
Abstract
This study is aimed at identifying risk factors of Low Anterior Resection Syndrome following ileostomy reversal in rectal cancer patients who had undergone preventive ileostomy. This retrospective analysis was conducted on a cohort of 605 patients treated at the Fourth Hospital of Hebei Medical University between January 2018 and December 2021. These patients were grouped based on LARS score, and Clinical and follow-up data were collected to conduct univariate analyses of potential factors influencing LARS occurrence based on variable type. Variables with statistical significance were included in a logistic regression model to analyze potential influences on the occurrence of LARS. Univariate and Multivariate logistic regression analysis showed that N2 stage (OR = 2.290 95%CI: 1.076–4.873, P = 0.031), chemoradiotherapy (OR = 2.271, 95%CI: 1.246–4.138, P = 0.007), and anastomosis height (OR = 0.836, 95%CI: 0.717–0.975, P = 0.022) were independent influences on the occurrence of LARS. In model 3 (adjusting for all covariates), the relationship between anastomotic height and patient LARS status showed a negative correlation. In subgroup analyses, there were significant differences in the effect of anastomotic height on LARS in subgroups with different hemoglobin concentrations. A high occurrence rate of LARS is observed in rectal cancer patients with preventive ileostomy reversal. N2 stage, history of chemoradiotherapy, and anastomotic height are independent influence factors for the occurrence of major LARS after ileostomy reversal.
Similar content being viewed by others

Introduction
Colorectal cancer is among the most common malignant tumors, and its incidence has significantly increased in recent years, with rectal cancer accounting for more than 30%1,2,3. Surgical treatment and diagnostics are continually improving, which has been enhancing the rate of sphincter-saving surgeries, especially for lower rectal cancer, reducing the necessity for permanent colostomies in many patients with rectal cancer4. Simultaneously, the proportion of patients receiving protective ileostomies has increased to mitigate the risk of anastomotic fistula5.
Low anterior resection syndrome (LARS) is characterized by a set of clinical symptoms resulting from impaired anal function following surgery in patients with low rectal cancer. Currently, several therapeutic strategies are available for LARS, including drug therapy, biofeedback, and sacral nerve stimulation6,7,8,9. Nevertheless, due to the underestimation of this complication, only a minority of patients receive these treatments10. Some studies have found that preventive enterostomy affects anal function and makes patients more susceptible to LARS11. Therefore, it is crucial to find the cause of anterior rectal resection syndrome.
In the current body of research, there is a significant focus on identifying the factors influencing Low Anterior Resection Syndrome (LARS) following radical rectal cancer surgery. However, studies specifically addressing the factors affecting LARS after the reversal of a prophylactic stoma are relatively scarce. Most of the existing research has primarily analyzed the presence or absence of an ileostomy as a factor influencing LARS. We found only one study similar to ours12, but it had a smaller sample size. This study examines the factors influencing LARS in these patients to establish a foundation for specific clinical interventions.
Materials and methods
Patient selection
We conducted a retrospective analysis of rectal cancer patients treated at the Fourth Hospital of Hebei Medical University from January 2018 to December 2021. The inclusion criteria were as follows: 1). Patients diagnosed with rectal cancer for the first time; 2). Patients who had undergone anterior rectal resection with preventive ileostomy; 3). Patients who had completed restorative ileostomy surgery; 4). Patients and their families who agreed to participate in the study; 5). Patients with complete clinical data and follow-up data. The exclusion criteria were: 1). Patients with tumours in other locations; 2). Patients with serious diseases such as diabetes; 3). Patients with perianal abscesses or fissures affecting anorectal function; 4). Patients with severe mental disorders; 5). Patients with recurrent or metastatic malignancies; 6). Patients with permanent stoma; 7). Patients are unable to complete follow-up. Based on these criteria, data from 602 patients were collected. This study received approval from the Ethics Committee of the Fourth Hospital of Hebei Medical University (approval number 2021111), and the study was conducted in accordance with the Declaration of Helsinki, and all patients provided informed consent before their inclusion in the study, adhering to ethical guidelines and standards. Figure 1 illustrates the study’s flow chart.
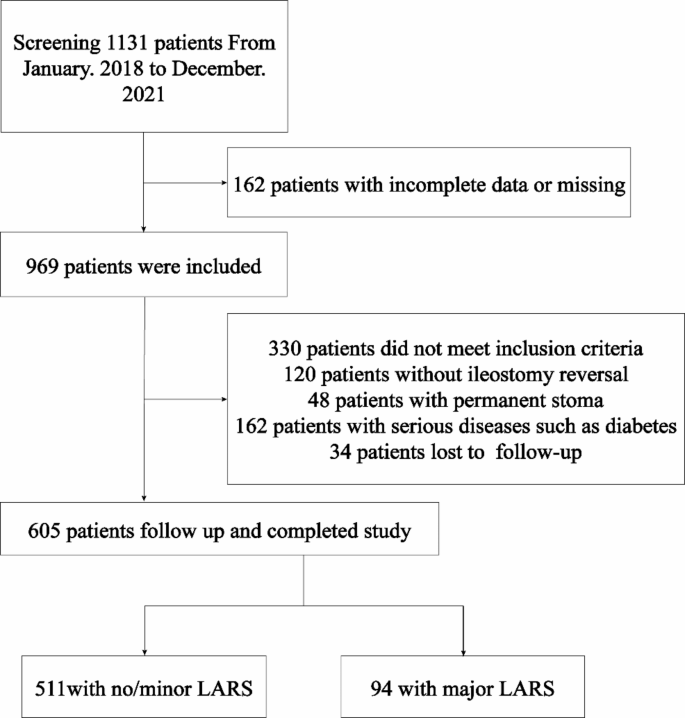
Flow chart of participants selection.
Surgical methods
All radical rectal cancer surgeries were performed following the principles of Total Mesolectal Excision (TME) and under the guidance of relevant standards and guidelines. The decision between laparoscopic surgery, robotic surgery, and open surgery is made collaboratively by the patient, the patient’s family. Patients with rectal cancer underwent anterior resection with preventive ileostomy, utilizing a double-barreled end ileostomy in the right lower quadrant of the abdomen. In this study, all included patients underwent anastomosis using the double-stapling technique (DST). Criteria for prophylactic ileostomy are as follows: (1) Patients who have undergone preoperative chemoradiotherapy. (2) Patients at high risk of anastomotic leakage, such as those with ultra-low anastomosis, extensive pelvic dissection, or when the anastomosis is created under tension. (3) Patients with potentially compromised blood supply to the anastomosis, as determined intraoperatively or through preoperative imaging studies. (4) Patients with significant comorbidities (such as diabetes mellitus, obesity, or chronic obstructive pulmonary disease) and those with poor overall health status. Ostomy care was managed by professional ostomy nurses in the department, which included perioperative education, guidance for examinations, and stoma care. Restorative ileostomy surgery was completed after the physician reassessed the patient’s condition.
Observation indicators
Taking into account baseline characteristics of the patients and particulars of their surgery and tumor, we logged variables including sex, age, TNM stage post-surgery, treatment category, adjuvant chemotherapy, Surgical Methods, the height of the anastomosis, lower margin height of the tumor, and the interval between the stoma creation and the restorative surgery. For patients with locally advanced disease or lymph node metastasis, we administered neoadjuvant chemoradiotherapy after obtaining consent from the patients and their families. The treatment approaches included Total Neoadjuvant Therapy (TNT) and neoadjuvant chemoradiotherapy followed by adjuvant chemotherapy post-surgery. For patients who refused radiotherapy but consented to neoadjuvant chemotherapy, we administered neoadjuvant chemotherapy alone. For measuring the tumor’s lower margin height in this research, preoperative scans were performed with Magnetic Resonance Imaging (MRI) in sagittal T2-weighted imaging (T2WI) sequences. After examinations, attending doctors with extensive clinical experience reviewed the images, with distance measurements defined upon appraisal by a chief physician. The height of the anastomosis was assessed using colonoscopy before the restorative surgery. The anastomotic leak and pelvic abscess were identified based on postoperative abdominal drainage fluid analysis and relevant imaging studies.
Low Anterior Resection Syndrome (LARS) scores were evaluated using standardized scoring criteria. The LARS scoring system provides greater specificity and sensitivity in assessing anal function following a low anterior resection of the rectum compared to the Wexner score, and its validity has been confirmed in multiple centers across various countries13. The LARS score includes five questions: exhaust incontinence, fecal incontinence, frequency of defecation, sense of tenseness and urgency of defecation. The maximum total score for all items is 42 points. Scores of 0 to 20 are classified as no anterior resection syndrome (no LARS), 21 to 29 are classified as minor anterior resection syndrome (minor LARS), and 30 to 42 are classified as major anterior resection syndrome (major LARS). In this study, the LARS score was evaluated one year after the ileostomy reversal. postoperatively were classified as the major LARS group, while those who had no LARS or only minor LARS were classified as the no/minor LARS group.
Data collection
LARS scores were obtained through telephone follow-up or outpatient visits. After obtaining informed consent from the patients,, the researchers administered questionnaires to be filled out or answered by the patients themselves, evaluating symptoms with the LARS scoring system and rigorously screening cases based on inclusion and exclusion criteria. In an effort to reduce bias, an independent team was formed to conduct follow-ups. All team members which, once confirmed to be accurate, were entered into the system by these same researchers. the credibility of the findings. Investigators garnered additional patient information, including surgery and radiological data, from the hospital’s medical record system. Two investigators were tasked with the arrangement, verification, and cross-checking of clinical and follow-up data, which, once confirmed to be accurate, were entered into the system by these same researchers.
Statistical methods
Data analysis was performed using SPSS 25.0 (IBM, Armonk, New York, USA) and R software (R Project for Statistical Computing, Vienna, Austria; version 4.3.2). Continuous variables were first subjected to tests for normality. Metrics distributed normally were expressed as mean ± standard deviation (x̄ ± s) and compared using the t-test, while metrics not distributed normally were expressed as the median (interquartile range) [M(IQR)] and compared using the Mann-Whitney U test. Categorical data were expressed as frequency and percentage (%) and compared using the chi-square test or Fisher’s exact test for dichotomous or unordered multicategory variables, with rank data compared using the Mann-Whitney U test. Variables were first analyzed using univariate logistic regression, with significant variables then included in a multivariate logistic regression model. Figures were created using R software (R Project for Statistical Computing, Vienna, Austria; version 4.3.2). Differences were considered statistically significant at P < 0.05.
Results
Patient characteristics
A cohort of 605 patients was enrolled in this study from January 2018 to December 2021, encompassing complete follow-up, clinical, and pathological profiles. Based on the LARS score, 91 patients (15.5%) experienced major LARS, while 511 patients (84.5%) experienced no or major LARS. There was no statistically significant difference between patients in the Major LARS group and the no/minor LARS group in terms of gender, age, T-stage, tumor location, Surgical Methods, adjuvant chemotherapy, postoperative complications, and ileostomy reversal interval time. There was a significant difference in the treatment category between patients in the major LARS group and those in the no/minor LARS group (P = 0.040). In the no/minor LARS group, the anastomotic height was [3.00 (2.00–4.00) cm], which was higher than that in the Major LARS group [2.00 (2.00–4.00) cm, P < 0.001]. Although the N stage differed between the two groups, there was no statistically significant difference in terms of regional lymph node metastasis in the Major LARS group (34 (18.8%)) compared to the no/minor LARS group [147 (28.8%), P = 0.150] [Table 1]. In our study, there were a total of four patients with postoperative anastomotic leaks and pelvic abscesses: three with anastomotic leaks and one with a pelvic abscess. All anastomotic leaks were classified as Grade A or B and were successfully treated with conservative management.
Logistic regression analysis of factors affecting lars after restorative ileostomy
Logistic regression analyses were performed to determine whether patients developed major Lars, and the variables included were gender, age, T stage, N stage, tumor location, anastomotic height, pathological stage, treatment category, adjuvant chemotherapy, Surgical Methods, HBG, ALB, anastomotic leakage or abscess, postoperative bowel obstruction, bleeding and reversal interval time. univariate analysis showed that N2stage, chemoradiotherapy, and anastomotic height were all associated with LARS, which was included in the multivariate regression analysis, which showed that N2 stage (OR = 2.290 95%CI: 1.076–4.873, P = 0.031), chemoradiotherapy (OR = 2.271, 95%CI: 1.246–4.138, P = 0.007), and anastomosis height (OR = 0.836, 95%CI: 0.717–0.975, P = 0.022). were all influential factors for the occurrence of major LARS after ileostomy reversal. These results can be seen in Table 2.
Table 3 presents the multivariate linear regression analysis results between anastomotic height and LARS in the three models. After adjusting for age, gender, T stage, N stage, treatment category, surgical methods, adjuvant chemotherapy, HBG, ALB, anastomotic leakage or abscess, postoperative bowel obstruction, bleeding and reversal interval time, a negative correlation was shown between anastomotic height and LARS status (OR = 0.84, 95%CI: 0.72–0.99, P = 0.034).
Subgroup analysis
We further performed a subgroup analysis of the effect of anastomotic height on LARS. The results showed that there was no statistically significant difference in the effect of anastomotic height on LARS among subgroups based on age, adjuvant chemotherapy, treatment category, or albumin (ALB) concentrations (< 40 and ≥ 40 g/L). However, the protective effect of anastomotic height was more pronounced in specific subgroups, including males, patients with T3-T4 stage tumors, those with local lymph node metastasis, those who underwent laparoscopic surgery, patients with a reduction interval of less than 228 days, and those with hemoglobin concentrations ≥ 120 g/L (Fig. 2).
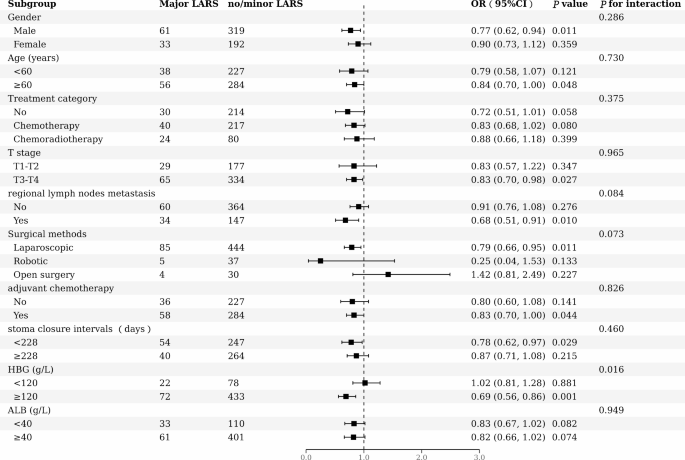
Subgroup analysis of the association between anastomotic height (cm) and the occurrence of major LARS. Age, gender, T stage, regional lymph node metastasis, treatment category, surgical methods, adjuvant chemotherapy, HBG, ALB, and reversal interval time were adjusted. In the subgroup analyses, the model is not adjusted for the stratification variable itself. Regional lymph node metastasis: Regional lymph node metastasis corresponds to N1 and N2 stages in the N staging system. Chemoradiotherapy: The patient underwent radiotherapy and chemotherapy. Robotic: Da Vinci Surgical Robot. HGB: Hemoglobin; ALB: albumin; LARS: Low anterior resection syndrome; OR: odds ratio; CI: confidence interval.
Discussion
As surgical techniques continue to advance and neoadjuvant chemoradiotherapy becomes more prevalent, the frequency of low and ultra-low anterior resections for rectal cancer patients has increased14. This trend has resulted in both an increase in prophylactic ileostomy procedures and a growing interest in managing the Low Anterior Resection Syndrome15. In our research, the occurrence rate of LARS in patients with prophylactic ileostomy reached 97.6%, which is higher than the rates reported in most previous studies on post-rectal anterior resection316;. This can be linked to prophylactic ileostomies being more common among patients with low anastomoses and those who received neoadjuvant therapy, both of which are associated with a higher risk of developing LARS17. Our research identified N2 stage, a history of chemoradiotherapy and anastomotic height were factors influencing LARS following prophylactic stoma reversal post-rectal cancer anterior resection. It is noteworthy that the stoma closure intervals did not significantly affect the occurrence rates of major LARS among patients.
Our research indicates that radiotherapy, whether administered either before or after surgery, escalates the risk of major postoperative LARS. As chemoradiotherapy advances, total mesorectal excision following concurrent chemoradiotherapy stands as the standard care for locally advanced rectal cancer, enhancing control over local relapse rates18,19,20,21. However, Neoadjuvant therapy has been associated with an increased rate of anastomotic fistulas post-surgery22, making prophylactic stoma formation necessary for more patients to mitigate symptoms23. Simultaneously, evidence suggests that neoadjuvant therapy raises the incidence of postoperative LARS24. A meta-analysis15identified radiotherapy within either neoadjuvant or adjuvant treatments as the most consistent contributing factor for major LARS, corroborating the outcomes of findings of this study. Radiotherapy impacts anal function irrespective of the performance of a prophylactic stoma. In the study by Bolton et al16., there was no significant difference in the incidence of major LARS between patients who received adjuvant therapy and those who did not (P= 0.1978), which might be related to a subset of patients in the study not receiving radiotherapy during adjuvant treatment. Our study suggests no significant link between undergoing neoadjuvant or adjuvant chemotherapy and the incidence of major postoperative LARS. However, some research indicates a heightened risk of LARS among patients treated with radiotherapy alone compared to those subjected to undergoing chemoradiotherapy25. The impact of radiotherapy on anal function may be due in part to fibrosis of neurons in the affected area, leading to disruption in neurological pathways following autonomic nerve fibrosis26, and fibrotic changes in the rectal wall and mesentery induced by radiotherapy, which reduces rectal sensitivity27.
Our study indicates a connection between regional lymph node metastasis, particularly at the N2 stage, and the occurrence of major LARS, aligning with the findings of a clinical predictive model for postoperative LARS in rectal cancer12. Similar to our study, the prediction model included patients with rectal cancer who underwent restoration after a preventive ileostomy. Multiple studies suggest that a higher N staging correlates with an increased probability of neural invasion, potentially affecting anorectal function and leading to LARS28,29. However, these studies also consider pathological staging and T staging as factors for neural invasion, whereas our study results do not indicate that these factors impact anorectal function. In additional research on predicting LARS, T staging and pathological staging have not been included in their prediction models13,30,31,32.
Our study results corroborate that anastomotic height is associated with LARS incidence, consistent with extensive research findings13,15,16,26,30,31,32,33. In those studies, stratification of patients based on anastomotic distance typically uses a 3–5 cm threshold. For patients with lower anastomotic sites, particularly those involving the distal one-third of the rectum, intersphincteric resection may be necessary, potentially impairing the anal sphincter’s function34. While some studies have identified the height of the tumor’s lower edge as a factor influencing LARS, this was not observed in our study, possibly due to the varying degrees of anatomical and physiological disruption caused by tumors of different sizes and locations35. A retrospective study indicated an association between the presence of a preventive ileostomy and LARS, but it did not demonstrate any clear link with the ostomy closure time14. Similarly, our study showed that the time for prophylactic ileostomy closure is not a risk factor for LARS postoperatively.
This study is retrospective and limited by the timeframe; there is a minimal inclusion of patients with influencing factors and surgical intervals greater than one year. Therefore, future research will involve an increased focus on factors and sample size post-stoma reversal surgery to provide a richer body of evidence for correlated clinical practice.
Conclusion
To conclude, patients who have a prophylactic ileostomy reversal after rectal cancer surgery experience a high incidence of LARS, although the rate of major LARS is proportionately low. N2 stage, history of chemoradiotherapy, and anastomotic height are identified as independent influence factors for the development of major LARS after ileostomy reversal.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Xia, C. et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin. Med. J. 135, 584–590 (2022).
Sung, H. et al. Global Cancer statistics 2020: Globocan estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. Ca-Cancer J. Clin. 71, 209–249 (2021).
Zhang, R. et al. Clinical management of low anterior resection syndrome: review of the current diagnosis and treatment. Cancers 15, (2023).
Keane, C. et al. International Consensus Definition of Low Anterior Resection Syndrome. Dis. Colon Rectum. 63, 274–284 (2020).
Coco, C. et al. Role and morbidity of Protective Ileostomy after Anterior Resection for rectal Cancer: one centre experience and review of literature. J. Clin. Med. 12, (2023).
Zahid, J. A., Madsen, M. T., Bulut, O., Christensen, P. & Gögenur, I. Effect of melatonin in patients with low anterior resection syndrome (Mellars): a study protocol for a Randomised, Placebo-Controlled, crossover trial. Bmj Open. 13, e067763 (2023).
Pires, M. et al. Sacral neuromodulation for low anterior resection syndrome: current Status-a systematic review and Meta-analysis. Int. J. Colorectal Dis. 38, 189 (2023).
Falletto, E. et al. Transanal Irrigation in Functional Bowel disorders and Lars: short-term results from an Italian National Study. Tech. Coloproctology. 27, 481–490 (2023).
Pieniowski, E. et al. A Randomized Controlled Clinical Trial of Transanal Irrigation Versus Conservative Treatment in patients with low anterior resection syndrome after rectal Cancer surgery. Ann. Surg. 277, 30–37 (2023).
McKenna, N. P., Bews, K. A., Yost, K. J., Cima, R. R. & Habermann, E. B. Bowel dysfunction after low anterior resection for Colorectal Cancer: a frequent late effect of surgery infrequently treated. J. Am. Coll. Surg. 234, 529–537 (2022).
Verkuijl, S. J. et al. The Effect of a Temporary Stoma on Long-Term Functional outcomes following surgery for rectal Cancer. Dis. Colon Rectum. 67, 291–301 (2024).
Xia, F., Zou, Y., Zhang, Q., Wu, J. & Sun, Z. A Novel Nomogram to Predict Low Anterior Resection Syndrome (Lars) after ileostomy reversal for rectal Cancer patients. Ejso. 49, 452–460 (2023).
Huang, M. J. et al. Development of Prediction Model of Low Anterior Resection Syndrome for Colorectal Cancer patients after surgery based on machine-learning technique. Cancer Med. 12, 1501–1519 (2023).
Pieniowski, E. et al. Defunctioning Stoma in rectal Cancer surgery - A risk factor for low anterior resection syndrome? Ejso. 48, 2518–2524 (2022).
Croese, A. D., Lonie, J. M., Trollope, A. F., Vangaveti, V. N. & Ho, Y. H. A Meta-analysis of the prevalence of low anterior resection syndrome and systematic review of risk factors. Int. J. Surg. 56, 234–241 (2018).
Bolton, W. S. et al. The incidence of low anterior resection syndrome as assessed in an International Randomized Controlled Trial (Mrc/Nihr Rolarr). Ann. Surg. 274, e1223–e1229 (2021).
Vogel, I. et al. Impact of a Defunctioning Ileostomy and Time to Stoma Closure on bowel function after low anterior resection for rectal Cancer: a systematic review and Meta-analysis. Tech. Coloproctology. 25, 751–760 (2021).
Lin, Z. et al. Phase II, single-arm trial of Preoperative Short-Course Radiotherapy followed by Chemotherapy and Camrelizumab in locally advanced rectal Cancer. J. Immunother Cancer 9, (2021).
Hazen, S. et al. Abandonment of routine radiotherapy for nonlocally advanced rectal Cancer and oncological outcomes. Jama Oncol. (2023).
Jin, J. et al. Multicenter, Randomized, Phase III Trial of short-term Radiotherapy Plus Chemotherapy Versus Long-Term Chemoradiotherapy in locally advanced rectal Cancer (stellar). J. Clin. Oncol. 40, 1681–1692 (2022).
Ji, D. et al. Combination of Radiotherapy and suppression of Tregs enhances Abscopal Antitumor Effect and inhibits metastasis in rectal Cancer. J. Immunother Cancer 8, (2020).
Ellebæk, M. B. et al. Early Versus late reversal of Diverting Loop Ileostomy in rectal Cancer surgery: a Multicentre Randomized Controlled Trial. Sci. Rep. 13, 5818 (2023).
Zhang, H. et al. Protective ileostomy increased the incidence of rectal stenosis after anterior resection for rectal Cancer. Radiat. Oncol. 17, 93 (2022).
Emmertsen, K. J. & Laurberg, S. Impact of Bowel Dysfunction on Quality of Life after sphincter-preserving resection for rectal Cancer. Br. J. Surg. 100, 1377–1387 (2013).
Xu, L. L. et al. Risk factors for severe low anterior resection syndrome in patients with rectal Cancer undergoing sphincter–preserving resection: a systematic review and Meta–analysis. Oncol. Lett. 27, 30 (2024).
Rosen, H., Sebesta, C. G. & Sebesta, C. Management of low anterior resection syndrome (Lars) following resection for rectal Cancer. Cancers 15, (2023).
Ye, L., Huang, M., Huang, Y., Yu, K. & Wang, X. Risk factors of postoperative low anterior resection syndrome for Colorectal Cancer: a Meta-analysis. Asian J. Surg. 45, 39–50 (2022).
Shin, J. K. et al. Clinical prediction model of pathological response following neoadjuvant chemoradiotherapy for rectal Cancer. Sci. Rep. 12, 7145 (2022).
Al-Sukhni, E. et al. Lymphovascular and Perineural Invasion are Associated with poor prognostic features and outcomes in Colorectal Cancer: a retrospective cohort study. Int. J. Surg. 37, 42–49 (2017).
Wang, Z. et al. Machine learning model for prediction of low anterior resection syndrome following laparoscopic anterior resection of rectal Cancer: a Multicenter Study. World J. Gastroenterol. 29, 2979–2991 (2023).
Yan, M., Lin, Z., Wu, Z., Zheng, H. & Shi, M. A predictive nomogram model for low anterior resection syndrome after rectal Cancer resection. Anz J. Surg. 92, 3224–3231 (2022).
Battersby, N. J. et al. Development and External Validation of a Nomogram and Online Tool to Predict Bowel Dysfunction following restorative rectal Cancer resection: the Polars score. Gut. 67, 688–696 (2018).
Qin, Q. et al. Development and validation of a Post-radiotherapy Prediction Model for Bowel Dysfunction after rectal Cancer resection. Gastroenterology. 165, 1430–1442 (2023).
Ho, H. A. et al. Assessment of Bowel Movement Dysfunction following laparoscopic low anterior resection for rectal Cancer: a single-center study from Vietnam. Eur. Rev. Med. Pharmacol. Sci. 27, 5677–5683 (2023).
Robitaille, S. et al. Predictors of pre- and post-treatment bowel dysfunction severity in patients with rectal Cancer. Surgery. 173, 681–686 (2023).
Acknowledgements
The authors would like to appreciate all the research participants for help in our report. We also sincerely acknowledge the Fourth Hospital of Hebei Medical University for their support.
Funding
Supported by Hebei Province Medical Science Research Key Project (20230828).
Author information
Authors and Affiliations
Contributions
Study concepts and study design: Wenbo Niu and Xuena Zhang. Data acquisition: Qingyu Meng, Jianna Du and Zhongtao Tian. Statistical analysis: Xuena Zhang. Manuscript editing: Xuena Zhang and Qingyu Meng. All authors have reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study received approval from the Ethics Committee of the Fourth Hospital of Hebei Medical University (approval number 2021111), and all patients provided informed consent before their inclusion in the study, adhering to ethical guidelines and standards.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, X., Meng, Q., Du, J. et al. Risk factors of the low anterior resection syndrome (LARS) after ileostomy reversal in rectal cancer patient. Sci Rep 14, 28281 (2024). https://doi.org/10.1038/s41598-024-79283-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79283-5
