
Abstract
Obesity and iron deficiency (ID) are widespread health issues, with subclinical inflammation in obesity potentially contributing to ID through unclear mechanisms. The aim of the present work was to elucidate how obesity-associated inflammation disturb iron metabolism and to investigate the effect of intravenous (IV) iron supplementation on absolute iron deficient pre-obese (BMI 25.0–29.9 kg/m2) and obese (BMI > 30 kg/m2) individuals compared to healthy weight (HW) group (BMI 18.5–24.9 kg/m2). Iron-related, hematological and inflammatory biomarkers along with erythropoietin (EPO) were studied based on body mass index (BMI) in a Spanish cohort of non-anemic participants (n = 721; 67% women; median age of 48 years [IQR: 39–57]) and in a subgroup of subjects (n = 110) with absolute ID (ferritin < 50 ng/mL) after completing an IV iron therapy. Obese group exhibited higher levels of ferritin, hemoglobin (Hb), soluble transferrin receptor (sTfR) and hepcidin compared to HW group. Elevated BMI was independently associated with increased sTfR levels. While no statistical differences were found in EPO among groups, obese showed increased levels that inversely correlated with Hb only in pre-obese and obese groups. IV iron therapy on obese participants had significant improvements on iron-related parameters and Hb levels. Notable obesity-associated disturbances in iron metabolism are described and indicate a mixed ID among both, women and men. These findings highlight the importance of tailored interventions to correctly address ID in obese population.
Similar content being viewed by others

Introduction
Obesity and iron deficiency (ID) are global health problems affecting billions of people worldwide1,2. Many studies have concluded that overweight and obese people are in a state of ongoing subclinical inflammation due to the hypertrophy and dysfunction of adipose tissue. This tissue is an active endocrine organ, rather than merely a fat depot, whose alteration can secondarily lead to serious complications such as obstructive sleep apnea, malignancy, ischemic heart disease, diabetes, and others3,4. At the same time, ID is one of the comorbidities related to obesity, but the underlying mechanisms for obesity-associated ID remain unclear5,6,7. Different mechanisms are proposed to explain this association, and although its etiology is probably multifactorial, the most widely accepted explanation is that the exacerbated secretion of adipokines and proinflammatory cytokines such as IL-6 induces the production of hepcidin, the main regulator of iron metabolism8. Hepcidin reduces iron export to plasma by decreasing intestinal absorption by acting as an inhibitor of the iron transporter ferroportin 1 in the duodenum and also diminishes iron release from erythrocyte-recycling macrophages9. However, a decrease in iron absorption, independent of hepcidin, has been described in a high-fat diet-induced obesity animal model10.
A relationship between obesity and ID likely exists in children and adolescents7,11. However, results appear more controversial in adults compared to adolescents, as reviews and meta-analysis in adults are limited by scarcity of available studies, significant heterogeneity, absence of consistent non-obese control groups, and frequently uncontrolled confounding variables (e.g. acute infection, menopausal status, oral contraceptive use, inclusion of both sexes without establishing differences in the same study, iron supplementation, obesity-related comorbidities)12. Often, research focused on pre- and post-menopausal women and adult men is underrepresented13. Thus, a study revealed lower serum iron concentrations in overweight women but no disparities in males14. Furthermore, these limitations are exacerbated by the lack of standardization in diagnosing ID. This issue is particularly critical as obesity is linked to chronic low-grade inflammation, which can elevate ferritin, an acute phase protein and the conventional biomarker for absolute ID15. Therefore, using serum ferritin as an indicator of ID in this population is debated16,17. In such cases, alternative iron-related biomarkers in obesity, such as elevated soluble transferrin receptor (sTfR), the extracellular cleaved portion of the cellular receptor, which is unaffected by inflammation, may prove beneficial for ID assessment but needs evaluation in large cohorts17,18.
Hence, despite indications of a potential association between ID and obesity, research in adults that compares ID prevalence using alternative iron-related biomarkers such as sTfR across body mass index (BMI) categories, including severe obesity, gender, and age, remains limited. Furthermore, due to the potential alteration of iron absorption and biomarkers of iron metabolism caused by inflammation related to obesity, the effectiveness of treating ID with oral iron supplementation in obese individuals may be limited. However, there is insufficient evidence focused on alternative intravenous (IV) iron treatments in obese patients with proven ID.
Objectives
The aim of this study was to elucidate how obesity-associated inflammation might disturb iron metabolism in pre-obese and obese individuals spanning a wide age range, both women and men. Furthermore, we sought to investigate the effect of IV iron supplementation on absolute ID in pre-obese and obese individuals compared to those with a healthy weight.
Results
General characteristics of the study population
Baseline characteristics and soluble proinflammatory biomarkers across BMI categories of the 721 participants who fulfilled the inclusion criteria (Fig. 1) are presented in Table 1. The prevalence of women was significantly higher in the healthy weight individuals compared to pre-obese and obese groups, while the age was lower in healthy weight group. As expected, the levels of the inflammatory biomarkers, soluble CRP, TNF-α, IL-6, and sedimentation velocity, increased markedly as the BMI increased within the groups (Table 1).

Flow chart of the participants selection. BMI, body mass index.
Iron-related and haematological parameters by body mass index and sex
Figure 2 shows iron-related and hematological parameters that exhibit differences according to BMI. Specifically, the pre-obese and obese groups exhibited higher levels on ferritin, Hb, hepcidin, anisocytosis index, and sTfR levels compared to healthy weight group. Regarding ferritin values as indicators of absolute ID, 55%, 39%, and 30% of healthy weight, pre-obese, and obese patients, respectively, had ferritin levels < 50 ng/ml. To evaluate the possible influence of sex, the participants were also categorized on women and men. Regarding those parameters, we observed marked differences based on sex, with increased levels of ferritin, Hb and hepcidin, and low levels of anisocytosis index in men compared to women (Fig. 2A–D). In the case of sTfR, we found no differences based on sex (Fig. 2E).

Inflammatory and iron-related parameters by body mass index category and sex. Bars show the median and interquartile range of serum ferritin (A), Hb (B), hepcidin (C), anisocytosis index (D) and sTfR (E) based on body mass index categories and sex. Women and men are indicated in purple and blue dots, respectively. BMI categories: healthy weight (18.5–24.9 kg/m2), pre-obese (25.0–29.9 kg/m2), obese (≥ 30–34.9 kg/m2). The yellow shading in A indicates the range of ferritin values < 50 ng/ml, threshold for absolute iron deficiency. Hb, hemoglobin; sTfR, soluble transferrin receptor. Differences between categories were determined using Mann–Whitney U-test. Only comparisons with p-value < 0.1 are indicated. Ө 0.1 > p-value ≥ 0.05; *0.01 ≤ p-value < 0.05; **0.001 ≤ p-value < 0.01; ***0.0001 ≤ p-value < 0.001; **** p-value < 0.0001.
Figure 3 displays other traditional biomarkers of ID and hematological parameters that showed no significant differences when comparing the three BMI-categories (sideremia, transferrin, TfSI, mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC) and mean corpuscular volume (MCV)), (Fig. 3A–F). However, marked differences were observed based on sex, with higher levels of sideremia, TfSI, MCH, and MCHC in men compared to women. Interestingly, for some of those parameters, BMI-dependent changes were observed only in the group of men, with a significant increase in sideremia and transferrin and a significant reduction in TfSI. In the case of MCV (Fig. 3F), a significant decreased in high BMI groups was observed only in men.

Iron-related and hematological parameters by body mass index category and sex. Bars show the median and interquartile range of sideremia (A), transferrin (B), TfSI (C), MCH (D), MCHC (E) and MCV (F) based on body mass index categories and sex. BMI categories: healthy weight (18.5–24.9 kg/m2), pre-obese (25.0–29.9 kg/m2), obesity (≥ 30–34.9 kg/m2). TfSI, transferrin saturation index; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume. Women and men are indicated in purple and blue dots, respectively. Differences between categories were determined using Mann–Whitney U-test. Only comparisons with p-value < 0.1 are indicated. Ө 0.1 > p-value ≥ 0.05; *0.01 ≤ p-value < 0.05; **0.001 ≤ p-value < 0.01; ***0.0001 ≤ p-value < 0.001; **** p-value < 0.0001.
An in-depth study was conducted considering three categories within the obesity group, and most of the changes in the aforementioned variables were more pronounced for obesity class III (data not shown). However, it is worth noting that no differences were found in ferritin and Hb levels (Supplementary Fig. 1A–B) comparing obesity class III and healthy weight group. In addition, sideremia and TfSI (Supplementary Fig. 1C–D) were significantly lower in this obesity class III group compared to other categories.
Factors associated with soluble transferrin receptor levels (sTfR)
Hence, this study also examined the factors associated with high sTfR levels (Supplementary Table 1). In the multivariate adjusted logistic regression model, BMI [regression coefficients (confidence interval [CI 95%]), 0.013 (0.006; 0.020), p < 0.001), Hb [0.047 (0.009; 0.084), p = 0.016], hepcidin [− 0.008 (− 0.014; − 0.002), p = 0.008], anisocytosis index [0.039 (0.014; 0.065), p = 0.002], sideremia [− 0.002 (− 0.003; − 0.001), p = 0.043] and transferrin [0.002 (0.002; 0.003), p < 0.001] remained significantly associated with high sTfR levels (Fig. 4).

Association of factors with increased sTfR levels. Statistics: data were calculated by univariate (left) and multivariate (right) logistic regression model after adjustment and by Stepwise methods. sTfR, soluble transferrin receptor; Hb, hemoglobin; BMI, body mass index; 95% CI, 95% of confidence interval; p-value, level of significance.
Erythropoietin correlations with iron-related and hematological biomarkers among BMI categories
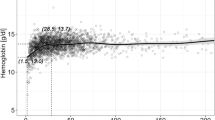
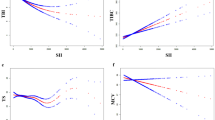
In order to evaluate the possible influence of BMI on erythropoiesis, EPO was measured in a subgroup of 76 participants. General characteristics of this group are presented in Supplementary Table 2. The obese group showed increased levels of EPO compared to healthy weight group despite no statistical significance, and women exhibited significantly higher levels compared to men (Fig. 5A). EPO levels showed strong correlations with iron-related biomarkers such as ferritin, Hb, sideremia, TfSI, MCH and MCV in the overall participants (Fig. 5B). However, interestingly, upon sub-analysis repeating the correlations stratified by BMI categories, the correlations with sideremia, TfSI, MCH and MCV remained significant only in healthy weight group, while the inverse correlation with Hb was only maintained in pre-obese and obese individuals (Fig. 5C). The correlation between EPO and with ferritin was significant in all three groups. We also examined the factors associated with high EPO levels, and in the multivariate logistic regression model after adjustment by sex, age, BMI, CRP, Hb and hepcidin, only BMI [regression coefficient (confidence interval [CI 95%]), 0.281 (0.002; 0.395), p = 0.048] and Hb [− 0.427 (− 2.957; − 0.624), p = 0.004] remained independently associated with EPO levels (Supplementary table 3).

Erythropoietin levels among BMI, sex and correlations with iron-related and hematological biomarkers. Bars show the median and interquartile range of erythropoietin based on body mass index categories and sex (A). Heat map showing the correlations between erythropoietin levels and iron-related and hematological variables in all participants and among body mass index categories (B). Detailed correlations between erythropoietin levels and hemoglobin among body mass index categories (C). EPO, erythropoietin; Hb, hemoglobin; sTfR, soluble transferrin receptor; TfSI, transferrin saturation index; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume. Differences between body mass index categories and women and men were determined using Mann–Whitney U-test. The Spearman rho correlation coefficient test was used. Only comparisons with p-value < 0.1 are indicated. Ө 0.1 > p-value ≥ 0.05; *0.01 ≤ p-value < 0.05; **0.001 ≤ p-value < 0.01; ***0.0001 ≤ p-value < 0.001; **** p-value < 0.0001.
Changes in hamatological and iron related parameters after IV iron therapy across BMI categories
Of all screened participants, 110 with absolute ID (ferritin < 50 ng/ml) received a complete treatment of IV iron infusion and had registered baseline and final hematological and iron-related data. Baseline characteristics of these participants by BMI category are presented in Supplementary Table 1, and the majority were women. All iron-related variables drastically changed independently of BMI with the exception of Hb, that increased in the pre-obese and obese, but not in healthy weight group (Fig. 6). In more detail, despite no differences in basal ferritin and Hb levels, after IV treatment, the obese group exhibited lower ferritin concentration and fold change, and higher Hb concentration and fold change compared to the healthy-weight group (Fig. 6A–B). Similarly, in the case of sTfR, the levels in the pre-obese and obese groups remained higher than those in the healthy-weight group even after treatment, while no differences were observed in the sTfR fold change (Fig. 6C). For sideremia, transferrin, and TfSI, the marked basal differences in the levels among BMI categories remained after treatment (Fig. 6D–F).

Changes in iron related levels before and after intravenous iron sucrose infusion by body mass index category. Bars show the median and interquartile range of serum ferritin (A), Hb (B), sTfR (C), transferrin (E), TfSI (F) and sideremia (G) before (baseline time-point, B) and after (final time-point, F) intravenous iron sucrose infusion and the respective fold change per BMI category. Body mass index categories: healthy weight (18.5–24.9 kg/m2), pre-obese (25.0–29.9 kg/m2), obese (≥ 30–34.9 kg/m2). HW, healthy weight; B, baseline time-point; F, final time-point; Hb, hemoglobin; sTfR, soluble transferrin receptor and TfSI, transferrin saturation index. Differences between paired time-points were determined using Wilcoxon signed rant test and differences between BMI categories were determined using Mann–Whitney U-test. Only comparisons with p-value < 0.1 are indicated. Ө 0.1 > p-value ≥ 0.05; *0.01 ≤ p-value < 0.05; **0.001 ≤ p-value < 0.01; ***0.0001 ≤ p-value < 0.001; **** p-value < 0.0001.
Regarding the set of hematological variables and hepcidin (Supplementary Fig. 1), in all categories there was a significant increase after IV treatment in the levels of HCM, MCV, and hepcidin, although the final levels after IV treatment between categories were not different. On the contrary, the observed increase in the anisocytosis index at the final time-point showed significantly higher levels for the pre-obese and obese groups compared to the healthy-weight group.
Discussion
In the present study, we conducted an analysis using data from a large population-based cross-sectional representative dataset from a Spanish cohort, comparing iron status biomarkers among non-anemic women and men aged 16–92 years. Overall, Hb and sTfR levels were higher in the obese group compared to healthy weight individuals of both genders, and high BMI was independently associated with elevated levels of the iron deficiency-related biomarker sTfR. In addition, we demonstrated marked differences in iron metabolism between obese women and men, with a predominance of mixed ID (absolute coupled with functional ID) in both sexes. Furthermore, we showed that obese patients undergoing IV iron therapy restored their iron metabolism, with a notable increase in Hb levels compared to healthy weight participants.
Increased adipocyte mass is the traditional hallmark of obesity. However, functional alterations in obese adipose tissue are equally crucial. This tissue acts as an active endocrine organ, exhibiting exacerbated production of CRP and pro-inflammatory cytokines like IL-6 and TNF-α, sustaining a state of low-grade systemic inflammation19,20, along with elevated hepcidin levels which account for reduced dietary iron absorption through diminished enterocyte iron uptake12,21. This aligns with the soluble proinflammatory profile observed in our pre-obese and obese patients compared to the healthy weight group. Our finding of high serum ferritin concentration (also an acute phase reactant) in participants with obesity is consistent with prior studies indicating that this iron-related biomarker, reflecting stored iron, significantly rises as BMI increases12,13. Our results also support those prior reports where lower sideremia and TfSI characterize obese subjects. While serum ferritin is conventionally used as the best indicator for detecting absolute ID, in conditions involving inflammatory processes such as obesity, sTfR stands as the most valuable indicator for assessing ID17,22, holding an inverse relationship with the magnitude of iron stores obtained through bone marrow aspiration measurement18,23, we identified dysregulation in both women and men and observed pronounced sex-dependent variations in many markers. For the first time, we identified in an adjusted multivariate logistic regression that high sTfR levels remained independently associated with BMI, reinforcing the potential of sTfR as an ID biomarker in this population.
In addition to the inhibitory role of hepcidin on iron absorption, elevated hepcidin and inflammatory cytokines contribute to iron sequestration in macrophages, reducing iron recycling, sideremia, and iron availability for erythropoiesis despite normal body iron stores. This situation in which iron is hardly mobilized from stores to the circulation and erythropoietic tissue in response to chronic inflammation and elevated hepcidin levels is called “functional” ID24,25. In our study, the high hepcidin levels observed characterize the pre-obese and obese subjects, mainly in men. Consequently, we could define a profile of mixed ID in those patients due to the coexistence of both absolute and functional ID. Interestingly, Rodríguez-Mortera et al. demonstrated that hepcidin elevation in adolescents with obesity is linked more to inflammation and metabolic disturbances, including dyslipidemia and insulin resistance, than to iron metabolism itself26. This is in line with our findings, where high hepcidin levels in obese patients could be indicative of a similar inflammatory-driven dysregulation in iron metabolism rather than an isolated absolute ID. Some authors highlighted the influence of estrogen hormones in inhibiting hepcidin, a possible mechanism to compensate iron loss during menstruation that could explain the markedly low hepcidin levels observed in women compared to men regardless of BMI27.
Iron is indispensable to support crucial biological processes, including Hb synthesis during erythropoiesis, facilitating efficient oxygen transportation28,29. Therefore, coordinated regulation between the physiology of hypoxic response and the control of iron availability is necessary. In parallel with hepcidin regulation, another potential mechanism in obesity (Fig. 7) involves tissue hypoxia caused by the accumulation of adipose tissue, requiring elevated levels of Hb for effective oxygen distribution, and restrictive ventilatory insufficiency as a result of compromised chest mobility during breathing. This, coupled with potential episodes of sleep apnea, further exacerbates tissue hypoxia, and the high demand for oxygen would explain the elevated Hb levels observed in pre-obese and obese participants. In addition, hypoxia stimulates the production of EPO, primarily synthesized in the kidney. EPO is released by peritubular capillary cells in response to hypoxia, leading to increased erythropoiesis and the production of more Hb, which transports oxygen to tissues. Its role in adipose tissue during obesity-induced inflammation has been extensively studied using in vitro and in vivo model systems30. EPO has been studied for the first time in this work within the context of obesity and iron metabolism. Elevated EPO demand in obese individuals, as a consequence of tissue hypoxia, could drive increased erythropoiesis, resulting in the elevation of Hb levels within this group. As systemic inflammation, including proinflammatory cytokines such as TNF-α and interleukin 1β (IL-1β), inhibits the production of EPO31,32, this could explain the slight increase in observed EPO levels in the obese group and the consequent lack of statistical significance. However, the multivariate adjusted analysis showed a strong association between EPO and BMI. Interestingly, in healthy weight individuals, EPO correlated with iron metabolism parameters (sTfR, transferrin, TfSI), as erythropoiesis is typically triggered by ID. However, in pre-obese and obese individuals, EPO appears to deviate from a mere association with ID. This deviation may be attributed to inflammation disrupting iron metabolism, and it no longer serves as a “switch” to activate erythropoiesis. Instead, in these groups, the need for tissue oxygen/Hb is evident and emerges as a more direct determinant for erythropoiesis, with probably insufficient Hb levels triggering EPO production. This shift is absent in healthy weight individuals, where EPO can directly detect ID, and there is no extra demand for tissue oxygen. This hypothesis gains support from the stronger inverse correlation observed between EPO and ferritin in healthy weight individuals compared to obese ones, likely due to inflammation-induced ferritin elevation in obesity. Consequently, it is noteworthy that the inverse correlation between EPO and hepcidin is also stronger in the healthy weight group than in pre-obese and obese ones. Moreover, this correlation weakens progressively in pre-obese individuals and inverts in obese individuals. Collectively, these findings suggest a primary level regulation of erythropoiesis in healthy weight individuals, where ID acts as a signal to activate erythropoiesis, preventing potential tissue oxygen deficiency. Conversely, in obesity, erythropoiesis appears to be directly linked to Hb levels, representing a secondary tier of regulation possibly influenced by impaired iron metabolism or heightened tissue oxygen demand.

Current understanding of links between obesity and iron deficiency. Obesity is marked by persistent systemic inflammation and increased production of pro-inflammatory cytokines and adipokines in adipose tissue. This directly impacts iron absorption from the duodenum enterocytes by inhibiting the iron transporter ferroportin 1, regulated by hepcidin. Moreover, pro-inflammatory cytokines like IL-6 act as powerful inducers of hepcidin in the liver, which may further impair iron absorption. Both, cytokines and hepcidin contribute to iron sequestration in macrophages, reducing iron recycling, sideremia, and iron availability for erythropoiesis. In obese conditions, compromised chest mobility during breathing causes restrictive ventilatory insufficiency which, along with potential episodes of sleep apnea, contribute to tissue hypoxia, another potential mechanism contributing to ID in obesity. These hypoxic conditions activate the hypoxia-inducible factor 1 pathway that induces the production of the hormone erythropoietin, primarily in the kidney, stimulating erythropoiesis in the bone marrow, leading to elevated circulating hemoglobin levels. This process demands a substantial amount of iron for hemoglobin synthesis, resulting in reduced availability. These combined factors result in an absolute and functional ID (mixed), reflected in low sideremia, TfSI and high sTfR as primary soluble biomarkers in serum. CRP, C-reactive protein; hypoxia-inducible factor 1, HIF-1; EPO, erythropoietin; TfSI, transferrin saturation index; sTfR, soluble transferrin receptor.
Given that ID can progress to ID anemia (IDA), one may expect to see an association between obesity and IDA. In our study, we attempted to mitigate the potential confounding role of anemia by including only non-anemic subjects, and we observed high Hb levels in the overall obese cohort, both in women and men, but with notably higher levels in men. However, it is worth noting that the segregated sub-analysis of the extreme type III obese group, despite the relatively low number of patients, showed no differences in Hb concentration compared to the healthy weight group, suggesting that Hb production may reach a maximum threshold due to lack of available iron. Additionally, the high Hb levels observed in obese individuals reinforce studies, including ours, which emphasized the unacceptably low sensitivity of Hb-based screening for detecting ID, thereby underestimating the prevalence of ID not only in obesity but also in the general population33,34.
The conventional method for treating ID is through oral iron supplement. However, due to the diminished iron absorption associated with elevated serum hepcidin in obese participants35,36, supplementation with IV iron may be a viable alternative to oral administration. Despite limited reports in the context of obesity, improved iron status after IV therapy was documented in patients with type 2 diabetes37, and our group demonstrated short-term efficacy independent of BMI in a different cohort of global population, possible because the majority of individuals had a BMI < 30 kg/m2 2,38. Nevertheless, as far as we know, this is the first study restricted to non-anemic patients with a high prevalence and grade of obesity who had absolute ID (ferritin < 50 ng/mL), with or without a functional component. In addition to confirming the effectiveness of short-term IV treatment with a comprehensive set of biomarkers of iron-related metabolism, we observed a significant increase in Hb in obese individuals compared to the other groups. This finding reinforces our hypothesis of an early iron requirement for tissue oxygen distribution, suggesting that administered iron may primarily serve to supply oxygen to tissues via increased Hb production and may lead to decreased iron availability over time. Despite IV administration bypassing the inhibitory effect of hepcidin on absorption, high levels of hepcidin are still acting at other levels, such as inhibiting iron recycling at the macrophage level, and absolute ID may manifest in later stages due to decreased iron absorption signaled by high hepcidin levels. However, we were unable to assess the long-term evolution or recurrence. To date, weight loss remains the preferred approach, as it has been reported to reduce altered levels of pro-inflammatory cytokines, potentially leading to reduced hepcidin release, improved iron homeostasis, and a positive effect on low-grade chronic inflammation and related chronic diseases commonly seen in individuals with overweight and obesity8,39,40.
It is important to highlight that among the limitations of previous studies, gender emerged as a primary confounding factor, with most studies predominantly focusing on premenopausal women. In contrast, our study is notable for its comprehensive design, and analysis, not only encompassing women but also men, and spanning a broad age range in both cohorts. Other limitations are its single-center design, which may impact its generalizability and the lack of information regarding other metabolic markers, such as insulin levels and altered lipid profiles, which are also related to obesity and iron metabolism.
Conclusions
Our findings reveal notable obesity-associated disturbances of iron metabolism, with higher levels of Hb, sTfR, and hepcidin in pre-obese and obese groups compared to healthy weight individuals of both genders. Together with the inflammatory status in this population, this indicates a predominant mixed ID profile characterized by both absolute and functional ID. Moreover, the inter-regulation between iron metabolism and erythropoiesis seems to be dysregulated in obese subjects. IV iron therapy in obese participants had significant short-term improvements in iron metabolism and Hb levels. These findings contribute to a better understanding of iron metabolism in obesity and underscore the importance of tailored interventions to correctly address ID in this population.
Material and methods
Participants and study design
All the methods were carried out in accordance with relevant standards and regulations, as outlined in the Declaration of Helsinki and approved by the local Ethical Committee from Virgen Macarena and Virgen del Rocio University Hospitals (code: 0465-N-22; acta CEI_03/2022). The study employed a two-part design: (1) a retrospective observational analysis of individuals who consecutively visited the Hospital Viamed Santa Ángela de la Cruz in Seville, Spain, as outpatients between April 1, 2020, and January 4, 2024, and whose doctor requested an iron metabolism study in their blood tests as part of routine clinical management (ViaIron cohort)38, and (2) a retrospective longitudinal subanalysis, where participants who received IV iron supplementation as part of their clinical care were followed during the intervention and post-treatment period. The exclusion criteria for this study were anemia (defined by the World Health Organization as hemoglobin [Hb] concentration lower than or equal to 12 and 13 g/dL for women and men, respectively), active neoplasia, age lower than 16 years old, BMI lower than 18.5 kg/m2, pregnancy, breastfeeding, hospitalization, and recent iron supplementation (Fig. 1).
Patients were categorized into three groups based on BMI: normal or healthy weight (< 24.9 kg/m2), overweight or pre-obese (25–29.9 kg/m2), or obese, which includes three subcategories: obesity class I (30–34.9 kg/m2), obesity class II (35–39.9 kg/m2), and obesity class III, also referred to as severe, extreme, or massive obesity (≥ 40 kg/m2)41.
Intervention with IV iron therapy
As part of routine clinical management, a subgroup of participants received and completed an IV iron supplementation therapy (n = 110). This subgroup consisted of non-anemic participants with serum ferritin levels < 50 ng/ml, indicative of absolute ID33,42, who received five IV standard doses of 200 ml of generic iron (III)-hydroxy sucrose, Feriv®, dissolved in 500 cc of saline solution and administered once a week for five consecutive weeks. The treatment’s final response was evaluated between 7 and 10 days after treatment completion. A detailed description of the study design and treatment efficacy in real-world settings can be found in Tarancon-Diez et al.38. Throughout the treatment protocol, no additional iron supplements, blood transfusions, or erythropoiesis-stimulating agents were allowed. To analyze changes in iron metabolism biomarkers following IV iron supplementation, participants who completed the protocol were also categorized according to their BMI as previously defined in the current methodology section.
Laboratory methods
Iron-related and hematological parameters, as well as inflammatory biomarkers, were measured after overnight fasting using standardized techniques at the Laboratory Service of Hospital Viamed Santa Ángela de la Cruz as described in previous works33,43. Briefly, total serum iron (sideremia), transferrin, and sTfR were measured by photometry, and ferritin by means of the particle-enhanced immunoturbidimetric assay in a Hitachi Cobas C702 modular analyzer (Roche Diagnostics, Rotkreuz, Switzerland). The transferrin saturation index (TfSI) was estimated as total plasma iron (μg/dL) × 100/transferrin (mg/dL) × 1.27. Plasma hepcidin was determined by ELISA (Hepcidin25 HS ELISA, DRG), C-reactive protein (CRP) was determined in serum by photometry using Cobas 701 (Roche Diagnostics, Mannheim, Germany), and interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) were measured using an Immulite 2000 Siemens and Immulite One Siemens, respectively (Siemens Healthcare Diagnostics, Siemens AG, Munich, Germany), according to the manufacturer’s instructions. Erythropoietin (EPO) was measured using an automatic Xpi Immulite 2000 analyzer (Siemens Healthcare Diagnostics, Siemens AG) according to the manufacturer’s instructions.
Statistical analysis
Continuous variables were expressed as medians and interquartile ranges [IQR], and categorical variables were expressed as the number of subjects and percentage (%). Non-parametric tests were performed after the Kolmogorov–Smirnov test, which confirmed that the variables did not follow a normal distribution. Group differences between categorical and continuous values were determined using the Chi-square test and the Mann–Whitney U-test, respectively. Correlations between variables were assessed using the Spearman rank test. For the analysis of changes in hematological and iron-related parameters after IV iron therapy, the fold-change of the variation during the intervention (final minus baseline time point) of each biomarker was calculated, and differences between both time points were determined using the Wilcoxon signed-rank test. A multivariate logistic regression model using the stepwise method was used to determine the factors associated with increased levels of sTfR and EPO. p-values < 0.05 were considered statistically significant. The Statistical Package for the Social Sciences software (SPSS 20.0, Chicago, IL, USA) and GraphPad Prism 9.0 (GraphPad Software, Inc., San Diego, CA, USA) were used for the statistical analysis and generation of graphs.
Data availability
Main datasets supporting the conclusions of this article are included within the article and its additional files. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ID:
-
Iron deficiency
- sTfR:
-
Soluble transferrin receptor
- BMI:
-
Body mass index
- IV:
-
Intravenous
- Hb:
-
Hemoglobin
- TfSI:
-
Transferrin saturation index
- CRP:
-
C-reactive protein
- IL-6:
-
Interleukin-6
- TNF-α:
-
Tumor necrosis factor-alpha
- EPO:
-
Erythropoietin
- IQR:
-
Interquartile ranges
- MCH:
-
Mean corpuscular hemoglobin
- MCHC:
-
Mean corpuscular hemoglobin concentration
- MCV:
-
Mean corpuscular volume
- IL-1β:
-
Interleukin 1β
- IDA:
-
Iron deficiency anemia
References
Cappellini, M. D., Musallam, K. M. & Taher, A. T. Iron deficiency anaemia revisited. J. Intern. Med. 287, 153–170 (2020).
Chooi, Y. C., Ding, C. & Magkos, F. The epidemiology of obesity. Metabolism 92, 6–10 (2019).
Kim, D.-S. & Scherer, P. E. Obesity, diabetes, and increased cancer progression. Diabetes Metab. J. 45, 799–812 (2021).
Myint, P. K., Kwok, C. S., Luben, R. N., Wareham, N. J. & Khaw, K.-T. Body fat percentage, body mass index and waist-to-hip ratio as predictors of mortality and cardiovascular disease. Heart 100, 1613–1619 (2014).
Hutchinson, C. A review of iron studies in overweight and obese children and adolescents: A double burden in the young?. Eur. J. Nutr. 55, 2179–2197 (2016).
Menzie, C. M. et al. Obesity-related hypoferremia is not explained by differences in reported intake of heme and nonheme iron or intake of dietary factors that can affect iron absorption. J. Am. Dietetic Assoc. 108, 145–148 (2008).
Wenzel, B. J., Stults, H. B. & Mayer, J. Hypoferraemia in obese adolescents. The Lancet 280, 327–328 (1962).
Coimbra, S., Catarino, C. & Santos-Silva, A. The role of adipocytes in the modulation of iron metabolism in obesity. Obesity Rev. 14, 771–779 (2013).
Nemeth, E. et al. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Invest. 113, 1271–1276 (2004).
Sonnweber, T. et al. High-fat diet causes iron deficiency via hepcidin-independent reduction of duodenal iron absorption. J. Nutr. Biochem. 23, 1600–1608 (2012).
Nead, K. G., Halterman, J. S., Kaczorowski, J. M., Auinger, P. & Weitzman, M. Overweight children and adolescents: A risk group for iron deficiency. Pediatrics 114, 104–108 (2004).
Cheng, H. L. et al. The relationship between obesity and hypoferraemia in adults: A systematic review: Obesity and hypoferraemia in adults. Obesity Rev. 13, 150–161 (2012).
Aguree, S., Owora, A., Hawkins, M. & Reddy, M. B. Iron deficiency and iron deficiency anemia in women with and without obesity: NHANES 2001–2006. Nutrients 15, 2272 (2023).
Micozzi, M. S., Albanes, D. & Stevens, R. G. Relation of body size and composition to clinical biochemical and hematologic indices in US men and women. Am. J. Clin. Nutr. 50, 1276–1281 (1989).
Dignass, A., Farrag, K. & Stein, J. Limitations of serum ferritin in diagnosing iron deficiency in inflammatory conditions. Int. J. Chron. Dis. 2018, 1–11 (2018).
Huang, Y.-F. et al. Relationship between being overweight and iron deficiency in adolescents. Pediatr. Neonatol. 56, 386–392 (2015).
Turgeon O’Brien, H., Blanchet, R., Gagné, D., Lauzière, J. & Vézina, C. Using soluble transferrin receptor and taking inflammation into account when defining serum ferritin cutoffs improved the diagnosis of iron deficiency in a group of Canadian preschool Inuit children from Nunavik. Anemia. 2016(1), 6430214 (2016).
Beguin, Y. Soluble transferrin receptor for the evaluation of erythropoiesis and iron status. Clinica Chim. Acta 329, 9–22 (2003).
Anty, R. et al. The inflammatory C-reactive protein is increased in both liver and adipose tissue in severely obese patients independently from metabolic syndrome, Type 2 diabetes, and NASH. Am. J. Gastroenterol. 101, 1824–1833 (2006).
Weisberg, S. P. et al. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Invest. 112, 1796–1808 (2003).
Bekri, S. et al. Increased adipose tissue expression of Hepcidin in severe obesity is independent from diabetes and NASH. Gastroenterology 131, 788–796 (2006).
Sierpinski, R. et al. High soluble transferrin receptor in patients with heart failure: A measure of iron deficiency and a strong predictor of mortality. Eur. J. Heart Fail 23, 919–932 (2021).
Khan, A., Khan, W. M., Ayub, M., Humayun, M. & Haroon, M. Ferritin is a marker of inflammation rather than iron deficiency in overweight and obese people. J. Obesity 2016, 1–7 (2016).
Camaschella, C. Iron deficiency. Blood 133, 30–39 (2019).
Iriarte-Gahete, M., Tarancon-Diez, L., Garrido-Rodríguez, V., Leal, M. & Pacheco, Y. M. Absolute and functional iron deficiency: Biomarkers, impact on immune system, and therapy. Blood Rev. 68, 101227 (2024).
Rodríguez-Mortera, R., Caccavello, R., Hermo, R., Garay-Sevilla, M. E. & Gugliucci, A. Higher Hepcidin levels in adolescents with obesity are associated with metabolic syndrome Dyslipidemia and visceral fat. Antioxidants 10, 751 (2021).
Yang, Q., Jian, J., Katz, S., Abramson, S. B. & Huang, X. 17β-Estradiol inhibits iron hormone Hepcidin through an Estrogen responsive element half-site. Endocrinology 153, 3170–3178 (2012).
AlRajeh, L., Zaher, A., Alghamdi, A., Alsheikh, R. & AlSultan, O. Effects of iron deficiency and its indicators on lymphocyte subsets: A study at king Fahd hospital of the university. Saudi Arabia. JBM 13, 61–67 (2022).
Weyh, C., Krüger, K., Peeling, P. & Castell, L. The role of minerals in the optimal functioning of the immune system. Nutrients 14, 644 (2022).
Alnaeeli, M. & Noguchi, C. T. Erythropoietin and obesity-induced white adipose tissue inflammation: Redefining the boundaries of the immunometabolism territory. Adipocyte 4, 153–157 (2015).
Rivkin, M. et al. Inflammation-induced expression and secretion of MicroRNA 122 leads to reduced blood levels of kidney-derived erythropoietin and Anemia. Gastroenterology 151, 999-1010.e3 (2016).
Krajewski, J., Batmunkh, C., Jelkmann, W. & Hellwig-Bürgel, T. Interleukin-1β inhibits the hypoxic inducibility of the erythropoietin enhancer by suppressing hepatocyte nuclear factor-4α. Cell. Mol. Life Sci. 64, 989–998 (2007).
Tarancon-Diez, L. et al. Threshold ferritin concentrations reflecting early iron deficiency based on Hepcidin and soluble transferrin receptor serum levels in patients with absolute iron deficiency. Nutrients 14, 4739 (2022).
Sekhar, D. L., Murray-Kolb, L. E., Kunselman, A. R. & Paul, I. M. Identifying factors predicting iron deficiency in United States adolescent females using the ferritin and the body iron models. Clin. Nutr. ESPEN 10, e118–e123 (2015).
Baumgartner, J. et al. Overweight impairs efficacy of iron supplementation in iron-deficient South African children: A randomized controlled intervention. Int J Obes 37, 24–30 (2013).
Zimmermann, M. B. et al. Adiposity in women and children from transition countries predicts decreased iron absorption, iron deficiency and a reduced response to iron fortification. Int J Obes 32, 1098–1104 (2008).
Schindler, C. et al. Intravenous ferric Carboxymaltose in patients with type 2 diabetes mellitus and iron deficiency: CLEVER trial study design and protocol. Diabetes Ther 9, 37–47 (2018).
Tarancon-Diez, L. et al. Real-world experience of intravenous iron sucrose supplementation and dynamics of soluble transferrin receptor and Hepcidin in a Spanish cohort of absolute iron deficient patients. Biomed. Pharmacother. 167, 115510 (2023).
Alshwaiyat, N., Ahmad, A., Wan Hassan, W. M. R. & Al-jamal, H. Association between obesity and iron deficiency (Review). Exp. Ther. Med. 22, 1268 (2021).
Cepeda-Lopez, A. C. et al. The effects of fat loss after bariatric surgery on inflammation, serum hepcidin, and iron absorption: A prospective 6-mo iron stable isotope study. Am. J. Clin. Nutr. 104, 1030–1038 (2016).
Weir, C. B. & Jan, A. BMI Classification Percentile And Cut Off Points (StatPearls Publishing, Treasure Island, 2023).
Galetti, V. et al. Threshold ferritin and Hepcidin concentrations indicating early iron deficiency in young women based on upregulation of iron absorption. EClinicalMedicine 39, 101052 (2021).
Garrido-Rodríguez, V. et al. Dysregulation of iron metabolism modulators in virologically suppressed HIV-infected patients. Front. Immunol. 13, 977316 (2022).
Acknowledgements
The authors would like to particularly acknowledge all patients as well as their families for their participation in this study.
Funding
This work was supported by the “Centro de Investigación Biomédica en Red de Enfermedades Infecciosas” (CIBERINFEC) [CB21/13/00077], “Centro de Investigación Biomédica en Red de Bioingeniería, Biomateriales y Nanomedicina” (CIBER-BBN) [CB22/01/00041], Fondo de Investigación Sanitaria [FIS; PI21/00357], Instituto de Salud Carlos III (ISCIII), and Ministry of Science, Innovation and Universities [CNS2023/144725], Madrid, Spain, which are co-funded by Fondos Europeos para el Desarrollo Regional (FEDER) “A way to make Europe”. LT-D is supported by the Instituto de Salud Carlos III (ISCIII) through the Miguel Servet Program (CP23/00009), GeSIDA through the “IV Premio para Jóvenes Investigadores 2021″, ESPID Small Grant Award 2023 and “Proyectos de I + D + i Programa Intramural IiSGM” (2023-II-PI-NOV-01). MI-G is supported by the Instituto de Salud Carlos III (ISCIII) through the Río Hortega Program (CM22/00198). YMP is supported by Nicolás Monardes Program from Junta de Andalucía (RC-0006-2021).
Author information
Authors and Affiliations
Contributions
Laura Tarancon-Diez: Conceptualization; Investigation; Formal analysis; Writing—Original Draft; Funding acquisition; Visualization. Marianela Iriarte-Gahete: Investigation, Data Curation, Writing—Review & Editing. Pilar Sanchez-Mingo: Resources, Writing—Review & Editing. Mª Ángeles Muñoz-Fernández: Investigation, Writing—Review & Editing. Maria Luisa Navarro-Gomez: Investigation, Writing—Review & Editing. Yolanda M Pacheco: Investigation, Writing—Review & Editing. Manuel Leal: Conceptualization, Resources, Data Curation, Supervision, Project administration, Writing—Review & Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was approved by the ethic committee of Hospital Universitario La Paz in Madrid (PI-4636). Written informed consent was obtained from all HIV participants before inclusion in CoRISpe-FARO and from all HD before inclusion in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tarancon-Diez, L., Iriarte-Gahete, M., Sanchez-Mingo, P. et al. Impact of obesity on iron metabolism and the effect of intravenous iron supplementation in obese patients with absolute iron deficiency. Sci Rep 15, 1343 (2025). https://doi.org/10.1038/s41598-024-84498-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84498-7
