
Abstract
This study aimed to explore the association between two major etiologies of paralysis and the in-hospital outcomes of patients with acute myocardial infarction (AMI) who had undergone percutaneous coronary intervention (PCI). We retrieved AMI patients undergoing PCI from the National Inpatient Sample (2003–2015) and divided them into without paralysis, spinal cord injury (SCI) paralysis, and stroke paralysis. Paralysis’ impact on hospital outcomes was explored using multivariate regression. Interaction analysis was used to investigate the sex differences. We observed the temporal trends of in-hospital outcomes from 2003 to 2015 by paralysis etiology. A total of 2,151,994 AMI cases were identified, with 6,711 SCI paralysis and 8,322 stroke paralysis. Compared to patients without paralysis, patients with SCI but not stroke paralysis had increased rates of in-hospital mortality (odds ratio [OR]: 2.8, 95% confidence interval [CI]: 1.9–3.9), cardiogenic shock (OR: 2.4, 95% CI: 1.8–3.3). Furthermore, this positive association between SCI and in-hospital adverse outcomes is more significant in females than males. In conclusion, SCI paralysis is associated with an increased risk of in-hospital mortality, cardiogenic shock in patients with AMI undergoing PCI, especially in females. These disparities lasted from 2003 to 2015.
Similar content being viewed by others

Introduction
According to the 2013 U.S. Paralysis Prevalence & Health Disparities Survey, almost 5.4 million persons in the United States (US) have paralysis, representing a large segment of the U.S. population1. Stroke and spinal cord injury (SCI) are the two leading causes of paralysis1. Compared to healthy adults, paralyzed patients have a high prevalence of conventional cardiovascular risk factors. However, traditional cardiovascular risk factors greatly underestimate the risk of cardiovascular morbidity and mortality in paralyzed individuals2. Cardiovascular diseases constitute 26.7% of all-cause mortality and are responsible for the greatest proportion of morbidity and mortality in the paralyzed population3. Patients with paralysis now have a longer life expectancy due to advancements in medical care and rehabilitation4. Moreover, prompt percutaneous coronary intervention (PCI) is currently considered the recommended reperfusion therapy for acute myocardial infarction (AMI)5. Using the New York State Inpatient Database (NY-SID) from 2007 to 2013, Dai and colleagues reported that acute myocardial infarction patients with concomitant paraplegia were less likely to receive revascularization therapy and had higher in-hospital mortality6.
However, the literature on AMI clinical outcomes among paralyzed patients remains limited, and even previous observational studies did not divide patients with paralysis into those with and without cerebrovascular disease. Recommendations derived from published clinical studies of AMI may not apply directly to patients with paralysis. Despite the growing focus on risk modification and primary prevention of coronary heart disease in patients with paralysis, its association with the in-hospital outcomes and the temporal trends of patients with AMI undergoing PCI remain unknown.
In the present study, using National Inpatient Sample (NIS) from 2003 to 2015, we examined the association between two major etiologies of paralysis and the in-hospital outcomes of patients with AMI who had undergone PCI.
Materials and methods
Study population and outcome measures
The NIS is the United States’ largest hospital inpatient stay database, which contains data from all payers. The NIS contains discharge data from a 20% stratified sample of community hospitals and is part of the Agency for Healthcare Cost and Utilization Project (HCUP)7. Based on the HCUP-NIS recommendations, survey methodologies were employed to generate national estimates using discharge weights (DISCWT, the discharge-level weight on the HCUP nationwide databases), clusters (HOSP_NIS, NIS hospital number), and strata (NIS_STRATUM, a four-digit stratum identifier used to post-stratify hospitals for the calculation of universe and frame weights) from the HCUP-NIS database. To account for the 2012 HCUP-NIS re-design, trend weights were utilized to re-balance samples from 2000 to 2011. The 2012 re-design of the HCUP-NIS involved sampling 20% of the national patient-level sample, in contrast to the previous years of 2000–2011, where 100% of discharges were sampled from 20% of hospitals8. The database includes information on patient demographics, primary payer, hospital features, principal diagnosis, secondary diagnoses (up to 24 h), and procedural diagnoses7. The HCUP-NIS doesn’t gather information on specific patients but does collect all admission-related data.
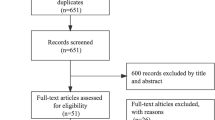
Using the NIS data from 2003 to 2015, we conducted a cohort study of patient admissions (≥ 18 years) with AMI in the primary diagnosis (International Classification of Diseases 9.0 Clinical Modification [ICD-9-CM] 410.x) who underwent PCI in the primary procedure ([ICD-9-CM] 360.x). We excluded cases if critical variables for risk stratification or outcomes were lacking. For analysis, we split the patients into two primary groups, with and without paralysis, based on paralysis status. Additionally, patients with AMI with paralysis were further identified using the ICD-9-CM procedure and Clinical Classification Software (CCS) codes and categorized as spinal cord injury (SCI) paralysis (CCS diagnosis code 82) or stroke paralysis ([ICD-9-CM] 438.20–438.53). The ICD-9-CM CCS is a scheme for categorizing illnesses and procedures that can be utilized in various projects that analyze data on diagnoses and procedures. Figure 1 depicts a study population flow chart highlighting the inclusion and exclusion criteria, while the ICD-9 codes that were used are listed in Supplementary Table S1.

Flow diagram of study population selection. Weighted selection of 2,843,915 patients aged ≥ 18 years with acute myocardial infarction (AMI) undergoing percutaneous coronary intervention (PCI) from the National Inpatient Sample database. A total of 2,151,994 patients were selected after excluding missing data. The selected patients were separated into the AMI undergoing PCI procedure non-paralysis group (2,136,961 patients) and the AMI undergoing PCI procedure paralysis group (15,033 patients). The paralysis group was further divided into the spinal cord injury (SCI) paralysis group (6,711 patients) and the stroke paralysis group (8,322 patients).
We described the temporal changes in in-hospital mortality over the study period according to paralysis status. The primary outcome of this study was the in-hospital mortality rate. The secondary outcomes included cardiogenic shock, urinary tract infection, acute kidney injury, length of hospital stay, and number of procedures during hospitalization. In addition, the NIS database captures short-term perioperative complications. Thus, these outcomes are perioperative outcomes. The HCUP reports baseline characteristics and clinical outcomes using the corresponding ICD-9-CM Revision codes and CCS.
Statistical analyses
In compliance with the HCUP requirements for using the NIS database, all analyses were conducted using weighted samples for national estimates. The survey-weighted chi-square test was used to compare categorical variables, which were presented as the survey-weighted percentage (95% confidence interval [CI]). The survey-weighted mean (95% CI) was used to compare continuous variables using survey-weighted linear regression. The effect sizes are presented as odds ratios (ORs) and 95% CIs. Associations were considered significant if the p-value was < 0.05. We used the statistical software package R 3.4.3 (available at: http://www.R-project.org; R Foundation for Statistical Computing, Vienna, Austria) and Empower-Stats 4.1 (X&Y Solutions, Inc, Boston, Mass) for all statistical analyses.
We conducted multivariate regression analysis for in-hospital outcomes in three patient groups and included statistically significant variables in univariate analysis. To reduce bias from the observed covariates, we used a 1:1 case-control matching (CCM) between the two major etiologies of paralysis groups to construct matched cohorts based on age, sex, race, median household income, primary expected payer, smoking status, AMI type, elective admissions, previous coronary artery bypass graft and Elixhauser classification system (in-hospital comorbidities were assessed using the Elixhauser classification system9). To further analyze the association of different paralysis types with in-hospital outcomes, a secondary model was performed for in-hospital outcomes, adjusting for baseline demographics such as age and sex, along with smoking, hypertension, hyperlipidemia, diabetes, and other comorbidities. These confounding factors were selected based on > 10% differences in association with or effect estimates on the outcomes of interest. Furthermore, the associations did not change markedly after adjusting for these confounding factors in the multivariable regression analyses. In addition, we used multiple imputation (MI) based on five replications and a chained equation approach in the R MI procedure to account for missing data for other covariates, such as age, race, and sex, to avoid the reduced power of statistical tests and the bias associated with direct exclusion of missing values. We also conducted sensitivity analyses among patients with paralysis, comparing males and females to evaluate the influence of sex on these associations within the outcome variables. The temporal trends of in-hospital outcomes were also studied among the three groups.
Results
Study population
From January 2003 to September 2015, 15,033 (0.70%) of the 2,151,994 patients with AMI who met all of the inclusion criteria and none of the exclusion criteria were included in the final analysis, as shown in Fig. 1. Table 1 displays the demographic characteristics of the weighted population. Among them, 6,711 (0.31%) were diagnosed with SCI paralysis, and 8,322 (0.39%) were diagnosed with stroke paralysis. Stroke patients with paralysis were older than those with SCI and those without paralysis. Patients with SCI were more likely to be male and Caucasian than stroke patients with paralysis. Notably, patients with SCI were less likely to have traditional coronary risk factors, including smoking and chronic disease histories, but had a greater risk of diabetes than stroke patients with paralysis (all p < 0.001). In addition, we analyzed the crude association of paralysis with baseline demographic and clinical characteristics (Supplementary Table S2). Overall, the results in univariate analyses were consistent with those in Table 1 above.
In-hospital outcomes
The in-hospital outcomes among the three groups are outlined in Table 2. Patients with SCI paralysis had the highest in-hospital mortality (6.4%), followed by patients with stroke paralysis (3.2%) and then finally by patients without paralysis (2.1%, p < 0.001). Additionally, patients with SCI paralysis had the most significant risk of cardiogenic shock, urinary tract infections, and extended hospitalization among the three groups (all p < 0.001).

In-hospital mortality and adverse outcomes in the multivariate regression analysis in 1:1 case-control matching model. (A) Adjusted odds ratios for in-hospital mortality and outcomes. (B) Adjusted β value for LOS and NPR; represented as odds ratio and β value (95% confidence interval), adjusted for age, sex, race, primary payer, socioeconomic status, smoking, previous CABG, and Elixhauser Comorbidity Index.
After 1:1 CCM, adjusting for demographics and Elixhauser Comorbidity Index (Fig. 2), AMI patients with SCI but not stroke paralysis had an increased risk of in-hospital mortality (OR: 2.8, 95% CI: 1.9–3.9) and cardiogenic shock (OR: 2.4, 95% CI: 1.8–3.3) compared to those without paralysis. Meanwhile, the risk of acute kidney injury and urinary tract infection were increased both in the SCI and stroke paralysis patients. In addition, we found an increased risk of acute kidney injury in SCI paralysis (OR: 2.1, 95% CI: 1.7–2.7) and stroke paralysis (OR: 2.3, 95% CI: 1.8–2.9). Notably, the adjusted odds of urinary tract infection were significantly higher in SCI paralysis patients (OR: 3.1, 95% CI: 2.3–4.0) and stroke patients with paralysis (OR: 2.5, 95% CI: 1.9–3.2). Patients with SCI paralysis (β: 3.1, 95% CI: 2.6–3.6) and stroke paralysis (β: 1.1, 95% CI: 0.6–1.6) had a longer length of hospital stay than patients without paralysis. Additionally, the number of procedures slightly decreased in patients with SCI paralysis (β: 0.9, 95% CI: 0.7–1.1) and stroke paralysis (β: 0.5, 95% CI: 0.4–0.7). Again, the results of the analyses were similar for mismatches and matches (Supplementary Fig. 1).
Sensitivity analyses by sex and AMI type
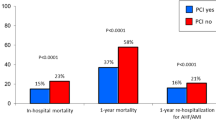
We conducted a sex-stratified analysis of outcomes in patients with SCI paralysis undergoing PCI. Female SCI patients exhibited a markedly elevated risk of in-hospital mortality (OR: 3.8, 95% CI: 2.7–5.3), while the risk increase in male patients was not statistically significant (OR: 1.2, 95% CI: 0.9–1.7). Our findings revealed a significant sex interaction in in-hospital mortality (p < 0.001). This pronounced sex disparity suggests that SCI had a more substantial impact on in-hospital mortality for female patients (Table 3).
To assess the robustness of our primary findings, we conducted a series of sensitivity analyses, including stratified analyses based on sex and type of myocardial infarction. The results demonstrated that both SCI and stroke paralysis were associated with higher risks of adverse outcomes across different subgroups. These stratified analysis results are consistent with our main analysis, further confirming the reliability of our findings across different subgroups. The observed associations in various strata suggest that the increased risks associated with paralysis are robust across different patient characteristics (Supplementary Table S3). In sensitivity analyses, we found that females were older and had more comorbidities than males (Supplementary Table S4).
Temporal trends
The temporal trends of in-hospital mortality and outcomes are shown in Fig. 3. Over the 2003–2015 study period, the SCI paralysis group remained consistently higher than the without paralysis and stroke paralysis groups in terms of in-hospital mortality and outcomes, with a consistent uptrend during the study period, as shown in Fig. 4. The annual in-hospital mortality rates for non-paralyzed patients who had undergone PCI for AMI from 2003 to 2015 remained low, ranging from 1.53 to 3.01%. The rate of in-hospital mortality among the SCI paralysis group increased remarkably from 11.43% in 2003 to 9.49% in 2015. The cardiogenic shock rate increased over time, and this trend was consistent

Temporal trend of in-hospital mortality and outcomes. The SCI paralysis group showed a fluctuating trend in the risk of in-hospital mortality and urinary tract infection; however, this was still greater than that of the without paralysis and stroke paralysis groups. (A) The in-hospital mortality in the SCI paralysis group (11.43% in 2003, 13.95% in 2006, and 9.49% in 2015). (B) In the SCI paralysis group, the cardiogenic shock rate (2.86% and 16.79% in 2003 and 2015, respectively) increased over time and was greater than that in the group without paralysis and the group with stroke paralysis. (C) In the SCI paralysis group, the acute renal injury rate steadily increased (0% and 28.47% in 2003 and 2015, respectively) and was higher than the rates in the without-paralysis and stroke-paralysis groups. (D) In the SCI paralysis group, the urinary tract infection rate had a fluctuating trend (14.29% in 2003, 29.27% in 2008, and 11.68% in 2015).

Graph displaying the study findings. The patients with AMI and spinal cord injury (SCI) paralysis who underwent PCI showed increased in-hospital mortality, cardiogenic shock, acute kidney injury, and urinary tract infection compared to patients with AMI and stroke paralysis who underwent PCI and patients without paralysis.
across three groups. In the SCI paralysis group, the proportion of cardiogenic shock increased from 2.86% in 2003 to 16.79% in 2015. The acute kidney injury rate increased steadily in both the SCI paralysis and without paralysis groups (0% and 28.47% vs. 3.81% and 9.43% in 2003–2015). In terms of urinary tract infection, a similar trend was observed in patients with SCI paralysis who underwent PCI (14.29% in 2003 to 11.68% in 2015), which showed an initial upward trend, reached a peak in 2008 (29.27%), and then showed a downward trend.
Discussion
This analysis involved a larger nationwide sample of patients with AMI who had been hospitalized and underwent PCI. We documented three major findings. First, in the US, between 2003 and 2015, patients with paralysis and AMI who underwent PCI with SCI but not stroke paralysis had a higher risk of in-hospital mortality than the group without paralysis. The rates of cardiogenic shock, acute kidney injury, urinary tract infection, and length of hospital stay during hospitalization were all higher in the SCI paralysis group. Second, female patients with paralysis and AMI may be more vulnerable to adverse in-hospital outcomes, especially in-hospital mortality. Finally, regardless of etiology, we observed a temporal increase in in-hospital mortality in patients with paralysis and AMI who underwent PCI.
As far as we know, this is the first study to address the association between paralysis of different etiologies and the in-hospital outcomes of patients with AMI who underwent PCI. Our findings showed that patients with AMI with SCI but not stroke paralysis had a greater risk of in-hospital mortality during AMI hospitalization, even after PCI. Several studies have identified risk factors that are unique to individuals with paralysis, including obesity, insulin resistance, diabetes, deconditioning, and inflammation, compared to the general population10,11. Furthermore, traditional cardiovascular risk factors strongly underestimate the incidence of cardiovascular morbidity and mortality in paralyzed people2. As a result, patients with paralysis and AMI will experience more adverse clinical cardiovascular events. We extend these findings to suggest that the SCI paralysis group is associated with worse in-hospital outcomes with comorbid AMI, even if they received early PCI, than patients with AMI with stroke paralysis, which has not been previously documented. This is especially noteworthy because, while patients with stroke paralysis and AMI who underwent PCI had more severe traditional coronary risk factors (Table 1), the SCI paralysis group had a worse prognosis and a longer hospital stay; this difference remained after adjusting for confounders using multiple regression analysis. This finding has the potential to greatly improve our capacity for assessing disease severity. These results may indicate a trend in which the disabling effects of cerebrovascular disease are reversible, whereas most SCIs are caused by irreversible trauma12. Additionally, a large percentage of patients with paralysis, mostly with SCI1, are admitted in an emergency setting, reflecting the clinical acuity and severity of their disease13.
Our results also indicated that the risk of urinary tract infection was higher in the SCI paralysis group, which has not been explored in most previous studies. Indeed, clinicians tend to pay little attention to urinary tract infections after PCI. However, lower-urinary tract dysfunction caused by SCI frequently results in recurring urinary tract infection and, eventually, renal failure, which is one of the leading causes of morbidity and mortality in patients with SCI14. Hence, severe infections can also lead to increased in-hospital mortality and burden of complications, as well as longer hospital stays. Currently, patients with SCI paralysis, as opposed to stroke patients with paralysis, lack effective pharmacological treatments. Taken together, all of these factors contribute to increased mortality in patients with SCI paralysis. In summary, we found that even after PCI, the in-hospital mortality rates remained significantly increased for patients with SCI paralysis with AMI.
Another important finding is that paralyzed female patients with AMI who underwent PCI may be more vulnerable to adverse in-hospital outcomes, including higher mortality and a longer length of hospital stay, regardless of the causes of paralysis. Previous research has found that female sex is an independent predictor of post-PCI adverse events, which are associated with increased mortality and a longer hospital stay15,16. This difference was considerably more obvious in patients with AMI who were paralyzed. Moreover, females are more likely than males to be wounded at an older age, and paralyzed females may reach menopause earlier than their able-bodied counterparts17,18. The reasons behind this observation may be multifactorial, including cardiovascular disease risk factors, autonomous dysfunction, dyslipidemia, blood pressure dysregulation, physical inactivity, and long-term inflammatory stress19,20. Studies focused solely on females are rare; thus, females have been underrepresented in cardiovascular clinical studies21.
Consequently, unexpected outcomes related to sex differences may occur when females receive treatment based on data from clinical studies mostly involving males22,23. Compounding this, socioeconomic disadvantages often observed in this population also contribute to increased mortality in females24. Therefore, female patients with paralysis with AMI are more likely to endure adverse in-hospital outcomes.
Lastly, we also found that the in-hospital mortality rates for patients with paralysis with AMI, regardless of etiology, have increased, and the overall trend is higher than for those without paralysis between 2003 and 2015. In a large study25 from the NIS database, with advances in medical treatment, the annual PCI volume decreased in the US between 2003 and 2016. However, the percentage of PCI for AMI has increased and remained relatively stable in terms of in-hospital mortality. Additionally, it is worth noting that the prevalence of myocardial infarction in paralyzed individuals is increasing annually26. The trend of in-hospital mortality is consistent with the results of our study. Although PCI has been shown to decrease mortality in patients with AMI, the increase in the incidence of paralysis over time might continue after population density increases, population aging, and increased use of vehicles, while the total number of cases also increased, which is consistent with our findings. Moreover, autonomic dysreflexia, which is highly prevalent in patients with paralysis, causes blood pressure disorders, leading to perioperative hemodynamic instability and unpredictability following cardiac surgery27,28,29,30. These paralysis-related anomalies complicate the risk of PCI, and in-hospital mortality increases over time after PCI. This trend may also be related to the increased frequency of paralysis diagnoses owing to the Paralysis Act, which was authorized by the U.S. Congress in 200931.
In the current study, we first explored the association between the two major etiologies of paralysis and the in-hospital outcomes of patients with AMI who underwent PCI. Our results suggest that more attention should be paid to SCI paralysis but not stroke patients with paralysis when referring to AMI. Furthermore, female patients with paralysis are more vulnerable in this clinical setting. This in-hospital outcome disparity in paralysis lasted from 2003 to 2015.
Strengths and limitations
This study has several notable strengths. First, we divided patients into SCI and stroke paralysis according to their etiologies, which is novel compared to the approach taken in previous studies. Second, we explored urinary tract infection as an in-hospital outcome in this AMI patient cohort. Finally, we conducted this study using data from a national representative database with a large sample size.
However, our research still has a few limitations that warrant discussion. First, the NIS data are derived from national health databases and may not accurately reflect the severity or duration of the paralysis. Moreover, the NIS database is the all-payer inpatient database of hospital discharge records. We can’t precisely define the timing of events such as urinary tract infection, which may occur before or after the admission day. Third, this study only adds data during the index event (in-hospital data). Hence, it is possible that a given patient, if admitted and readmitted multiple times during this study period, may be counted more than once. Additionally, the observational nature of this study and the lack of randomization raise the possibility of selection bias.
Conclusion
SCI paralysis is associated with an increased risk of in-hospital mortality, cardiogenic shock, acute kidney injury, and urinary tract infection in patients with AMI undergoing PCI, and prolongs the length of hospital stay, especially in females. These disparities lasted from 2003 to 2015 (Fig. 4). More attention should be paid to patients with SCI paralysis when comorbid with AMI to conduct PCI promptly.
Data availability
The data supporting this study’s findings are available from the NIS databases. Specifically, the researchers purchased the NIS databases. Furthermore, the data sources are publicly accessible online (URL: https://www.hcup-us.ahrq.gov/nisoverview.jsp). The raw data supporting the conclusions of this article will be made available by the authors without undue reservation. All other supporting data in this study are available on request from Haohong Qi, MD, and Guangzhi Cong, Ph.D.
References
Armour, B. S., Courtney-Long, E. A., Fox, M. H., Fredine, H. & Cahill, A. Prevalence and causes of Paralysis-United States, 2013. Am. J. Public. Health. 106, 1855–1857. https://doi.org/10.2105/ajph.2016.303270 (2016).
Barton, T. J. et al. Traditional Cardiovascular Risk factors strongly underestimate the 5-Year occurrence of Cardiovascular Morbidity and Mortality in spinal cord injured individuals. Arch. Phys. Med. Rehabil. 102, 27–34. https://doi.org/10.1016/j.apmr.2020.07.013 (2021).
Osterthun, R., Post, M. W., van Asbeck, F. W., van Leeuwen, C. M. & van Koppenhagen, C. F. Causes of death following spinal cord injury during inpatient rehabilitation and the first five years after discharge. A Dutch cohort study. Spinal Cord. 52, 483–488. https://doi.org/10.1038/sc.2014.28 (2014).
Middleton, J. W. et al. Life expectancy after spinal cord injury: a 50-year study. Spinal Cord. 50, 803–811. https://doi.org/10.1038/sc.2012.55 (2012).
Ibánez, B. et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Rev. Esp. Cardiol. (Engl Ed). 70, 1082. https://doi.org/10.1016/j.rec.2017.11.010 (2017).
Lu, S. F., Lu, L. X., Smith, S. C. Jr. & Dai, X. Acute myocardial infarction in patients with paraplegia: characteristics, management, and outcomes. Am. J. Med. 131, 574. .e571-574.e511 (2018).
Introduction to the HCUP Nationwide Inpatient Sample. ). (2009). http://www.hcup-us.ahrq.gov/db/nation/nis/NIS_2009_INTRODUCTION.pdf.. Accessed January 18, 2023.
Chatterjee, K. et al. 2009–2013) for Palliative Care utilization for patients receiving prolonged mechanical ventilation. Crit. Care Med. 46, 1230–1237. https://doi.org/10.1097/ccm.0000000000003182 (2018).
Elixhauser, A., Steiner, C., Harris, D. R. & Coffey, R. M. Comorbidity measures for use with administrative data. Med. Care. 36, 8–27. https://doi.org/10.1097/00005650-199801000-00004 (1998).
Bauman, W. A. & Spungen, A. M. Coronary heart disease in individuals with spinal cord injury: assessment of risk factors. Spinal Cord. 46, 466–476. https://doi.org/10.1038/sj.sc.3102161 (2008).
Calvo-Infante, F. Cardiovascular complications associated with spinal cord injury. J. Acute Disease. 7, 139–144. https://doi.org/10.4103/2221-6189.241006 (2018).
Fox, M. H., Krahn, G. L., Sinclair, L. B. & Cahill, A. Using the international classification of functioning, disability and health to expand understanding of paralysis in the United States through improved surveillance. Disabil. Health J. 8, 457–463. https://doi.org/10.1016/j.dhjo.2015.03.002 (2015).
Jain, N. B. et al. Traumatic spinal cord injury in the United States, 1993–2012. Jama. 313, 2236–2243. https://doi.org/10.1001/jama.2015.6250 (2015).
Deng, L. et al. Locomotor Exercise enhances Supraspinal Control of Lower-urinary-tract activity to improve micturition function after Contusive spinal-cord Injury. Cells. 11 https://doi.org/10.3390/cells11091398 (2022).
Ndrepepa, G. et al. Bleeding after percutaneous coronary intervention in women and men matched for age, body mass index, and type of antithrombotic therapy. Am. Heart J. 166, 534–540. https://doi.org/10.1016/j.ahj.2013.07.006 (2013).
Regitz-Zagrosek, V. et al. Gender in cardiovascular diseases: impact on clinical manifestations, management, and outcomes. Eur. Heart J. 37, 24–34. https://doi.org/10.1093/eurheartj/ehv598 (2016).
Raguindin, P. F., Muka, T. & Glisic, M. Sex and gender gap in spinal cord injury research: focus on cardiometabolic diseases. A mini review. Maturitas. 147, 14–18. https://doi.org/10.1016/j.maturitas.2021.03.004 (2021).
McColl, M. A., Charlifue, S., Glass, C., Lawson, N. & Savic, G. Aging, gender, and spinal cord injury. Arch. Phys. Med. Rehabil. 85, 363–367. https://doi.org/10.1016/j.apmr.2003.06.022 (2004).
Cowan, R. E. & Nash, M. S. Cardiovascular disease, SCI and exercise: unique risks and focused countermeasures. Disabil. Rehabil. 32, 2228–2236. https://doi.org/10.3109/09638288.2010.491579 (2010).
Nash, M. S. & Mendez, A. J. A guideline-driven assessment of need for cardiovascular disease risk intervention in persons with chronic paraplegia. Arch. Phys. Med. Rehabil. 88, 751–757. https://doi.org/10.1016/j.apmr.2007.02.031 (2007).
Feldman, S. et al. Quantifying sex Bias in Clinical studies at Scale with Automated Data extraction. JAMA Netw. Open. 2, e196700. https://doi.org/10.1001/jamanetworkopen.2019.6700 (2019).
Yu, Y. et al. Systematic analysis of adverse event reports for sex differences in adverse drug events. Sci. Rep. 6, 24955. https://doi.org/10.1038/srep24955 (2016).
Haller, P. M. et al. Sex-based differences in autologous cell therapy trials in patients with Acute myocardial infarction: Subanalysis of the ACCRUE database. Front. Cardiovasc. Med. 8, 664277. https://doi.org/10.3389/fcvm.2021.664277 (2021).
Mehta, L. S. et al. Acute myocardial infarction in women: A Scientific Statement from the American Heart Association. Circulation. 133, 916–947. https://doi.org/10.1161/cir.0000000000000351 (2016).
Alkhouli, M. et al. Trends in characteristics and outcomes of patients undergoing coronary revascularization in the United States, 2003–2016. JAMA Netw. Open. 3 https://doi.org/10.1001/jamanetworkopen.2019.21326 (2020).
Yang, T. Y., Chen, H. J., Sung, F. C. & Kao, C. H. The association between spinal cord injury and acute myocardial infarction in a nationwide population-based cohort study. Spine (Phila Pa. 1976). 40, 147–152. https://doi.org/10.1097/brs.0000000000000704 (2015).
Phillips, A. A. & Krassioukov, A. V. Contemporary Cardiovascular concerns after spinal cord Injury: mechanisms, maladaptations, and management. J. Neurotrauma. 32, 1927–1942. https://doi.org/10.1089/neu.2015.3903 (2015).
West, C. R. et al. Cardiac consequences of Autonomic Dysreflexia in spinal cord Injury. Hypertension. 68, 1281–1289. https://doi.org/10.1161/hypertensionaha.116.07919 (2016).
Libin, A. et al. Cardiometabolic risk clustering in spinal cord injury: results of exploratory factor analysis. Top. Spinal Cord Inj Rehabil. 19, 183–194. https://doi.org/10.1310/sci1903-183 (2013).
Molinares, D. M., Gater, D. R., Daniel, S. & Pontee, N. L. Nontraumatic spinal cord Injury: Epidemiology, etiology and management. J. Pers. Med. 12 https://doi.org/10.3390/jpm12111872 (2022).
Committee on Energy and Commerce. Christopher and Dana Reeve Paralysis Act. Report (To Accompany H.R. 1727) (Including Cost Estimate of the Congressional Budget Office). Volume 110, Issue 378 of Report. http://www.gpo.gov/fdsys/pkg/CRPT-110hrpt937/html/CRPT-110hrpt937.htm
Acknowledgements
The authors thank the millions of patients who contributed to the NIS database and the numerous professionals who created the database.
Funding
This work was supported by Natural Science Foundation of Ningxia Province (Project No. 2023AAC02071, 2022AAC03479), Open competition mechanism to select the best candidates for key research projects of Ningxia Medical University (Project No. XJKF230205), the Central government guided local science and technology project (Project No. 2022FRD05046). and National Natural Science Foundation of China (82260086, 82060057, 8226020417).
Author information
Authors and Affiliations
Contributions
Guangzhi Cong, Shaobin Jia and Ru Yan: conception or design of the work, data analysis and interpretation, critical revision of the draft, and final approval of the version to be published; Haohong Qi Mingzhi Cui and Xueping Ma: data collection and drafting of the article; Bo Shi, Rui Yan, Shizhe Fu, Kairu Wang, and Congyan Ye: data collection and revision of the draft; and Ru Yan and Ting Zhang: data visualization. All authors had access to the data and a role in writing the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Because the database contains deidentified patient information, our institution determined that the study did not require Institutional Review Board approval.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qi, H., Cui, M., Zhang, T. et al. In-hospital outcomes and temporal analysis of paralyzed patients with acute myocardial infarction undergoing percutaneous coronary intervention. Sci Rep 16, 9554 (2026). https://doi.org/10.1038/s41598-024-78013-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-78013-1
