
Abstract
Despite extensive research on pediatric trigger thumb, nationwide data on patient characteristics, coexisting birth defects, and development remain limited. This cohort study, using Korean National Health Insurance data, analyzed 1.9 million births (2009–2012) followed to age 6. We identified 10,167 trigger thumb cases and matched them 1:10 by sex and birth year with controls. Baseline features, congenital malformations (International Classification of Disease-10, Q00-Q89), and development at ages 4–6 (Korean Developmental Screening Test) were compared. Conditional logistic regression assessed comorbidity risk, expressed as odds ratio (OR), while generalized estimating equations evaluated the association between trigger thumb and developmental outcomes. The trigger thumb group (average diagnosis age: 31.3 months, 46.6% male) had 32.6% of surgery rate at an average age of 43 months. Trigger thumb group had significantly higher rates of renal agenesis and other reduction defects of kidney (OR 2.95, 95% CI 1.63–5.37), cleft palate (OR 1.79, 95% CI 1.19–2.70), and circulatory system malformations (OR 1.65, 95% CI 1.10–2.49) compared to controls. However, assessment using the Korean Developmental Screening Test revealed no significant delays in development, including gross and fine motor skills. Pediatric trigger thumb is linked to increased congenital malformations but doesn’t seem to hinder development. Screening for coexisting conditions and reassuring parents about development are crucial.
Similar content being viewed by others


Introduction
Pediatric trigger thumb is characterized by the locking or catching of a finger in a bent position by thickening and trapping in the tendon sheath (A1 pulley). There is some controversy over the exact etiology of pediatric trigger thumb1,2,3. Previously classified as a congenital anomaly, pediatric trigger thumb is rarely detected at birth; approximately 69% of cases are diagnosed at age 2–5 years4,5,6,7. Understanding the prevalence and characteristics of pediatric trigger thumb is essential for effective diagnosis and management. Previous studies have reported varying incidence rates and management plans4,7,8,9.
There is no histological evidence that trigger thumb in children is a congenital condition5. Microscopic examination has shown no signs of infection, inflammation, or degeneration in the thumbs of pediatric patients with trigger thumb10. However, several studies have suggested that genetic factors play an important role in its etiology3,11,12,13. Hence, the potential association with congenital abnormalities highlights the need for further research in pediatric patients with trigger thumbs. Despite these congenital issues, research on developmental delays in children with trigger thumbs remains lacking.
Although pediatric trigger thumb is not a rare disease, there is still a knowledge gap regarding its management and associated congenital comorbidities based on nationwide data. To fill this gap, we analyzed multiple epidemiological features of pediatric patients with trigger thumb in a nationwide cohort population, including the initial diagnosis and surgical treatment rate. In addition, we aimed to comprehensively investigate the presence of congenital comorbidities. We also investigated whether children with trigger thumb experienced developmental delays when comorbid conditions were present.
Methods
Study design and population
This study was approved by the Institutional Review Board (IRB) of our institution (2023-10-204). The requirement for informed consent was waived by the IRB as all personal identifying information was removed from the database. Data for this study was derived from the National Health Insurance Service (NHIS) of Korea, encompassing a cohort of 2,395,966 individuals between 2009 and 2018. Among this cohort, 1,919,162 participants born between 2009 and 2012 were selected and followed up until 2018.
Trigger thumb was defined using Internation Classification of Disease-10 codes (ICD-10), and participants with trigger thumb were matched at a 1:10 ratio with control participants who had no history of trigger thumb. The matching criteria were sex and birth year.
The exposed cohort for trigger thumb was defined using the ICD-10 code M65.3, including M65.30 to M65.35 for various fingers and thumbs, with surgical intervention identified using the operation code N0830 in the Korea NHIS database. This encompassed both general and specific diagnoses for each finger, including the thumb. Both trigger finger and trigger thumb were included in this study because of the interchangeable use of clinical diagnostic codes, and the prevalence of pediatric trigger finger (2nd, 3rd, 4th, or 5th ) was much lower than that of trigger thumb14,15.
The exclusion criteria were the absence of the Korean Developmental Screening Test for Infants and Children (K-DST)16, missing birth weight records, and chromosomal anomalies (ICD-10 codes Q90 to Q99) due to multiple anomalies associated with chromosomal anomalies.
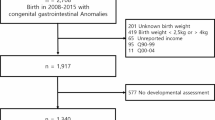
This resulted in 10,167 participants with trigger thumbs and 101,670 control participants (Fig. 1).

Study population. Korea development screening test, The K-DST assessments were conducted at 42–48 months (5th K-DST), 54–60 months (6th K-DST), and 66–71 months (7th K-DST).
The surgical history of trigger thumb was also examined. The trigger thumb group was further divided into surgical and nonsurgical groups for analysis, and their characteristics were compared.
Concurrent congenital comorbidity
Associations between pediatric trigger thumb and other congenital comorbidities were also considered. The presence of congenital comorbidities was examined based on ICD-10 codes, starting with the Q code, to ensure comprehensive assessment17. The percentage of patients with congenital comorbidities was compared between the trigger thumb and control groups. The higher and lower ICD-10 categories were analyzed separately. The details of the ICD-10 codes, including the higher and lower categories of congenital anomalies, are summarized in Supplemental Table 118.
K-DST for developmental screening
K-DST is a validated developmental screening tool specifically designed for Korean children. Pediatricians use this tool to screen for developmental issues, monitor progress, and assess the effects of interventions19. K-DST assessments were conducted at 42–48 months (5th K-DST), 54–60 months (6th K-DST), and 66–71 months (7th K-DST). This study analyzed changes in K-DST results over time using these assessments.
K-DST evaluates six developmental domains: gross motor skills, fine motor skills, cognition, language, social skills, and self-help. Each domain has eight questions scored from 0 to 3, resulting in a total score of 0 to 24 for each domain. These scores are categorized into four levels based on the total score in each domain: advanced development (total score ≥ 1 standard deviation [SD]), age-appropriate (total score ≥ − 1 SD and < 1 SD), need for follow-up (total score ≥ − 2 SD and < − 1 SD), and recommendation for further evaluation (total score < − 2 SD)19,20.
In this study, the primary focus was identifying adverse outcomes, defined as scores indicating a “need for follow-up” or a “recommendation for further evaluation” across any of the domains. A child was considered to have an unfavorable overall K-DST score if they recorded an unfavorable result in any of the six domains. The rate of K-DST completion was comparable between the control and pediatric thumb groups, with 81.15% vs. 82.29% for the 5th, 73.12% vs. 75.55% for the 6th, and 50.81% vs. 52.15% for the 7th K-DST. Imputation was used to address the missing values.
Covariates
For comprehensive assessment, the covariates included in this study encompassed a wide range of demographic and clinical characteristics. Demographic characteristics included sex (boys or girls), prematurity status (yes or no), birth weight (kg), breastfeeding status (yes or no), region of birth, and income. Specifically, birth weight, prematurity status, and breastfeeding information were obtained from parental responses to questionnaire items in the first round of the national health screening program. Prematurity was defined as birth before 37 weeks of gestation.
Birth residence was categorized as urban (Seoul, metropolitan, or city), or rural. Seoul is the biggest city of our country. The six metropolitan cities are smaller regional hubs than Seoul and are determined administratively rather than by population. ‘City’ refers to smaller urban areas excluding Seoul and the metropolitan cities. The remaining areas were defined as rural. Income was estimated based on premium quartiles from the Korean National Health Insurance Statistical Yearbook. As all Koreans must pay insurance premiums based on their housing income, we assumed that income would be higher if a patient paid a higher insurance premium. The patients were divided into four groups for convenience of analysis (Q1–Q4). The lowest 25% and top 25% of the patients were classified as Q1 and Q4, respectively.
Statistical analysis
General characteristics were compared between the pediatric trigger thumb and control groups using the chi-square (for categorical data) and t-tests (for continuous data). The data are expressed as the mean ± SD for continuous variables. For continuous variables such as age or duration, median and interquartile range values were also reported as needed. Categorical variable was expressed as number (percentile).
Conditional logistic regression was used to assess the association between pediatric trigger thumb and congenital comorbidities by calculating odds ratios (ORs) and 95% confidence intervals (CIs). The K-DST results were compared between the pediatric trigger thumb and control groups. Generalized estimating equation (GEE) analysis was used to determine interactions at different time points (5th, 6th, and 7th K-DSTs)21. The results of the GEE analyses are described using group estimates and Wald 95% CIs. All analyses were adjusted for premature birth, income, region of birth, breastfeeding at 4 months of age, and birth weight. The significance level was set at p < 0.05. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
General characteristics of pediatric trigger thumb patients
Table 1 presents the basic demographic characteristics of children with trigger thumb compared with those of the control group. The overall incidence of pediatric trigger thumb was 0.64% (approximately 6 in 1000 births). In the trigger thumb group, 46.8% of the patients were male. In general, no significant clinical differences were found in birth weight or breastfeeding habits between the two groups, although statistical significance was observed, likely because of the large sample size of the study. There were no significant differences in income between the pediatric trigger thumb and control groups (p = 0.191).
The average age at the diagnosis of pediatric trigger thumb was 31.3 months, and the median age was 26 months (Q1–Q3:16–41 months). In total, 32.6% of the patients in the trigger thumb group underwent surgical treatment. The average duration from the initial diagnosis of pediatric trigger thumb to surgical treatment was 11.3 months, with a median of 3 (Q1–Q3: 1–17) months. The average age at surgery was 43.0 (4–113) months, and the median age at surgery was 40 (30–53) months. When comparing the general characteristics of the operated and non-operated trigger thumb groups, there were no differences in sex, prematurity, birth weight, breastfeeding, or income level (p > 0.05, Supplemental Table 2).
Concurrent congenital comorbidity
We analyzed congenital malformations among children with trigger thumb and found several significant associations compared with the matched unexposed cohort. Overall, the trigger thumb group exhibited a higher prevalence of congenital malformations in some disease categories. We found that children with trigger thumb had notably greater odds of renal agenesis and other reduction defects of kidney, with an OR of 2.95 (95% CI 1.63–5.37). In addition, there was a significantly increased risk of cleft palate among children with trigger thumb, with an OR of 1.79 (95% CI 1.19–2.70). Furthermore, our analysis revealed a significant association with circulatory system conditions, where the odds ratio was 1.65 (95% CI 1.10–2.49), indicating a modest but statistically significant increase. These results underscore the broader association of pediatric trigger thumb, which extends beyond the musculoskeletal system to include other congenital malformations, such as kidney malformations and circulatory system conditions. The statistical results for each disease category are summarized in Fig. 2.

Forest plot of odds ratios for congenital comorbidity between unexposed matched cohort and trigger thumb cohorts. This forest plot illustrates the odds ratios (OR) with 95% confidence intervals (CI) for the prevalence of various ICD-10 based Q codes comparing matched unexposed cohorts and trigger thumb cohorts. Each row represents a specific diagnosis category, showing the number of event cases in both cohorts and the corresponding odds ratio. The plot helps visualize the differences in disease prevalence, highlighting areas where the trigger thumb cohorts show significantly higher or lower odds compared to the matched unexposed cohorts.
W
Development
Developmental assessments of children with trigger thumb, analyzed using GEE from ages 4 to 6 years, revealed no significant interaction with time (all p < 0.05). The overall developmental outcomes according to the K-DST did not significantly differ between the trigger thumb and control groups (OR 1.05, 95% CI 0.99–1.16, p = 0.0560). Gross and fine motor skill assessments indicated no developmental delay attributable to trigger thumb. Cognitive, language, and self-help skill development were comparable to the control group, while social skills showed a slight improvement compared to the control group, indicating no significant deficits. These results indicate that despite the presence of congenital malformations associated with trigger thumb, the condition does not adversely affect developmental milestones in various domains during early childhood. The detailed statistical results for each developmental domain are summarized in Table 2.
Discussion
This study provides insights into the characteristics, congenital comorbidities, and developmental outcomes of children with trigger thumbs. The incidence was 0.64%, with no significant demographic differences in birth weight, breastfeeding habits, or income levels between the affected and control groups. Notably, children with trigger thumb have greater odds of developing musculoskeletal malformations, lens malformations, or circulatory system conditions. Despite these associations, developmental assessments using GEE showed no significant delays in gross motor, fine motor, cognitive, language, social, or self-help skills. These results indicate that although pediatric trigger thumb is linked to certain congenital malformations, it does not adversely affect the overall developmental milestones during early childhood, emphasizing the need for comprehensive care and monitoring.
Our study revealed a trigger thumb incidence of 6 per 1,000 births in this cohort, which is slightly greater than the previously reported range of 1–3 per 1,000 births5,22,23,24,25. This discrepancy may be due to underestimation in previous studies with limited sample sizes, overestimation in our study due to the inclusion of cases that mimic trigger thumb, and ethnic variations, as seen in the higher rates among Hispanic populations26. A Japanese study reported an incidence of 3.3 cases per 1,000 births5, and their method of postal questionnaires to parents one year after birth might have underestimated the true prevalence. Further research is warranted to investigate these potential explanations and to establish a more accurate understanding of trigger thumb incidence across different populations.
The mean time to diagnosis of trigger thumb was 31.3 months, which is similar to or slightly earlier than the previously reported age4,22,27. Generally, pediatric patients visit clinics with an abnormally flexed thumb and/or an inability to extend the thumb, which is often noticed by their parents or caregivers at approximately age 2 years22. Improved medical accessibility and government pediatric health checkup programs may facilitate earlier diagnosis. In Korea, all children aged 4 months to 6 years are required to undergo pediatric health examinations, which may lead to earlier diagnosis.
More than half of the patients in this study were managed non-surgically. The 32.6% rate of surgical treatment for pediatric trigger thumbs was lower than that previously reported4. In the US, national health claims data showed a 49% rate of surgical treatment for trigger thumb4. The low surgical rate in our study may be due to the early diagnosis of less severe cases, which could be managed with observation or conservative treatment. The outcomes of nonsurgical treatment vary; an observational US study reported spontaneous resolution in approximately one-third of patients8. However, for patients with > 30° interphalangeal joint flexion and contracture at diagnosis, surgical treatment is more likely8. In another prospective follow-up study, the spontaneous resolution rate was estimated to be greater than 75% after at least 5 years of follow-up28. Given the high rate of spontaneous recovery9,29, early detection and supportive care in our study may explain the lower rate of surgical intervention.
Our study found that children with trigger thumb had a higher prevalence of concomitant congenital malformations including renal agenesis and other reduction defect of kidney, cleft palate, and the circulatory system. In addition to these, the items that showed an odds ratio of 1.5 or higher are as follows: congenital malformations and deformations of the musculoskeletal system, congenital malformations of the urinary system, congenital malformations of eye, ear, face and neck, congenital malformations of the respiratory system, congenital malformations of genital organs. This association may be attributed to genetic, environmental, or physiological factors. Pediatric trigger thumb, although not diagnosed at birth, has been reported in twins and siblings, suggesting a congenital or genetic link3,13,30,31. Specific genetic mutations may cause both trigger finger and congenital malformations owing to their impact on musculoskeletal and connective tissue development. Environmental stressors or toxins during critical stages of fetal development can also result in malformations in various body systems, including the lens and circulatory system. These systems are particularly sensitive during early gestation, and disruptions can lead to malformations. Moreover, the trigger thumb itself may indicate abnormalities in specific physiological processes during fetal development, potentially leading to other developmental abnormalities. Mechanical stress or abnormal growth patterns associated with the development of trigger finger can result in systemic malformations. These findings suggest that the association between pediatric trigger finger and concurrent malformations is multifaceted and involves genetic, environmental, and physiological influences, warranting further research to clarify the causal pathways involved.
One point to consider here is the high likelihood of developing musculoskeletal system disorders (ICD-10 codes Q65-79, OR 1.67, 95% CI 1.56–1.78). This could be due to misdiagnosis, as the trigger thumb is often mistaken for a congenital abnormality of the musculoskeletal system, although the actual co-occurrence rate is not high. Some primary care physicians are unfamiliar with this condition and may miscode it as a musculoskeletal malformation. To further clarify this issue and gain a more accurate understanding of the comorbidities associated with pediatric trigger thumb, a more detailed analysis of the lower-level codes within the Q65-79 category is required.
Our study found no significant association between trigger thumb and developmental delay. Despite the presence of trigger thumb and associated congenital malformations, affected children generally achieve developmental milestones at a rate comparable to that of their peers. This lack of association can be attributed to the fact that the trigger thumb primarily affects the tendons and does not disrupt the neurological or muscular systems critical for overall development. These findings highlight the importance of distinguishing between congenital physical abnormalities and their effects on development. Although it is crucial to monitor and manage trigger finger and its associated conditions, parents and healthcare providers can be reassured that the condition alone is unlikely to hinder a child’s development. Further research should continue to monitor developmental outcomes in children with trigger finger to confirm these findings and explore any long-term effects.
A key strength of this study lies in its substantial sample size, exceeding 2,000,000 children, encompassing both those with trigger thumb and a well-matched control group. This large dataset provides robust and representative findings. Furthermore, the use of Generalized Estimating Equations (GEE) effectively addressed potential correlations within the data and allowed for the adjustment of multiple confounders, thereby enhancing the reliability of our results. The inclusion of crucial confounding factors such as sex, birth weight, prematurity, breastfeeding, and socioeconomic status significantly strengthened the validity of our conclusions. Finally, the detailed analysis of specific congenital malformations associated with trigger thumbs offers valuable insights into their broader health implications.
However, this study had some limitations. First, the initial diagnostic code for congenital malformations of the trigger thumb and comorbidities could have been incorrectly recorded due to incomplete diagnostic work-up, potentially overestimating the prevalence in patients with trigger thumbs. Second, the health claims data lacked detailed information, making it difficult to discriminate trigger thumb from trigger finger and to analyze laterality and bilateral cases. Third, this study only included patients who visited clinics, potentially excluding subclinical or undiagnosed patients. Finally, the follow-up period ending in 2018 may have missed some children who later underwent surgery.
Conclusion
The prevalence of pediatric trigger thumb was 6 per 1,000 births, with the diagnosis occurring at approximately 31.3 months and surgery performed in 32.6% of cases. Pediatric trigger thumb was associated with a greater incidence of congenital malformations such as musculoskeletal, lens, and circulatory system malformations. However, there was no motor or developmental delay in children with trigger thumbs. These epidemiological features and comorbid conditions of pediatric trigger thumb can be valuable in managing pediatric patients with this condition.
Data availability
The data used in this study cannot be shared publicly due to legal restrictions but are available from the corresponding author upon reasonable request.
References
Murgai, R. R. & Lightdale-Miric, N. Pediatric trigger thumb caused by a flexor tendon sheath ganglion. J. Pediatr. Orthop. B. 29 (2), 203–205. https://doi.org/10.1097/BPB.0000000000000561 (2020).
Twu, J. & Angeles, J. Developmental trigger thumb. Pediatr. Ann. 45 (4), e135–e138. https://doi.org/10.3928/00904481-20160317-02 (2016).
Ahmadi, S., Akbari, H., Shafaei, Y. & Akbari, P. Trigger thumb in twins: case report. World J. Plast. Surg. 10 (2), 110–114. https://doi.org/10.29252/wjps.10.2.110 (2021).
Park, K. M., Immerman, I. & Rahgozar, P. Trends in the management of pediatric trigger thumb in the united States. Hand (N Y). 18 (4), 568–574. https://doi.org/10.1177/15589447211049517 (2023).
Kikuchi, N. & Ogino, T. Incidence and development of trigger thumb in children. J. Hand Surg. Am. 31 (4), 541–543. https://doi.org/10.1016/j.jhsa.2005.12.024 (2006).
Rodgers, W. B. & Waters, P. M. Incidence of trigger digits in newborns. J. Hand Surg. Am. 19 (3), 364–368. https://doi.org/10.1016/0363-5023(94)90046-9 (1994).
Slakey, J. B. & Hennrikus, W. L. Acquired thumb flexion contracture in children: congenital trigger thumb. J. Bone Joint Surg. Br. 78 (3), 481–483 (1996).
Hutchinson, D. T., Rane, A. A. & Montanez, A. The Natural History of Pediatric Trigger Thumb in the United States. J Hand Surg Am. ;46(5):424 e1- e7. (2021). https://doi.org/10.1016/j.jhsa.2020.10.016
Baek, G. H. et al. The natural history of pediatric trigger thumb. J. Bone Joint Surg. Am. 90 (5), 980–985. https://doi.org/10.2106/JBJS.G.00296 (2008).
Buchman, M. T., Gibson, T. W., McCallum, D., Cuda, D. D. & Ramos, A. G. Jr. Transmission electron microscopic pathoanatomy of congenital trigger thumb. J. Pediatr. Orthop. 19 (3), 411–412 (1999).
Wong, A. L., Wong, M. J., Parker, R. & Wheelock, M. E. Presentation and aetiology of paediatric trigger finger: a systematic review. J. Hand Surg. Eur. Vol. 47 (2), 192–196. https://doi.org/10.1177/17531934211035642 (2022).
Shim, V. C., Admire, A. A., Heidenreich, R. A. & Samimi, K. J. Autosomal dominant inheritance pattern for trigger thumb. Plast. Reconstr. Surg. 109 (1), 240–241. https://doi.org/10.1097/00006534-200201000-00036 (2002). discussion 2.
Kakel, R., Van Heerden, P., Gallagher, B. & Verniquet, A. Pediatric trigger thumb in identical twins: congenital or acquired? Orthopedics 33 (3). https://doi.org/10.3928/01477447-20100129-33 (2010).
Shah, A. S. & Bae, D. S. Management of pediatric trigger thumb and trigger finger. J. Am. Acad. Orthop. Surg. 20 (4), 206–213. https://doi.org/10.5435/JAAOS-20-04-206 (2012).
Cardon, L. J., Ezaki, M. & Carter, P. R. Trigger finger in children. J. Hand Surg. Am. 24 (6), 1156–1161. https://doi.org/10.1053/jhsu.1999.1156 (1999).
Kim, D. et al. Korean developmental screening test for infants and children (K-DST): development, applications, and implications for future early childhood development interventions. Clin. Exp. Pediatr. 66 (7), 288–293 (2023).
Teggi, R., Familiari, M., Gatti, O. & Bussi, M. Vertigo without cochlear symptoms: vestibular migraine or Meniere disease? Neurol. Sci. https://doi.org/10.1007/s10072-021-05215-0 (2021).
The Structure of an ICD-10-CM. Code https://training.seer.cancer.gov/icd10cm/icd10cm-code-structure.html
Yi, Y. Y. et al. Neurodevelopment in term infants with normal birthweight following postnatal systemic steroid exposure. Neuroepidemiology https://doi.org/10.1159/000536100 (2024).
Kim, J. H. et al. Cohort profile: National investigation of birth cohort in Korea study 2008 (NICKs-2008). Clin. Exp. Pediatr. 64 (9), 480–488. https://doi.org/10.3345/cep.2020.01284 (2021).
Ha, E. K. et al. Rotavirus hospitalization in early childhood: fine motor skills and cognition at six years old-Population-based cohort study. J. Infect. Dis. https://doi.org/10.1093/infdis/jiae218 (2024).
Dinham, J. M. & Meggitt, B. F. Trigger thumbs in children. A review of the natural history and indications for treatment in 105 patients. J. Bone Joint Surg. Br. 56 (1), 153–155 (1974).
Hudson, D. A., Grobbelaar, A. O. & Bloch, C. E. Trigger thumb in children–results of simple surgical treatment. S Afr. J. Surg. 36 (3), 91–92 (1998).
Steenwerckx, A., De Smet, L. & Fabry, G. Congenital trigger digit. J. Hand Surg. Am. 21 (5), 909–911. https://doi.org/10.1016/S0363-5023(96)80213-9 (1996).
Ger, E., Kupcha, P. & Ger, D. The management of trigger thumb in children. J. Hand Surg. Am. 16 (5), 944–947. https://doi.org/10.1016/s0363-5023(10)80165-0 (1991).
Ashford, J. S. & Bidic, S. M. Evaluation of pediatric trigger thumb in the Hispanic population at a Southwest urban medical center. Plast. Reconstr. Surg. 124 (4), 1221–1224. https://doi.org/10.1097/PRS.0b013e3181b59ac1 (2009).
Bae, D. S., Sodha, S. & Waters, P. M. Surgical treatment of the pediatric trigger finger. J. Hand Surg. Am. 32 (7), 1043–1047. https://doi.org/10.1016/j.jhsa.2007.05.031 (2007).
Baek, G. H. & Lee, H. J. The natural history of pediatric trigger thumb: a study with a minimum of five years follow-up. Clin. Orthop. Surg. 3 (2), 157–159. https://doi.org/10.4055/cios.2011.3.2.157 (2011).
Leong, L., Chai, S. C., Howell, J. W. & Hirth, M. J. Orthotic intervention options to non-surgically manage adult and pediatric trigger finger: A systematic review. J. Hand Ther. 36 (2), 302–315. https://doi.org/10.1016/j.jht.2023.05.016 (2023).
Wang, E. D., Xu, X. & Dagum, A. B. Mirror-image trigger thumb in dichorionic identical twins. Orthopedics 35 (6), e981–e983. https://doi.org/10.3928/01477447-20120525-48 (2012).
Brinkman, D., Sheridan, G. & O’Sullivan, M. Trigger twins: 2 cases of ipsilateral twin trigger digit and a review of published literature. Case Rep. Orthop. 2019, 8697360. https://doi.org/10.1155/2019/8697360 (2019).
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2022R1F1A1074057) and by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (No. HR22C1605).
Author information
Authors and Affiliations
Contributions
S.K.: Project administration; data curation; formal analysis; writing original draftH.L.: Data curation; formal analysis; writing original draftH.Y.: Data curation, formal analysisB.H.: Data curationM.H.: Conceptualization; funding acquisition; investigation; methodology; manuscript review and editingS.L.: Conceptualization; funding acquisition; investigation; methodology; manuscript review and editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, S.Y., Lee, H.I., Yoo, HN. et al. Association of trigger thumb with congenital malformations and developmental milestones among children in a nationwide birth cohort. Sci Rep 15, 16952 (2025). https://doi.org/10.1038/s41598-025-01423-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01423-2
