
Abstract
Objective: This study aims to gain a deeper understanding of the patterns of allergen detection positivity rates among different age and gender groups, and to explore cross-reactivity patterns among allergens. Methods: We conducted a retrospective analysis of patients who underwent allergen testing at our hospital. The sample for this study included all patients who underwent allergen testing. We utilized immune blotting to detect specific IgE antibodies to 20 allergens in patient sera. Results: The study results showed a higher proportion of female samples (72.35%) compared to male samples (27.65%). Among all participants, the age distribution was primarily concentrated in the 25–35 age group, accounting for 37.43% of the total sample, followed by the 45 years and older age group, accounting for 27.00%. This indicates that allergic symptoms may occur not only in children and adolescents but also at any time after adulthood. We further observed significant influences of factors such as gender and age on individual sensitivity to specific allergens. For example, compared to males, females were found to be more sensitive to certain allergens such as cat hair, dust mites, and dog epithelium. Similarly, we also found variations in sensitivity to specific allergens among different age groups. Conclusion: Close monitoring of allergen distribution in populations facilitates active engagement of allergic individuals in self-management, while gender and age may be important factors influencing individual sensitivity to specific allergens. These findings provide valuable insights for understanding the pathogenesis of allergic diseases and designing more effective prevention and treatment strategies.
Similar content being viewed by others

Introduction
Allergic diseases, also referred to as hypersensitivity conditions, encompass a group of disorders in which the body produces specific antibodies in response to antigenic substances, commonly known as allergens1,2,3. Upon re-exposure to similar antigens, these conditions provoke exaggerated or pathological immune reactions, leading to physiological dysfunction in tissues and organs4,5. The prevalence of allergic diseases is notably high across the globe. According to the World Allergy Organization, approximately 22% of the global population suffers from allergic conditions, meaning that one in five individuals worldwide is affected6. In China, the prevalence surpasses 20%, with an estimated affected population exceeding 200 million7. Furthermore, data suggests that nearly 40% of the global population has either experienced or is currently experiencing some form of allergy8.
Due to the widespread prevalence, wide age range of sufferers, and the challenges associated with treatment—characterized by low efficacy and high recurrence rates—the primary focus of allergic disease management is on prevention9,10. Common allergens include foods such as wheat, peanuts, soybeans, nuts, milk, eggs, fish, and shellfish; inhalants such as pollen, house dust, and mites; microorganisms like molds and bacteria; as well as insect toxins, certain drugs such as penicillin and sulfonamides, heterologous serum, and physical factors like cold air, humidity, and friction11,12,13,14. Monitoring the distribution of allergens in populations is crucial for allergic individuals, as it aids in effective self-management15.
Allergen types and concentrations can vary across different regions and even within the same region over time16,17. By identifying allergens within a regional population, healthcare providers can gain insight into the allergen distribution in the area, offering a valuable foundation for the prevention and treatment of allergies. In this study, we conducted a retrospective analysis of allergen test results from our hospital between January and November 2023, providing data to support understanding of regional allergen distribution.
Materials and methods
Study population
This retrospective analysis included patients who underwent allergen testing at Beijing Chaoyang Hospital, Capital Medical University, from January 2023 to November 2023. The study employed the immunoblot method to detect specific IgE antibodies against 20 allergens in the patients’ sera. The characteristics and distribution patterns of allergens were analyzed based on gender, age, and the positive rates of allergen test results, including cross-reactivity. Ethical approval for this study was obtained from the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University.
Allergen detection
Serum samples were collected from each patient and stored at -80 °C until analysis. Specific IgE antibodies against 20 allergens, including common inhalants (e.g., house dust mites, pollens, molds, and animal dander) and food allergens, were detected using the immunoblot method. The allergen-specific IgE testing was carried out using the EUROLINE test kit (EUROIMMUN, Lübeck, Germany), following the manufacturer’s instructions. Briefly, serum samples were incubated with a nitrocellulose membrane pre-coated with allergen extracts. After washing, a biotin-labeled anti-human IgE antibody was added, followed by incubation with streptavidin-alkaline phosphatase. The immunoblot strips were then developed using a chromogenic substrate, and the color intensity of each band corresponding to specific allergens was measured using dedicated EUROLineScan software. The results were interpreted based on the intensity of the bands, categorized into classes ranging from 0 to 2, where class 0 represents no detectable IgE, and classes 1 to 2 indicate increasing levels of specific IgE. For each patient, a result of class 1 or above was considered positive for the corresponding allergen.
Inclusion and exclusion criteria
Inclusion Criteria: Patients with complete demographic information who underwent allergen testing at our hospital from January 2023 to November 2023. Exclusion Criteria: None.
Statistical analysis
Data processing was performed using IBM SPSS Statistics 21 software, and graphical representations were created using Microsoft Office Excel 2019. The Chi-square test was employed to compare differences among different genders, age groups, and allergy diagnoses. In cases where the sample size was small or the data did not meet the prerequisites for the Chi-square test, Fisher’s Exact Test was used to assess differences between two categorical variables. Network clustering diagrams were generated using R version 4.1.1 software (R Core Team, 2021), utilizing the pheatmap package for heatmap procedures and the igraph package for network procedures. A p-value < 0.05 was considered statistically significant.
Results
Overview of allergen detection results
Table 1 presents the frequency and cumulative frequency of different allergen detection results, alongside their respective variable levels. In terms of gender distribution, the number of female samples (72.35%) substantially exceeds that of males (27.65%). The age distribution shows a predominance of the 25–35 age group, constituting 37.43% of the total sample, followed by the 45 years and older age group, comprising 27.00%. When grouped by age, using 35 years as the boundary, 53.07% of the samples are below 35 years old, while 46.93% are 35 years or older. September emerges as the month with the highest sample count, representing 15.83% of the total. Most samples (69.83%) exhibit a negative reaction to allergens, while positive reactions to one allergen and two or more allergens constitute 14.80% and 15.36%, respectively. The top 10 allergens ranked by their combined weak and strong positivity rates are as follows: Cat Hair (9.87%), House Dust Mite, Powder Mite (9.50%), Artemisia (9.31%), Chicken Egg White (3.80%), Dog Epithelium (3.91%), Ryegrass (3.54%), House Dust (4.75%), Willow Tree, Poplar Tree, Elm Tree (2.79%), Crab (2.51%), and Lamb (2.24%).
Gender disparities in allergen sensitivity
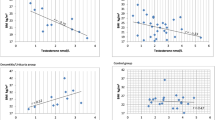
Our study observed significant differences in sensitivity to various allergens between males and females (Table 2). Regarding age grading, a statistically significant difference in allergen sensitivity between males and females was found (χ2 = 8.778, P = 0.032). Additionally, a statistically significant difference in the distribution of allergic dermatitis between males and females was observed (χ2 = 20.587, P = 0.000). Furthermore, significant differences in sensitivity to Penicillium, Aspergillus, and related fungi were found between males and females (P = 0.024). Gender-based differences in sensitivity to the milk allergen also exhibited statistical significance (P = 0.041). Likewise, sensitivity to herbaceous plant allergens showed statistically significant differences between males and females (χ2 = 4.112, P = 0.043). Lastly, significant differences in sensitivity to house dust mite allergens between males and females were noted (χ2 = 15.270, P = 0.000). These findings provide valuable insights into the distribution of allergens among different genders, contributing to a better understanding of allergen profiles.
Age-related variations in allergen sensitivity
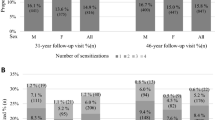
We compared allergen sensitivity across different age groups and observed statistically significant differences (p < 0.05). In the age groups under 18, 18–40, 40–60, and ≥ 60 years, the allergen positivity rates were 56.3%, 32%, 26.6%, and 17.6%, respectively (Fig. 1). The results from Table 3 reveal significant differences in allergen sensitivity among different age groups. Firstly, regarding the number of allergens, individuals with two or more allergens exhibit significant differences in distribution across different age brackets (χ2 = 46.186, p < 0.001). Additionally, concerning the total number of allergies, there are significant differences in the distribution of negative reactions across different age groups (χ2 = 27.407, p < 0.001). In terms of diagnosis, the distribution of allergic dermatitis also shows significant differences across different age groups (χ2 = 25.438, p = 0.003). Regarding specific allergens, the sensitivity distribution of Artemisia (χ2 = 13.318, p = 0.004), dog epithelium (Fisher’s Exact Test, p < 0.001), chicken protein (Fisher’s Exact Test, p = 0.001), cat hair (χ2 = 49.883, p < 0.000), milk (Fisher’s Exact Test, p = 0.002), house dust (χ2 = 19.439, p < 0.000), house dust mite (χ2 = 21.031, p < 0.000), and lamb (Fisher’s Exact Test, p = 0.008) exhibit significant differences in sensitivity distribution across different age groups. These results suggest that age may be an important factor influencing individual sensitivity to specific allergens.

The overall positivity rate of allergens across different age groups.
Analysis of concurrent positive reactions to two allergens
We further analyzed data of concurrent positive reactions to two allergens and calculated their percentages. The top 10 combinations with the highest proportions were as follows: dog epithelium and cat hair at 11.1%, common pigweed and Artemisia at 9.9%, Artemisia and cat hair at 9.0%, dust mite and cat hair at 8.6%, house dust and cat hair at 8.6%, willow, poplar, elm, and Artemisia at 7.7%, Artemisia and dust mite at 7.1%, Artemisia and herb grass at 6.5%, Artemisia and house dust at 6.5%, and dust mite and crab at 4.6% (Fig. 2). Additionally, we presented the results using a clustering diagram (Fig. 3).

Cross-reactivity heatmap of antigen (allergen) testing: The numbers in the figure represent the percentage of simultaneous positivity for two antigens, with darker colors indicating higher percentages. The antigens represented by each letter are listed in the table on the right.

Network clustering diagram of cross-reactive antigens: The size of each circle in the figure represents the corresponding antigen’s positivity proportion, with larger circles indicating higher positivity rates. The lines connecting two circles represent the proportion of simultaneous positivity for both antigens; thicker lines indicate higher simultaneous positivity rates. Clustering of circles indicates a tendency for certain antigens to co-occur positively. The specific antigens represented by each letter are detailed in the table on the right.
The logistic regression analysis demonstrated that age was a significant risk factor in allergen positivity across multiple categories. Specifically, individuals under 18 years old had significantly higher odds of testing positive for several allergens. For IgE positivity, those under 18 years had a notably increased risk (Wald Chi-Square = 19.58, p < 0.001), while other age groups showed no significant associations. Regarding common allergens, positivity for Artemisia absinthium was significantly associated with being under 18 years of age (p = 0.001), with no such relationship observed in older age groups. Similarly, for dust mites, both male sex and age under 18 were significant factors, with males showing increased odds (p < 0.001) and children under 18 years also demonstrating a higher risk of sensitization (p < 0.001). For Penicillium nodosum and related fungi, males were more likely to test positive (p = 0.019), though age did not emerge as a significant factor. Likewise, positivity for egg white allergen was significantly linked to both children under 18 years (p = 0.001) and individuals aged 18–40 years (p = 0.001). Interestingly, for cat hair allergen, being younger than 18 years (p < 0.001) or between 18 and 40 years (p = 0.005) was associated with higher positivity rates. However, male sex was not a significant factor for these allergens. Conversely, factors like sex and age did not significantly affect positivity for allergens like crab, cod, or other shellfish, as reflected by non-significant p-values (Table 4). In summary, age under 18 years appeared to be the most consistent predictor of allergen positivity across various categories, with male sex showing specific associations for certain allergens such as dust mites and fungal allergens.
Discussion
Our research findings reveal significant disparities in allergen sensitivity across different genders and age groups. Females exhibited higher sensitivity rates compared to males, with notable differences in specific allergens such as cat hair and house dust mites. Age-wise, children and adolescents showed the highest positivity rates, indicating heightened susceptibility at a younger age. Our comprehensive analysis of allergen detection results unveils nuanced insights into the complexities of allergen sensitivity, shedding light on significant variations across different demographic groups. By integrating our findings with existing knowledge, we can better understand the intricate interplay between gender, age, and allergen exposure in shaping individual allergic responses.
Gender Disparities in Allergen Sensitivity Our study underscores notable gender disparities in allergen sensitivity, with females exhibiting a substantially higher prevalence of sensitivity compared to males. This observation aligns with previous research indicating that females are more prone to allergic conditions18,19,20. Several factors may contribute to this gender-based variation. Firstly, hormonal influences, particularly estrogen, may modulate immune responses and predispose females to heightened allergic reactions20,21,22,23. Additionally, differences in skin barrier function and exposure to environmental allergens could contribute to increased sensitivity among females24,25. Our findings further elucidate specific allergens where gender differences are particularly pronounced, including Penicillium, Aspergillus, milk, herbaceous plants, and house dust mites. These gender-specific patterns underscore the importance of tailoring allergy management strategies to account for gender-related factors and highlight the need for further research into the underlying mechanisms driving these differences.
Age-Related Variations in Allergen Sensitivity Our analysis reveals significant age-related variations in allergen sensitivity, with distinct patterns emerging across different age groups. Younger individuals, particularly those under 18 years old, demonstrate a higher prevalence of allergen sensitivity compared to older age groups. This finding is consistent with the notion that allergic conditions often manifest early in life and may gradually decline with age26,27,28. Interestingly, our study identifies specific allergens that exhibit differential sensitivity distribution across age groups, including Artemisia, dog epithelium, cat hair, and others. These age-specific patterns underscore the dynamic nature of allergic responses and suggest that age-related factors play a crucial role in shaping individual susceptibility to allergens29. Clinically, our findings emphasize the importance of considering age-related factors in allergy diagnosis and management, as tailored approaches may be necessary to effectively address allergen sensitivities across different life stages.
Analysis of Concurrent Positive Reactions to Two Allergens Furthermore, our analysis of concurrent positive reactions to multiple allergens provides valuable insights into the complex nature of allergic responses. We identified several combinations of allergens that elicited concurrent positive reactions, suggesting potential cross-reactivity or synergistic effects. Notably, the top combinations included dog epithelium and cat hair, common pigweed and Artemisia, and Artemisia and cat hair, among others. The simultaneous positive reactions to these allergens suggest potential cross-reactivity or co-sensitization among them. This implies that individuals allergic to one allergen may exhibit similar allergic reactions to another allergen, thereby adding complexity to allergic symptoms30. These findings underscore the need for comprehensive allergen testing to identify coexisting sensitivities and inform personalized allergy management strategies. By elucidating these complex interactions, our study contributes to a deeper understanding of the underlying mechanisms driving allergic responses and provides valuable insights into the development of targeted interventions to alleviate allergic symptoms effectively.
Although our study has yielded important findings, there are several limitations that should be considered. Firstly, our research is based on sample data from a single region, which may introduce regional variations and limit the generalizability of our results. Secondly, our study employs a cross-sectional design, which precludes establishing causality and only allows for observing correlations. Additionally, the relatively small sample size in our study may restrict the analysis of certain subgroups, such as finer age groupings. Lastly, we only considered some common allergens in our study and may have overlooked other potential allergens. Therefore, when interpreting our results and formulating relevant policies, it is important to carefully consider these limitations and further refine and validate our findings in future research.
In conclusion, our study offers valuable contributions to the field of allergy research by elucidating the intricate relationships between gender, age, and allergen sensitivity. By integrating our findings with existing knowledge, we enhance our understanding of allergen profiles and pave the way for more effective approaches to allergy diagnosis, management, and treatment. However, further research is warranted to explore the underlying mechanisms driving gender and age-related differences in allergen sensitivity and to develop personalized strategies to address individual allergic responses comprehensively.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Hamilton, R. G. Assessment of human allergic diseases. In Clinical Immunology. 1283–1295. e1281 (Elsevier, 2019).
Pascal, M. et al. Microbiome and allergic diseases. Front. Immunol. 9, 1584 (2018).
Breiteneder, H., O’Hehir, R.E., O’Mahony, L. et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy. 75 (12), 3039–3068 (2020).
Kay, A. B. Allergy and allergic diseases. N. Engl. J. Med. 344 (1), 30–37 (2001).
Ogulur, I. et al. Advances and highlights in biomarkers of allergic diseases. Allergy. 76 (12), 3659–3686 (2021).
Warner, J. O. et al. Allergy practice worldwide: A report by the World Allergy Organization Specialty and Training Council. Int. Arch. Allergy Immunol. 139 (2), 166–174 (2006).
Li, F. et al. Prevalence and risk factors of childhood allergic diseases in eight metropolitan cities in China: A multicenter study. BMC Public. Health. 11 (1), 1–9 (2011).
Prescott, S. L. et al. A global survey of changing patterns of food allergy burden in children. World Allergy Organ. J. 6, 1–12 (2013).
Arshad, S. H., Bateman, B., Sadeghnejad, A., Gant, C. & Matthews, S. M. Prevention of allergic disease during childhood by allergen avoidance: The Isle of Wight prevention study. J. Allergy Clin. Immunol. 119 (2), 307–313 (2007).
Solomon, W. R. Prevention of allergic disorders. Pediatr. Rev. 15 (8), 301–309 (1994).
Francis, O. L., Wang, K. Y., Kim, E. H. & Moran, T. P. Common food allergens and cross-reactivity. J. Food Allergy (USA). 2 (1), 17–21 (2020).
Valenta, R. et al. Molecular aspects of allergens and allergy. Adv. Immunol. 138, 195–256 (2018).
Breiteneder, H. & Radauer, C. A classification of plant food allergens. J. Allergy Clin. Immunol. 113 (5), 821–830 (2004).
Foo, A. C. & Mueller, G. A. Abundance and stability as common properties of allergens. Front. Allergy. 2, 769728 (2021).
Shipp, C. L., Gergen, P. J., Gern, J. E., Matsui, E. C. & Guilbert, T. W. Asthma management in children. J. Allergy Clin. Immunol. Pract. 11 (1), 9–18 (2023).
McClain, S. et al. Variation in seed allergen content from three varieties of soybean cultivated in nine different locations in Iowa, Illinois, and Indiana. Front. Plant Sci. 9, 1025 (2018).
Sultana, S. et al. The impact of changing seasons: Seasonal allergy prevalence and management. Migration Lett. 21 (S6), 406–429 (2024).
Jensen-Jarolim, E. & Untersmayr, E. Gender‐medicine aspects in allergology. Allergy 63(5), 610–615 (2008) .
Cazzoletti, L. et al. The gender, age and risk factor distribution differs in self-reported allergic and non-allergic rhinitis: A cross-sectional population-based study. Allergy Asthma Clin. Immunol. 11 (1), 1–9 (2015).
Nowak-Wegrzyn, A., Ellis, A. & Castells, M. Sex and allergic diseases. Ann. Allergy Asthma Immunol. 122 (2), 134–135 (2019).
Chen, W., Mempel, M., Schober, W., Behrendt, H. & Ring, J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy. 63 (11), 1418–1427 (2008).
Leffler, J., Stumbles, P. A. & Strickland, D. H. Immunological processes driving IgE sensitisation and disease development in males and females. Int. J. Mol. Sci. 19 (6), 1554 (2018).
Goldhahn, K. et al. Sex-specific differences in allergic sensitization to house dust mites: A meta-analysis. Ann. Allergy Asthma Immunol. 102 (6), 487–494 (2009).
Modjtahedi, B., Modjtahedi, S. & Maibach, H. The sex of the individual as a factor in allergic contact dermatitis. Contact Dermat. 50 (2), 53–59 (2004).
Chen, W., Mempel, M., Traidl-Hofmann, C., Al Khusaei, S. & Ring, J. Gender aspects in skin diseases. J. Eur. Acad. Dermatol. Venereol. 24 (12), 1378–1385 (2010).
Futamura, M. et al. Age-related prevalence of allergic diseases in Tokyo schoolchildren. Allergology Int. 60 (4), 509–515 (2011).
Bunne, J. et al. The majority of children sensitized before school-age develop allergic disease before adulthood: A longitudinal population-based study. J. Allergy Clin. Immunology: Pract. 10 (2), 577–585 (2022). e573.
Chang, W-S. et al. Age-related changes in immunological factors and their relevance in allergic disease development during childhood. Allergy Asthma Immunol. Res. 8 (4), 338–345 (2016).
Di Lorenzo, G., Di Bona, D., Belluzzo, F. & Macchia, L. Immunological and non-immunological mechanisms of allergic diseases in the elderly: Biological and clinical characteristics. Immun. Ageing. 14, 1–8 (2017).
Li, W. & Zou, Z. Cross-reactivity. Allergy Bioinf. 67–92 (2015).
Acknowledgements
We are grateful to all staff professionals and participants.
Author information
Authors and Affiliations
Contributions
BW and DZ contributed to the conception and design of the study; ZH J and DZ performed the experiments, collected and analyzed data; BW and ZH J wrote the manuscript; FL revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The current study was conducted in accordance with the Helsinki Declaration of the World Medical Association and approved by the Ethics Committee of Beijing Chao-yang Hospital, Capital Medical University. Informed consent was obtained from all the study subjects before enrollment.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, B., Zhang, D., Jiang, Z. et al. Analysis of allergen positivity rates in relation to gender, age, and cross-reactivity patterns. Sci Rep 14, 27840 (2024). https://doi.org/10.1038/s41598-024-78909-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-78909-y
Keywords
This article is cited by
-
Guilty by association: direct interaction with the tetraspanin CD63 suggests a role for organic cation transporter 3 in histamine release from granulocytes
Journal of Biomedical Science (2025)
-
Exploring Barriers to Adherence in Allergen Immunotherapy and Vas Score Changes After Each Dose
Indian Journal of Otolaryngology and Head & Neck Surgery (2025)
-
A Clinical Study to Assess prevalance of Allergen Sensitivity in Patients With Allergic Rhinitis
Indian Journal of Otolaryngology and Head & Neck Surgery (2025)
