
Abstract
This study aimed to develop and validate a nomogram using clinical variables to guide personalized treatment strategies for adenoid cystic carcinoma of the head and neck (ACCHN). Data from 1069 patients with ACCHN diagnosed between 2004 and 2015 in the Surveillance, Epidemiology, and End Results (SEER) database were used to construct the nomogram. External validation was performed using an independent cohort of 70 patients from Fujian Cancer Hospital. Multivariate Cox regression analysis was conducted using IBM SPSS version 26.0 and R Software version 4.2.3. The concordance index (C-index) and receiver operating characteristic (ROC) curves were used to assess the predictive accuracy of the nomogram. Age, tumor site, surgery, N stage, M stage, and TNM stage were identified as independent prognostic factors through univariate and multivariate Cox analyses. The nomogram demonstrated superior predictive performance compared to the TNM staging system, effectively stratifying patients into high-risk and low-risk groups. This nomogram offers a valuable tool for predicting overall survival in patients with ACCHN and tailoring individualized treatment approaches.
Similar content being viewed by others

Introduction
Adenoid cystic carcinoma (ACC) is a relatively rare tumor in head and neck cancers1. Adenoid cystic carcinoma of the head and neck (ACCHN) primarily affects the salivary glands, including the parotid, submandibular, and sublingual glands, though it may originate from other regions such as the sinuses, nasopharynx, and lacrimal glands2. Characterized by perineural invasion (PNI), local recurrence, and distant metastases, regional lymph node involvement in ACCHN is uncommon3,4. This malignancy can occur in patients of all ages and is more frequently diagnosed in women (59%), with a median age of 57.4 years at diagnosis5,6. The standard treatment involves surgical excision with negative margins, frequently followed by radiation therapy2.
ACCHN is an indolent yet highly aggressive malignancy with slow growth and a prolonged clinical course. While 5-year survival rates are generally favorable, ranging from 64% to 91.7%6,7,8,9,10,11, the long-term prognosis remains poor, with 10-year survival rates between 37 and 64%11,12,13,14. Despite its unpredictable clinical behavior and challenges in prognosis, some patients may live for several years even after recurrence15, making long-term monitoring particularly difficult. Traditionally, the American Joint Committee on Cancer (AJCC) staging system has been employed to assess prognosis and guide treatment decisions. However, the AJCC system may be too simplistic to account for the complexity of prognostic risks in patients with ACCHN16.
Various factors influence patient outcomes, including the tumor’s primary site, size, lymph node involvement, distant metastasis, TNM stage, histopathological grading, surgical margins, and PNI6,17,18. A study conducted at a Canadian Center demonstrated that younger patients with ACCHN who had negative lymph node status, had undergone surgical treatment, and had achieved negative surgical margins experienced improved overall survival (OS)19. Similarly, a 2016 study found that patients with tumors in the sublingual glands or those in stage IV had poorer survival outcomes20. Despite these studies, few studies have focused on creating a prognostic nomogram for patients with ACCHN.
Therefore, this research developed and validated a predictive model to estimate long-term survival in patients with ACCHN using data from the Surveillance, Epidemiology, and End Results (SEER) database and a retrospective cohort from Fujian Cancer Hospital. This model aimed to accurately identify high-risk individuals, thereby assisting clinicians in making more informed, personalized treatment decisions.
Method
Population selection
This retrospective study analyzed data from the SEER database using SEER*Stat software (version 8.4.0.1). The SEER database contains extensive records on patients with cancer from various regions across the United States21. A total of 1069 patients diagnosed with ACCHN between 2004 and 2015 were selected. The variables included age, gender, race, marital status, tumor site, AJCC seventh edition staging, TNM stage, treatment modalities (surgery, radiation, chemotherapy), lymph node dissection, survival duration, and status. Inclusion criteria were: (1) histologically confirmed ACCHN, (2) staging based on AJCC seventh edition, and (3) complete follow-up data. Tumor sites were categorized into six groups based on the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) site codes: (a) salivary gland; (b) pharynx and larynx; (c) gum and other mouth; (d) tongue; (e) oral cavity, including lip, floor of mouth, tonsil; and (f) nose, nasal cavity, and middle ear. Exclusion criteria included (a) incomplete clinical data, (b) unknown survival time, and (c) incomplete AJCC seventh edition staging. SEER is publicly accessible; therefore, Institutional Review Board approval was not required.
For external validation, 70 patients with ACCHN treated at Fujian Cancer Hospital between 2006 and 2019 were included, following identical criteria. Two oncologists re-staged these cases according to AJCC’s seventh edition. The study adhered to the Helsinki Declaration principles and was approved by the Institutional Review Board of Fujian Cancer Hospital.
Identification of prognostic factors
The Cox proportional hazards model was employed to determine the predictive power of each variable for OS to eliminate potential confounding variables. First, the Schoenfeld residual test verified the proportional hazard (PH) assumption. Univariate Cox analysis and Kaplan–Meier curves were utilized to identify prognostic factors. Variables with statistical significance (P < 0.05) in the univariate analysis were further analyzed in a multivariate Cox proportional hazards model to identify independent predictors of survival. The hazard ratios (HR) and 95% confidence intervals (CI) were recorded, and nonsignificant factors (P > 0.05) were excluded unless they held clinical significance.
Construction of the prognostic model and subgroup analysis
Independent variables were incorporated into the development of a prognostic model. A nomogram was constructed using the ‘rms’ package in R, designed to predict 5-, 7-, and 9-year OS rates in patients with ACCHN. The model’s accuracy and predictive consistency were evaluated using the concordance index (C-index) and receiver operating characteristic (ROC) curves. A higher C-index value indicated greater predictive accuracy. Moreover, decision curve analysis (DCA) was performed to evaluate the clinical utility of the nomogram in comparison to the seventh edition TNM staging system. Finally, patients were stratified into high-risk and low-risk subgroups based on the median risk score. Using the log-rank test, Kaplan–Meier survival curves were used to compare outcomes across validation and training cohorts.
Statistical analysis
The OS was measured as the time from ACCHN diagnosis to death or the last follow-up. Patients from our hospital were followed until October 2022. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) statistical software (version 26.0, International Business Machines Corporation, New York, USA) and R Software version 4.2.3. Statistical significance was defined using a two-sided P-value of 0.05.
Results
Patient and disease characteristics
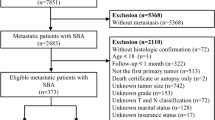
The SEER*Stat software identified 3671 patients diagnosed with ACC between 2004 and 2015. Of these, 2602 patients were excluded: 1214 cases were not diagnosed in the head and neck region, 1353 had incomplete AJCC seventh edition staging, and 35 lacked data on age, race, survival time, pathological diagnosis, or were identified via autopsy or death certificate. Finally, 1069 patients with ACCHN were included in the training cohort (Fig. S1).
In this training cohort, the median follow-up duration was 64 months, and the median patient age was 59 years (range: 11-94). Female patients accounted for 57.5% (615), while male patients comprised 42.5% (454). Half of the patients were younger than 60 years. The most frequently affected site was the salivary glands (51.1%), followed by the gum and other mouth (17.4%), nose, nasal cavity, and middle ear (14.8%), tongue (6.6%), pharynx and larynx (5.4%), and oral cavity (4.7%). According to the AJCC seventh edition staging, the distribution across stages I, II, III, and IV was 25.2%, 21.0%, 16.6%, and 37.3%, respectively. A total of 906 patients (84.8%) had no lymph node metastasis, while 7.7% (82) presented with distant metastases. Surgical treatment, radiotherapy, and chemotherapy were administered to 937 (87.7%), 765 (71.6%), and 159 (14.9%) patients, respectively. Detailed clinical characteristics are summarized in Table 1. Survival analysis revealed that the OS rates for patients with ACCHN at 5, 7, and 9 years were 71.7%, 62.0%, and 55.0%, respectively (Fig. S2A). Kaplan–Meier analysis demonstrated that better OS outcomes were associated with patients younger than 60 years, those with tumors in the gum and other mouth region, T1-2 tumor classification, negative lymph node metastasis, absence of distant metastasis, early-stage TNM classification, and those who underwent surgery without receiving chemotherapy (Fig. S3).
The validation cohort included 70 individuals with ACCHN from Fujian Cancer Hospital, with a median follow-up of 86 months. The median age in this cohort was 49 (range: 22-81). The most common tumor sites were the salivary glands (54.3%), followed by the nose, nasal cavity, and middle ear (17.1%), gum and other mouth (11.4%), pharynx and larynx (10%), tongue (4.3%), and oral cavity (2.9%). Table S1 outlines the clinical features of the validation cohort. Survival analysis indicated this cohort’s 5-, 7-, and 9-year OS rates as 82.3%, 67.3%, and 50.1%, respectively (Fig. S2B).
Screening for predictive factors
Several parameters, including age, gender, marital status, race, tumor site, treatment modality (surgery, radiation, chemotherapy), T stage, N stage, M stage, TNM stage, and lymph node dissection, were assessed to identify potential prognostic factors. A total of 13 variables were analyzed, all satisfying the PH assumption based on the Schoenfeld residual test (Fig. S4). The Cox proportional hazards model was applied to the training cohort to eliminate confounding variables, enabling evaluation of each factor’s predictive power for OS. Among the assessed variables, several factors emerged as significant risk indicators for long-term outcomes in individuals with ACCHN. Univariate analysis revealed that age (HR 2.084, 95% CI 1.692-2.569), tumor site (pharynx and larynx vs. salivary gland: HR 1.579, 95% CI 1.031-2.420; gum and other mouth vs. salivary gland: HR 0.866, 95% CI 0.639-1.174; tongue vs. salivary gland: HR 1.195, 95% CI 0.797-1.791; oral cavity vs. salivary gland: HR 1.619, 95% CI 1.049-2.500; nose, nasal cavity and middle ear vs. salivary gland: HR 1.754, 95% CI 1.344-2.289), surgery (yes vs. no: HR 0.259, 95% CI 0.205-0.327), chemotherapy (yes vs. no: HR 2.098, 95% CI 1.648-2.672), T stage (T2 vs. T1: HR 1.939, 95% CI 1.351-2.783; T3 vs. T1: HR 3.548, 95% CI 2.495-5.046; T4 vs. T1: HR 4.379, 95% CI 3.178-6.033), N stage (N1 vs. N0: HR 1.720, 95% CI 1.235-2.395; N2-N3 vs. N0: HR 4.589, 95% CI 3.444-6.115), M stage (M1 vs. M0: HR 4.679, 95% CI 3.584-6.109), and the overall TNM stage (II vs. I: HR 1.784, 95% CI 1.198-2.659; III vs. I: HR 2.441, 95% CI 1.635-3.643; IV vs. I: HR 5.532, 95% CI 3.978-7.695) significantly influenced the OS (Table 2). In the multivariate analysis, independent clinical predictors for OS included age (HR 2.330, 95% CI 1.874-2.896), tumor site (pharynx and larynx vs. salivary gland: HR 1.094, 95% CI 0.679-1.716; gum and other mouth vs. salivary gland: HR 0.839, 95% CI 0.609-1.155; tongue vs. salivary gland: HR 0.607, 95% CI 0.399-0.923; oral cavity vs. salivary gland: HR 1.616 95% CI 1.036-2.521; nose, nasal cavity, and middle ear vs. salivary gland: HR 1.349, 95% CI 1.011-1.800), surgery (yes vs. no: HR 0.370, 95% CI 0.282-0.484), N stage (N1 vs. N0: HR 1.315, 95% CI 0.911-1.899; N2-N3 vs. N0: HR 2.312, 95% CI 1.613-3.314), M stage (M1 vs. M0: HR 1.721, 95% CI 1.240-2.389), and TNM stage (II vs. I: HR 2.277, 95% CI 0.809-6.411; III vs. I: HR 1.395, 95% CI 0.558-3.491; IV vs. I: HR 3.341, 95% CI 1.299-8.592) (Table 2).
Nomogram construction and validation
Independent prognostic factors (including age, tumor site, surgery, N stage, M stage, and TNM stage) were incorporated into the nomogram (Fig. 1). The area under the curve (AUC) values for the primary cohort demonstrated the model’s predictive accuracy, which were 0.80, 0.80, and 0.82 for 5-, 7-, and 9-year OS predictions, respectively (Fig. 2A). Similarly, for the validation cohort, AUCs were 0.73, 0.84, and 0.83, respectively (Fig. 2B). The C-index values, 0.769 (95% CI [0.745-0.793]) for the training cohort and 0.741 (95% CI [0.649-0.833]) for the validation cohort, further confirmed the nomogram’s robust discriminatory power. The DCA demonstrated that the nomogram consistently outperformed the AJCC stage model across all groups, providing a higher net clinical benefit in predicting 5-, 7-, and 9-year OS rates (Fig. 3). Therefore, the nomogram was a valuable tool for generating clinically relevant predictions.

Nomograms for predicting 5-, 7-, and 9-year OS probabilities in patients with ACCHN assign a point score based on six key predictors. The total points accumulated by a patient are plotted on the “Total Points” axis to estimate the corresponding OS probabilities. The "linear predictor (lp)" reflects the relative weight of each variable, mapped to a corresponding line. The possibility of 5-, 7-, and 9-year OS is determined by drawing a line downward from the total points. ACCHN, adenoid cystic carcinoma of the head and neck; OS, overall survival.

ROC curves of the nomogram in predicting the prognosis at (A) 5-year, 7-year, and 9-year points in the training set, and (B) 5-year, 7-year, and 9-year points in the validation set. ROC, receiver operating characteristic curve; AUC, the area under the ROC curve.

DCA curves for the nomogram and AJCC stage model in predicting the prognosis of patients with ACCHN at (A) 5-year, (B) 7-year, and (C) 9-year points in the training cohort, and (D) 5-year, (E) 7-year, and (F) 9-year points in the validation cohort. The x-axis shows threshold probabilities, while the y-axis represents net benefits, calculated by adding true positives and subtracting false positives. DCA, decision curve analysis; ACCHN, adenoid cystic carcinoma of the head and neck; AJCC, American Joint Committee on Cancer.
Risk classification
The study employed a nomogram to calculate risk scores for every patient, followed by risk stratification. Participants were categorized into two groups based on median risk scores: low risk (scores ≤ 100) and high risk (scores > 100). Kaplan–Meier survival curves effectively differentiated between the two groups, with the high-risk group showing significantly poorer survival outcomes. The survival curves displayed a clear distinction in survival probabilities between high- and low-risk groups in the primary and validation cohorts (P < 0.0001), underscoring the nomogram’s capability in stratifying patients by risk level (Fig. 4).

Kaplan–Meier curves illustrating OS for patients in the low- and high-risk groups in the (A) training and (B) validation cohorts. OS, overall survival.
The subgroup analysis demonstrated substantial differences between the high- and low-risk groups. All subgroups, except for unoperated, stage II, and oral cavity subgroups, showed improved OS in low-risk patients compared to high-risk patients (Fig. 5). However, some subgroups, such as patients with metastases and N2-N3 stages, could not be thoroughly analyzed due to insufficient data in the low-risk group.

Subgroup analysis of OS for low- and high-risk patients. OS, overall survival.
Discussion
This retrospective study developed and validated a novel nomogram incorporating various clinical risk factors to provide individualized predictions for individuals with ACCHN. Stratifying patients into low- and high-risk groups significantly improved the prediction of OS. The nomogram outperformed the traditional TNM staging system in prognostic accuracy. This strategy may offer valuable clinical utility, guiding therapeutic decisions and individualized follow-up strategies for patients with ACCHN.
The ACCHN is recognized as a malignant neoplasm marked by aggressive growth, infiltration into surrounding tissues, PNI, and frequent local recurrences22. Moreover, distant metastasis significantly worsens the prognosis10. Accurately predicting clinical outcomes and survival in patients with ACC is crucial, which led to developing a prognostic model for those with ACCHN. A strong correlation is highlighted between tumor location and patient prognosis14,23. Those ACCs originating in the sinus cavity are associated with worse survival rates than those arising from the oral cavity or salivary glands24,25. Specifically, tumors in the minor salivary glands tend to have poorer outcomes than those in the major glands26, whereas ACC of the palate generally has a relatively favorable prognosis11,26. Consistent with previous findings, our study’s Kaplan–Meier survival curves indicated superior OS for ACCs in the gum and the palate. These observations were further confirmed through multivariate analysis.
Lymph node involvement has also been identified as a significant independent prognostic factor, as Ian Ganly et al. demonstrated23. Elective neck dissection did not improve survival outcomes27. Our study revealed that patients with ACC and lymph node metastases had considerably worse survival rates. Moreover, lower disease stages at presentation were associated with higher OS. In an earlier work by Ellington et al., the 5-, 10-, and 15-year survival rates across all stages were 90.34%, 79.88%, and 69.22%, respectively6. These findings underscore the importance of stringent screening and early detection to improve the prognosis of patients with ACCHN.
The primary approach to treating ACC is comprehensive surgical resection. However, the high risk of PNI, challenges in achieving negative margins, and elevated risks of recurrence and metastasis make achieving optimal outcomes difficult. Given these factors, the American Society of Clinical Oncology guidelines recommend postoperative radiotherapy (PORT) as a critical component of treatment for ACC28. The role of radiotherapy in improving OS remains controversial, although patients who receive it have greater odds of achieving favorable outcomes. A Danish study on head and neck cancers found no significant improvement in OS with PORT based on multivariate analysis29. Similarly, other studies suggest that outcomes in patients treated with surgery and adjuvant radiotherapy are comparable to those treated with surgery alone13. Although some research indicates that adding PORT to radical surgical resection enhances local tumor control, the benefit of PORT in extending OS in ACCHN remains inconclusive8,30. This uncertainty may be attributed to the invasive nature of ACC, its long-term survival even after recurrence or metastasis, and the difficulty in observing survival differences over extended periods. Chemotherapy possesses no noticeable impact on OS in patients with ACC and is generally reserved for palliative care in cases of symptomatic local recurrence or metastatic disease that are unsuitable for further surgery or radiation31. As the SEER dataset in this study lacks detailed chemotherapy information, subgroup analyses based on different chemotherapy regimens could not be conducted.
While TNM staging is widely used to guide treatment and predict prognosis, it does not fully account for the complex nature of tumor progression or the impact of other factors on patient survival. Nomograms have emerged as a more precise tool for estimating long-term outcomes in various malignancies, as they incorporate additional prognostic factors beyond TNM staging32,33. Our study demonstrates that the nomogram provides a superior net clinical benefit compared to AJCC staging by more effectively predicting 5-, 7-, and 9-year OS rates, as evidenced by DCA. Li et al. recently used a multivariate Cox proportional hazards model to identify independent predictors of OS in patients with early-onset ACCHN, including tumor size, chemotherapy, surgery, and stage, based on the SEER database34. Moreover, Ganly et al. constructed a comprehensive nomogram in 2015 using a multinational dataset of patients with ACCHN, incorporating variables such as age, gender, tumor site, PNI, margin status, clinical T stage, pathologic N stage, and M stage. Their nomogram predicted 10-year OS, with a C-index of 0.71, and was validated using data from 99 patients across two institutions23. The present study validated the nomogram’s performance using the C-index, ROC, and DCA curves, demonstrating its robust discrimination and consistency. While the previous research by Ganly et al. achieved external validation with high C-indices, their cohort was limited to major salivary gland cancers. The multicenter dataset likely mitigated some variability in ACC management strategies across institutions; however, it may reduce its precision in predicting survival outcomes for the Chinese population. Furthermore, these prognostic models lack thorough external validation. Therefore, Cox regression analysis was utilized to assess OS predictors, and the nomogram was tested with Chinese cohorts for external validation. The nomogram demonstrated superior predictive accuracy and clinical relevance for ACCHN in both cohorts, with risk stratification effectively differentiating patient groups based on mortality risk.
While this study provides valuable insights into ACCHN prognostic models, it has limitations. First, the retrospective study design introduces potential biases despite strict inclusion criteria. Moreover, the SEER database lacks critical data points, such as PNI, alcohol and tobacco use, surgical margins, specific chemotherapy regimens, and radiotherapy doses. Furthermore, the small sample size in the validation set may bias the results, underscoring the need for further research to confirm the nomogram’s clinical utility before broad application.
Conclusion
A nomogram was developed for predicting OS in patients with ACCHN, offering a valuable tool for prognostic guidance and personalized treatment planning in clinical settings.
Data availability
The training dataset used in this study was obtained from the Surveillance, Epidemiology, and End Results Program (SEER) database (https://seer.cancer.gov/data/access.html). The validation dataset was sourced from clinical records at the corresponding author’s institution. Detailed information or requests for access to either dataset can be obtained by contacting the corresponding author, subject to reasonable request.
References
Coca-Pelaz, A. et al. Adenoid cystic carcinoma of the head and neck – An update. Oral Oncol. 51, 652–661 (2015).
Nightingale, J., Lum, B., Ladwa, R., Simpson, F. & Panizza, B. Adenoid cystic carcinoma: A review of clinical features, treatment targets and advances in improving the immune response to monoclonal antibody therapy. Biochim. et Biophys. Acta (BBA) Rev. Cancer 1875, 188523 (2021).
Fang, Y. et al. Current opinions on diagnosis and treatment of adenoid cystic carcinoma. Oral Oncol. 130, 105945 (2022).
Barrett, A. W. & Speight, P. M. Perineural invasion in adenoid cystic carcinoma of the salivary glands: A valid prognostic indicator?. Oral Oncol. 45, 936–940 (2009).
Dewenter, I., Otto, S., Kakoschke, T. K., Smolka, W. & Obermeier, K. T. Recent advances, systemic therapy, and molecular targets in adenoid cystic carcinoma of the head and neck. JCM 12, 1463 (2023).
Ellington, C. L. et al. Adenoid cystic carcinoma of the head and neck: Incidence and survival trends based on 1973–2007 surveillance, epidemiology, and end results data. Cancer 118, 4444–4451 (2012).
Lloyd, S., Yu, J. B., Wilson, L. D. & Decker, R. H. Determinants and patterns of survival in adenoid cystic carcinoma of the head and neck, including an analysis of adjuvant radiation therapy. Am. J. Clin. Oncol. 34, 76–81 (2011).
Shen, C., Xu, T., Huang, C., Hu, C. & He, S. Treatment outcomes and prognostic features in adenoid cystic carcinoma originated from the head and neck. Oral Oncol. 48, 445–449 (2012).
Oplatek, A., Ozer, E., Agrawal, A., Bapna, S. & Schuller, D. E. Patterns of recurrence and survival of head and neck adenoid cystic carcinoma after definitive resection. The Laryngoscope 120, 65–70 (2010).
Jang, S., Patel, P. N., Kimple, R. J. & McCulloch, T. M. Clinical outcomes and prognostic factors of adenoid cystic carcinoma of the head and neck. Anticancer Res. 37(6), 3045–3052 (2017).
Huang, M. et al. Factors influencing survival rate in adenoid cystic carcinoma of the salivary glands. Int. J. Oral Maxillofac. Surg. 26, 435–439 (1997).
Chen, A. M. et al. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: Prognostic features of recurrence. Int. J. Radiat. Oncol. Biol. Phys. 66, 152–1594 (2006).
Van Weert, S. et al. Adenoid cystic carcinoma of the head and neck: A single-center analysis of 105 consecutive cases over a 30-year period. Oral Oncol. 49, 824–829 (2013).
Khan, A. J. et al. Adenoid cystic carcinoma: A retrospective clinical review. Intl. J. Cancer 96, 149–158 (2001).
Lombardi, D. et al. Baseline prognostic factors affecting survival in recurrent and/or metastatic salivary gland adenoid cystic carcinoma. Oral Oncol. 126, 105764 (2022).
Mu, X. et al. Prognostic nomogram for adenoid cystic carcinoma in different anatomic sites. Head Neck 43, 48–59 (2021).
Cantù, G. Adenoid cystic carcinoma. An indolent but aggressive tumour. Part B: Treatment and prognosis. Acta Otorhinolaryngol. Ital. 41, 296–307 (2021).
Bakst, R. L. et al. Perineural invasion and perineural tumor spread in head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 103, 1109–1124 (2019).
Ko, J. J., Siever, J. E., Hao, D., Simpson, R. & Lau, H. Y. Adenoid cystic carcinoma of head and neck: Clinical predictors of outcome from a Canadian centre. Curr. Oncol. 23, 26–33 (2016).
Takebayashi, S. et al. Adenoid cystic carcinoma of the head and neck: A retrospective multicenter study. Acta Oto-Laryngol. 138, 73–79 (2018).
Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/.
Moskaluk, C. A. Adenoid cystic carcinoma: Clinical and molecular features. Head Neck Pathol. 7, 17–22 (2013).
Ganly, I. et al. Nomograms for predicting survival and recurrence in patients with adenoid cystic carcinoma. An international collaborative study. Eur. J. Cancer 51, 2768–2776 (2015).
Marcinow, A. et al. Clinicopathologic predictors of recurrence and overall survival in adenoid cystic carcinoma of the head and neck: A single institutional experience at a tertiary care center. Head Neck 36, 1705–1711 (2014).
Choi, Y. et al. Clinical characteristics and prognostic factors of adenoid cystic carcinoma of the head and neck. The Laryngoscope 123, 1430–1438 (2013).
Nascimento, A. G., Amaral, A. L. P., Prado, L. A. F., Kligerman, J. & Silveira, T. R. P. Adenoid cystic carcinoma of salivary glands. A study of 61 cases with clinicopathologic correlation. Cancer 57, 312–319 (1986).
Amit, M. et al. Elective neck dissection in patients with head and neck adenoid cystic carcinoma: An international collaborative study. Ann. Surg. Oncol. 22, 1353–1359 (2015).
Pfister, D. G. et al. Head and neck cancers, version 2.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 18, 873–898 (2020).
Bjørndal, K. et al. Salivary adenoid cystic carcinoma in Denmark 1990–2005: Outcome and independent prognostic factors including the benefit of radiotherapy. Results of the Danish Head and Neck Cancer Group (DAHANCA). Oral Oncol. 51, 1138–1142 (2015).
Choi, S. H. et al. Role of postoperative radiotherapy in resected adenoid cystic carcinoma of the head and neck. Radiat. Oncol. 17, 197 (2022).
Laurie, S. A., Ho, A. L., Fury, M. G., Sherman, E. & Pfister, D. G. Systemic therapy in the management of metastatic or locally recurrent adenoid cystic carcinoma of the salivary glands: A systematic review. Lancet Oncol. 12, 815–824 (2011).
Wang, S. et al. Development and validation of a nomogram prognostic model for SCLC patients. J. Thoracic Oncol. 13, 1338–1348 (2018).
Huang, X. et al. Survival nomogram for young breast cancer patients based on the SEER database and an external validation cohort. Ann. Surg. Oncol. 29, 5772–5781 (2022).
Dai, L., Zhang, S. & Wu, Y. Prognostic model and nomogram for early-onset adenoid cystic carcinoma of head and neck: A retrospective SEER-based analysis. Technol. Cancer Res. Treat 22, 153303382311630 (2023).
Funding
This work was supported by the grants of Science and Technology Program of Fujian Province, China (2018Y2003); Fujian Provincial Clinical Research Center for Cancer Radiotherapy and Immunotherapy (2020Y2012); Supported by the National Clinical Key Specialty Construction Program (2021); Fujian Clinical Research Center for Radiation and Therapy of Digestive, Respiratory and Genitourinary Malignancies; National Natural Science Foundation of China (82072986); Major Research Projects for Young and Middle-aged Researchers of Fujian Provincial Health Commission (2021ZQNZD010); Science and Technology Pilot Program of Fujian Province, China (2021Y0053); Wu Jieping Medical Foundation (320.6750.2021-01-27); Joint Funds for the Innovation of Science and Technology, Fujian province (2021Y9196); High-level Talent Training Program of Fujian Cancer Hospital (2022YNG07); Innovative Medicine Subject of Fujian Provincial Health Commission, China (2021CXA029); and Natural Science Foundation of Fujian province (2023J011267).
Author information
Authors and Affiliations
Contributions
Yuhui Pan: Conceptualization, Writing-Original draft preparation, Writing-Reviewing and Editing. Libin Zhang: Conceptualization, Writing-Original draft preparation, Writing-Reviewing and Editing. Siqi Xu: Methodology, Data curation, Software. Ying Li: Methodology, Data curation, Software. Zongwei Huang: Investigation, Supervision, Validation. Chao Li: Investigation, Supervision, Validation. Sunqin Cai: Formal analysis, Resources, Visualization. Zihan Chen: Formal analysis, Resources, Visualization. Jinghua Lai: Formal analysis, Resources, Visualization. Jun Lu: Funding acquisition, Project administration. Sufang Qiu: Funding acquisition, Project administration.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study was conducted in compliance with the principles of the Declaration of Helsinki. The Ethical Review Committee at our center approved this study.
Informed consent
Informed consent was waived by the Ethical Review Committee at our center due to retrospective nature.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pan, Y., Zhang, L., Xu, S. et al. Development and validation of a nomogram for predicting overall survival of head and neck adenoid cystic carcinoma. Sci Rep 14, 26406 (2024). https://doi.org/10.1038/s41598-024-77322-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-77322-9
