
Abstract
Endometriosis is a chronic inflammatory disease and an estrogen-dependent disease, so dietary factors that can modulate estrogen activity may be clinically important. Dietary fiber, widely distributed in vegetables and fruits, is closely associated with a plant-based diet. Therefore, this study aims to analyze and explore the relationship between dietary fiber intake and the risk of endometriosis providing insights for future clinical significance and treatment approaches. This cross-sectional study obtained data from the National Health and Nutrition Examination Survey (NHANES) 1999–2006 for women aged 20–54 years. A total of 2840 subjects were finally included for analysis, 2599 (91.51%) in the non-endometriosis group and 241 (8.49%) in the endometriosis group. The study used dietary fibre intake as exposure variable and endometriosis risk as outcome variable. Through the use of multiple regression modelling, subgroup analyses, smoothed curve fitting, and threshold effect tests, we uncovered a significant link between exposure and outcome. In Model 2 (Multiple regression equation model after adjusting all confounding variables), after adjusting for confounders, dietary fiber intake was negatively associated with the likelihood of developing endometriosis(OR = 0.588, 95% CI = 0.360–0.959, p = 0.041). In subgroup analyses stratified by age, race, BMI, educational level, hypertension, diabetes,and hyperlipidemia, significant interactions were visualised from smoothed fitted curves. In the cross-sectional study, a connection was observed between a higher intake of dietary fiber and a decreased risk of endometriosis.
Similar content being viewed by others


Introduction
The implantation and growth of endometrial cells outside the uterus is the defining feature of endometriosis, a chronic inflammatory disease1,2, often in the pelvic region, such as the ovaries, ligaments, and peritoneum3. Common signs of this condition include discomfort, dysmenorrhea, and persistent pelvic pain, which may also result in fertility issues4,5,6. Roughly 10–15% of women in their reproductive years are impacted by endometriosis7, and the cyclical or continuous pain it causes can last for decades, potentially leading to anxiety and depression in patients and having a negative impact on society8. Hence, it is imperative to research methods of decreasing the likelihood of developing endometriosis.
Currently, the pathological mechanisms of endometriosis remain incompletely understood9, and there are no mature early diagnostic methods or treatment plans available10. A cross-sectional study in 2013 showed that approximately 60% of patients experienced chronic pain regardless of the type of drug treatment, adversely affecting their quality of life11. Similarly, a systematic review in 2017 indicated that 5–59% of patients still experienced pain after drug treatment, with recurrence of pain symptoms in 17–34% of patients after treatment cessation12. Although current research remains limited, dietary intake has significant potential as a nonpharmacologic intervention in the management of endometriosis treatment.
Since endometriosis is an estrogen-dependent disease, dietary factors that modulate estrogen activity may be clinically important13. Despite this, as endometriosis is an estrogen-dependent disease, dietary factors that can modulate estrogen activity may have significant clinical implications13. Previous studies have shown that a diet focused on plant-based foods can lead to higher levels of sex hormone-binding globulin in the blood, resulting in decreased estrogen activity14. At the same time, a clinical trial confirmed that a plant-based diet also has anti-inflammatory properties that can effectively relieve pain caused by the inflammatory response associated with endometriosis15,16,17. In addition, two independent studies have shown that an increased intake of vegetables and fruits may be linked to a decreased risk of endometriosis18,19. However, the focus of the above studies was on plant-based diets, and it is not clear which specific major components of plant-based diets reduce the risk of endometriosis, and it is important to fill this gap in order to rationalize dietary intake patterns for effective management of the condition.
Dietary fiber, widely distributed in vegetables and fruits, is closely associated with a plant-based diet. With the advancement of scientific knowledge on dietary fiber, its definition has expanded to encompass a wider variety of compounds and their crucial physiological functions20. Studies have shown that increasing dietary fiber intake can reduce circulating estrogen levels by about 10–25%21,22, which, because it is an estrogen-dependent disease, can significantly reduce the risk of endometriosis13. Meanwhile, dietary fiber is thought to reduce symptoms, especially pain, by modulating intestinal microecology and reducing inflammatory responses in the body23. However, while existing studies encourage high-fiber diets, the specific recommended intake with the specific mechanism of action of different fiber types in treatment has not been clarified24. Therefore, future research should focus on determining the specific mechanisms of action and optimal intake of different fiber types (e.g. soluble and insoluble fibers) in therapy. This will help to develop more effective nutritional intervention strategies to optimize endometriosis management and treatment outcomes.
The primary objective of this study is to examine and elucidate the connection between dietary fiber consumption and the likelihood of developing endometriosis, utilizing data gathered from the National Health and Nutrition Examination Survey (NHANES), to provide insight for future identification of the exact mechanism of dietary fiber’s role in this disease, so that it can be most effectively applied in clinical practice, and consequently, to improve the quality of life of the patients and the effectiveness of the treatment.
Materials and methods
Study design and participants
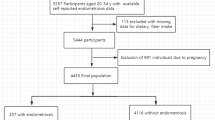
The National Health and Nutrition Examination Survey (NHANES) 1999–2006, administered by the National Center for Health Statistics (NCHS), provided the data for this study. The NHANES survey is a thorough and all-encompassing study that aims to evaluate the health and nutritional wellbeing of the entire U.S. population. It utilizes a sizable and diverse sample, carefully selected through interviews and physical assessments. Ethical approval for all NHANES study protocols was granted by the Research Ethics Review Board at the National Center for Health Statistics, and written informed consent was obtained from each survey participant. All analyses were conducted in accordance with NHANES guidelines and regulations. In this study, 2840 women between the ages of 20–54 were ultimately selected, with 241 (8.49%) having endometriosis and 2599 (91.51%) without the condition. Exclusion criteria included those with incomplete information related to Body Mass Index (BMI) (n = 123), marital status(n = 158), education level (n = 5), Poverty-to-income ratio (PIR) (n = 410), smoking status (n = 1), alcohol use status (n = 488), Metabolic Equivalent Task (MET) score for physical activity (n = 1314), diabetes mellitus (n = 706), hyperlipidemia (n = 1), endometriosis (n = 13), dietary fiber (n = 149) and whether they were pregnant or not (n = 0). Refer to Fig. 1 for the flow chart of the screening process.

Flow diagram.
Assessment of dietary fiber intake
Within the dietary interview segment, there is data recorded regarding the intake of dietary fiber. The information gathered from dietary intake was utilized to approximate the amount and variety of food and drinks consumed within 24 h before the interview, from midnight to midnight and to assess the consumption of energy, nutrients, and other dietary components in these food and drink products.The section on dietary interviews, known as "What We Eat in America" (WWEIA), was created through a partnership between the U.S. Department of Agriculture (USDA) and the U.S. Department of Health and Human Services (DHHS) utilizing the USDA’s Diet Recall Automated Multiple Access system (developed by the Agricultural Research Service) with the Automated Multiple Access (AMPM) tool. All participants in NHANES were qualified for two 24-h dietary recall interviews. The initial dietary recall interview was conducted face-to-face at the examination center (MEC), followed by a second telephone interview within 3–10 days. Dietary intake is the average intake of two 24-h dietary review survey data. If the participant did not participate in the second survey, the participant is eliminated. In 1999–2002, only the first day food recall was publicly available, so only the first day food recall amount was used. In order to ensure the quality and accuracy of interviews, all diet interviewers are required to undergo a rigorous one-week training program and conduct supervised practical interviews before being allowed to work independently.
Assessment of endometriosis
Within the Reproductive Health division, there is information available on endometriosis. The NHANES database defines endometriosis by gathering data from personal interviews, "Has a doctor or other health professional ever told you that you have endometriosis?" Individuals who gave a positive response were categorized as participants. Self-reporting of endometriosis has been shown to be reasonably accurate, with greater than 95% accuracy of reports confirming endometriosis by laparoscopy25.
Assessment of covariates
Information on age, body mass index (BMI), race, education level, marital status, household income to poverty ratio (PIR), physical activity, history of alcohol consumption, history of smoking, hypertension, diabetes mellitus, and hyperlipidemia was also collected from the NHANES data for this study. Participants were categorized into three groups based on age distribution: group 1 (20–32 years old), group 2 (33–41 years old), and group 3 (42–54 years old). BMI was categorized as not overweight (BMI < 25 kg/m2), overweight (BMI = 25–30 kg/m2), obese (BMI > 30 kg/m2)26. The categorization of education level included below high school, high school, and above high school. The data included information on marital status, including married, never married, and divorced. The PIR categorized household income as low (< 1.3), medium (1.3–3.5), and high (≥ 3.5)27. In the world of energy metabolism, the Metabolic Equivalent (MET) reigns supreme as a well-established measure for evaluating relative energy levels during different activities, taking into account energy expenditure while sedentary or at rest28. It is advised to divide physical activity into three distinct tiers: low (< 600 MET-min/week), moderate (600 to 3000 MET-min/week) and high (≥ 3000 MET-min/week)29. Tobacco Use Questionnaire, smoking status was categorized as never, former or light (< 10 cigarettes/day), moderate (10–19 cigarettes/day) or heavy(> or = 20 cigarettes/day)30, while alcohol consumption was categorized as never (had < 12 drinks in lifetime), former (had ≥ 12 drinks in 1 year and did not drink last year, or did not drink last year but drank > 12 drinks in lifetime), light (≥ 1 drinks per day for females, ≥ 2 drinks per day for males), moderate (≥ 2 drinks per day for females, ≥ 3 drinks per day for males, or binge drinking ≥ 2 days per month & binge drinking < 5 days per month), or heavy(≥ 3 drinks per day for females, ≥ 4 drinks per day for males, or binge drinking ≥ 5 days per month)31.
Statistical analyses
Mean (with standard deviation) or median (with interquartile range) were used to define the continuous variables, and the Kruskal Wallis rank-sum test was employed to assess differences between groups; the quantity of cases (n) and percentages (%) within each category were utilized to define categorical variables and were contrasted between groups using the weighted χ2 test. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed through logistic regression models to determine the correlation between dietary fiber intake and endometriosis risk. The unadjusted model was univariate. Age, race, BMI, education level, and marital status were taken into account when adjusting for model 1. Model 2 was extensively calibrated to include all sociodemographic factors (age, education level, marital status, and household PIR), race, smoking status, BMI, physical activity, hypertension, diabetes, hyperlipidemia, and alcohol use. Trend test based on median values for each subgroup of dietary fiber. Additionally, we conducted subgroup analyses and utilized smoothed curve fitting to evaluate the potential impact of various factors on the association between dietary fiber intake and endometriosis: age (20–32, 33–41, and 42–54 years), ethnicity, BMI (25, 25–30, and > 30), household PIR (low, moderate, and high), education level (below high school, high school, and above high school), hypertension (yes or no), hyperlipidemia (yes or no) and alcohol use (never drink, previous drink, mild, moderate or severe). Subgroup differences were evaluated through the use of multifactorial logistic regression. And threshold effects were also tested for subgroups that had significant results in the subgroup analyses and showed U-shaped curves in the smoothed curve fitting. In addition, we considered the covariate of menopausal status and performed multivariable regression analyses with increased adjustment for menopausal status. This study used weighted data for analysis because the survey design used by NHANES32. Weighted models mean that in each model we applied a weight suggested by the Centers for Disease Control and Prevention to take into account the oversampling of minorities to provide a final unbiased and accurate estimate of effects for the population33. All analyses were performed using EmpowerStats software (version 4.1), and p < 0.05 was used to indicate statistical significance.
Results
Baseline characteristics of participants
The sample size for our study was 2840 patients, of which 241 (8.49%) were found to have endometriosis. Following the new Nutrition Facts of America (NF) recommendation, a daily fiber intake of 28 g was targeted for a 2000 kcal/d diet34. The distribution of dietary fiber intake was subdivided into four groups based on the distribution of dietary fiber intake. The participants’ baseline characteristics are outlined in Table 1. The results suggest that there were notable distinctions in dietary fiber consumption based on age, race, education level, PIR, smoking patterns, alcohol usage and hyperlipidemia (p < 0.05).
Relationships between dietary fiber and endometriosis
The impact of dietary fiber intake on endometriosis was studied through the creation of three multivariate logistic regression models. After multivariate adjustment for age, education level, marital status, household PIR, ethnicity, smoking status, BMI, physical activity, hypertension, diabetes mellitus, hyperlipidemia, and alcohol use, a inverse correlation was observed between dietary fiber consumption and the likelihood of developing endometriosis. In all three models, only the high dietary fiber intake group (Q4) showed a significant negative association with the prevalence of endometriosis. This relationship remained significant in the fully adjusted Model II: in the high dietary fiber intake group (Q4 : 27.95–111.40), the prevalence of endometriosis was statistically significantly reduced by 41.2% for every 1 g increase in dietary fiber compared to Q1 (p = 0.041). Whereas the relationship was not statistically significant in low (Q2: 10.90–18.12) and medium (Q3: 18.12–27.95) intake groups. Furthermore, p-values for trend test was done (p = 0.037) (Table 2). Smoothed curve-fit plots indicated that the incidence of EM decreased with increasing intake of dietary fiber (Fig. 2). Appendix Table 1 is based on the adjustment of menopausal status variable on the basis of Table 2. Due to the small number of people with data on this variable (N = 303), the result is not significant, and the loss of a large number of population data will greatly reduce the credibility of the result, we decide to include it in the appendix.

Relationship between dietary fiber and endometriosis risk by smooth curve fitting. The red line demonstrates the risk of endometriosis, and the blue ribbons illustrate its 95% confidence interval. The X-axis is dietary fiber (continuous variable), and the Y-axis is endometriosis. Adjustment for: Age; Race; BMI; Marital Status; PIR; Education Level; Physical activity; Hypertension; Diabetes Mellitus; Hyperlipidemia; Smoking Status; Alcohol Use Status.
Stratified analyses based on additional variables
The data presented in Table 3 highlights the potential impact of dietary fiber intake on endometriosis among different subgroups. In the various subgroups stratified by age, race, BMI, education, hypertension, Diabetes Mellitus and hyperlipidemia, with the combination of the smoothed fitted curves visualizes significant interactions (Figs. 3, 4, 5, 6, 7, 8, 9). Age 43–54 years, non-hispanic white, BMI < 25, less than high school, hypertension, non-diabetes mellitus and non-hyperlipidemic showed a significant interaction for dietary fiber intake and endometriosis (all p-values less than 0.05). Age 43–54 years, hypertension, and non-diabetes mellitus showed stratification with inverted U-shaped distribution. The remaining sub-layer groups with significant interactions between dietary fiber intake and endometriosis were negatively correlated. In contrast, there is no significant difference in the relationship between dietary fiber and endometriosis in the different stratified subgroups of PIR and alcohol use status.

Correlation between dietary fiber and endometriosis stratified by Age. In age-stratified analysis, the red line indicates ages 20–32, the green line indicates ages 33–41, and the blue line indicates ages 42–54. Adjustment for: race, BMI, marital status, PIR, education level, MET score for physical activity, hypertension, diabetes mellitus, hyperlipidemia, smoking status, alcohol use status.

Correlation between dietary fiber and endometriosis stratified by Ethnicity. In the Ethnicity-stratified analysis, the red line represents Mexican American, the yellow line represents non-Hispanic black, the green line represents non-Hispanic white, the blue line represents other Hispanic, and the purple line represents other races including multi-racial. Adjustment for: age, BMI, marital status, PIR, education level, MET score for physical activity, hypertension, diabetes mellitus, hyperlipidemia, smoking status, alcohol use status.

Correlation between dietary fiber and endometriosis stratified by BMI. In BMI-stratified analysis, the red line represents BMI < 25, the green line represents BMI > = 25 or < = 30, and the blue line represents BMI > 30. Adjustment for: age, race, marital status, PIR, education level, MET score for physical activity, hypertension, diabetes mellitus, hyperlipidemia, smoking status, alcohol use status.

Correlation between dietary fiber and endometriosis stratified by education level. In the Education Level-stratified analysis, the red line represents under high school, the green line represents high school, and the blue line represents more than high school. Adjustment for: age, race, BMI, marital status, PIR, MET score for physical activity, hypertension, diabetes mellitus, hyperlipidemia, smoking status, alcohol use status.

Correlation between dietary fiber and endometriosis stratified by hypertension. In hypertension-stratified analysis, the red line represents hypertension while the blue line represents no hypertension. Adjustment for: age, race, BMI, marital status, PIR, education level, MET score for physical activity, diabetes mellitus, hyperlipidemia, smoking status, alcohol use status.

Correlation between dietary fiber and endometriosis stratified by diabetes mellitus. In the stratified diabetes analysis, the red line represents diabetes and the blue line represents no diabetes. Adjustment for: age, race, BMI, marital status, PIR, education level, MET score for physical activity, hypertension, diabetes mellitus, hyperlipidemia, smoking status.

Correlation between dietary fiber and endometriosis stratified by hyperlipidemia. In hyperlipidemia-stratified analysis, the red line represents hypertension while the blue line represents no hyperlipidemia. Adjustment for: age, race, BMI, marital status, PIR, education level, MET score for physical activity, hypertension, diabetes mellitus, smoking status, alcohol use status.
Threshold effect analysis
Based on the stratification analysis and smooth curve fitting results, we further performed threshold analysis for significant stratification with inverted U-shaped distribution (age43-54, Hpertension and no Diabetes Mellitus) (Table 4). The inflection point was 9.65 g in the age 43–54 group, 6.15 g in the Hpertension group, and 9.6 g in the no Diabetes Mellitus group. When the dietary fiber intake was less than 9.65 g in the age43-54 population, it was positively correlated with the prevalence of endometriosis. When the dietary fiber intake of age43-54 population was greater than 9.65 g, the dietary fiber intake of Hypertesion population was greater than 6.15 g, and the dietary fiber intake of no Diabetes mellitus population was greater than 9.6 g, there was a significant negative correlation with the prevalence of endometriosis.
Discussion
In a research involving 241 individuals diagnosed with endometriosis and 2599 individuals without the condition, it was found that a high dietary fiber intake is linked to a lower prevalence of endometriosis. By adjusting the degree of dietary fiber intake, the study found that high dietary fiber intake was particularly significant in reducing the risk of endometriosis.
Studies have proven that hormones such as estradiol can promote growth and inflammation of the tissues associated with the endometrium, which can lead to endometriosis13. Thus endometriosis is a hormone-dependent disease35. The role of diet and lifestyle for endometriosis may influence estrogenic activity36. Research on the relationship between dietary fiber and fruit and vegetable intake and endometriosis is relatively limited. A study demonstrates that increased dietary fiber intake reduces serum estrogen concentrations in premenopausal women22, suggesting that it may be beneficial for patients with endometriosis13. This result is consistent with the study of Schwartz et al37. A study in Iran also mentioned that vegetables, fruits and red meat were associated with a lower risk of endometriosis38. However some studies have concluded the opposite39. A study by Savaris et al. showed that endometriosis may be associated with increased intake of dietary fiber40. According to Trabert et al., there is no evidence to suggest a link between endometriosis and dietary fiber consumption41. This may be due to the fact that the population of the study was itself severely deficient in fibre intake, which is conducive to inflammation, or it may be due to the difference in the populations studied as well as the small sample size of the study, which has some sampling error. As for the influence of human intake and endometriosis, studies mainly focus on diet. Annalisa Capannolo and Nina Shigesi mentioned in her study that many immunological symptoms of endometriosis highly coincide with symptoms of wheat sensitivity42,43. As is known for us, there are many active substances in wheat bran, which contains 50% of dietary fiber. In contrast, Fred Brouns contends that the existing research on the connection between gluten and gluten-free diet and endometriosis lacks sufficient clinical support. so it is not recommended that pregnant women and endometriosis patients adopt gluten-free diet as dietary intervention44. In her research, Agata Gorek found that bioactive compounds of plant origin have some potential for treating endometriosis45.
We further analyzed the different sublayers. Hypertesion population was greater than 6.15 g, there was a significant negative correlation with the prevalence of endometriosis. A study on hypertension and endometriosis46 concluded that the inflammatory response due to hypertension has an impact on the incidence of endometriosis, which may contribute to the effect of dietary fiber on the efficacy of endometriosis. In our study, we found that the relationship between excess body mass index and the incidence of endometriosis was significantly negative and excess BMI may lead to the development of some cardiovascular diseases and in the study of Pantelis et al.47 also found that excess body mass index has a strong effect on the incidence of endometriosis. Schwartz37 in their study found that Consumption of foods with high glycemic index increases the risk of endometriosis, which may be the reason why the results of diabetic patients were not significant, while the results of patients without diabetes were significant and inverted U distribution and the inflection point was at 9.6 g. The possible reason for this may be related to the fact that the risk is associated with the type and amount of dietary fiber consumed by the population as mentioned by Harris18 in his study that the fractions that consume less dietary fiber Lack of comprehensive dietary fiber led to a certain degree of increased risk in this population segment, while the American Cancer Society recommended intake of dietary fiber is 20–30 g, too little intake of dietary fiber amplifies the effect of other factors, which may also be the reason for the results of this study. Age at 43–54 was significantly inverted u distribution with the incidence of endometriosis and the inflection point at 9.65 g, the inflection point is still in the lower class compared to the previous intake. Houston48 in a study on age of endometriosis mentioned that the incidence of endometriosis is not high in adolescents (Age 18–30). Considering the lower intake of dietary fibers and the different genetic factors in each individual, the lower intake of dietary fibers may lead to different pathological changes in endometriosis. Non-Hispanic White showed a significant negative correlation with the prevalence of endometriosis. Bougie49 mentioned in his study that the prevalence of endometriosis is higher in Whites in relation to other races. It is also seen in the images of the present study that Non-Hispanic Whites have a relatively high prevalence curve. It can be assumed that higher prevalence rate can help to show that the the effect of the degree of dietary fiber intake on the incidence of endometriosis. The dietary fiber intake of no Diabetes mellitus population was significantly negatively correlated with the incidence of endometriosis,Li et al.50 found that hyperlipidemia was associated with the incidence of endometriosis, probably because adipose tissue promotes the conversion of androgens to estrogens in women51 .The study by Szymańska et al.52 showed that the higher the level of knowledge of the patients, the greater their interest in health behaviors, which may explain why dietary fiber intake was negatively correlated with the incidence of endometriosis in women with education levels lower than high school in our study.
Despite our study’s limitations, there is still room for improvement. First, this cross-sectional study did not establish a causal relationship between dietary fiber intake and the risk of developing endometriosis53. Future longitudinal studies are necessary to determine this relationship. Second, the survey in this study was conducted in the form of a questionnaire through self-reported dietary recall, and some errors in self-reporting of dietary intake were expected54. Dietary recall bias may exist due to the measurement of a single component of the diet due to the large variation in dietary intake from day to day. Third, in the study by Samaneh et al., it is mentioned that dietary fiber can be broken down into insoluble and soluble forms, necessitating specific division afterward38. Endometriosis may be affected differently by different dietary fibers, including those found in vegetables and fruits, as observed in certain studies55. Harris et al.'s research revealed that a higher intake of fruit was correlated with a lower risk of endometriosis, while a higher intake of cruciferous vegetables was linked to an increased risk of the condition18. So the current findings do not give a clear, scientific recommendation56. Fourth, with the aim of comprehending the correlation between dietary fiber intake and the prevalence of endometriosis, our study did not take into account the menopausal status of the women with respect to age, and thus there may be some errors in the classification of age. Fifth, sampling error may have occurred due to the fact that the overall sample was out of NHNAES and was small.
This study has several strengths. First, we used a nationally representative statistical sample of U.S. women, which is representative of the U.S. female population, thus contributing to the generalizability of our findings. Second, our study reinforces our conclusions by controlling for other confounding variables such as age, ethnicity, BMI, PIR, and other rows of comparative studies under different amounts of dietary fiber intake, which makes it easier to observe differences and effects between variables. In addition, we also considered the interaction of various covariates differently stratified on dietary fiber intake and endometriosis to facilitate further identification and exploration of special populations.
Conclusion
In summary, our findings suggest that the higher the intake of dietary fiber, the more effective it is in reducing the risk of endometriosis. Non-hispanic white, BMI < 25, less than high school, non-hyperlipidemic, When the dietary fiber intake of age 43–54 group was greater than 9.65 g, the dietary fiber intake of hypertension group was greater than 6.15 g, and the dietary fiber intake of diabetic group was greater than 9.6 g, the two groups showed a significant negative correlation. When the dietary fiber intake was lower than 9.65 g in 43–54 years old, the two showed a significant positive correlation. Despite this, the connection between age and endometriosis risk remains unclear.
Data availability
This study utilizes datasets from the NHANES repository, which can be found at https://www.cdc.gov/nchs/nhanes/. All data is publicly available.
Abbreviations
- BMI:
-
Body Mass Index
- PIR:
-
Poverty-to-income ratio
- MET:
-
Metabolic equivalent task
References
Tassinari, V. et al. Endometriosis treatment: Role of natural polyphenols as anti-inflammatory agents. Nutrients 15, 2967. https://doi.org/10.3390/nu15132967 (2023).
Zhang, T., De Carolis, C., Man, G. C. W. & Wang, C. C. The link between immunity, autoimmunity and endometriosis: A literature update. Autoimmun. Rev. 17, 945–955. https://doi.org/10.1016/j.autrev.2018.03.017 (2018).
Zondervan, K. T. et al. Endometriosis. Nat. Rev. Dis. Primers 4, 9. https://doi.org/10.1038/s41572-018-0008-5 (2018).
Bulletti, C., Coccia, M. E., Battistoni, S. & Borini, A. Endometriosis and infertility. J. Assist. Reprod. Genet. 27, 441–447. https://doi.org/10.1007/s10815-010-9436-1 (2010).
Rock, J. A. & Markham, S. M. Pathogenesis of endometriosis. Lancet 340, 1264–1267. https://doi.org/10.1016/0140-6736(92)92959-j (1992).
Tanbo, T. & Fedorcsak, P. Endometriosis-associated infertility: Aspects of pathophysiological mechanisms and treatment options. Acta Obstet. Gynecol. Scand. 96, 659–667. https://doi.org/10.1111/aogs.13082 (2017).
Sayasneh, A., Tsivos, D. & Crawford, R. Endometriosis and ovarian cancer: A systematic review. ISRN Obstet. Gynecol. 2011, 140310. https://doi.org/10.5402/2011/140310 (2011).
Chen, L. C. et al. Risk of developing major depression and anxiety disorders among women with endometriosis: A longitudinal follow-up study. J. Affect. Disord. 190, 282–285. https://doi.org/10.1016/j.jad.2015.10.030 (2016).
França, P. R. C., Lontra, A. C. P. & Fernandes, P. D. Endometriosis: A disease with few direct treatment options. Molecules 27, 4034. https://doi.org/10.3390/molecules27134034 (2022).
Kapoor, R., Stratopoulou, C. A. & Dolmans, M. M. Pathogenesis of endometriosis: New insights into prospective therapies. Int. J. Mol. Sci. 22, 11700. https://doi.org/10.3390/ijms222111700 (2021).
De Graaff, A. A. et al. The significant effect of endometriosis on physical, mental and social wellbeing: Results from an international cross-sectional survey. Hum. Reprod. 28, 2677–2685. https://doi.org/10.1093/humrep/det284 (2013).
Becker, C. M., Gattrell, W. T., Gude, K. & Singh, S. S. Reevaluating response and failure of medical treatment of endometriosis: A systematic review. Fertil. Steril. 108, 125–136. https://doi.org/10.1016/j.fertnstert.2017.05.004 (2017).
Barnard, N. D. et al. Nutrition in the prevention and treatment of endometriosis: A review. Front. Nutr. 10, 1089891. https://doi.org/10.3389/fnut.2023.1089891 (2023).
Barnard, N. D., Scialli, A. R., Hurlock, D. & Bertron, P. Diet and sex-hormone binding globulin, dysmenorrhea, and premenstrual symptoms. Obstet. Gynecol. 95, 245–250. https://doi.org/10.1016/s0029-7844(99)00525-6 (2000).
Shah, B. et al. Anti-inflammatory effects of a vegan diet versus the American heart association-recommended diet in coronary artery disease trial. J. Am. Heart Assoc. 7, e011367. https://doi.org/10.1161/jaha.118.011367 (2018).
Teas, J., Vena, S., Cone, D. L. & Irhimeh, M. The consumption of seaweed as a protective factor in the etiology of breast cancer: Proof of principle. J. Appl. Phycol. 25, 771–779. https://doi.org/10.1007/s10811-012-9931-0 (2013).
Wei, Y., Liang, Y., Lin, H., Dai, Y. & Yao, S. Autonomic nervous system and inflammation interaction in endometriosis-associated pain. J. Neuroinflamm. 17, 80. https://doi.org/10.1186/s12974-020-01752-1 (2020).
Harris, H. R., Eke, A. C., Chavarro, J. E. & Missmer, S. A. Fruit and vegetable consumption and risk of endometriosis. Hum. Reprod. 33, 715–727. https://doi.org/10.1093/humrep/dey014 (2018).
Parazzini, F. et al. Selected food intake and risk of endometriosis. Hum. Reprod. 19, 1755–1759. https://doi.org/10.1093/humrep/deh395 (2004).
Mudgil, D. & Barak, S. Composition, properties and health benefits of indigestible carbohydrate polymers as dietary fiber: A review. Int. J. Biol. Macromol. 61, 1–6. https://doi.org/10.1016/j.ijbiomac.2013.06.044 (2013).
Bagga, D. et al. Effects of a very low fat, high fiber diet on serum hormones and menstrual function. Implications for breast cancer prevention. Cancer 76, 2491–2496. https://doi.org/10.1002/1097-0142(19951215)76:12%3c2491::aid-cncr2820761213%3e3.0.co;2-r (1995).
Rose, D. P., Goldman, M., Connolly, J. M. & Strong, L. E. High-fiber diet reduces serum estrogen concentrations in premenopausal women. Am. J. Clin. Nutr. 54, 520–525. https://doi.org/10.1093/ajcn/54.3.520 (1991).
Fuller, S., Beck, E., Salman, H. & Tapsell, L. New horizons for the study of dietary fiber and health: A review. Plant Foods Hum. Nutr. 71, 1–12. https://doi.org/10.1007/s11130-016-0529-6 (2016).
Youseflu, S., Jahanian Sadatmahalleh, S., Mottaghi, A. & Kazemnejad, A. Corrigendum to “The association of food consumption and nutrient intake with endometriosis risk in Iranian women: A case-control study” [Int J Reprod BioMed 2019; 17: 661–670]. Int. J. Reprod. Biomed. 20, 989. https://doi.org/10.18502/ijrm.v20i11.12366 (2022).
Shafrir, A. L. et al. Validity of self-reported endometriosis: A comparison across four cohorts. Hum. Reprod. 36, 1268–1278. https://doi.org/10.1093/humrep/deab012 (2021).
Xie, B. et al. Association between vitamin D and endometriosis among American women: National Health and Nutrition Examination Survey. PloS one 19, e0296190. https://doi.org/10.1371/journal.pone.0296190 (2024).
Fan, C., Zhu, W., He, Y. & Da, M. The association between Life’s Essential 8 and all-cause, cancer and non-cancer mortality in US Cancer Survivors: A retrospective cohort study of NHANES. Prev. Med. 179, 107853. https://doi.org/10.1016/j.ypmed.2024.107853 (2024).
Deng, X., Liu, D., Li, M., He, J. & Fu, Y. Physical activity can reduce the risk of blood cadmium and blood lead on stroke: Evidence from NHANES. Toxicol. Appl. Pharmacol. 483, 116831. https://doi.org/10.1016/j.taap.2024.116831 (2024).
Midgley, A. W., Carroll, S., Marchant, D., McNaughton, L. R. & Siegler, J. Evaluation of true maximal oxygen uptake based on a novel set of standardized criteria. Appl. Physiol. Nutr. Metab. 34, 115–123. https://doi.org/10.1139/h08-146 (2009).
Okuyemi, K. S., Ahluwalia, J. S., Richter, K. P., Mayo, M. S. & Resnicow, K. Differences among African American light, moderate, and heavy smokers. Nicotine Tob. Res. 3, 45–50. https://doi.org/10.1080/14622200020032097 (2001).
Rattan, P. et al. Inverse association of telomere length with liver disease and mortality in the US population. Hepatol. Commun. 6, 399–410. https://doi.org/10.1002/hep4.1803 (2022).
Curtin, L. R. et al. The National Health and Nutrition Examination Survey: Sample Design, 1999–2006. Vital and health statistics. Series 2, Data evaluation and methods research, 1–39 (2012).
Hernaez, R. et al. Association between variants in or near PNPLA3, GCKR, and PPP1R3B with ultrasound-defined steatosis based on data from the third National Health and Nutrition Examination Survey. Clin. Gastroenterol. Hepatol. 11, 1183–1190. https://doi.org/10.1016/j.cgh.2013.02.011 (2013).
Korczak, R. & Slavin, J. L. Definitions, regulations, and new frontiers for dietary fiber and whole grains. Nutr. Rev. 78, 6–12. https://doi.org/10.1093/nutrit/nuz061 (2020).
Chapron, C., Marcellin, L., Borghese, B. & Santulli, P. Rethinking mechanisms, diagnosis and management of endometriosis. Nat. Rev. Endocrinol. 15, 666–682. https://doi.org/10.1038/s41574-019-0245-z (2019).
Jurkiewicz-Przondziono, J., Lemm, M., Kwiatkowska-Pamuła, A., Ziółko, E. & Wójtowicz, M. K. Influence of diet on the risk of developing endometriosis. Ginekologia polska 88, 96–102. https://doi.org/10.5603/GP.a2017.0017 (2017).
Schwartz, N. R. M. et al. Glycemic index, glycemic load, fiber, and gluten intake and risk of laparoscopically confirmed endometriosis in premenopausal women. J. Nutr. 152, 2088–2096. https://doi.org/10.1093/jn/nxac107 (2022).
Samaneh, Y., ShahidehJahanian, S., Azadeh, M. & Anoshirvan, K. The association of food consumption and nutrient intake with endometriosis risk in Iranian women: A case-control study. Int. J. Reprod. Biomed. 17, 661–670. https://doi.org/10.18502/ijrm.v17i9.5102 (2019).
Abramiuk, M. et al. How can selected dietary ingredients influence the development and progression of endometriosis?. Nutrients 16, 154. https://doi.org/10.3390/nu16010154 (2024).
Savaris, A. L. & do Amaral, V. F. Nutrient intake, anthropometric data and correlations with the systemic antioxidant capacity of women with pelvic endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 158, 314–318. https://doi.org/10.1016/j.ejogrb.2011.05.014 (2011).
Trabert, B., Peters, U., De Roos, A. J., Scholes, D. & Holt, V. L. Diet and risk of endometriosis in a population-based case-control study. Br. J. Nutr. 105, 459–467. https://doi.org/10.1017/s0007114510003661 (2011).
Shigesi, N. et al. The association between endometriosis and autoimmune diseases: A systematic review and meta-analysis. Hum. Reprod. Update 25, 486–503. https://doi.org/10.1093/humupd/dmz014 (2019).
Capannolo, A. et al. Non-celiac gluten sensitivity among patients perceiving gluten-related symptoms. Digestion 92, 8–13. https://doi.org/10.1159/000430090 (2015).
Brouns, F. et al. Diet associations in endometriosis: A critical narrative assessment with special reference to gluten. Front. Nutr. 10, 1166929. https://doi.org/10.3389/fnut.2023.1166929 (2023).
Gołąbek, A., Kowalska, K. & Olejnik, A. Polyphenols as a diet therapy concept for endometriosis-current opinion and future perspectives. Nutrients 13, 1347. https://doi.org/10.3390/nu13041347 (2021).
Mu, F. et al. Association between endometriosis and hypercholesterolemia or hypertension. Hypertension 70, 59–65. https://doi.org/10.1161/hypertensionaha.117.09056 (2017).
Pantelis, A., Machairiotis, N. & Lapatsanis, D. P. The formidable yet unresolved interplay between endometriosis and obesity. Sci. World J. 2021, 6653677. https://doi.org/10.1155/2021/6653677 (2021).
Houston, D. E. Evidence for the risk of pelvic endometriosis by age, race and socioeconomic status. Epidemiol. Rev. 6, 167–191. https://doi.org/10.1093/oxfordjournals.epirev.a036270 (1984).
Bougie, O., Yap, M. I., Sikora, L., Flaxman, T. & Singh, S. Influence of race/ethnicity on prevalence and presentation of endometriosis: A systematic review and meta-analysis. Bjog 126, 1104–1115. https://doi.org/10.1111/1471-0528.15692 (2019).
Li, B., Zhang, Y., Zhang, L. & Zhang, L. Association between endometriosis and metabolic syndrome: A cross-sectional study based on the National Health and Nutrition Examination Survey data. Gynecol. Endocrinol. 39, 2254844. https://doi.org/10.1080/09513590.2023.2254844 (2023).
Zheng, R., Du, X. & Lei, Y. Correlations between endometriosis, lipid profile, and estrogen levels. Medicine 102, e34348. https://doi.org/10.1097/md.0000000000034348 (2023).
Szymańska, J. & Dąbrowska-Galas, M. An assessment of Polish women’s level of knowledge about endometriosis: A pilot study. BMC Womens Health 21, 404. https://doi.org/10.1186/s12905-021-01556-2 (2021).
Patel, S., Hawkley, L. C., Cacioppo, J. T. & Masi, C. M. Dietary fiber and serum 16α-hydroxyestrone, an estrogen metabolite associated with lower systolic blood pressure. Nutrition 27, 778–781. https://doi.org/10.1016/j.nut.2010.08.017 (2011).
Blank, M. M., Wentzensen, N., Murphy, M. A., Hollenbeck, A. & Park, Y. Dietary fat intake and risk of ovarian cancer in the NIH-AARP Diet and Health Study. Br. J. Cancer 106, 596–602. https://doi.org/10.1038/bjc.2011.572 (2012).
Parazzini, F., Viganò, P., Candiani, M. & Fedele, L. Diet and endometriosis risk: A literature review. Reprod. Biomed. Online 26, 323–336. https://doi.org/10.1016/j.rbmo.2012.12.011 (2013).
Helbig, M., Vesper, A. S., Beyer, I. & Fehm, T. Does Nutrition affect endometriosis?. Geburtshilfe Frauenheilkd 81, 191–199. https://doi.org/10.1055/a-1207-0557 (2021).
Acknowledgements
The authors would like to acknowledge and thank the participants for their valuable contributions during the data collection phase of the NHANES project.
Funding
There was no funding designated for this research project.
Author information
Authors and Affiliations
Contributions
Z.Y.F. and G.Y.M. collaborated in gathering, assessing, creating, and composing data for academic writing and completed all graphs and tables. With contributions from L.G.C., S.C.J., and C.S.Y., the manuscript was created. Z.Y.F. was integral to the project’s conceptualization and management. G.X.G. and L.L.H. reviewed and made modifications to the manuscript. The final version has been approved by each author.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The National Center for Health Statistics’ Ethics Committee has granted approval for this study, in accordance with the Declaration of Helsinki. The retrospective analysis used in this study ensured that no potential harm was caused to the participants. The study was conducted without revealing any personal information or compromising the privacy of the participants. Before attending, all participants were asked to sign a form stating their informed consent. Electronic downloads enable quick and convenient access to all necessary materials, which can be found at https://wwwn.cdc.gov/nchs/nhanes/default.aspx
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zheng, YF., Guo, YM., Song, CJ. et al. A cross-sectional study on the relationship between dietary fiber and endometriosis risk based on NHANES 1999–2006. Sci Rep 14, 28502 (2024). https://doi.org/10.1038/s41598-024-79746-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79746-9
