
Abstract
Numerous studies have shown that wasp stings can lead to serious, sometimes fatal, health outcomes. Predicting deaths associated with wasp stings remains challenging yet is of critical importance. This study was conducted to identify predictors and develop a visual model for predicting mortality following wasp stings. Clinical data from 486 patients were analyzed, dividing them into two groups: survival group (N = 435) and death group (N = 51). Various statistical methods were used to create a prognostic model, including one-way analysis, the least absolute shrinkage and selection operator (LASSO) regression, and binary logistic regression. The model’s accuracy was evaluated through ROC curves, calibration plots, and decision curve analysis (DCA). The study identified four key predictors of mortality: receiving more than 50 stings, having serum lactate dehydrogenase (LDH) levels of ≥ 2200 U/L, activated partial thromboplastin time (APTT) of ≥ 90 s, and the requirement for invasive mechanical ventilation within 24 h. These factors contributed to a model with an area under the ROC curve of 0.980 (95% CI: [0.968–0.992]), indicating high calibration and applicability. The decision curve analysis confirmed the model’s substantial net clinical benefit. Thus, the number of stings, serum LDH, APTT, and the need for early invasive mechanical ventilation are reliable, independent predictors of death among patients experiencing wasp stings. The developed predictive model exhibits high levels of accuracy, sensitivity, consistency, and practical use.
Similar content being viewed by others

Introduction
During the past three decades, Hymenoptera (stings due to hornets, wasps, and bees) has increased in number, posing significant public health challenges. When threatened by humans, Hymenoptera can release venom via stings, leading to diverse clinical outcomes from local reactions to severe allergic responses and even multiple organ failure due to allergic reactions and direct toxicity1. Diverse dominant bee species and races across regions lead to significant variability in clinical symptoms and mortality rates from wasp stings, hindering adequate understanding and intervention. Between 2009 and 2019, Brazil recorded 1,957,096 injuries and 2,970 fatalities from venomous animals, with Hymenoptera accounting for 144,790 (7.40%) injuries and 425 (14.31%) deaths. The mortality rate associated with bee incidents was reported at 0.29%, corresponding to an average annual incidence rate of 6.89 per 100,000 residents2. Annually, Hymenoptera stings prompt approximately 220,000 emergency department visits and cause an average of 62 deaths in the United States, making stings from hornets, wasps, and bees the deadliest of all venomous animal encounters3. Between 1994 and 2016, Hymenoptera stings, including those from hornets, wasps, and bees, caused 1,691 fatalities due to severe allergic reactions across 32 European countries4. In 2013, XIE et al. conducted a multi-center study in Hubei Province, Central China, analyzing 1,091 wasp sting cases5. They found that the majority were wasp stings, primarily causing toxic injuries, with an in-hospital mortality rate of 5.1%. A multi-centre study in Sichuan Province in 2021, Western China, revealed that wasp sting mortality rates reached 37% with over 30 stings and escalated to 75% when the sting count exceeded 1006. In addition to these regions, a significant public health concern has emerged in northwestern Galicia, Spain, where recent studies reveal alarmingly high mortality rates from Hymenoptera stings, exacerbated by the invasive Vespa velutina (Asian hornet). Since its introduction in 2012, this species has rapidly spread, leading to a sharp increase in sting-related fatalities. From 1999 to 2018, mortality rates in Galicia reached 1.82, 1.10, and 2.22 deaths per million inhabitants in 2014, 2016, and 2018, respectively7. These findings underscore the global underestimation of wasp stings as a public health threat, calling for urgent and focused intervention.
Presently, there is no globally recognized, effective specific treatment for wasp stings. Early identification of clinical characteristics indicative of potential fatal progression can enable targeted interventions. This approach is anticipated to delay disease progression, optimize the use of medical resources, and ultimately reduce mortality rates. Prior research has identified oliguria, shock, and anaemia as prognostic risk factors in wasp sting cases, yet these are not early symptoms of such stings5. Some studies have established a correlation between Hymenoptera species, number of stings, age, hematuria, and lactate dehydrogenase levels with renal failure8,9,10. This study addresses the scarcity of research on using basic clinical and hematological markers to predict early mortality from wasp stings, aiming to identify early patient traits and independent risk factors and develop and validate a mortality prediction nomogram.
Materials and methods
Study population
X Hospital, a major medical and teaching centre affiliated with the Hubei University of Medicine, is located in northwest Hubei Province, China. With 4800 beds, it annually handles 50–100 wasp sting cases. Our study retrospectively examined 570 wasp sting cases admitted to the Emergency Department from January 2015 to December 2023, all from within China. Inclusion criteria were as follows: (1) diagnosis of wasp stings relied on patient-reported history, clinical symptoms consistent with envenomation, and insect identification by the patient or attending physician, and (2) age ≥ 18 years old. Exclusion criteria were as follows: (1) Age < 18 years old; (2) cases involving stings from hornets, wasps, and bees where the species could not be confirmed; (3) patients with incomplete clinical data; and (4) pregnant or breastfeeding women.
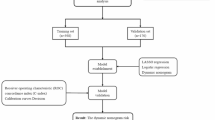
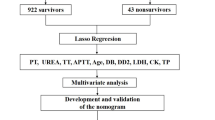
Out of 570 wasp sting cases, 84 were excluded: 41 minors, 9 with unconfirmed sting species, 7 pregnant or breastfeeding, and 27 with incomplete data. This left 486 cases for final analysis, categorized into 435 survivors and 51 fatalities at 28 days. Figure 1 illustrates the schematic representation of the study’s flow.

Flowchart of the processing step for predicting wasp stings mortality.
The Medical Ethics Committee of Taihe Hospital, associated with Hubei University of Medicine, provided ethical approval for this retrospective study (Approval No. 2024KS04). Adhering to the principles of the Declaration of Helsinki, the requirement for informed consent was exempted as all patient data were anonymized and de-identified before the analysis.
Data collection
The Emergency Department’s scientific research team at X Hospital analyzed medical records. Data were collected using the Haitai System electronic medical record and follow-up system, encompassing epidemiological and clinical data, laboratory examinations, treatment, and 28-day outcomes. This included demographic information, underlying diseases, sting count, complications, laboratory tests (blood routine, liver function, myocardial enzymes spectrum, and coagulation function), and treatment measures. In cases where the same parameter is tested multiple times within 24 h, the result indicating the most severe abnormality will be selected for record and analysis. Data collection was performed using Microsoft Excel. For missing data, we used prior data, such as records from other hospitals, or data from 48 to 72 h post-admission to supplement data within 24 h of admission.
For the purpose of this study, 28-day survival status is defined as survival over a period of 28 days, counting from the day the patient was stung by a wasp. This study includes deaths from all causes and is not limited to deaths directly or indirectly caused by wasp stings. We obtained information on patients’ survival status by telephone follow-up.
In our study, hematological parameters were primarily derived from peripheral venous blood, except for arterial blood used in blood gas analysis. Peripheral blood samples were analyzed using the Mindray BC-5800, a sophisticated automatic blood cell analyzer from Shenzhen, China. Kidney and liver functions were evaluated using Hitachi’s Automatic Biochemistry Analyzer 7600. Coagulation function was assessed with the Sysmex CS5100, an automatic coagulation analyzer from Japan. Arterial blood gas analysis utilized Roche’s COBASb 123 autoanalyzer, based in Basel, Switzerland. All tests adhered strictly to instrument-specific test kits and followed the manufacturers’ guidelines to ensure consistent and accurate results.
Definition of variables
Wasp species identification was based on a combined assessment of species map comparisons and the characteristics of skin lesions observed at admission. The 'number of stings’ is defined as the total count of skin lesions observed and recorded at admission. In alignment with the 'Expert Consensus on Standardized Diagnosis and Treatment of Wasp Stings in China’11 and recent research9 from Taiwan Province, China, and our clinical practice, we categorize sting counts into three intervals: < 25, 25–50, and ≥ 50.
Rhabdomyolysis diagnosis is established when CK concentration is ≥ 1000 U/L, or myoglobin exceeds the standard upper limit12. Elevated transaminases are defined as AST or ALT concentrations exceeding three times the standard upper limit13. APTT levels were categorized as < 90 s or ≥ 90 s, based on twice the standard upper limit14. The diagnosis of acute kidney injury adhered to the Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guidelines in 201215.
Gross hematuria is characterized by urine appearing brown or reddish-brown16. Acute intravascular hemolysis is indirectly inferred from elevated blood-free hemoglobin, reduced red blood cell and hemoglobin counts, increased blood unconjugated bilirubin, and elevated lactate dehydrogenase levels17. Blood purification treatments encompass hemoperfusion (HP), plasma exchange (PE), continuous renal replacement therapy (CRRT), and hemodiafiltration (HD/HF). Typically, these treatments involve combining two different methods18.
Treatments followed the 'Expert Consensus on Standardized Diagnosis and Treatment of Wasp Stings in China’11. For acute respiratory failure from wasp stings, if high-flow nasal oxygen or non-invasive ventilation fails or hypoxia persists, immediate tracheal intubation and invasive mechanical ventilation are recommended.
Statistical analysis
Data was analyzed using RStudio on Windows, with categorical data assessed via chi-square or Fisher’s exact test, and continuous data through t-tests or Mann–Whitney U tests. SPSS 26.0 identified significant factors among 26 variables, and LASSO regression and multifactorial logistic regression were applied for feature selection and numerical modeling, respectively. Nomograms were created using the “regplot” package, with a significance threshold set at p < 0.05.
Development and assessment of the nomogram
Variables significant in univariate analysis were subjected to LASSO regression, targeting mortality as the outcome, with λ optimized via ten-fold cross-validation. Variables with non-zero coefficients advanced to multivariable logistic regression and ROC curve analysis, culminating in a predictive nomogram. Model validation encompassed discrimination, calibration, and clinical applicability. The area under the receiver operating characteristic (ROC) curve (AUC), a measure of model discrimination, was computed using the ‘pROC’ package. Model calibration was evaluated through Calibration curve analysis, implemented with the ‘calibrate’ package. Furthermore, the ‘rmda’ package was utilized for decision curve analysis (DCA), which quantifies the net benefits at different threshold probabilities, thereby assessing the clinical utility of the model.
Result
Characteristics of the study population
Of the 486 cases meeting the inclusion criteria, 286 were male (58.85%) and 200 female (41.15%), with an average age of 51.36 ± 14.63 years. The survival group comprised 435 cases (89.51%), averaging 50.26 ± 14.21 years, while the death group included 51 cases (10.49%), averaging 60.71 ± 14.98 years. The age within the death group was significantly higher than that in the survival group, with a statistically significant difference (P < 0.05). However, there was no statistically significant difference in gender distribution between the two groups (P > 0.05). Table 1 presents the comprehensive clinical data for both groups.
Variable transformation and selected predictors
In this study, the median LDH level among cases with elevated blood LDH (≥ 240U/L) was 1086U/L (425.0, 2468.0), approximated as 1100U/L. LDH values were categorized as LDH ≥ 2200U/L, representing twice the integral multiple of 1100U/L. Similarly, continuous variables like CK, AST, and APTT were converted into categorical variables: CK ≥ 1000U/L, AST ≥ 120U/L, and APTT ≥ 90 s. A value of 1 was assigned when the actual measurement matched the category; otherwise, it was set to 0.
Single-factor difference analysis revealed no significant differences between the two groups in 10 variables (P > 0.05): gender, number of stings between 25 and 50, platelet count, chronic liver insufficiency, chronic renal insufficiency, chronic respiratory disease, cerebrovascular disease, hypertension, cardiovascular disease, and diabetes as shown in Table 1. However, significant differences were observed in 16 variables (P < 0.05): age ≥ 65 years, number of stings < 25, number of stings ≥ 50, hematuria, hemolysis, AST ≥ 120 U/L, CK ≥ 1000 U/L, LDH ≥ 2200 U/L, APTT ≥ 90 s, the need for blood purification, and the need for invasive mechanical ventilation within 24 h. From the initial set of 16 variables, LASSO regression analysis led to the identification of 4 features with potential predictive value, including the number of stings ≥ 50, LDH ≥ 2200 U/L, APTT ≥ 90 s, and the progression to needing invasive mechanical ventilation within 24 h, as illustrated in Fig. 2A, B. The final model, constructed via multivariable logistic regression, incorporated the 4 potential predictive features discerned from the LASSO regression analysis.

Features selection using the LASSO binary logistic regression model. (a) Log (Lambda) value of the 16 features in the LASSO model. A coefficient profile plot was produced against the log (lambda) sequence. (b) Parameter selection in the LASSO model used tenfold cross-validation via minimum criterion. Partial likelihood deviation (binomial deviation) curves and logarithmic (lambda) curves were plotted. Use the minimum standard and 1se (1-SE standard) of the minimum standard to draw a vertical dashed line at the optimal value. The optimal lambda produced four nonzero coefficients. Abbreviations: LASSO: Least Absolute Shrinkage and Selection Operator; SE, Standard Error.
Establishment and validation of the model
Multivariate logistic regression analysis identified that a number of stings ≥ 50, LDH ≥ 2200 U/L, APTT ≥ 90 s, and the need for invasive mechanical ventilation for 24 h were independent predictive factors of mortality from wasp stings (Table 2). These predictors were used to create a predictive nomogram (Fig. 3).

Nomogram for Predicting Wasp Sting Mortality Based on Four Indicators If a patient has a total score of 134, then the probability of death is about 0.4. (number of stitches ≥ 50, LDH ≥ 2200, and APTT ≥ 90). Abbreviation:IMV(24 h):Invasive Mechanical Ventilation Required within 24 h. LDH: Lactate Dehydrogenase. APTT: Activated Partial Thromboplastin Time.
The model’s AUC for differentiating positive and negative outcomes was 0.98(95%CI: [0.97–0.99]), demonstrating its strong capability in distinguishing between mortality and survival cases (Fig. 4a). Furthermore, the calibration plot (Fig. 4b) indicates a good concordance between the mortality risk predicted by the model and the actual observed mortality risk. The decision curve shows that if the threshold probability of an individual is between 0% and 82.5%, using this model to predict the mortality rate with wasp stings adds more benefit than either the treat-all or treat-none tactics (Fig. 4c).

Model evaluation and validation (a) Evaluation of ROC column line. The area under the receiver operating characteristic curve of the model was 0.980 (95%CI:[0.968–0.992]); (b) Calibration curve of the nomogram prediction in the cohort. The diagonal dotted line depicts a perfect prediction by an ideal model. The solid line reflects the performance of the nomogram; a closer fit to the diagonal dotted line indicates a better prediction; (c) Decision curve analysis curve of the nomogram for predicting the probability of mortality with wasp stings. The horizontal and vertical axes represent the threshold probability and net benefit, respectively. The lines between the horizontal axis and vertical axis display the benefit of different predictive variables. The DCA curve shows that if the threshold probability is between 0% and 82.5%, using this nomogram in the current study to predict mortality risk with wasp stings could add more benefit.
Discussion
This study is the first single-centre retrospective analysis to develop an early prediction model for mortality from wasp stings. It delineates the initial clinical features of patients who succumbed to wasp stings and identifies four independent risk factors: number of stings ≥ 50, LDH ≥ 2200 U/L, APTT ≥ 90 s, and the requirement for Invasive mechanical ventilation within 24 h. A nomogram prediction model for early mortality from wasp stings has been established, demonstrating strong predictive capability and clinical relevance. It holds promise as a tool for early management and decision-making in cases of wasp stings. A recent study by Wang Maohe et al. in Suining City, Sichuan Province, identified female gender, age, number of stings, and the Poisoning Severity Score (PSS) as independent risk factors for mortality in patients with wasp stings19. The higher mortality rate from wasp stings among women in this study may be primarily due to the higher proportion of older women in the group.In Sichuan Province, a significant labor-export region in China, older women working in farming at home are more susceptible to wasp stings. While PSS is straightforward, it encompasses multiple systems. The prognostic implications of damage to different systems vary significantly. Moreover, much of the scoring relies on subjective assessments rather than objective laboratory tests. Advancing age correlates with chronic cardiovascular, pulmonary, and renal function deterioration alongside a diminished compensatory reserve capacity20,21. However, our study found that age did not significantly impact prognosis, and underlying diseases were similarly distributed across groups, possibly because the participants were mostly healthy outdoor workers with low rates of underlying conditions. Addressing past research gaps, this study includes sting count and basic hematological indicators, offering a more objective, comprehensive, and accessible approach with broader applicability and accuracy.
In clinical practice, precise quantification of wasp venom is not feasible. Consequently, the direct toxic effect of wasp venom is typically inferred from the number of stings. Prior research often utilized a cutoff at 10 stings without conducting subgroup analyses for counts exceeding this number5,9. This approach raises concerns about the accuracy of the dose–effect relationship between the number of stings and the resultant poisoning effects. Species distribution varies by region, leading to differences in the quantity and composition of venom per sting. In Europe and America, life-threatening reactions to African Hymenoptera stings typically occur at counts of 1,000–2,000 stings, which is a stark contrast to the findings of this study22. In this study, the mortality rate was 2% (6 out of 300 cases) for sting counts below 25, 9.6% (12 out of 125 cases) for counts between 25 and 50, and 54.1%(33 out of 61 cases) for counts of 50 or more. This aligns with findings from a recent study in Taiwan, which reported a mortality rate of approximately 50% for cases involving more than 50 stings9. Both single-factor and multi-factor logistic regression analyses were conducted, revealing that a sting count above 50 independently predicts mortality risk in patients with wasp stings. Early in the treatment process, the prognosis can be initially assessed based on the number of stings. Patients with over 50 stings require particularly close attention and prompt, intensified treatment. However, it is essential to recognize that individual responses to the same number of stings can vary significantly. The possibility of a ‘dry bite’ phenomenon in wasps, similar to that in venomous snakes, remains unclear. This could impact the accuracy of sting counts, especially when skin lesions are inconspicuous in the early stages, potentially complicating the assessment of the toxic dose–response relationship.
Respiratory system involvement frequently occurs when individuals are stung by wasps. The necessity for invasive mechanical ventilation due to early acute respiratory failure is linked with unfavorable prognoses. The underlying pathogenesis is likely linked to early allergic reactions, toxic pulmonary edema, acute renal failure, heart failure, and other factors. Wasp venom is a natural composite of peptides, enzymes, and amines. Its primary components, melittin and phospholipase A2 (PLA2), synergistically induce cytolytic activity. This leads to the extensive release of cellular contents and cytokines, triggering an inflammatory storm and potentially a severe toxic syndrome23. In 2010, ZHANG L documented three cases of pulmonary edema and renal failure following wasp stings24. Two of these cases were successfully treated using a hybrid blood purification approach that combined Continuous Veno-Venous Hemofiltration (CVVH), Plasma Exchange (PE), and Sustained Low-Efficiency Dialysis (SLED). In 2022, Cai ZY managed a patient who experienced a severe case of ARDS due to a wasp sting25. Despite receiving mechanical ventilation and other treatments, the patient’s respiratory function continued to deteriorate. However, early intervention with Extracorporeal Membrane Oxygenation (ECMO) proved to be successful. It is common for patients who require invasive mechanical ventilation within the first 24 h after a wasp sting to develop severe multi-organ failure. This rapid progression poses challenges in treatment and requires significant medical resources, thus indicating a significant predictive value for mortality risk.
Lactate dehydrogenase (LDH) is an enzyme group that facilitates the reversible conversion of lactate to pyruvate during glucose metabolism. It plays a crucial role in anaerobic conversion of pyruvate to lactate. LDH is extensively distributed throughout the body and is released into the bloodstream following cellular damage or death from various causes. Elevated serum LDH levels indicate the extent of cellular and tissue damage. A comprehensive study encompassing 8,436 cases revealed that the mortality rate in critically ill patients with Acute Kidney Injury (AKI) rose almost linearly with increasing levels of LDH26. Another multi-centre retrospective analysis involving 1,981 critically ill patients across 208 ICUs in the United States found that serum LDH levels within the first 24 h of ICU admission were independently associated with both ICU and in-hospital mortality27. Wang et al. discovered a significant increase in the risk of Acute Kidney Injury (AKI) when serum LDH exceeded 463.5 U/L in wasp sting patients upon hospital admission16. However, the correlation between early serum LDH levels and early mortality in wasp sting patients remains unclear. Our study observed that an early increase in LDH levels in patients with wasp stings correlates with higher mortality rates. Specifically, when LDH levels reached ≥ 2200 U/L, the mortality rate escalated to 55.22% (37 out of 67 cases). The early rise in LDH is thought to be associated with hemolysis, rhabdomyolysis, and subsequent Multiple Organ Dysfunction Syndrome (MODS). Thus, LDH serves as a comprehensive marker for assessing disease severity and predicting short-term prognosis in patients with wasp stings.
In cases of wasp stings, coagulation dysfunction typically presents as abnormal Activated Partial Thromboplastin Time (APTT) and either standard or decreased platelet counts28,29. Lai D et al. reported on two severe wasp sting cases, each involving over 80 stings, leading to hemolysis, toxic hepatitis, and rhabdomyolysis30. Thromboelastography dynamic analysis in these cases revealed the presence of endogenous heparinization, which was rapidly reversible with protamine sulfate administration. In this study, the mortality rate was 5.4% (11 out of 370 cases) when APTT was < 90 s, and 34.5% (40 out of 116 cases) when APTT was ≥ 90 s. Single-factor and multi-factor logistic regression analyses indicated that an APTT ≥ 90 s in wasp sting patients is an independent predictor of mortality. Heparin, an acidic mucopolysaccharide primarily produced by mast cells and basophils, is abundantly present in human vascular endothelial cells, liver, intestines, and muscle tissues. Activation of these cells during allergic reactions, or in cases of endothelial injury, rhabdomyolysis, and liver failure, leads to the release of large amounts of endogenous heparin-like substances, causing coagulation disorders. Consequently, endogenous heparinization, resulting from toxic reactions or severe allergic events, can be indicated by prolonged Activated Partial Thromboplastin Time (APTT), serving as a marker for the severity and poor prognosis of wasp sting injuries.
We acknowledge several limitations in our study. As a retrospective, single-center analysis with a small sample size and no external validation, our findings may be affected by selection, information, and confounding biases, limiting generalizability. We only examined initial 24-h lab results, lacking ongoing monitoring of parameters like LDH or APTT, leaving their prognostic value uncertain. Our focus on patients with toxic reactions to wasp venom excluded those who died outside the hospital from severe allergic reactions, highlighting the need for future studies to develop prediction models that consider both toxic and allergic responses, including out-of-hospital mortality. Additionally, we did not gather specific geographical data for each patient and could not accurately determine the time from sting to hospital presentation for all. These factors further limit our work, underscoring the need for such data in future prospective studies. Despite these limitations, our study offers valuable insights into early mortality prediction following wasp stings, particularly for toxic reactions in hospitalized patients. Future prospective, multi-center studies with larger sample sizes are essential to refine the model and examine the influence of geographical factors, time to care, and the inclusion of both toxic and allergic reactions on outcomes.
In summary, this study identifies independent risk factors for mortality from wasp stings as a sting count ≥ 50, LDH ≥ 2200 U/L, APTT ≥ 90 s, and the requirement for invasive mechanical ventilation within 24 h. A predictive model, structured as a nomogram and based on these factors, could aid clinicians in recognizing high-risk patients early. This early detection may facilitate the initiation of more intensive treatments sooner, potentially improving patient outcomes.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due they contain sensitive personal information, but are available from the corresponding author on reasonable request.
References
Walker, A. A. et al. Entomovenomics: The evolution, biology and biochemistry of insect venoms. Toxicon 154, 15–27 (2018).
Kono, I. S. et al. Bee stings in Brazil: Epidemiological aspects in humans. Toxicon 201, 59–65 (2021).
Forrester, J. A., Weiser, T. G. & Forrester, J. D. An update on fatalities due to venomous and nonvenomous animals in the United States (2008–2015). Wilderness Environ. Med. 29, 36–44 (2018).
Feás, X., Vidal, C. & Remesar, S. What we know about sting-related deaths? Human Fatalities caused by hornet, wasp and bee stings in Europe (1994–2016). Biology 11, 282 (2022).
Xie, C. et al. Clinical features of severe wasp sting patients with dominantly toxic reaction: Analysis of 1091 cases. PLoS One. 8(12), e83164 (2013).
Liu, Y. et al. Development and internal validation of a Wasp Sting Severity Score to assess severity and indicate blood purification in persons with Asian wasp stings. Clin Kidney J. 15(2), 320–327 (2021).
Feás X. Human fatalities caused by hornet, wasp and bee stings in Spain: Epidemiology at state and sub-state level from 1999 to 2018. Biology (Basel). 2021;10(2):73. Published 2021 Jan 20. https://doi.org/10.3390/biology10020073
Tang, X. et al. Development and validation of a model to predict acute kidney injury following wasp stings: A multi-centre study. Toxicon. 209, 43–49 (2022).
Nguyen, T. N., Jeng, M. J., Chen, N. Y. & Yang, C. C. Outcomes of wasp and bee stings in Taiwan. Clin Toxicol (Phila). 61(3), 181–185 (2023).
Srisuwarn, P. et al. Clinical effects and factors associated with adverse clinical outcomes of hymenopteran stings treated in a Thai Poison Centre: A retrospective cross-sectional study. Clin Toxicol (Phila). 60(2), 168–174 (2022).
Yang, X. et al. Expert consensus statement on standardized diagnosis and treatment of wasp sting in China. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 30(9), 819–823 (2018).
Cabral, B. M. I. et al. Rhabdomyolysis. Dis Mon. 66(8), 101015 (2020).
Kalas, M. A. et al. Abnormal liver enzymes: a review for clinicians. World J Hepatol. 13(11), 1688–1698 (2021).
Cossette, B. et al. Evaluation of bleeding risk in patients exposed to therapeutic unfractionated or low molecular-weight heparin: a cohort study in the context of a quality improvement initiative. Ann Pharmacother. 44(6), 994–1002 (2010).
Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 120(4), c179–c184 (2012).
Wang, M. et al. Macroscopic hematuria in wasp sting patients: A retrospective study. Ren Fail. 43(1), 500–509 (2021).
Barcellini, W. & Fattizzo, B. Clinical applications of hemolytic markers in the differential diagnosis and management of hemolytic anemia. Dis Markers. 2015, 635670 (2015).
Gong, J. et al. Wasp venom and acute kidney injury: The mechanisms and therapeutic role of renal replacement therapy. Toxicon. 163, 1–7 (2019).
Wang, M. et al. Clinical manifestations and risk factors associated with 14 deaths following swarm wasp stings in a chinese tertiary grade a general hospital: A retrospective database analysis study. J Clin Med. 12(18), 5789 (2023).
Bland, J. S. Age as a modifiable risk factor for chronic disease. Integr. Med. (Encinitas). 2018;17(4):16–19.
Prasad, S., Sung, B. & Aggarwal, B. B. Age-associated chronic diseases require age-old medicine: Role of chronic inflammation. PrevMed. 54(Suppl), S29–S37 (2012).
Schmidt, J. O. Clinical consequences of toxic envenomations by hymenoptera. Toxicon. 150, 96–104 (2018).
Ferreira, R. S. Jr., Almeida, R. A., Barraviera, S. R. & Barraviera, B. Historical perspective and human consequences of Africanized bee stings in the Americas. J Toxicol Environ Health B Crit Rev 15, 97–108 (2012).
Zhang, L. et al. Hybrid renal replacement treatment in acute pulmonary edema with acute kidney injury following multiple wasp stings: A report of 3 cases. Blood Purif. 30(2), 106–107 (2010).
Cai, Z. Y. et al. Acute respiratory distress syndrome following multiple wasp stings treated with extracorporeal membrane oxygenation: A case report. World J Clin Cases. 10(30), 11122–11127 (2022).
Zhang, D. & Shi, L. Serum lactate dehydrogenase level is associated with in-hospital mortality in critically Ill patients with acute kidney injury. Int Urol Nephrol. 53(11), 2341–2348 (2021).
Su, D. et al. The relationship between serum lactate dehydrogenase level and mortality in critically ill patients. Biomark Med. 15(8), 551–559 (2021).
Wang, J. L., Shen, E. Y. & Ho, M. Y. Isolated prolongation of activated partial thromboplastin time following wasp sting. Acta Paediatr Taiwan. 46(3), 164–165 (2005).
Lombardini, C., Helia, R. E., Boehlen, F., et al. “Heparinization” and hyperfibrinogenolysis by wasp sting. Am J Emerg Med. 2009;27(9):1176.
Lai, D. et al. Hyperendogenous heparinization suggests a guideline for the management of massive wasp stings in two victims. Wilderness Environ Med. 32(3), 344–350 (2021).
Funding
This research was supported by a research grant from the Health Commission of Hubei Province, China (WJ2023M164).
Author information
Authors and Affiliations
Contributions
Sm Z conceived and designed the research strategy. Sm Z, Yh W, and Xy Y wrote and revised the manuscript text. Sm Z, Yh W, Zl Q, K Y and Hc Z performed the data collection. Sm Z, Yh W, Zc F, and Xy Y were involved in analyzing and interpreting the data. All authors made contributions to the manuscript and have given their approval for the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, S., Wang, Y., Quan, Z. et al. A prediction nomogram for mortality in patients following wasp stings: a retrospective study. Sci Rep 14, 26242 (2024). https://doi.org/10.1038/s41598-024-77152-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-77152-9
Keywords
This article is cited by
-
From sting to STING: role of inflammation in wasp sting induced AKI - a narrative review
BMC Nephrology (2025)
