
Abstract
This study aimed to evaluate the association between the triglyceride-glucose (TyG) index and high-sensitivity C-reactive protein-to-albumin ratio (hsCAR) and the prognosis of patients with STEMI and hypertension. A total of 699 patients diagnosed with STEMI and hypertension were included in this study database. Compared to the low TyG index group (< 7.8), the high TyG index group (≥ 7.8) was associated with an increased risk of MACE (HR 2.09, 95% CI = 1.58–2.77; P < 0.001). Similarly, a higher hsCAR (≥ 0.15) was linked to an increased risk of MACE (HR 1.46, 95% CI = 1.12–1.90; P = 0.005). Subsequently, we categorized the population into four groups based on the defined cutoff points. Compared to the low TyG–low hsCAR subgroup, the other three subgroups demonstrated an elevated risk of MACE. Among patients treated with PCSK9 and SGLT2 inhibitors, the combined effect of the TyG index and hsCAR on MACE was attenuated. Finally, The combined TyG index and hsCAR model exhibited optimal performance (AUC = 0.71, 95% CI = 0.67–0.75; P < 0.001). This study demonstrates that the TyG index and hsCAR provide strong combined predictive power. The synergistic utilization offers a comprehensive approach to cardiovascular risk assessment.
Similar content being viewed by others
Introduction
Acute coronary syndrome (ACS) remains a leading cause of both morbidity and mortality. The Global Registry of Acute Coronary Events (GRACE) reports a one-year mortality rate of about 15% among ACS patients, with a cumulative five-year mortality rate nearing 20%1. Of all ACS forms, acute ST-segment elevation myocardial infarction (STEMI) is especially severe, underscoring the need for early risk assessment to improve ACS prevention and management of ACS. Additionally, hypertension is a significant contributor to the long-term development of major adverse cardiovascular events (MACE). In China, the rates of awareness, treatment, and control of hypertension are 51.6%, 45.8%, and 16.8%, respectively, underscoring the need for improvement in these areas2,3. Therefore, early detection and timely management of hypertension in patients at risk for cardiovascular disease (CVD) are essential for guiding clinical decisions and reducing the overall burden of CVD.
Metabolic dysregulation and inflammation are intricately linked to cardiovascular diseases4,5. Research has demonstrated that insulin resistance is associated with dyslipidemia, endothelial dysfunction, vascular smooth muscle cell proliferation, inflammation, hypercoagulability, atherosclerosis, and thrombosis6. The triglyceride-glucose (TyG) index is currently recognized as a reliable surrogate marker for insulin resistance assessment7. Evidence indicates that the TyG index is strongly correlated with cardiovascular disease progression, myocardial infarction risk, in-stent restenosis, and the severity of coronary artery disease8,9,10,11. Furthermore, recent findings suggest that a high TyG index could serve as a predictor of adverse outcomes in patients with coronary heart disease and hypertension12.
The high-sensitivity CRP-to-albumin ratio (hsCAR) is a novel inflammatory marker with prognostic value across a range of conditions, including infections, rheumatic diseases, malignancies, and critical illnesses13,14,15,16. As a risk stratification tool, hsCAR has demonstrated strong predictive power for 30-day mortality in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement and serves as an independent mortality predictor in STEMI cases17,18,19. Additionally, hsCAR is a valuable prognostic indicator for patients with coronary chronic total occlusion (CTO) undergoing percutaneous coronary intervention (PCI), enhancing patient stratification20. It also outperforms CRP or albumin levels alone in predicting new-onset atrial fibrillation following coronary artery bypass grafting (CABG)21.
However, the pathophysiology of patients with STEMI and hypertension is complex, and the association between the combined TyG index and hsCAR and clinical outcomes in STEMI patients with hypertension undergoing PCI remains unclear. This study assessed the predictive value of combining the TyG index and hsCAR for MACE incidence in STEMI patients with hypertension post-PCI, providing insights for improving risk stratification in STEMI management.
Methods
Study design and population
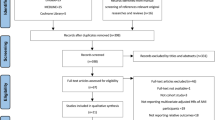
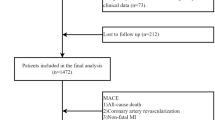
We retrospectively assessed admission data from consecutive STEMI patients in the Hospital Inpatient System database at Tianjin Medical University General Hospital between August 2018 and March 2023. All eligible participants were aged 18 years or older and had a hospital diagnosis of STEMI, with MACE evaluated through in-hospital information and telephone follow-up. Of the 1,262 candidates, 563 participants were excluded based on the study’s exclusion criteria: (1) patients who did not undergo coronary angiography (CAG) or received only CAG (n = 30), (2) those with severe hepatic or renal disease or active infection (n = 15), (3) patients with a history of prior myocardial infarction, PCI or CABG (n = 113), (4) cases with missing clinical data (n = 16), (5) participants lost to follow-up (n = 66), and (6) those who did not meet the diagnostic criteria for hypertension (n = 323). Ultimately, a total of 699 participants were included in this study, with 316 patients experienced MACE during the follow-up period (Fig. S1).
The diagnosis and treatment of STEMI patients were conducted according to established guidelines22,23. A patient was classified as a current smoker if they had smoked at least one cigarette per day within the month preceding the index hospitalization24. Diabetes was defined as a previous diagnosis of the disease or prior use of glucose-lowering medications. Hypertension was defined as a prior diagnosis of hypertension, previous antihypertensive treatment, or a new diagnosis made during the index admission. The study protocol adheres to the ethical guidelines of the 1975 Declaration of Helsinki, as evidenced by prior approval from the Ethics Committee of Tianjin Medical University General Hospital (Approval No: IRB2023-YX-301-01/2023). For this retrospective analysis of clinically acquired data, the institutional review board waived the requirement for written informed consent.
Sample size calculation
A formal sample size calculation was conducted using the Schoenfeld formula for Cox proportional hazards models. Based on prior literature on STEMI patients with hypertension, a hazard ratio (HR) of 1.5 was assumed, with an estimated event rate of 35% for MACE, consistent with existing studies25,26.
The calculation targeted a significance level (α) of 0.05 and a statistical power of 80%. After accounting for potential confounding factors, an adjustment factor of 1.2 to 1.3 was applied, resulting in a minimum required sample size of 252–273 patients. The final cohort included 699 participants, exceeding this requirement and ensuring sufficient statistical power.
Data collection and definitions
Data were extracted and processed from existing inpatient and outpatient medical records. Baseline information collected for each patient included demographics, clinical history, hematological parameters, echocardiographic findings, and percutaneous coronary intervention data. Demographic data included sex, age, height, weight (used to compute body mass index [BMI]), heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and smoking status. Clinical history covered diagnoses of diabetes and stroke. Hematological parameters included platelet count, hemoglobin, serum albumin, total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), high-sensitivity C-reactive protein (hs-CRP), serum creatinine (Scr), B-type natriuretic peptide (BNP), fasting blood glucose (FBG), and glycated hemoglobin A1c (HbA1c). The estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) formula. FBG and TG levels were initially converted from mmol/L to mg/dL, and the TyG index was calculated as the natural logarithm of [fasting TG (mg/dL) × FBG (mg/dL) / 2]. The hsCAR was calculated as the high-sensitivity CRP-to-albumin ratio. Echocardiographic features included left ventricular ejection fraction (LVEF). The PCI data included surgical strategy, number of stents, and coronary artery lesions. The SYNergy between PCI with TAXUS and Cardiac Surgery (SYNTAX) and residual SYNTAX (rSS) scores were calculated based on the coronary artery lesion characteristics before and after the procedure. The GRACE score is derived from a comprehensive assessment of clinical parameters. Medication data were recorded.
Percutaneous coronary intervention
Percutaneous coronary intervention (PCI) involves balloon dilation and/or stent implantation for infarct-related vessels, performed by experienced operators following standard techniques. Before the procedure, all patients received aspirin (300 mg), ticagrelor (180 mg) or clopidogrel (300 mg). After the procedure, aspirin (100 mg, QD), ticagrelor (90 mg, Q12H), or clopidogrel (75 mg, QD) was administered. Statins, angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs)/angiotensin receptor and neprilysin inhibitors (ARNIs) and beta-blockers were routinely administered to all patients without contraindications. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) and proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9i) were prescribed based on blood glucose, cardiac function, and LDL-C during hospitalization.
Follow-up and endpoints
Clinical follow-up data were obtained from hospital records or through telephone interviews conducted by skilled clinicians with patients and their families, with standardized computerized case report forms were completed. The study endpoint was the occurrence of MACE during the follow-up period after PCI. MACE included all-cause death, nonfatal myocardial infarction, repeat revascularization, heart failure, stroke or transient cerebral ischemia.
Statistical analysis
Continuous variables with a normal distribution are reported as means with standard deviations, while those with a skewed distribution are expressed as medians with the interquartile range (25th to 75th percentiles). Baseline demographic and clinical characteristics were compared among patients with different outcomes and varying TyG indices combined with hsCAR. For categorical variables, the chi-square test was applied. Depending on the data distribution, either one-way ANOVA or the Kruskal‒Wallis test was used for continuous variables.
Multivariable Cox regression models with restricted cubic splines (RCS) were used to explore the potential nonlinear relationship between the TyG index, hsCAR, and MACE occurrence. RCS is a statistical method used to model nonlinear relationships between a continuous independent variable and an outcome. Traditional linear models assume that the effect of a continuous variable on the outcome is constant throughout its range, which may oversimplify complex biological relationships. RCS addresses this limitation by dividing the range of the independent variable into multiple segments (splines) and fitting piecewise cubic polynomials to each segment. The RCS method allows for flexible modeling of continuous variables by fitting smooth curves to the data, without assuming a strictly linear relationship. This is particularly useful in cardiovascular research, where many biomarker effects are not purely linear. We assessed nonlinearity using the Box–Tidwell test and identified the cutoff points for both indicators. When nonlinearity was present, we used RCS to determine the cutoff values for the TyG index and hsCAR, which represent the points where the hazard ratios (HRs) for MACE begin to show a significant increase.
The study population was stratified into four distinct groups based on the combined TyG index and hsCAR. To estimate HRs and 95% confidence intervals (CIs) for each group, we utilized Cox regression models, constructing five separate models as follows: Model 1, unadjusted; Model 2, adjusted for sex, age, and BMI; Model 3, including Model 2 variables plus heart rate, SBP, DBP, smoking status, diabetes status, history of stroke, LVEF, and SYNTAX score; Model 4, building on Model 3 by incorporating rSS, number of stents, antiplatelet therapy, beta-blockers, ACEIs/ARBs/ARNIs, hemoglobin, platelet count, eGFR, HbA1c, and LDL-C; Model 5, applying bootstrapping techniques to enhance statistical robustness. Additional subgroup analyses were conducted to assess whether the impact of the TyG index combined with the hsCAR on MACE differed across subgroups. Finally, we computed the area under the curve (AUC) for the TyG index, hsCAR, and their combination to evaluate MACE predictive ability and compared these predictors with the traditional GRACE score model.
All analyses were conducted using Stata (version 16; StataCorp, College Station, TX), with a two-tailed P-value of < 0.05 considered statistically significant.
Results
Comparison of baseline characteristics between groups
From August 2018 to March 2023, a study at Tianjin Medical University General Hospital initially identified 1,262 STEMI patients, of whom 699 met the inclusion criteria and were enrolled. During follow-up, 316 of the 699 patients (45.2%) developed MACE. The baseline characteristics of patients with and without MACE were compared (Table S1). Patients with MACE had higher SBP, a greater incidence of diabetes, and elevated SYNTAX and rSS scores, indicating more severe coronary artery disease. Additionally, these patients exhibited more adverse metabolic and inflammatory profiles, as shown by higher levels of laboratory markers such as Scr, BNP, and TG. Furthermore, the TyG index and hsCAR were significantly elevated in the MACE group.
Correlation between the TyG index, hsCAR, and the risk of MACE, and analysis using the Cox proportional hazards model
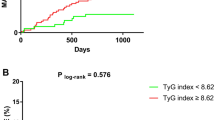
The frequency distributions of the TyG index and hsCAR are shown in Fig. S2. Figure 1A and B illustrate the nonlinear association between the TyG index or hsCAR and the risk of MACE. Specifically, RCS identified threshold points (TyG index ≥ 7.8 and hsCAR ≥ 0.15) at which the risk of MACE began to increase. Beyond these thresholds, the hazard ratio for MACE rose significantly. Figure 1C and D display the MACE risk according to the TyG index and hsCAR grouped by the respective cutoff points. The high TyG index group (≥ 7.8) was associated with a higher risk of MACE compared to the low TyG index group (< 7.8) (HR 2.09, 95% CI: 1.58–2.77; P < 0.001). Similarly, the high hsCAR group (≥ 0.15) was associated with an increased risk of MACE (HR 1.46, 95% CI: 1.12–1.90; P = 0.005).

Restricted Cubic Splines (RCS) and Cox Proportional-Hazards Models for TyG Index and hsCAR with MACE. (A) Multivariable RCS regression shows the nonlinear association between the TyG index and MACE occurrence. The cut-off value of the TyG index for predicting MACE is 7.8. (B) Multivariable RCS regression shows the nonlinear association between hsCAR and MACE occurrence. The cut-off value of hsCAR for predicting MACE is 0.15. (C) Multivariable Cox regression analysis illustrates MACE occurrence in STEMI and hypertension patients by TyG index groups. (D) Multivariable Cox regression analysis illustrates MACE occurrence in STEMI and hypertension patients by hsCAR groups.
Comparison of baseline characteristics by TyG index and hsCAR grouping
The population was categorized into four groups based on the cutoff points of these indicators: low TyG, low hsCAR; low TyG, high hsCAR; high TyG, low hsCAR; and high TyG, high hsCAR. Table 1 illustrates the baseline characteristics of these four groups. Compared to those in the low TyG-low hsCAR subgroup, patients in the other subgroups had a higher incidence of diabetes, elevated SYNTAX and rSS scores, gradually increasing lipid metabolism indices, and a greater proportion of individuals using PCSK9i and SGLT2i posthospitalization.
Cox proportional hazards model analysis of MACE occurrence based on combined TyG index and hsCAR
Table 2; Fig. 2 illustrate the combined impact of the TyG index and hsCAR on MACE. In the unadjusted model (Model 1), all three groups had a higher risk of MACE than the low TyG–low hsCAR subgroup. Even after successive adjustments, the high TyG–low hsCAR and high TyG–high hsCAR groups continued to show an elevated risk of MACE (HR 1.99, 95% CI = 1.28–3.09; HR 2.94, 95% CI = 2.01–4.30, respectively, in Model 4). Further robustness of the results was confirmed through bootstrapping.

Combined Impact of TyG Index and hsCAR on MACE. All three groups show a higher MACE risk compared to the low TyG–low hsCAR subgroup.
Subgroup analysis
Table 3 presents the results of the subgroup analysis. Regarding age and sex, the combined impact of the TyG index and hsCAR on MACE was similar. However, in patients with diabetes, those with a SYNTAX score < 22, and those treated with a PCSK9i or SGLT2i, the combined effect of the TyG index and hsCAR on MACE appeared attenuated.
Finally, we employed Receiver Operating Characteristic (ROC) analysis to assess the impact of combining the TyG index and hsCAR on MACE risk compared to using each indicator individually. The results indicated that the combined TyG index and hsCAR demonstrated optimal model performance (AUC = 0.71, 95% CI = 0.67–0.75; P < 0.001) (Fig. 3). Additionally, the combined TyG index and hsCAR were compared with the traditional GRACE score risk prediction model, and the results revealed that the combination outperformed the GRACE score (AUC = 0.71, 95% CI: 0.67–0.75 vs. AUC = 0.57, 95% CI: 0.52–0.61; P < 0.001) (Fig. 4).

Receiver Operating Characteristic (ROC) curve for Predicting MACE. The combined TyG index and hsCAR model exhibits optimal performance for MACE prediction.

Comparison of Predictive Models for MACE. The ROC evaluation demonstrates that the combined TyG index and hsCAR model outperforms the GRACE score risk prediction model.
Discussion
This study provides novel insights into the combined predictive value of the TyG index and hsCAR for MACE among STEMI patients with hypertension post-PCI. While these markers have been previously studied individually, our work is among the first to assess their synergistic effect in this high-risk population. This combined approach enhances risk stratification, offering better predictive power than either marker alone. The cutoff values for the TyG index (≥ 7.8) and hsCAR (≥ 0.15) were determined using RCS analysis, identifying points where the risk of MACE significantly increased. These cutoffs align with prior research: for example, a TyG index of 7.8 has been shown by Tao et al. and Tian et al. to correlate with heightened cardiovascular risk8. Similarly, an hsCAR threshold of 0.15 has been validated in studies by Acet et al. and Wang et al., where it predicted adverse outcomes in STEMI patients undergoing PCI25,27. Thus, our findings not only reflect statistical inflection points but are also consistent with established literature, supporting their application in risk stratification. This study also found a reduced stratification effect in patients treated with PCSK9i or SGLT2i, suggesting that these therapies might alter cardiovascular risk linked to specific biomarker levels. These findings suggest that integrating both markers into clinical practice could improve personalized management strategies, enabling more targeted interventions for high-risk patients.
The TyG index, a surrogate marker of insulin resistance, has been strongly associated with CVD. A study involving 2,107 non-ST-segment elevation acute coronary syndrome (NST-ACS) patients who underwent PCI revealed that the TyG index had the strongest correlation with the MACE risk compared to other insulin resistance surrogate markers28. This relationship highlights the pivotal role of metabolic dysregulation in cardiovascular risk. Notably, the TyG index has consistently emerged as a robust predictor of cardiovascular events and mortality across various studies29,30,31,32,33,34,35. Additionally, some researchers have found that combining the TyG index with plaque characteristics observed via intravascular optical coherence tomography (OCT) or postoperative quantitative flow ratio (QFR) values can better predict the MACE risk in STEMI patients36,37. Recent studies have also shown a relationship between the TyG index and adverse cardiovascular events in patients with coronary heart disease and hypertension12. The findings of this study further underscore the significance of the TyG index as a key marker for assessing cardiovascular risk, particularly in STEMI patients and hypertension.
Similarly, hsCAR, a novel marker of inflammation, has demonstrated a strong correlation with cardiovascular diseases. CAR has shown stronger associations with the complexity and severity of CAD than CRP or albumin alone and serves as an independent predictor for the intermediate-high SYNTAX score group38. In a study of 539 STEMI patients undergoing primary PCI, hsCAR outperformed CRP (AUC = 0.770 vs. 0.761) and albumin (AUC = 0.770 vs. 0.658) in predicting MACE27. Another study of 659 acute coronary syndrome patients found that those in the high-hsCAR group had a 27.6% greater risk of MACE than those in the low-hsCAR group25. Finally, a study of 9,375 coronary heart disease patients receiving drug-eluting stent implantation found hsCAR to be an independent predictor of adverse cardiovascular events and myocardial infarction occurrence39. The substantial predictive value of hsCAR for MACE observed in this study aligns with existing literature, positioning inflammation as a fundamental driver of atherosclerosis and subsequent cardiovascular events. This study provides further evidence of hsCAR as an independent predictor of adverse cardiovascular outcomes, underscoring its utility in clinical risk assessment.
The interplay between the TyG index and the hsCAR in predicting CVD represents a critical aspect of this study’s findings. The combined utilization of these two markers offers a synergistic approach to risk assessment. To further validate the clinical utility of the TyG index and hsCAR combination, we compared its predictive performance with the established GRACE score. The combined TyG index and hsCAR demonstrated superior predictive performance for MACE compared to the traditional GRACE score, underscoring the added value of incorporating metabolic and inflammatory markers into risk stratification for STEMI patients with hypertension. While the GRACE score remains a widely used tool, its reliance primarily on clinical parameters may overlook critical aspects of metabolic dysfunction and systemic inflammation, both of which play pivotal roles in cardiovascular disease progression, particularly in high-risk populations40. Emerging evidence suggests that markers such as the TyG index and hsCAR are not only indicative of underlying metabolic and inflammatory disturbances but are also directly associated with adverse cardiovascular outcomes8,27. This finding aligns with recent studies showing that metabolic-inflammatory markers can more accurately capture the complex pathophysiology in patients with comorbid conditions like hypertension and STEMI41. Therefore, integrating these biomarkers could enhance risk prediction beyond what traditional models achieve, providing clinicians with a more nuanced tool for identifying high-risk patients and tailoring interventions accordingly. Further research should assess how combining these markers with clinical scores could improve prediction accuracy across diverse patient groups and settings. Such studies would help determine whether an updated model combining GRACE with TyG index and hsCAR might offer an optimized risk assessment approach.
The subgroup analysis in this study reveals nuanced insights into the impact of various factors on risk stratification. Specifically, the study highlights the differential influence of diabetes status, SYNTAX score, and the use of PCSK9i or SGLT2i on biomarker-based risk stratification. This differentiation underscores the critical role that underlying disease states and therapeutic interventions play in shaping the predictive accuracy of the TyG index and hsCAR. This finding is clinically significant and suggests that early use of PCSK9i and SGLT2i may improve the prognosis of high-risk patients with elevated TyG index and a high hsCAR. In a prospective study involving 1,541 STEMI patients undergoing primary PCI, elevated PCSK9 levels were associated with all-cause and cardiac-related mortality when TyG levels were above the median but not when they were below the median. These findings suggest that reducing circulating PCSK9 levels may potentially improve insulin resistance in STEMI patients42. This result emphasizes the need for a personalized approach to risk assessment and management in clinical practice.
The combined predictive effect of the TyG index and hsCAR in cardiovascular diseases primarily arises from their ability to capture two key drivers of cardiovascular pathophysiology: metabolic dysregulation and systemic inflammation. The TyG index reflects insulin resistance, which disrupts glucose and lipid metabolism, leading to chronic inflammation and oxidative stress43,44. This process accelerates atherosclerosis development by increasing pro-inflammatory cytokines production, such as TNF-α and IL-6, which damage the endothelium and promote plaque formation41. Simultaneously, insulin resistance impairs nitric oxide synthesis, reducing its bioavailability and causing endothelial dysfunction. This dysfunction not only triggers vasoconstriction and hypertension but also exacerbates inflammation and oxidative stress, further advancing atherosclerosis6,45. Conversely, hsCAR, as a marker of systemic inflammation, reflects the inflammatory burden in cardiovascular diseases, indicated by elevated high-sensitivity CRP levels and reduced albumin, markers of poor nutritional status and heightened inflammation25. During inflammation, immune cells like macrophages and neutrophils release pro-inflammatory cytokines that disrupt endothelial cell function and generate large quantities of reactive oxygen species (ROS). These ROS not only directly damage tissues but also worsen metabolic disturbances, such as insulin resistance and lipid peroxidation46,47. Additionally, inflammation enhances platelet adhesion and activation, promoting thrombosis formation48. Recent studies also suggest that inflammation is associated with ischemia in patients with non-obstructive coronary arteries49.The interaction between these biomarkers suggests that insulin resistance intensifies systemic inflammation, while inflammation further exacerbates metabolic dysregulation, creating a cycle that elevates the risk of cardiovascular events50,51. The combination of TyG and hsCAR provides a more comprehensive cardiovascular risk assessment by integrating these metabolic and inflammatory pathways. This synergistic approach enhances risk stratification and may aid in identifying patients who could benefit from early interventions, such as SGLT2i and PCSK9i targeting dysregulation of glucose and lipid metabolism, along with anti-inflammatory treatments like colchicine. Further research is warranted to elucidate the molecular mechanisms driving this metabolic-inflammatory interaction and optimize therapeutic strategies for high-risk individuals.
This study demonstrates that the combined use of the TyG index and hsCAR significantly improves the predictive power for MACE in STEMI patients with hypertension, providing a clear basis for personalized treatment. For patients with elevated TyG and hsCAR, early intervention with PCSK9 inhibitors or SGLT2 inhibitors is recommended to reduce cardiovascular events. Additionally, integrating TyG and hsCAR into existing clinical risk assessment tools, such as the GRACE or TIMI scores, may further enhance the identification of high-risk patients. This multidimensional approach to risk stratification can help clinicians tailor treatment plans, optimize resource allocation, and ultimately reduce the incidence of MACE.
While this study offers valuable insights, certain limitations should be acknowledged. Although the sample size was sufficient to meet statistical power requirements for detecting significant effects, the single-center, retrospective design may limit the generalizability of these findings. Additionally, excluding patients with incomplete data may have introduced selection bias. Acute stress from STEMI onset could influence insulin resistance and inflammatory marker levels, especially as laboratory parameters were measured only once at admission. This single-time-point measurement may overlook dynamic biomarker changes, potentially impacting the analysis. Larger, prospective, multicenter studies incorporating repeated biomarker assessments would help validate these results and provide deeper insights into risk stratification.
Conclusions
Our findings highlight the strong combined predictive value of the TyG index and hsCAR for MACE in high-risk patients with STEMI and hypertension, supporting their integration into clinical risk stratification. Future research should validate these markers across broader populations and explore targeted interventions to improve outcomes for high-risk individuals.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ACS:
-
acute coronary syndrome
- ACEI:
-
angiotensin-converting enzyme inhibitor
- ARB:
-
angiotensin receptor blocker
- ARNI:
-
angiotensin receptor and neprilysin inhibitor
- BMI:
-
body mass index
- BNP:
-
B-type natriuretic peptide
- CAD:
-
coronary artery disease
- CVD:
-
cardiovascular disease
- DBP:
-
diastolic blood pressure
- FBG:
-
fasting blood glucose
- GLP1-RA:
-
glucagon-like peptide-1 receptor agonist
- hsCRP:
-
high-sensitivity C-reactive protein
- HDL-C:
-
high-density lipoprotein cholesterol
- HbA1c:
-
glycated hemoglobin A1c
- LVEF:
-
left ventricular ejection fraction
- LDL-C:
-
low-density lipoprotein cholesterol
- MRA:
-
mineralocorticoid receptor antagonist
- MACEs:
-
major adverse cardiovascular events
- PCI:
-
percutaneous coronary intervention
- PCSK9i:
-
proprotein convertase subtilisin/kexin type 9 inhibitor
- rSS:
-
residual SYNTAX score
- ROC:
-
receiver operating characteristic
- SBP:
-
systolic blood pressure
- Scr:
-
serum creatinine
- SYNTAX score:
-
SYNergy between PCI with TAXUS and Cardiac Surgery score
- STEMI:
-
ST-elevation myocardial infarction
- SGLT2i:
-
sodium–glucose cotransporter 2 inhibitor
- TyG:
-
triglyceride glucose
- TNT:
-
troponin T
- TC:
-
total cholesterol
- TG:
-
triglyceride
References
Fox, K. A. et al. Underestimated and under-recognized: the late consequences of acute coronary syndrome (GRACE UK-Belgian study). Eur. Heart J. 31, 2755–2764. https://doi.org/10.1093/eurheartj/ehq326 (2010).
Wang, Z. et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. 137, 2344–2356. https://doi.org/10.1161/circulationaha.117.032380 (2018).
Joint Committee for Guideline Revision. Chinese guidelines for prevention and treatment of hypertension—a report of the revision committee of Chinese guidelines for prevention and treatment of hypertension. J. Geriatr. Cardiol. 16, 182–241 (2019). (2018). https://doi.org/10.11909/j.issn.1671-5411.2019.03.014
Karakayalı, M. et al. Relationship between nonobstructive coronary arteries and metabolic parameters. Kafkas J. Med. Sci. 14, 138–143 (2024).
Karakayali, M. et al. The relationship between the systemic immune-inflammation index and reverse-dipper circadian pattern in newly diagnosed hypertensive patients. J. Clin. Hypertens. 25, 700–707. https://doi.org/10.1111/jch.14688 (2023).
Ormazabal, V. et al. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 17, 122. https://doi.org/10.1186/s12933-018-0762-4 (2018).
Li, S., An, L., Fu, Z., Zhang, W. & Liu, H. Association between triglyceride-glucose related indices and all-cause and cause-specific mortality in the general population: a cohort study. Cardiovasc. Diabetol. 23, 286. https://doi.org/10.1186/s12933-024-02390-0 (2024).
Tao, L. C., Xu, J. N., Wang, T. T., Hua, F. & Li, J. J. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc. Diabetol. 21, 68. https://doi.org/10.1186/s12933-022-01511-x (2022).
Tian, X. et al. Triglyceride-glucose index is associated with the risk of myocardial infarction: an 11-year prospective study in the Kailuan cohort. Cardiovasc. Diabetol. 20, 19. https://doi.org/10.1186/s12933-020-01210-5 (2021).
Zhu, Y. et al. Triglyceride-glucose index is associated with in-stent restenosis in patients with acute coronary syndrome after percutaneous coronary intervention with drug-eluting stents. Cardiovasc. Diabetol. 20, 137. https://doi.org/10.1186/s12933-021-01332-4 (2021).
Su, J. et al. Triglyceride glucose index for the detection of the severity of coronary artery disease in different glucose metabolic states in patients with coronary heart disease: a RCSCD-TCM study in China. Cardiovasc. Diabetol. 21, 96. https://doi.org/10.1186/s12933-022-01523-7 (2022).
Tao, S. et al. Association between the triglyceride-glucose index and 1-year major adverse cardiovascular events in patients with coronary heart disease and hypertension. Cardiovasc. Diabetol. 22, 305. https://doi.org/10.1186/s12933-023-02018-9 (2023).
Ranzani, O. T., Zampieri, F. G., Forte, D. N., Azevedo, L. C. & Park, M. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One. 8, e59321. https://doi.org/10.1371/journal.pone.0059321 (2013).
Afifi, N., Medhat, B. M., Ghani, A. M. A., Hassan, H. G. E. M. A. & Behiry, M. E. Value of albumin-fibrinogen ratio and CRP-albumin ratio as predictor markers of disease activity in Egyptian RA patients, correlated with musculoskeletal sonography. Open. Access. Rheumatol. 12, 241–248. https://doi.org/10.2147/oarrr.S268668 (2020).
Oubaya, N. et al. Prognostic value of routinely measured inflammatory biomarkers in older cancer patients: pooled analysis of three cohorts. Cancers. 13, 6154. https://doi.org/10.3390/cancers13246154 (2021).
Park, J. E. et al. The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients. J. Clin. Med. 7, 333. https://doi.org/10.3390/jcm7100333 (2018).
Seoudy, H. et al. C-reactive protein to albumin ratio in patients undergoing transcatheter aortic valve replacement. Mayo Clin. Proc. 97, 931–940. https://doi.org/10.1016/j.mayocp.2021.11.022 (2022).
Katkat, F. et al. C-reactive protein to albumin ratio as a novel inflammatory-based marker for 30-day mortality in patients undergoing transcatheter aortic valve replacement. Braz J. Cardiovasc. Surg. 37, 292–300. https://doi.org/10.21470/1678-9741-2020-0482 (2022).
Söğüt, Ö., Akdemir, T. & Can, M. M. Prognostic value of the C-reactive protein to albumin ratio in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Turk. J. Med. Sci. 51, 1281–1288. https://doi.org/10.3906/sag-2003-188 (2021).
Cheng, L. et al. The usefulness of C-reactive protein to albumin ratio in the prediction of adverse cardiovascular events in coronary chronic total occlusion undergoing percutaneous coronary intervention. Front. Cardiovasc. Med. 8, 731261. https://doi.org/10.3389/fcvm.2021.731261 (2021).
Ma, M., He, L. & Zhou, L. Comment on relationship between C-reactive protein/albumin ratio and new-onset atrial fibrillation after coronary artery bypass grafting. Rev. Assoc. Med. Bras. 68, 742–743. https://doi.org/10.1590/1806-9282.20220341 (2022).
Thygesen, K. et al. Fourth universal definition of myocardial infarction (2018). Circulation. 138, e618–e651. https://doi.org/10.1161/cir.0000000000000617 (2018).
Ibanez, B. et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European society of cardiology (ESC). Eur. Heart J. 39, 119–177. https://doi.org/10.1093/eurheartj/ehx393 (2018).
Figtree, G. A. et al. Mortality in STEMI patients without standard modifiable risk factors: a sex-disaggregated analysis of SWEDEHEART registry data. Lancet. 397, 1085–1094. https://doi.org/10.1016/s0140-6736(21)00272-5 (2021).
Wang, W. et al. High sensitivity C-reactive protein to prealbumin ratio measurement as a marker of the prognosis in acute coronary syndrome. Sci. Rep. 9, 11583. https://doi.org/10.1038/s41598-019-48189-y (2019).
Gencer, B. et al. Prognostic value of C-reactive protein and albumin in ST-segment elevation myocardial infarction patients. Eur. Heart J. 42, 2310–2320. https://doi.org/10.1093/eurheartj/ehab229 (2021).
Acet, H., Güzel, T., Aslan, B., Isik, M. A. & Ertas, F. Predictive value of C-reactive protein to albumin ratio in ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention. Angiology. 72, 244–251. https://doi.org/10.1177/0003319720963697 (2021).
Zhao, Q. et al. Comparison of various insulin resistance surrogates on prognostic prediction and stratification following percutaneous coronary intervention in patients with and without type 2 diabetes mellitus. Cardiovasc. Diabetol. 20, 190. https://doi.org/10.1186/s12933-021-01383-7 (2021).
Hu, C. et al. Discordance between the triglyceride glucose index and fasting plasma glucose or HbA1C in patients with acute coronary syndrome undergoing percutaneous coronary intervention predicts cardiovascular events: a cohort study from China. Cardiovasc. Diabetol. 19, 116. https://doi.org/10.1186/s12933-020-01091-8 (2020).
Huang, R. et al. Prognostic value of triglyceride glucose (TyG) index in patients with acute decompensated heart failure. Cardiovasc. Diabetol. 21, 88. https://doi.org/10.1186/s12933-022-01507-7 (2022).
Fu, R. et al. Triglyceride glucose index predicts in-hospital mortality in patients with ST-segment elevation myocardial infarction who underwent primary angiography. J. Geriatr. Cardiol. 20, 185–194. https://doi.org/10.26599/1671-5411.2023.03.001 (2023).
Şaylık, F., Çınar, T., Selçuk, M. & Tanboğaİ, H. The predictive value of triglyceride-glucose index for in-hospital and one-year mortality in elderly non-diabetic patients with ST-segment elevation myocardial infarction. J. Geriatr. Cardiol. 19, 610–617. https://doi.org/10.11909/j.issn.1671-5411.2022.08.006 (2022).
Zhao, Q. et al. Impacts of triglyceride-glucose index on prognosis of patients with type 2 diabetes mellitus and non-ST-segment elevation acute coronary syndrome: results from an observational cohort study in China. Cardiovasc. Diabetol. 19, 108. https://doi.org/10.1186/s12933-020-01086-5 (2020).
Zhao, Q. et al. Triglyceride-glucose index as a surrogate marker of insulin resistance for predicting cardiovascular outcomes in nondiabetic patients with non-ST-segment elevation acute coronary syndrome undergoing percutaneous coronary intervention. J. Atheroscler Thromb. 28, 1175–1194. https://doi.org/10.5551/jat.59840 (2021).
Luo, E. et al. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc. Diabetol. 18, 150. https://doi.org/10.1186/s12933-019-0957-3 (2019).
Zhao, X. et al. Triglyceride glucose index combined with plaque characteristics as a novel biomarker for cardiovascular outcomes after percutaneous coronary intervention in ST-elevated myocardial infarction patients: an intravascular optical coherence tomography study. Cardiovasc. Diabetol. 20, 131. https://doi.org/10.1186/s12933-021-01321-7 (2021).
Yu, B. et al. Triglyceride-glucose index is associated with quantitative flow ratio in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Front. Cardiovasc. Med. 9, 1002030. https://doi.org/10.3389/fcvm.2022.1002030 (2022).
Karabağ, Y. et al. Relationship between C-reactive protein/albumin ratio and coronary artery disease severity in patients with stable angina pectoris. J. Clin. Lab. Anal. 32, e22457. https://doi.org/10.1002/jcla.22457 (2018).
Yang, J. et al. The association between high-sensitivity C-reactive protein/albumin ratio and cardiovascular prognosis in patients undergoing percutaneous coronary intervention. Angiology. 73, 818–826. https://doi.org/10.1177/00033197221110715 (2022).
Eagle, K. A. et al. A validated prediction model for all forms of acute coronary syndrome. JAMA. 291, 2727–2733. https://doi.org/10.1001/jama.291.22.2727 (2004).
Libby, P., Ridker, P. M. & Maseri, A. Inflammation and atherosclerosis. Circulation. 105, 1135–1143. https://doi.org/10.1161/hc0902.104353 (2002).
Zhao, X. et al. Effect of triglyceride-glucose indices and circulating PCSK9-associated cardiovascular risk in STEMI patients with primary percutaneous coronary artery disease: a prospective cohort study. J. Inflamm. Res. 16, 269–282. https://doi.org/10.2147/jir.S389778 (2023).
Li, T. et al. Inflammation and insulin resistance in diabetic chronic coronary syndrome patients. Nutrients. 15, 2808. https://doi.org/10.3390/nu15122808 (2023).
Yang, Q., Vijayakumar, A. & Kahn, B. B. Metabolites as regulators of insulin sensitivity and metabolism. Nat. Rev. Mol. Cell. Biol. 19, 654–672. https://doi.org/10.1038/s41580-018-0044-8 (2018).
Hill, M. A. et al. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism. 119, 154766. https://doi.org/10.1016/j.metabol.2021.154766 (2021).
Libby, P., Ridker, P. M. & Hansson, G. K. Leducq Transatlantic Network on atherothrombosis. Inflammation in atherosclerosis: from pathophysiology to practice. J. Am. Coll. Cardiol. 54, 2129–2138. https://doi.org/10.1016/j.jacc.2009.09.009 (2009).
Houstis, N., Rosen, E. D. & Lander, E. S. Reactive oxygen species have a causal role in multiple forms of insulin resistance. Nature. 440, 944–948. https://doi.org/10.1038/nature04634 (2006).
Libby, P. & Simon, D. I. Inflammation and thrombosis: the clot thickens. Circulation. 103, 1718–1720. https://doi.org/10.1161/01.cir.103.13.1718 (2001).
Karakayali, M. et al. The relationship between the systemic immune-inflammation index and ischemia with non-obstructive coronary arteries in patients undergoing coronary angiography. Arq. Bras. Cardiol. 121, e20230540 (2024).
Fahed, G. et al. Metabolic syndrome: updates on pathophysiology and management in 2021. Int. J. Mol. Sci. 23, 786. https://doi.org/10.3390/ijms23020786 (2022).
Clemente-Suárez, V. J. et al. New insights and potential therapeutic interventions in metabolic diseases. Int. J. Mol. Sci. 24, 10672. https://doi.org/10.3390/ijms241310672 (2023).
Acknowledgements
We thank the patients and their families for their support and understanding.
Funding
This study was supported by the Suzhou Industrial Park Xinxin Cardiovascular Health Foundation (Grant No. 2020-CAA-ACCESS-151). The funder had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
SX: Conceptualization, methodology, funding acquisition, writing-review and editing. QY: Conceptualization, methodology, funding acquisition. JH: Methodology, data curation, visualization, writing-original draft preparation. JZ: Data curation, formal analysis, visualization. LL: Formal analysis. MC: Data curation. YL: Data curation. XY: Data curation. SD: Data curation. QW: Data curation. JC: Data curation. All the authors have and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Tianjin Medical University General Hospital (approval no. IRB2023-YX-301-01/2023). As this was a retrospective analysis of clinically acquired data, the institutional review board waived the requirement for written informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, J., Zhang, J., Li, L. et al. Triglyceride-glucose index and hsCRP-to-albumin ratio as predictors of major adverse cardiovascular events in STEMI patients with hypertension. Sci Rep 14, 28112 (2024). https://doi.org/10.1038/s41598-024-79673-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79673-9
