
Abstract
As glyphosate’s application becomes increasingly widespread across the globe, its potential adverse effects on humans have garnered growing concerns. Little evidence has revealed the associations between glyphosate and glucose homeostasis. A total of 2094 individuals were recruited from the NHANES 2013–2018. Urinary glyphosate, alkaline phosphatase (ALP), fasting plasma glucose (FPG), fasting insulin, and glycated hemoglobin A1c (HbA1c) were measured. Homeostatic model assessment of beta-cell function (HOMA2-β), insulin resistance (HOMA2-IR), and insulin sensitivity (HOMA2-IS) were assessed. Generalized linear models and mediation analyses were fitted to estimate the potential associations between glyphosate, glucose homeostasis, and ALP. Urinary glyphosate demonstrated a statistically significant positive association with FPG and HbA1c in a linear positive dose–response manner, while showing a linear negative association with HOMA2-β. Each doubling increase in urinary glyphosate was associated with a 1.13%, 1.50%, and − 2.80% alteration in FPG, HbA1c, and HOMA2-β, respectively. Obesity modified the association between urinary glyphosate and glucose dyshomeostasis with stronger associations in obese individuals. In addition, elevated ALP significantly mediated the associations of urinary glyphosate with FPG and HbA1c, with mediated proportions of 9.91% and 20.23%, respectively. Environmental glyphosate exposure was associated with glucose dyshomeostasis, which was more pronounced in obese individuals and was partly mediated by ALP.
Similar content being viewed by others

Introduction
Glyphosate, a highly effective broad-spectrum herbicide, is one of the most commonly used herbicides worldwide. Since its registration in 1974, glyphosate has been extensively utilized in the US, with more than 1.6 billion kilograms of the active ingredient deployed across the country1. On a global scale, it has witnessed an application of 6.1 billion kilograms of glyphosate in the last decade, remarkably constituting 71.6% of the cumulative worldwide usage spanning from 1974 to 20141. The escalating consumption of glyphosate in recent years has sparked heightened apprehension regarding its potential impact on the ecosystem. Notable evidence uncovered that glyphosate was ubiquitous in soils, ditches, precipitation, and rivers, with the maximum level observed reaching up to 476 µg/kg across 38 states in the US2. Also, glyphosate was detectable in solid matrices, with maximum concentrations of 8100 µg/kg in soil and 3300 µg/kg in sediment from Argentina, respectively3. In addition to glyphosate in the environment, an investigation detected that 42.3% of foods from the Canadian retail markets contained detectable glyphosate residues4. Glyphosate poses a threat to the environment and food, and consequently to human health5.
Human exposure to glyphosate occurs through ingestion of food and water, dermal contact with products containing residues of this chemical, and inhaled relevant aerosol particles6,7. The international SPRINT study demonstrated that 70% of the participants, including farmers, their neighbors, and urban residents, had glyphosate residues in their feces8. Recently, a nationally representative study also suggested that over 80% of the US population aged ≥ 6 years experienced recent exposure to glyphosate7. Glyphosate is largely not metabolized in the human body and the parent compound can be eliminated in urine9,10. Urinary glyphosate has been proven to highly correlate with the external exposure dose, which could reflect the actual exposure11. Thus, quantification of urinary glyphosate is a noninvasive and widely used method for assessing the level of glyphosate exposure7,12.
Although glyphosate has long been recognized as a relatively harmless herbicide, the risks associated with glyphosate herbicides have gradually surfaced in recent years13. More studies have documented the potential adverse effects associated with glyphosate exposure, including the increased risk of osteoarthritis14, non-alcoholic fatty liver disease15, neurological unhealthy outcomes16, non-Hodgkin lymphoma17, and even mortality18. Meanwhile, glyphosate may pose cardiovascular metabolic toxicity, increasing cardiovascular disease and diabetes risk19,20. Noteworthily, high fasting plasma glucose (FPG), recognized as an independent predictor of cardiovascular disease and diabetes onset, has emerged as a pervasive health threat with a contribution to 6.50 million global deaths in 201921. Environmental pollution has been identified as a key risk factor for elevated FPG and insulin resistance22,23. However, epidemiological research has been sparse in assessing the relationships between glyphosate exposure and glucose homeostasis indices such as FPG and insulin resistance.
Alkaline phosphatase (ALP) is extensively adopted as a clinical biomarker because of the close correlations between abnormal ALP levels and diverse disease conditions24. Apart from being a routine clinical indicator for hepatobiliary and bone disorders, ALP is also related to cardiovascular risk factors, such as obesity, blood pressure, blood lipids, and blood glucose levels25,26. Moreover, a cross-sectional study reported that exposure to glyphosate resulted in elevation of ALP27. Nevertheless, whether ALP plays an important role in the underlying associations between glyphosate exposure and glucose homeostasis remains unknown. Accordingly, this study encompassed 2094 individuals from the National Health and Nutrition Examination Survey (NHANES) 2013–2018 to explore the potential associations between urinary glyphosate, glucose homeostasis, and ALP.
Results
Basic characteristics of the study participants
The basic characteristics of the study participants across the quartiles of urinary glyphosate are summarized in Table 1. A total of 1009 (48.19%) were males. The mean [standard deviation (SD)] age and body mass index (BMI) of the total participants were 48.61 (18.28) years and 29.50 (7.28) kg/m2, respectively. The median [interquartile range (IQR)] level of urinary glyphosate was 0.304 (0.175–0.513) μg/g creatinine (Cr). Participants with a higher quartile of urinary glyphosate were more likely to be female, older, non-Hispanic White, and current drinkers (P < 0.05). Statistically significant differences in ALP, FPG, glycated hemoglobin A1c (HbA1c), and homeostatic model assessment of beta-cell function (HOMA2-β) were noted across the quartiles of urinary glyphosate (P < 0.05), whereas no statistically significant differences were observed for fasting insulin (FINS), homeostasis model assessment of insulin resistance (HOMA2-IR), or homeostasis model assessment of insulin sensitivity (HOMA2-IS) (P > 0.05). The distribution of glucose homeostasis indices after correction for confounders results showed that as the concentration of urinary glyphosate increased, FPG and HbA1c gradually increased and HOMA2-β gradually decreased (Table S1, P < 0.05).
Associations between urinary glyphosate and glucose homeostasis indices
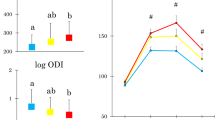
Percent changes in glucose homeostasis indices associated with urinary glyphosate are presented in Table S2 and Fig. 1. After full adjustments, statistically significant dose–response relationships between urinary glyphosate, FPG, HbA1c, and HOMA2-β were observed (all P for trend < 0.05). Compared with individuals in the lowest quartile of urinary glyphosate, those in the second, third, and highest quartiles separately had a 0.82% (95% confidence interval [CI] − 1.77%, 3.47%), 1.20% (− 1.45%, 3.93%), and 4.14% (1.34%, 7.02%) increase in FPG, a 0.93% (− 0.80%, 2.70%), 1.32% (− 0.47%, 3.13%), and 4.48% (2.60%, 6.40%) increase in HbA1c, and a − 1.98% (− 7.96%, 4.39%), 0.12% (− 6.13%, 6.79%), and − 9.24% (− 15.04%, − 3.03%) alteration in HOMA2-β. No statistically significant associations of urinary glyphosate with HOMA2-IR and HOMA2-IS were observed in all models (all P and P for trend > 0.05). Meanwhile, restricted cubic spline (RCS) also showed statistically significant linear positive dose-response associations of urinary glyphosate with FPG and HbA1c (all P for overall < 0.05 and P for non-linear > 0.05, Fig. 2). A linear negative relationship between urinary glyphosate and HOMA2-β was also noted (P for overall < 0.05 and P for non-linear > 0.05, Fig. 2). For each twofold increase in urinary glyphosate levels, FPG and HbA1c increased by 1.13% and 1.50%, respectively, while HOMA2-β decreased by 2.80% (all P < 0.05, Table S2).

Associations of urinary glyphosate with glucose homeostasis indices (N = 2094). Model 1 was unadjusted for any confounders; Model 2 was adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), and survey cycles (2013–2014/2015–2016/2017–2018); Model 3 was adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), survey cycles (2013–2014/2015–2016/2017–2018), BMI (continuous, kg/m2), education level (less than high school/high school or equivalent/college or above), smoking status (yes/no), drinking status (yes/no), physical activity (no/moderate/vigorous), family history of diabetes (yes/no), and antidiabetic medication history (yes/no). CI confidence interval, FPG fasting plasma glucose, FINS fasting insulin, HbA1c glycated hemoglobin A1c, HOMA2-β homeostatic model assessment of beta-cell function, HOMA2-IR homeostasis model assessment of insulin resistance, HOMA2-IS homeostasis model assessment of insulin sensitivity. Significant values are in [bold].

Restricted cubic splines of the associations between urinary glyphosate and glucose homeostasis indices (N = 2094). Models were adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), survey cycles (2013–2014/2015–2016/2017–2018), BMI (continuous, kg/m2), smoking status (yes/no), drinking status (yes/no), physical activity (no/moderate/vigorous), educational level (less than high school/high school or equivalent/college or above), family history of diabetes (yes/no), and antidiabetic medication history (yes/no). CI confidence interval, FPG fasting plasma glucose, FINSfasting insulin, HbA1c glycated hemoglobin A1c, HOMA2-β homeostatic model assessment of beta-cell function, HOMA2-IR homeostasis model assessment of insulin resistance, HOMA2-IS homeostasis model assessment of insulin sensitivity. Significant values are in [bold].
Figures 3 and 4 show the modification effect of overweight/obesity and central obesity on the associations between urinary glyphosate and glucose homeostasis indices. Noteworthily, central obesity may be a more important effect modifier of the association between glyphosate and glucose homeostasis than general overweight/obesity. Overweight/obesity only significantly modified the association of urinary glyphosate with HOMA2-β (P for modification < 0.05, Fig. 3). Each doubling increase in urinary glyphosate was associated with a − 0.39% (95% CI − 3.47%, 2.80%) and − 4.21% (− 6.77%, − 1.58%) alteration in non-overweight/obese and overweight/obese individuals, respectively (Table S4). Central obesity remarkably modified the associations of urinary glyphosate with FINS, HbA1c, and HOMA2-β (all P for modification < 0.05, Fig. 4). The associations between urinary glyphosate and homeostasis indices were all more reinforced in central obese individuals. Each twofold increase in urinary glyphosate was associated with a 1.32% (0.03%, 2.63%), − 4.54% (− 7.98%, − 0.98%), 1.89% (1.00%, 2.78%), − 5.25% (− 8.00%, − 2.42%), 4.03% (0.30%, 7.90%), and − 3.88% (− 7.32%, − 0.30%) alteration of FPG, FINS, HbA1c, HOMA2-β, HOMA2-IS, and HOMA2-IR in central obese individuals, respectively (Table S4).

Restricted cubic splines of the associations between urinary glyphosate and glucose homeostasis indices stratified by overweight/obesity (N = 2094). Models were adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), survey cycles (2013–2014/2015–2016/2017–2018), smoking status (yes/no), drinking status (yes/no), physical activity (no/moderate/vigorous), educational level (less than high school/high school or equivalent/college or above), family history of diabetes (yes/no), and antidiabetic medication history (yes/no). CI confidence interval, FPG fasting plasma glucose, FINS fasting insulin, HbA1c glycated hemoglobin A1c, HOMA2-β homeostatic model assessment of beta-cell function, HOMA2-IR homeostasis model assessment of insulin resistance, HOMA2-IS homeostasis model assessment of insulin sensitivity. Significant values are in [bold].

Restricted cubic splines of the associations between urinary glyphosate and glucose homeostasis indices stratified by central obesity (N = 2094). Models were adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), survey cycles (2013–2014/2015–2016/2017–2018), smoking status (yes/no), drinking status (yes/no), physical activity (no/moderate/vigorous), educational level (less than high school/high school or equivalent/college or above), family history of diabetes (yes/no), and antidiabetic medication history (yes/no). CI confidence interval, FPG fasting plasma glucose, FINS fasting insulin, HbA1c glycated hemoglobin A1c, HOMA2-β homeostatic model assessment of beta-cell function, HOMA2-IR homeostasis model assessment of insulin resistance, HOMA2-IS homeostasis model assessment of insulin sensitivity. Significant values are in [bold].
Stratified analyses showed that sex, smoking status, drinking status, and physical exercise did not exert a statistically significant modification effect on the associations between urinary glyphosate and glucose homeostasis indices (all P for modification > 0.05, Table S4). Of note, age significantly modified the association between urinary glyphosate and HbA1c (P for modification < 0.05). The above association was more evident among individuals aged > 45 years (percent change: 1.85%, 95% CI 1.02%, 2.70%). Sensitivity analysis also showed similar associations between urinary glyphosate and glucose homeostasis indices. When regarding unadjusted urinary glyphosate level as the exposure, compared with participants in the lowest quartile of urinary glyphosate, those in the highest quartile had a 3.74% and 5.45% increase in FPG and HbA1c, respectively (all P for trend < 0.05, Table S5). The relationships between urinary glyphosate and FPG, HbA1c, and HOMA2-β remained statistically significant after excluding participants with potentially invalid urinary samples (all P for trend < 0.05, Table S6).
Association of urinary glyphosate with ALP
Table S3 and Fig. 5 reveal a significant association between urinary glyphosate and ALP. In the fully adjusted model, participants in the fourth quartile of urinary glyphosate had a 4.68% (95% CI 0.71%, 8.81%) increment in ALP as compared with those in the lowest quartile (P trend < 0.05) (Fig. 5A). RCS also displayed a statistically significant positive association between urinary glyphosate and ALP (Fig. 5B). Continuous variable analysis showed that each twofold increase in urinary glyphosate was corresponding to a 1.69% (95% CI 0.48%, 2.92%) increase in ALP (Table S3). Stratified analyses showed that both age, sex, and central obesity statistically significantly modified the relationship between urinary glyphosate and ALP (all P for modification < 0.05, Table S4). Notably, the association was more pronounced among individuals aged > 45 years, females, and individuals with central obesity. Additionally, sensitivity analyses also showed robust results (Tables S5 and S6).

Associations of urinary glyphosate with ALP (N = 2094). (A) Model 1 was unadjusted for any confounders; Model 2 was adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), and survey cycles (2013–2014/2015–2016/2017–2018); Model 3 was adjusted for age (continuous, years), sex (male/female), race/ethnicity (Mexican American/Non-Hispanic White/Non-Hispanic Black/others), survey cycles (2013–2014/2015–2016/2017–2018), BMI (continuous, kg/m2), education level (less than high school/high school or equivalent/college or above), smoking status (yes/no), drinking status (yes/no), physical activity (no/moderate/vigorous), family history of diabetes (yes/no), and antidiabetic medication history (yes/no). (B) Restricted cubic spline of the association between urinary glyphosate and ALP with fully adjusted model. ALP alkaline phosphatase, CI confidence interval. Significant values are in [bold].
Role of ALP in the associations between urinary glyphosate and glucose homeostasis indices
Significant dose-response associations were observed between ALP level and glucose homeostasis indices, including FPG, FINS, HbA1c, HOMA2-IR, and HOMA2-IS levels (all P and P for trend < 0.05, Table S7), except for HOMA2-β (P and P for trend > 0.05). Each twofold augment in ALP level was significantly linked with a 5.08%, 14.21%, 4.45%, 16.35%, and − 14.05% alteration in FPG, FINS, HbA1c, HOMA2-IR, and HOMA2-IS levels, respectively (all P < 0.05, Table S7). Urinary glyphosate and ALP showed no interaction effects on FPG, FINS, HOMA2-IR, and HOMA2-IS levels (data not shown, all P > 0.05), but HbA1c (data not shown, P < 0.05). Table 2 shows the results of further mediation analyses. ALP partially mediated the associations of urinary glyphosate with FPG and HbA1c, with mediated proportions of 9.91% and 20.23%, respectively.
Discussion
In the present study, urinary glyphosate was linearly associated with glucose homeostasis indices, including FPG, HbA1c, and HOMA2-β, which indicated that exposure to glyphosate may result in abnormal blood glucose and β cell dysfunction. Intriguingly, the associations between urinary glyphosate and homeostasis indices were modified by overweight/obesity and central obesity, with more reinforced associations observed among overweight/obese and central obese participants. Moreover, this study revealed a mediated effect of urinary glyphosate on FPG and HbA1c through ALP. These findings provide evidence for the potential impact of environmental exposure on glyphosate and glucose metabolism abnormalities, suggesting the need to strengthen the regulation of glyphosate use to safeguard human health.
As a leading herbicide globally, glyphosate is extensively utilized across an array of broad-spectrum herbicidal formulations, serving residential, commercial, and agricultural purposes. Previously, most research focused on assessing glyphosate exposure in occupational or agricultural populations. A review comprehensively summarized glyphosate exposure levels in occupational settings, with concentrations detected in urine ranging from 0.26 to 292 μg/L28. In contrast, the level of exposure to glyphosate in the general population from the NHANES 2013–2014 was relatively low, with a median (IQR) of 0.392 (0.263–0.656) μg/L7. Despite the relatively low levels of glyphosate exposure in the general population, the adverse health effects resulting from exposure to glyphosate in the general population have aroused growing concerns. A review study has demonstrated that glyphosate satisfies important characteristics of endocrine-disrupting chemicals (EDCs), including activating hormone receptors, altering hormone receptor expression, affecting signal transduction in hormone-responding cells, inducing epigenetic modifications in hormone-producing cells, and altering hormone synthesis and distribution19, and some of these characteristics were closely associated with altered β cell physiology and increased the risk of diabetes29,30. Previous studies have also evaluated the impact of glyphosate exposure on the risk of diabetes prevalence20,31. However, evidence on the associations of glyphosate exposure with glucose dyshomeostasis was scarce. The current study substantiated the links between glyphosate exposure and glucose dyshomeostasis indices and provided vital insights for elucidating the underlying mechanisms.
The present study directly examined the associations between urinary glyphosate levels and glucose homeostasis indices, finding that exposure to glyphosate was associated with elevated FPG and HbA1c levels, as well as reduced HOMA2-β. Our results revealed that glyphosate exposure might disrupt the normal regulation of blood glucose metabolism. Similar to our findings, prior literature assessing the potential health risks of glyphosate exposure among occupational workers documented significant alterations in amino acid metabolism, and energy metabolism (glycolysis and tricarboxylic acid cycle) in the exposed group as compared to the control group32. An in vivo study confirmed that glyphosate exposure altered glucose and lipid metabolism through the escalation of oxidative stress markers33. In-depth, it elucidated that glyphosate could exert detrimental effects on the insulin receptor substrate-1/phosphatidylinositol-3 kinase/Akt (IRS-1/PI3K/Akt) signaling pathways, which might disturb β cell function, destabilize glucose homeostasis, and potentially precipitate the onset of diabetes33.
Interestingly, the associations between urinary glyphosate levels and glucose homeostasis indices were significantly modified by both overweight/obesity and central obesity. More pronounced associations between glyphosate exposure and glucose homeostasis indices were observed among overweight/obese or central obese individuals. As widely acknowledged, obesity itself is a well-established risk factor for diabetes. It can trigger chronic tissue inflammation, which may subsequently lead to insulin resistance, β-cell dysfunction, and eventually diabetes34. Of note, the prevalence of adult obesity is likely to continue to rise nationwide in the US, with nearly 50% of adults becoming obese by 203035,36. In light of this alarming trend, it is imperative that public health efforts increasingly focus on the potential health hazards of environmental glyphosate exposure, particularly among overweight/obese populations. It was noteworthy that central obesity had a more pronounced modification effect on the associations between glyphosate and glucose homeostasis indices than general overweight/obesity. This implies that centrally obese individuals may be more sensitive to the adverse effects of glyphosate exposure on glycaemic metabolism. Previous evidence has demonstrated that central obesity may be a more important risk factor for the development of diabetes than general obesity37. General obesity is typically characterized by subcutaneous fat accumulation, while central obesity is often characterized by an increase in visceral fat. Visceral obesity may partly be a marker of a dysmetabolic state, which can result in insulin resistance by increasing the delivery of free fatty acids to the liver and promoting the secretion of inflammatory cytokines such as interleukin-6 and tumor necrosis factor-α38.
The mediation analysis demonstrated that the associations between urinary glyphosate and both FPG and HbA1c were partially mediated by ALP. This finding indicates that ALP may be a vital intermediary in the pathways linking glyphosate exposure to the disruption of glucose metabolism. On the one hand, ALP has emerged as a biomarker for chronic low-grade inflammation25,39. A single-cell transcriptome analysis revealed that glyphosate exposure augmented the production of reactive oxygen species, induced oxidative stress, and triggered inflammatory responses across various cell populations40. Glyphosate could impair the normal functionality of the typical inflammation pathways such as the Wnt pathway41. Inflammatory responses directly activated Toll-like receptors, which in turn triggered the JNK/IKK and NF-κB signaling pathways, and ultimately resulted in insulin resistance and, in some cases, diabetes42. Furthermore, inflammatory mediators also triggered insulin resistance in insulin target tissues by activating a cascade of intracellular regulators, including suppressors of cytokine signaling proteins, several kinases, and protein tyrosine phosphatases. This activation could subsequently disrupt insulin signaling at the level of the insulin receptor and its substrates4. On the other hand, a significantly positive association was observed between urinary glyphosate and ALP, which implicated the potential hepatotoxic effects of glyphosate and suggested it could induce the release of ALP. In fact, the liver is instrumental in maintaining glucose homeostasis, exerting critical control over a spectrum of metabolic pathways, such as glycogenesis, glycogenolysis, glycolysis, and gluconeogenesis43. Therefore, as a consequence of glyphosate exposure, liver damage could also contribute to glucose dyshomeostasis. Indeed, the mediated effect through ALP appears to only partially account for glucose dyshomeostasis associated with glyphosate exposure. This implied that additional mechanisms, including oxidative stress, might contribute to the dysregulation of glucose homeostasis, as previously mentioned. Further research is required in future studies to elucidate the spectrum of potential mechanisms.
There were several strengths in this study. Firstly, the study investigated the associations between glyphosate exposure and glucose homeostasis in the US general population. Secondly, glucose homeostasis in obese individuals was more likely to be affected by glyphosate exposure. Additionally, the above associations were partly mediated by ALP, which offered an opportunity to dissect and assess the underlying mechanisms linking glyphosate exposure to glucose dyshomeostasis. Of course, a few limitations should also be acknowledged. Firstly, the cross-sectional study design can only provide epidemiological clues for the adverse effects associated with glyphosate exposure, but not infer causality. Secondly, although we attempted to avoid interference from the confounders by using multiple-model analyses, stratified analyses, and even sensitivity analyses, it remained challenging to fully cover all potential factors. Furthermore, we primarily concentrated on the impact of glyphosate exposure on glucose homeostasis, while overlooking the possible disturbance of other environmental pollutants. Multiple pollutants analyses are necessary to consider and examine the synergistic and antagonistic effects in further studies.
Conclusion
In summary, urinary glyphosate level was dose-dependently associated with glucose dyshomeostasis, especially for overweight/obese or central obese individuals. ALP played a mediating role in the associations between environmental glyphosate exposure and elevated FPG and HbA1c. The findings not only deliver evidence linking glyphosate exposure to disruptions in glucose homeostasis, but also underscore the underlying mechanisms of glyphosate-related metabolic abnormalities in glucose regulation. Subsequent research is strongly encouraged to validate our findings and delve deeper into the intrinsic mechanisms.
Methods
Study population
The continuous NHANES is an ongoing annual survey implemented by the National Center for Health Statistics to provide national estimates on various health-related topics since 199944. Face-to-face interviews, physical examinations, as well as laboratory tests were carried out for data collection. After excluding individuals without measurements of urinary glyphosate, urinary Cr, FPG, FINS, HbA1c, and ALP, and individuals with kidney disease, 2094 individuals aged ≥ 18 years were finally eligible for analyses. A flow chart of the exclusion of study participants is presented in Fig. S1. The NHANES protocol received approval from the National Center for Health Statistics Ethics Review Board, and all participants provided their informed consent.
Measurement of urinary glyphosate
In general, urine specimens were stored under appropriate frozen (− 70 °C) until analysis. Urinary glyphosate level was quantified with 200 uL urine using ion chromatography isotope dilution tandem mass spectrometry as described elsewhere12. The limit of detection (LOD) and detection rate was 0.2 μg/L and 78.53%, respectively. Results below the LOD were assigned a value of LOD/\(\sqrt{2}\). Valid glyphosate concentrations were calibrated by dividing urinary Cr levels and expressed as μg/g Cr.
Assessment of outcomes
Blood samples were collected in the corresponding survey years (2013–2014, 2015–2016, 2017–2018) by phlebotomists at the mobile examination center (MEC) in the NHANES. All blood specimens were transported at − 20 to − 30 °C and stored frozen at − 70 °C until analysis. FPG, FINS, HbA1c, HOMA2-β, HOMA2-IR, and HOMA2-IS were used to profile glucose homeostasis. Detailed information on the measurements of FPG, FINS, HbA1c, and ALP is summarized in Table S8 according to the NHANES laboratory methods. HOMA2-β, HOMA2-IR, and HOMA2-IS were calculated based on the updated Homeostasis Model Assessment model using the HOMA2 calculator v2.2.3 (https://www.dtu.ox.ac.uk/homacalculator/). Information on how the glucose homeostasis indices related to clinical outcomes and/or the disease process was provided in the Supplementary Material.
Definitions of covariates
Demographic information (age, sex, race/ethnicity, education level), lifestyles (smoking status, drinking status, and physical activity), family disease history, and medication history were obtained by questionnaires at household interviews. Height, weight, and waist circumference were all measured by physical examination. BMI was constructed by dividing weight (kg) by the square of height (m2) and classified as non-overweight/obesity (< 25 kg/m2) and overweight/obesity (≥ 25 kg/m2). Central obesity was defined as a waist circumference of 102 cm or higher in men and 88 cm or higher in women36. Race/ethnicity was categorized as Non-Hispanic White, Non-Hispanic Black, Mexican American, and others. Education level was divided into less than high school, high school, and college or above. Current smokers were defined as participants who smoked at the time of the survey and smoked no less than 100 cigarettes in life45. Current drinkers were defined as participants who consumed at least 12 alcoholic drinks each year45,46. Participants were surveyed about their engagement in regular moderate and/or vigorous recreational physical activities, and the levels of physical activity were categorized as no, moderate, and vigorous47. Family history of diabetes and antidiabetic medication history were obtained by directly asking participants whether they had a family history and took diabetic pills to lower blood glucose.
Statistical analysis
Continuous variables were presented as mean (SD) or median (IQR), while categorical variables were expressed as number (percentage). Continuous variables and categorical variables across the quartiles of urinary glyphosate were compared by using analysis of variance and χ2 test, respectively. Given that urinary glyphosate, glucose homeostasis indices, and ALP were all right-skewed distributions, they were log2-transformed for further analyses.
Three generalized linear models were established to quantify the relationships between urinary glyphosate, glucose homeostasis indices, and ALP. Model 1 was unadjusted for any confounders; Model 2 was adjusted for age, sex, race/ethnicity, and survey cycles; Model 3 was additionally adjusted for BMI, education level, smoking status, drinking status, physical activity, family history of diabetes, and antidiabetic medication history. Based on log2-transformation for exposure and outcome variables, the regression coefficients (βs) and 95% CIs were further converted to percent changes [100% × (2β − 1)] to facilitate the interpretation of the results47. Meanwhile, RCS models were carried out to verify the linearity/nonlinearity of the dose-response relationships between urinary glyphosate, glucose homeostasis indices, and ALP with fully adjusted models.
As obesity was a well-known risk factor for high FPG, we further explored the modification effect of obesity status (including overweight/obesity and central obesity) on the associations between urinary glyphosate and glucose homeostasis. Subsequently, stratified analyses were also performed on the above associations by age (≤ 45 years/> 45 years), sex (male/female), current smoking (no/yes), current drinking (no/yes), or physical exercise (no/yes). Several sensitivity analyses were conducted to test the associations between urinary glyphosate, glucose homeostasis, and ALP. The crude concentration of urinary glyphosate was regarded as the exposure with urinary Cr considered as an independent covariate. Besides, since urine with urinary Cr < 30 mg/dL and urinary Cr > 300 mg/dL might be regarded as invalid samples, we further ruled out participants with invalid urine samples to examine the above associations.
Mediation analyses were adopted to identify the role of ALP in the associations between urinary glyphosate and glucose homeostasis indices by using the R mediation package. All statistical analyses were comprehensively executed utilizing R version 4.2.2 (R Core Team, 2022) and SAS software 9.4 (SAS Institute, Cary, NC, USA). All P values were calculated as two-tailed, with a significance threshold set at 0.05.
Data availability
Data was available from the NHANES public databases (https://www.cdc.gov/nchs/nhanes/index.htm).
References
Benbrook, C. M. Trends in glyphosate herbicide use in the United States and globally. Environ. Sci. Eur. 28, 3. https://doi.org/10.1186/s12302-016-0070-0 (2016).
Battaglin, W. A., Meyer, M. T., Kuivila, K. M. & Dietze, J. E. Glyphosate and its degradation product AMPA occur frequently and widely in U.S. soils, surface water, groundwater, and precipitation. J. Am. Water Resour. Assoc. 50, 275–290. https://doi.org/10.1111/jawr.12159 (2014).
Primost, J. E., Marino, D. J. G., Aparicio, V. C., Costa, J. L. & Carriquiriborde, P. Glyphosate and AMPA, “pseudo-persistent” pollutants under real-world agricultural management practices in the Mesopotamic Pampas agroecosystem, Argentina. Environ. Pollut. 229, 771–779. https://doi.org/10.1016/j.envpol.2017.06.006 (2017).
Kolakowski, B. M. et al. Analysis of glyphosate residues in foods from the canadian retail markets between 2015 and 2017. J. Agric. Food Chem. 68, 5201–5211. https://doi.org/10.1021/acs.jafc.9b07819 (2020).
Van Bruggen, A. H. C. et al. Environmental and health effects of the herbicide glyphosate. Sci. Total Environ. 616–617, 255–268. https://doi.org/10.1016/j.scitotenv.2017.10.309 (2018).
ATSDR. Toxicological profile for glyphosate. U.S. Department of Health and Human Services, Public Health Service, Atlanta, GA. https://www.atsdr.cdc.gov/ToxProfiles/tp214.pdf (2020).
Ospina, M. et al. Exposure to glyphosate in the United States: Data from the 2013–2014 National Health and Nutrition Examination Survey. Environ. Int. 170, 107620. https://doi.org/10.1016/j.envint.2022.107620 (2022).
Bloem, B. R. & Boonstra, T. A. The inadequacy of current pesticide regulations for protecting brain health: The case of glyphosate and Parkinson’s disease. Lancet Planet. Health 7, e948–e949. https://doi.org/10.1016/s2542-5196(23)00255-3 (2023).
Connolly, A. et al. Exploring the half-life of glyphosate in human urine samples. Int. J. Hyg. Environ. Health 222, 205–210. https://doi.org/10.1016/j.ijheh.2018.09.004 (2019).
Zoller, O., Rhyn, P., Zarn, J. A. & Dudler, V. Urine glyphosate level as a quantitative biomarker of oral exposure. Int. J. Hyg. Environ. Health 228, 113526. https://doi.org/10.1016/j.ijheh.2020.113526 (2020).
Zhang, F. et al. Concentration distribution and analysis of urinary glyphosate and its metabolites in occupationally exposed workers in eastern China. Int. J. Environ. Res. Public Health 17, 2943. https://doi.org/10.3390/ijerph17082943 (2020).
Schütze, A., Morales-Agudelo, P., Vidal, M., Calafat, A. M. & Ospina, M. Quantification of glyphosate and other organophosphorus compounds in human urine via ion chromatography isotope dilution tandem mass spectrometry. Chemosphere 274, 129427. https://doi.org/10.1016/j.chemosphere.2020.129427 (2021).
Casassus, B. EU allows use of controversial weedkiller glyphosate for 10 more years. Nature https://doi.org/10.1038/d41586-023-03589-z (2023).
Liang, Z. et al. Association between glyphosate exposure and osteoarthritis in US adults: Especially in people who are obese and inactive in leisure time physical activity. Sci. Total Environ. 927, 172008. https://doi.org/10.1016/j.scitotenv.2024.172008 (2024).
Han, K. et al. Analysis of the association between urinary glyphosate exposure and fatty liver index: A study for US adults. BMC Public Health 24, 703. https://doi.org/10.1186/s12889-024-18189-3 (2024).
Hsiao, C. C., Yang, A. M., Wang, C. & Lin, C. Y. Association between glyphosate exposure and cognitive function, depression, and neurological diseases in a representative sample of US adults: NHANES 2013–2014 analysis. Environ. Res. 237, 116860. https://doi.org/10.1016/j.envres.2023.116860 (2023).
IARC. Monographs Volume 112: Evaluation of Five Organophosphate Insecticides and Herbicides. https://www.iarc.fr/en/media-centre/iarcnews/pdf/MonographVolume112.pdf (2015).
Untalan, M., Ivic-Pavlicic, T. & Taioli, E. Urinary glyphosate levels and association with mortality in the 2013–16 National Health and Nutrition Examination Survey. Carcinogenesis 45, 163–169. https://doi.org/10.1093/carcin/bgad088 (2024).
Muñoz, J. P., Bleak, T. C. & Calaf, G. M. Glyphosate and the key characteristics of an endocrine disruptor: A review. Chemosphere 270, 128619. https://doi.org/10.1016/j.chemosphere.2020.128619 (2021).
Li, W. et al. Association of glyphosate exposure with multiple adverse outcomes and potential mediators. Chemosphere 345, 140477. https://doi.org/10.1016/j.chemosphere.2023.140477 (2023).
Liang, R. et al. The global burden of disease attributable to high fasting plasma glucose in 204 countries and territories, 1990–2019: An updated analysis for the Global Burden of Disease Study 2019. Diabetes Metab. Res. Rev. 38, e3572. https://doi.org/10.1002/dmrr.3572 (2022).
Goodrich, J. A. et al. Exposure to perfluoroalkyl substances and glucose homeostasis in youth. Environ. Health Perspect. 129, 97002. https://doi.org/10.1289/ehp9200 (2021).
Liang, R. et al. Associations of bifenthrin exposure with glucose homeostasis and type 2 diabetes mellitus in a general Chinese population: Roles of protein carbonylation. Environ. Pollut. 315, 120352. https://doi.org/10.1016/j.envpol.2022.120352 (2022).
Zaher, D. M. et al. Recent advances with alkaline phosphatase isoenzymes and their inhibitors. Arch. Pharm. (Weinheim) 353, e2000011. https://doi.org/10.1002/ardp.202000011 (2020).
Webber, M., Krishnan, A., Thomas, N. G. & Cheung, B. M. Association between serum alkaline phosphatase and C-reactive protein in the United States National Health and Nutrition Examination Survey 2005–2006. Clin. Chem. Lab. Med. 48, 167–173. https://doi.org/10.1515/cclm.2010.052 (2010).
Xiong, T. et al. Early maternal circulating alkaline phosphatase with subsequent gestational diabetes mellitus and glucose regulation: A prospective cohort study in China. Endocrine 65, 295–303. https://doi.org/10.1007/s12020-019-01954-5 (2019).
Xiao, T. et al. Higher urinary glyphosate exposure is associated with increased risk of liver dysfunction in adults: An analysis of NHANES, 2013–2016. Environ. Sci. Pollut. Res. Int. https://doi.org/10.1007/s11356-023-30463-2 (2023).
Muñoz, J. P., Silva-Pavez, E., Carrillo-Beltrán, D. & Calaf, G. M. Occurrence and exposure assessment of glyphosate in the environment and its impact on human beings. Environ. Res. 231, 116201. https://doi.org/10.1016/j.envres.2023.116201 (2023).
Martínez-Pinna, J. et al. Endocrine disruptors in plastics alter β-cell physiology and increase the risk of diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 324, E488-e505. https://doi.org/10.1152/ajpendo.00068.2023 (2023).
Al-Abdulla, R., Ferrero, H., Soriano, S., Boronat-Belda, T. & Alonso-Magdalena, P. Screening of relevant metabolism-disrupting chemicals on pancreatic β-cells: Evaluation of murine and human in vitro models. Int. J. Mol. Sci. 23, 4182. https://doi.org/10.3390/ijms23084182 (2022).
Qi, X. et al. Associations between urinary glyphosate and diabetes mellitus in the US general adult: A cross-sectional study from NHANES 2013–2016. Environ. Sci. Pollut. Res. Int. 30, 124195–124203. https://doi.org/10.1007/s11356-023-31015-4 (2023).
Zhang, Q. et al. The study of human serum metabolome on the health effects of glyphosate and early warning of potential damage. Chemosphere 298, 134308. https://doi.org/10.1016/j.chemosphere.2022.134308 (2022).
Jayaraman, S. et al. Glyphosate potentiates insulin resistance in skeletal muscle through the modulation of IRS-1/PI3K/Akt mediated mechanisms: An in vivo and in silico analysis. Int. J. Biol. Macromol. 242, 124917. https://doi.org/10.1016/j.ijbiomac.2023.124917 (2023).
Rohm, T. V., Meier, D. T., Olefsky, J. M. & Donath, M. Y. Inflammation in obesity, diabetes, and related disorders. Immunity 55, 31–55. https://doi.org/10.1016/j.immuni.2021.12.013 (2022).
Ward, Z. J. et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 381, 2440–2450. https://doi.org/10.1056/NEJMsa1909301 (2019).
Liu, B. et al. Trends in obesity and adiposity measures by race or ethnicity among adults in the United States 2011–18: Population based study. BMJ 372, n365. https://doi.org/10.1136/bmj.n365 (2021).
Frank, L. K. et al. Measures of general and central obesity and risk of type 2 diabetes in a Ghanaian population. Trop. Med. Int. Health 18, 141–151. https://doi.org/10.1111/tmi.12024 (2013).
Després, J. P. et al. Abdominal obesity and the metabolic syndrome: Contribution to global cardiometabolic risk. Arterioscler. Thromb. Vasc. Biol. 28, 1039–1049. https://doi.org/10.1161/atvbaha.107.159228 (2008).
Seo, M. S., Shim, J. Y. & Lee, Y. J. Relationship between serum alkaline phosphatase level, C-reactive protein and leukocyte counts in adults aged 60 years or older. Scand. J. Clin. Lab. Investig. 79, 233–237. https://doi.org/10.1080/00365513.2019.1585567 (2019).
Wu, J. et al. Single-cell transcriptome analysis reveals liver injury induced by glyphosate in mice. Cell. Mol. Biol. Lett. 28, 11. https://doi.org/10.1186/s11658-023-00426-z (2023).
Marino, M. et al. Pleiotropic outcomes of glyphosate exposure: From organ damage to effects on inflammation, cancer, reproduction and development. Int. J. Mol. Sci. 22, 12606. https://doi.org/10.3390/ijms222212606 (2021).
Lontchi-Yimagou, E., Sobngwi, E., Matsha, T. E. & Kengne, A. P. Diabetes mellitus and inflammation. Curr. Diabetes Rep. 13, 435–444. https://doi.org/10.1007/s11892-013-0375-y (2013).
Han, H. S., Kang, G., Kim, J. S., Choi, B. H. & Koo, S. H. Regulation of glucose metabolism from a liver-centric perspective. Exp. Mol. Med. 48, e218. https://doi.org/10.1038/emm.2015.122 (2016).
NCHS. About the National Health and Nutrition Examination Survey. https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (2023).
Feng, X. et al. Exposure to volatile organic compounds and mortality in US adults: A population-based prospective cohort study. Sci. Total Environ. 928, 172512. https://doi.org/10.1016/j.scitotenv.2024.172512 (2024).
Kang, D. E. & Oh, S. N. Association between alcohol consumption and metabolic dysfunction-associated steatotic liver disease based on alcohol flushing response in men: The Korea National Health and Nutrition Examination Survey 2019–2021. Nutrients 15, 3901. https://doi.org/10.3390/nu15183901 (2023).
Barrera-Gómez, J. & Basagaña, X. Models with transformed variables: Interpretation and software. Epidemiology 26, e16-17. https://doi.org/10.1097/ede.0000000000000247 (2015).
Acknowledgements
We express our profound gratitude to the NHANES team for their dedication in democratizing access to their valuable data for the public.
Funding
This study was supported by the Major Research Program of the Fundamental Research Funds for the Central Universities (Grand No. YCJJ20242418).
Author information
Authors and Affiliations
Contributions
X.F. designed the study; analyzed data; drafted the work and substantively revised it. M.W. designed the study; analyzed data; and revised the work. Y.W. designed the study; analyzed data; and revised the work. R.L. and C.Y. acquired and interpreted data, designed methods, and comprehensively revised the work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Feng, X., Wang, M., Wang, Y. et al. Associations between environmental glyphosate exposure and glucose homeostasis indices in US general adults: a national population-based cross-sectional study. Sci Rep 15, 1627 (2025). https://doi.org/10.1038/s41598-024-84694-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84694-5
Keywords
This article is cited by
-
First trimester urine glyphosate concentrations and gestational diabetes in nulliparas: a nested case-control study
Environmental Health (2025)
-
Association between visceral adiposity index and hyperuricemia and gout among US adults: a cross-sectional analysis of NHANES 2007–2018
Scientific Reports (2025)
-
Why internists should be concerned about glyphosate
Internal and Emergency Medicine (2025)
-
Toxicological concerns regarding glyphosate, its formulations, and co-formulants as environmental pollutants: a review of published studies from 2010 to 2025
Archives of Toxicology (2025)
