41, 552–557 (2009).
Pietrasz, D. et al. Plasma Circulating Tumor DNA in Pancreatic Cancer Patients Is a Prognostic Marker. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 23, 116–123 (2017).
Nagai, M., Sho, M., Akahori, T., Nakagawa, K. & Nakamura, K. Application of liquid biopsy for surgical management of pancreatic cancer. Ann. Gastroenterol. Surg. 4, 216–223 (2020).
Guven, D. C. et al. A systematic review and meta-analysis of the association between circulating tumor DNA (ctDNA) and prognosis in pancreatic cancer. Crit. Rev. Oncol. Hematol. 168, 103528 (2021).
Bunduc, S. et al. Prognostic role of cell-free DNA biomarkers in pancreatic adenocarcinoma: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 169, 103548 (2022).
Groot, V. P. et al. Circulating Tumor DNA as a Clinical Test in Resected Pancreatic Cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 25, 4973–4984 (2019).
Pietrasz, D. et al. Circulating tumour DNA: a challenging innovation to develop ‘precision onco-surgery’ in pancreatic adenocarcinoma. Br. J. Cancer 126, 1676–1683 (2022).
Griffiths, J. D., McKinna, J. A., Rowbotham, H. D., Tsolakidis, P. & Salsbury, A. J. Carcinoma of the colon and rectum: circulating malignant cells and five-year survival. Cancer 31, 226–236 (1973).
Takii, Y. et al. The Conventional Technique Versus the No-touch Isolation Technique for Primary Tumor Resection in Patients With Colon Cancer (JCOG1006): A Multicenter, Open-label, Randomized. Phase III Trial. Ann. Surg. 275, 849–855 (2022).
Strijker, M. et al. Circulating tumor DNA quantity is related to tumor volume and both predict survival in metastatic pancreatic ductal adenocarcinoma. Int. J. Cancer 146, 1445–1456 (2020).
Kruger, S. et al. Repeated mutKRAS ctDNA measurements represent a novel and promising tool for early response prediction and therapy monitoring in advanced pancreatic cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 29, 2348–2355 (2018).
Mohan, S. et al. Analysis of circulating cell-free DNA identifies KRAS copy number gain and mutation as a novel prognostic marker in Pancreatic cancer. Sci. Rep. 9, 11610 (2019).
Kim, M. K. et al. Prognostic Implications of Multiplex Detection of KRAS Mutations in Cell-Free DNA from Patients with Pancreatic Ductal Adenocarcinoma. Clin. Chem. 64, 726–734 (2018).
Patel, H. et al. Clinical correlates of blood-derived circulating tumor DNA in pancreatic cancer. J. Hematol. Oncol.J Hematol Oncol 12, 130 (2019).
Edland, K. H. et al. Monitoring of circulating tumour DNA in advanced pancreatic ductal adenocarcinoma predicts clinical outcome and reveals disease progression earlier than radiological imaging. Mol. Oncol. 17, 1857–1870 (2023).
Lee, B. et al. Circulating tumor DNA as a potential marker of adjuvant chemotherapy benefit following surgery for localized pancreatic cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 30, 1472–1478 (2019).
Buscail, E. et al. Liquid Biopsy Approach for Pancreatic Ductal Adenocarcinoma. Cancers 11, (2019).
Sausen, M. et al. Clinical implications of genomic alterations in the tumour and circulation of pancreatic cancer patients. Nat. Commun. 6, 7686 (2015).
Hadano, N. et al. Prognostic value of circulating tumour DNA in patients undergoing curative resection for pancreatic cancer. Br. J. Cancer 115, 59–65 (2016).
Shah, D. et al. Prospective Evaluation of Circulating Tumor DNA using Next Generation Sequencing as a Biomarker during Neoadjuvant Chemotherapy in Localized Pancreatic Cancer. Ann. Surg. https://doi.org/10.1097/SLA.0000000000006209 (2024).
Zhang, X. et al. Characterization of the genomic landscape in large-scale Chinese patients with pancreatic cancer. EBioMedicine 77, 103897 (2022).
Witkiewicz, A. K. et al. Whole-exome sequencing of pancreatic cancer defines genetic diversity and therapeutic targets. Nat. Commun. 6, 6744 (2015).
Perkins, G., Lu, H., Garlan, F. & Taly, V. Droplet-Based Digital PCR: Application in Cancer Research. Adv. Clin. Chem. 79, 43–91 (2017).
Huerta, M. et al. Circulating Tumor DNA Detection by Digital-Droplet PCR in Pancreatic Ductal Adenocarcinoma: A Systematic Review. Cancers 13, (2021).
Evan, T., Wang, V.M.-Y. & Behrens, A. The roles of intratumour heterogeneity in the biology and treatment of pancreatic ductal adenocarcinoma. Oncogene 41, 4686–4695 (2022).
Shin, S. H. et al. Chronologic changes in clinical and survival features of pancreatic ductal adenocarcinoma since 2000: A single-center experience with 2,029 patients. Surgery 164, 432–442 (2018).
Yamaguchi, T. et al. Clinical Implications of Pre- and Postoperative Circulating Tumor DNA in Patients with Resected Pancreatic Ductal Adenocarcinoma. Ann. Surg. Oncol. 28, 3135–3144 (2021).
Műzes, G., Bohusné Barta, B., Szabó, O., Horgas, V. & Sipos, F. Cell-Free DNA in the Pathogenesis and Therapy of Non-Infectious Inflammations and Tumors. Biomedicines 10, 2853 (2022).
Sanjay, P., Takaori, K., Govil, S., Shrikhande, S. V. & Windsor, J. A. ‘Artery-first’ approaches to pancreatoduodenectomy. Br. J. Surg. 99, 1027–1035 (2012).
Hussung, S. et al. Longitudinal analysis of cell-free mutated KRAS and CA 19–9 predicts survival following curative resection of pancreatic cancer. BMC Cancer 21, 49 (2021).
Nakano, Y. et al. KRAS mutations in cell-free DNA from preoperative and postoperative sera as a pancreatic cancer marker: a retrospective study. Br. J. Cancer 118, 662–669 (2018).
Wang, S.-E. et al. Circulating Cell-Free DNA in Pancreatic Head Adenocarcinoma Undergoing Pancreaticoduodenectomy. Pancreas 50, 214–218 (2021).
Dekker, E. N. et al. Improved Clinical Staging System for Localized Pancreatic Cancer Using the ABC Factors: A TAPS Consortium Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 42, 1357–1367 (2024).
Conroy, T. et al. Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 34, 987–1002 (2023).
National Comprehensive Cancer Network. Pancreatic Adenocarcinoma, Version 3.2024. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). (2024).
Buscail, E. et al. High Clinical Value of Liquid Biopsy to Detect Circulating Tumor Cells and Tumor Exosomes in Pancreatic Ductal Adenocarcinoma Patients Eligible for Up-Front Surgery. Cancers 11, (2019).
Yang, Z. et al. A Multianalyte Panel Consisting of Extracellular Vesicle miRNAs and mRNAs, cfDNA, and CA19–9 Shows Utility for Diagnosis and Staging of Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. (2020) https://doi.org/10.1158/1078-0432.CCR-19-3313.
Ben-Ami, R. et al. Protein biomarkers and alternatively methylated cell-free DNA detect early stage pancreatic cancer. Gut gutjnl-2023–331074 (2023) https://doi.org/10.1136/gutjnl-2023-331074.
Pietrasz, D. et al. Prognostic value of circulating tumour DNA in metastatic pancreatic cancer patients: post-hoc analyses of two clinical trials. Br. J. Cancer https://doi.org/10.1038/s41416-021-01624-2 (2021).
Boutonnet, A. et al. Size and Concentration of Cell-Free DNA Measured Directly from Blood Plasma, without Prior DNA Extraction. Anal. Chem. 95, 9263–9270 (2023).
Hagey, D. W. et al. Extracellular vesicles are the primary source of blood-borne tumour-derived mutant KRAS DNA early in pancreatic cancer. J. Extracell. Vesicles 10, e12142 (2021).
Yang, S. et al. Detection of mutant KRAS and TP53 DNA in circulating exosomes from healthy individuals and patients with pancreatic cancer. Cancer Biol. Ther. 1–8 (2017) https://doi.org/10.1080/15384047.2017.1281499.
Allenson, K. et al. High prevalence of mutant KRAS in circulating exosome-derived DNA from early-stage pancreatic cancer patients. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 28, 741–747 (2017).
Bassi, C. et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 161, 584–591 (2017).
Dindo, D., Demartines, N. & Clavien, P.-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240, 205–213 (2004).
Slankamenac, K., Graf, R., Barkun, J., Puhan, M. A. & Clavien, P.-A. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann. Surg. 258, 1–7 (2013).
Funding
This study was supported by a grant from the Toulouse University Hospital, local grant 2017, no. RC31/17/0327 and was registered on the ClinicalTrials.gov website under the reference NCT03435536.
Author information
Authors and Affiliations
Contributions
(I) Conception and Design: Charlotte Maulat, Cindy Canivet, Louis Buscail, Barbara Bournet, Fabrice Muscari and Pierre Cordelier. (II) Administrative Support: Charlotte Maulat, Cindy Canivet, Louis Buscail, Barbara Bournet, Fabrice Muscari and Pierre Cordelier. (III) Provision of Study Materials or Patients: Charlotte Maulat, Cindy Canivet, Anne Pradines, Janick Selves, Anne Casanova, Aurélia Doussine, Naïma Hanoun, Paul Boulard, Emmanuel Cuellar, Nicolas Carrère, Louis Buscail, Barbara Bournet, Fabrice Muscari and Pierre Cordelier. (IV) Collection and Assembly of Data: Charlotte Maulat, Cindy Canivet, Anne Pradines, Janick Selves, Anne Casanova, Aurélia Doussine, Naïma Hanoun, Paul Boulard, Emmanuel Cuellar, Nicolas Carrère, Louis Buscail, Barbara Bournet, Fabrice Muscari and Pierre Cordelier. (V) Data Analysis and Interpretation: Charlotte Maulat, Cindy Canivet, Bastien Cabarrou, Anne Pradines, Janick Selves, Anne Casanova, Aurélia Doussine, Naïma Hanoun, Barbara Bournet, Fabrice Muscari and Pierre Cordelier. (VI) Manuscript Writing: Charlotte Maulat and Pierre Cordelier (first draft). Revision: All Authors. (VII) Final Approval of Manuscript: All Authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Maulat, C., Canivet, C., Cabarrou, B. et al. Prognostic impact of circulating tumor DNA detection in portal and peripheral blood in resected pancreatic ductal adenocarcinoma patients. Sci Rep 14, 27296 (2024). https://doi.org/10.1038/s41598-024-76903-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76903-y
Keywords
This article is cited by
-
Circulating tumor DNA–guided early detection and minimal residual disease monitoring in pancreatic and biliary cancers: evidence, barriers, and opportunities
World Journal of Surgical Oncology (2026)
-
Research progress on early diagnostic markers for pancreatic cancer
World Journal of Surgical Oncology (2026)
