
Abstract
Durvalumab has demonstrated significant efficacy in several types of malignancies, while large-scale real-world safety studies remain limited. This study aimed to systematically evaluate the safety of durvalumab through data mining of the U.S. Food and Drug Administration Adverse Event Reporting System (FAERS). We extracted reports of durvalumab as the primary suspected drug from the FAERS database (January 2017 to June 2024). Four disproportionality analysis algorithms were used to detect signals between durvalumab and adverse events (AEs). Durvalumab was recorded in 10,120 reports as the primary suspected drug. Of these, 43.6% of AEs occurred during the first month of treatment, with a median onset time of 40 days (IQR: 14–99 ). Among 181 potential signals, 64 were unexpected preferred terms not listed in the prescribing information, including cytokine release syndrome (CRS), pulmonary tuberculosis, radiation esophagitis, oesophageal fistula, oesophageal perforation, pleural effusion, pneumothorax, cerebral infarction, biliary tract infection, cholecystitis, psoriasiform dermatitis, portal vein thrombosis, acute cholangitis and pericarditis malignant. Serious adverse events accounted for 93.3% of cases. Males exhibited a significantly higher risk of experiencing serious outcomes compared to females (OR = 1.83, 95% CI: 1.52–2.19, P < 0.001). Older age groups demonstrated an elevated risk of severe outcomes relative to those under 65 years (65–74 years: OR = 1.52, 95% CI: 1.15-2.00, P = 0.003; ≥75 years: OR = 1.40, 95% CI: 1.02–1.92, P = 0.038). This study comprehensively assessed the safety of durvalumab and discovered potential new adverse event signals, which may provide critical support for risk identification and monitoring of durvalumab.
Similar content being viewed by others


Introduction
Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of cancer patients by modifying the interactions between T lymphocytes, antigen-presenting cells, and tumor cells. ICIs modify the immune system rather than directly target the cancer cells1,2. Since the approval of anti-cytotoxic T-lymphocyte-associated protein 4 (anti-CTLA-4) for the treatment of metastatic melanoma in 2011, antibodies targeting programmed death-1 (PD-1) and its ligand programmed death-ligand 1 (PD-L1) have also been successively approved for clinical cancer therapy3. These ICIs interfere with co-inhibitory signaling pathways, activate antitumor immune responses, and help the immune system clear cancer cells2.
Durvalumab, formerly MEDI-4736, is a highly selective human immunoglobulin (Ig)G1 monoclonal antibody with high affinity. It prevents PD-L1 from attaching to PD-1 and CD80, helping T cells to identify and kill tumor cells4. Due to the significant efficacy of durvalumab demonstrated in clinical trials, it was approved for immunotherapy of various advanced tumors: accelerated approval in May 2017 for platinum-refractory metastatic urothelial carcinoma5; consolidation therapy for unresectable stage III NSCLC after chemoradiotherapy (PACIFIC trial, 2018)6, first-line treatment for extensive-stage SCLC (CASPIAN trial, March 2022)7, combination therapy with tremelimumab (Imjudo®) for unresectable hepatocellular carcinoma (HIMALAYA study, October 2022)8, and combination with gemcitabine/cisplatin for advanced biliary tract cancer (TOPAZ-1 trial, 2022)9,10.
With the growing number of approved indications, durvalumab is being used more extensively in clinical practice. Although it demonstrates a favorable safety profile compared to conventional chemotherapy, the agent carries risks of immune-related adverse events (irAEs) that can affect any organ system and lead to severe or fatal outcomes11. In the pivotal PACIFIC trial of stage III NSCLC, patients without progression after platinum-based chemoradiotherapy received durvalumab consolidation therapy, which resulted in grade 3–4 AEs in 29.9% of patients, with 15% discontinuing treatment and 4.4% mortality attributed to AEs12. Therefore, early identification and management of adverse drug reactions are essential to ensuring the safe use of durvalumab. Reported AEs encompass diverse manifestations including pneumonitis, endocrine disorders, gastrointestinal toxicity, hematological complications, and cardiovascular events12,13,14,15,16,17,18. Given that durvalumab has been commercially available for less than ten years, current safety evidence primarily originates from clinical trials limited by restricted sample sizes, stringent eligibility criteria, and underdetection of rare/long-term events. To address these knowledge gaps, this pharmacovigilance study systematically evaluates the post-marketing safety profile of durvalumab using data mining from the FAERS database.
Method
Data sources
This observational, retrospective pharmacovigilance investigation employed a disproportionality analysis to explore potential connections between durvalumab and reported AEs. Ethics approval was unnecessary for this investigation since the data downloaded did not include patient privacy. We extracted data from the FAERS database covering 30 quarterly data files (January 2017–June 2024).
Data processing
FAERS raw data were analyzed using SAS 9.4. Duplicate reports were resolved using the FDA-recommended method: (1) retaining the most recent FDA_DT for identical CASE IDs; (2) selecting higher PRIMARY IDs when CASE ID and FDA_DT are the same; (3) excluding reports listed in FDA quarterly deletion updates19. Durvalumab-related cases were identified through the PROD_AI and DRUGNAME fields using both generic name (durvalumab) and brand name (Imfinzi®). Only cases designating durvalumab as the “Primary Suspect” were included for exposure assessment. The preferred term (PT) from MedDRA(version 27.0) was used to code AEs in the FAERS database.
Data analysis
A disproportionality analysis determined the proportion of AEs between a particular drug and all other drugs. Four disproportionality analysis algorithms were employed to detect potential AE signals associated with durvalumab, including the reporting odds ratio (ROR)20, proportional reporting ratio (PRR)21, Bayesian confidence propagation neural network (BCPNN)22, and multi-item gamma Poisson shrinker (MGPS)23. All algorithms were based on a fourfold Table19. The combination of these four algorithms overcomes the limitations of individual methods and improves result reliability. AE signals were generated when meeting the criteria of all four algorithms simultaneously. Equations and thresholds for the algorithms are detailed in Table 1. Given that the primary indications for durvalumab are unresectable stage III non-small cell lung cancer (NSCLC), extensive-stage small cell lung cancer (ES-SCLC), metastatic biliary tract cancer (BTC), and unresectable hepatocellular carcinoma (uHCC), it is predominantly used in advanced malignancies. To minimize confounding by disease progression, AE signals plausibly linked to tumor progression (malignant neoplasm progression, central nervous system metastases, hepatic metastases, osseous metastases, recurrence of non-small cell lung carcinoma, and metastases to specified anatomical sites) were excluded. Corresponding preferred terms (PTs) were removed from analysis. A flowchart of data processing is provided in Fig. 1.

Flowchart of identification of positive signals associated with durvalumab from FAERS between Q1 of 2017 and Q2 of 2024.
AEs that were life-threatening or resulted in hospitalization, disability, or death were classified as serious adverse events (SAEs). The proportion of SAEs was calculated by dividing the number of SAEs by the total AE count. Reports were stratified into SAE and non-SAE groups to assess the impact of age and gender on severe outcomes.To ensure analytical accuracy, reports with missing values for sex or age were excluded. Pearson’s chi-square test was used to compare SAE incidence24. Risk associations were quantified using odds ratios (OR) with 95% confidence intervals (CI). All analyses were performed in IBM SPSS Statistics v22.0 (IBM Corp., Armonk, NY, USA); P-value < 0.05 was considered statistically significant.
Time-to-onset (TTO) was defined as the interval between the initiation of durvalumab therapy and the occurrence of adverse events (AEs). Reports with invalid data or missing/incomplete dates were excluded from the analysis. The median and interquartile range (IQR) were used to characterize TTO in this study.
Results
Basic characteristics of AEs
Between Q1 of 2017 and Q2 of 2024, 10,781,117 AE reports were retrieved from the FAERS database, among which 10,120 reports (0.1%) listed durvalumab as the primary suspected drug. Demographic and clinical details are summarized in Table 2. Gender information was available for 8,580 patients, with a male predominance (56.9%) compared to females (27.9%). Excluding reports with missing age data, AEs primarily occurred in older patients (≥ 65 years, n = 4,067, 40.2%). The most frequent indication for durvalumab use was non-small cell lung cancer (34.5%). Japan reported the highest number of AE cases (n = 2,763, 27.3%), followed by the United States (n = 2,223, 22.0%) and China (n = 1,214, 12.0%). Regarding outcomes, the most common were hospitalization/prolonged hospitalization (n = 3,389, 33.5%), death (n = 3,089, 30.5%), and life-threatening events (n = 851, 8.4%). A total of 9,444 reports were classified as serious, representing 93.3% of all reports. Additionally, approximately 71.9% of AEs were reported by healthcare professionals (physicians/pharmacists), suggesting high credibility of these reports.
Signal detection at the system organ class level
In this study, AEs occurred across 27 system organ classes (SOCs); however, significant disproportionality signals were identified in 21 SOCs. The top 5 SOCs by AE frequency were: general disorders and administration site conditions (17.1%), respiratory/thoracic/mediastinal disorders (12.0%), neoplasms (benign/malignant/unspecified) (9.4%), investigations (7.1%), and gastrointestinal disorders (7.0%) (Table 3). The AEs in these SOC categories are consistent with those listed in the prescribing information of durvalumab and are frequently reported in patients treated with this drug.
Signal detection at the PT level
Using four disproportionality analysis algorithms, we detected 223 significant signals that consistently met the predefined threshold criteria across all algorithms. After excluding signals potentially attributable to disease progression, 181 signals were retained. The five most frequent signals were: death (n = 1,848), radiation pneumonitis (n = 707), pneumonitis (n = 556), interstitial lung disease (n = 237), and decreased neutrophil count (n = 227) (Table 4).
Among the 181 signals, 64 unexpected PTs—defined as adverse events not documented in the prescribing information of durvalumab—were identified (Supplementary Table 1), including pulmonary tuberculosis (n = 10; ROR = 6.22), cytokine release syndrome (n = 54; ROR = 5.35), radiation oesophagitis (n = 20; ROR = 145.09), oesophageal perforation (n = 4; ROR = 10.29), and oesophageal fistula (n = 4; ROR = 29.78).
Time to onset analysis
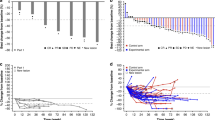
The time to onset of AEs for durvalumab was gathered from the database. Among the 3,719 AEs ( 3719/10120, 36.7%) with available time data, the median onset time was 40 days (IQR 14–99). Most AEs occurred during the first month (n = 1,623; 43.6%) and the second month (n = 686; 18.5%) after treatment initiation(Fig. 2.)

Time to onset of AEs with durvalumab as the primary suspected drug.
Serious vs. non-serious reports
In our study, serious adverse events (SAEs) were recorded in 9,444 reports (93.3%). Men accounted for a higher proportion of SAE cases than women (68.0% vs. 32.0%). Compared to females, males exhibited a significantly higher likelihood of SAEs (OR = 1.83, 95% CI: 1.52–2.19, P < 0.001). Additionally, patients in older age groups demonstrated an increased risk of SAEs compared to those under 65 years (65–74 years: OR = 1.52, 95% CI: 1.15-2.00, P = 0.003; ≥75 years: OR = 1.40, 95% CI: 1.02–1.92, P = 0.038), as shown in Table 5.
Discussion
The use of durvalumab in clinical settings has increased. Due to its mechanism of action, durvalumab is associated with irAEs, some of which can be life-threatening. Currently, most safety data originate from clinical trials or isolated case reports25,26,27, which might offer only a limited perspective on potential safety issues. This study conducted a large-scale real-world pharmacovigilance research, comprehensively evaluating the safety profile of durvalumab based on the FAERS database system.
Among the 181 signals, pneumonia, interstitial lung disease, febrile neutropenia, decreased platelet count, hypothyroidism, colitis, immune-mediated lung disease, myocarditis, and adrenal insufficiency were frequently reported in patients treated with durvalumab. These adverse events have also been documented in the drug’s prescribing information and observed in prior clinical trials, including PACIFIC6, CASPIAN7, TOPAZ-19, and HIMALAYA8 studies. Among the 181 signals, death emerged as the most frequently reported event (n = 1,848; ROR = 5.02), representing 8.73% (1,848/21,164) of all AEs. After the exclusion of missing data, the median time from treatment initiation to death was 75 days (IQR: 26–157), with a median patient age of 67 years (IQR: 60–73). Due to confounding factors such as disease severity and combined medications, it is difficult to determine whether death are related to durvalumab. Given that durvalumab is mainly used for advanced malignancies, where baseline mortality is high, deaths during treatment may be reported regardless of whether they are directly related to the drug, potentially leading to false positive signals.
It is important to highlight that among these 181 signals, 64 were not included in the current prescribing information of durvalumab, such as pulmonary tuberculosis, cytokine release syndrome, radiation oesophagitis, oesophageal fistula, and oesophageal perforation. These findings are important as they contribute to a deeper understanding of the safety profile of durvalumab and identify previously unrecognized risks requiring requiring focused monitoring and further investigation.
We observed a significant association between durvalumab and overreporting of pulmonary tuberculosis (n = 10, ROR = 6.22; PRR = 6.21; χ²=43.49; IC025 = 1.20; EBGM05 = 3.32). No published clinical studies or observational studies have reported tuberculosis reactivation associated with durvalumab. However, However, several cases of tuberculosis reactivation linked to PD-1/PD-L1 inhibitors have been documented28,29. An 87-year-old Chinese patient receiving pembrolizumab (2 mg/kg) for recurrent Hodgkin’s lymphoma developed fever and weight loss after the fifth cycle. Mycobacterium tuberculosis was detected in sputum culture. Despite anti-TB treatment, pembrolizumab was discontinued due to persistent active tuberculosis (no prior immunosuppressive therapy)30. A Japanese patient with advanced NSCLC developed active pulmonary tuberculosis after eight cycles of nivolumab, despite no prior immunocompromised status31. Preclinical studies in TB-infected mice showed that PD-1-deficient mice had shorter survival than wild-type mice due to excessive inflammatory responses and extensive focal necrosis31. Severe immunoinflammatory damage may be the cause of death. Without PD-1 mediated inhibition, CD4 T cells do not control TB but promote TB development32,33. The reactivation mechanism remains unclear, but PD-1/PD-L1 blockade enhances inflammatory cytokine release (e.g., IFN-γ, TNF-α), which may disrupt extracellular matrix and facilitate M. tuberculosis growth34. These findings suggest durvalumab may increase tuberculosis risk. Clinicians should monitor for TB in patients receiving durvalumab, particularly those with positive interferon-gamma release assay (IGRA) results.
Another unexpected PT of durvalumab is CRS, (n = 54; ROR = 5.35; PRR = 5.33, χ2 = 189.22; IC025 = 1.91; EBGM05 = 4.06). CRS is an acute systemic inflammatory syndrome characterized by fever and multiple organ dysfunction. While most strongly associated with chimeric antigen receptor T (CAR-T) cell therapy, CRS may also occur with bispecific T cell engagers (BiTEs), immune checkpoint inhibitors (ICIs), other immunotherapies, or even severe infections35. Although CRS is rarely reported in durvalumab clinical trials, other ICIs have documented similar events. In a phase 3 trial comparing nivolumab-ipilimumab combination versus pembrolizumab (both with platinum-based chemotherapy) in untreated advanced NSCLC, CRS occurred in 5/148 patients (3.4%) in the nivolumab-ipilimumab arm36. A retrospective study by Tay et al. found 25 cases (4.6%) of ICI-induced CRS among 539 ICI-treated patients, involving pembrolizumab, nivolumab, and ipilimumab37. CRS manifestations range from mild symptoms to life-threatening or fatal outcomes38.By overstimulating the immune system to overcome the inhibitory signals of cancer cells, ICIs can result in both on-target autoimmune toxicity (when the targeted tumor antigen is on host non-cancer cells) and off-target cytokine-associated toxicity(CRS)39.Combined with the above evidence, durvalumab may be associated with an increased risk for CRS. Since CRS is characterized by various inflammatory symptoms and indicators, most of which are non-specific, diagnosing it can be challenging39.Therefore, clinicians should maintain high vigilance for CRS in patients receiving durvalumab, given its potential mortality risk.
Among the 64 unexpected PTs, we found PTs related to oesophageal toxicity, including radiation oesophagitis (n = 20; ROR = 145.09; PRR = 144.81, χ²=2514.24; IC025 = 3.51; EBGM05 = 79.94), oesophageal fistula (n = 4; ROR = 29.78; PRR = 29.77, χ²=108.20; IC025 = 0.82; EBGM05 = 10.73), and esophageal perforation (n = 4; ROR = 10.29; PRR = 10.28, χ²=33.20; IC025 = 0.54; EBGM05 = 3.81). Although reports of oesophageal toxicity associated with durvalumab are rare, similar adverse reactions have been documented in the literature for other ICIs. A retrospective study by Kavea Panneerselvam et al. analyzed patients who developed esophagitis after ICI treatment at The University of Texas MD Anderson Cancer Center between June 2011 and January 2020, excluding cases with other definitive etiologies. Among 657 consecutive patients undergoing esophagogastroduodenoscopy (EGD), 21 (3%) were identified as having ICI-associated esophagitis40. A case involved a 69-year-old patient with recurrent supraglottic laryngeal squamous cell carcinoma and lung metastases who developed dysphagia, grade 4 oropharyngeal mucositis, and esophagitis after 14 cycles of pembrolizumab, leading to treatment discontinuation41. Due to the low incidence of such events, their pathogenesis remains poorly understood. Among 28 reports of oesophageal toxicity, including 20 cases in lung cancer and 4 in esophageal squamous cell carcinoma, radiotherapy is commonly used to treat these cancers. However, thoracic or head-and-neck radiation itself increases oesophagitis risk. Given the uncertainty regarding prior radiotherapy exposure, the potential combined effect of durvalumab and radiation cannot be excluded. Physicians should closely monitor oesophageal toxicity risk when administering combination therapy.
The study demonstrated that 43.6% of AEs occurred during the first month of durvalumab treatment, highlighting the need for enhanced clinical monitoring during this period. Early detection and timely intervention are essential to mitigate potential harm. Notably, male patients and those aged ≥ 65 years showed a significantly higher risk of serious adverse events (SAEs). Given this elevated risk, proactive monitoring should be prioritized in these high-risk populations.
When conducting AE signal detection based on spontaneous reporting systems (SRS), the selection of a comparator is crucial. The principle of signal detection algorithms is primarily based on disproportionality analysis, which indicates that an AE signal is detected when the frequency of the target AE for the target drug exceeds that of the target AE for other drugs (background data) in the entire database, reaching a certain threshold. During the data analysis process, we initially selected AE reports of nine ICIs marketed in the United States from the FAERS database as the comparator. However, compared to using “all other drugs” as the comparator, this class-restricted approach faileded to detect signals of class-specific ADRs (e.g., hypothyroidism, hyperthyroidism, immune-mediated myocarditis, immune-mediated hepatitis, and thyroiditis) due to shared toxicity profiles among ICIs. To ensure the most comprehensive signal detection, we ultimately adopted “all other drugs” as the comparator.
This study has several limitations. First, disproportionality analyses detect drug-event reporting imbalances but cannot establish causality between durvalumab and AEs. Prospective controlled studies are needed to confirm findings. Second, the total number of durvalumab-treated patients is unknown, we were unable to calculate absolute incidence rates of AEs. Third, we analyzed 54 cases with cytokine release syndrome (CRS) as the primary term (PT), where combination therapy predominated: Durvalumab monotherapy (n = 2), Durvalumab + tremelimumab (n = 20), Durvalumab + tremelimumab + chemotherapy (n = 24), and Durvalumab combined with other symptomatic treatment drugs (n = 8). No CAR-T combination cases were reported. The influence of CAR-T cell therapy could be excluded, while the frequent combination of tremelimumab, chemotherapy, and symptomatic treatment drugs may introduce potential confounding effects on the attribution of CRS. Finally, of the 64 unexpected signals identified, only pulmonary tuberculosis, CRS, radiation esophagitis, esophageal fistula, and esophageal perforation underwent discussion. The remaining signals—including pleural effusion, respiratory failure, pneumothorax, cerebral infarction, biliary tract infection, cholecystitis, psoriasiform dermatitis, venous thrombosis of the limb, portal vein thrombosis, acute cholangitis and pericarditis malignant—represent clinically relevant safety concerns that warrant further investigation to elucidate their potential association with durvalumab.
Conclusion
This study comprehensively evaluated the safety profile of durvalumab using a large-scale real-world pharmacovigilance database. Through disproportionality analysis, 181 potential safety signals were identified, including 64 unexpected preferred terms (PTs) not documented in the prescribing information, such as cytokine release syndrome, pulmonary tuberculosis, radiation oesophagitis, and esophageal fistula. However, further clinical validation is required to confirm these findings. Continuous real-world monitoring of the safety profile of durvalumab remains essential.
Data availability
Publicly available datasets were analyzed in this study. All data come from the FAERS database, which is available at https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html.
Abbreviations
- FDA:
-
Food and drug administration
- FAERS:
-
Food and drug administration adverse event reporting system
- ICI:
-
Immune checkpoint inhibitor
- CRS:
-
Cytokine release syndrome
- PT:
-
Pulmonary tuberculosis
- AEs:
-
Adverse events
- PT:
-
Preferred terms
References
Kramer, R. et al. Hematological immune related adverse events after treatment with immune checkpoint inhibitors. Eur. J. Cancer. 147, 170–181. https://doi.org/10.1016/j.ejca.2021.01.013 (2021).
Zhao, Y. et al. Exploring the safety profile of Tremelimumab: an analysis of the FDA adverse event reporting system. Int. J. Clin. Pharm. 46 (2), 480–487. https://doi.org/10.1007/s11096-023-01678-7 (2024).
Bagchi, S., Yuan, R. & Engleman, E. G. Immune checkpoint inhibitors for the treatment of cancer: clinical impact and mechanisms of response and resistance. Annu. Rev. Pathol. 16, 223–249. https://doi.org/10.1146/annurev-pathol-042020-042741 (2021).
Stewart, R. et al. Identification and characterization of MEDI4736, an antagonistic Anti-PD-L1 monoclonal antibody. Cancer Immunol. Res. 3 (9), 1052–1062. https://doi.org/10.1158/2326-6066.CIR-14-0191 (2015).
Syed, Y. Y. & Durvalumab First global approval. Drugs 77 (12), 1369–1376. https://doi.org/10.1007/s40265-017-0782-5 (2017).
Murakami, S. Durvalumab for the treatment of non-small cell lung cancer. Expert Rev. Anticancer Ther. 19 (12), 1009–1016. https://doi.org/10.1080/14737140.2019.1699407 (2019).
Mathieu, L. et al. FDA approval summary: Atezolizumab and durvalumab in combination with Platinum-Based chemotherapy in extensive stage small cell lung Cancer. Oncologist 26 (5), 433–438. https://doi.org/10.1002/onco.13752 (2021).
Patel, T. H. et al. FDA approval summary: Tremelimumab in combination with durvalumab for the treatment of patients with unresectable hepatocellular carcinoma. Clin. Cancer Res. 30 (2), 269–273. https://doi.org/10.1158/1078-0432.CCR-23-2124 (2024).
Blondet, L. & Sarabi, M. [New drug approval: durvalumab in combinaison with cisplatin and gemcitabine in first-line in patient with advanced biliary tract cancer]. Bull. Cancer. 110 (7–8), 742–744. https://doi.org/10.1016/j.bulcan.2023.04.004 (2023).
Fung, S., Syed, Y. Y. & Durvalumab A review in advanced biliary tract Cancer. Target. Oncol. 18 (6), 965–972. https://doi.org/10.1007/s11523-023-01007-y (2023).
Antonia, S. J. et al. Clinical activity, tolerability, and Long-Term Follow-Up of durvalumab in patients with advanced NSCLC. J. Thorac. Oncol. 14 (10), 1794–1806. https://doi.org/10.1016/j.jtho.2019.06.010 (2019).
Antonia, S. J. et al. Durvalumab after chemoradiotherapy in stage III Non-Small-Cell lung Cancer. N Engl. J. Med. 377 (20), 1919–1929. https://doi.org/10.1056/NEJMoa1709937 (2017).
Garassino, M. C. et al. Durvalumab as third-line or later treatment for advanced non-small-cell lung cancer (ATLANTIC): an open-label, single-arm, phase 2 study. Lancet Oncol. 19 (4), 521–536. https://doi.org/10.1016/S1470-2045(18)30144-X (2018).
Goldman, J. W. et al. Durvalumab, with or without Tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 22 (1), 51–65. https://doi.org/10.1016/S1470-2045(20)30539-8 (2021).
Johnson, M. L. et al. Durvalumab with or without Tremelimumab in combination with chemotherapy as First-Line therapy for metastatic Non-Small-Cell lung cancer: the phase III POSEIDON study. J. Clin. Oncol. 41 (6), 1213–1227. https://doi.org/10.1200/JCO.22.00975 (2023).
Burris, H. A. 3 et al. Durvalumab plus gemcitabine and cisplatin in advanced biliary tract cancer (TOPAZ-1): patient-reported outcomes from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 25 (5), 626–635. https://doi.org/10.1016/S1470-2045(24)00082-2 (2024).
Herbst, R. S. et al. An Open-Label, phase II, multidrug platform study of durvalumab alone or in combination with oleclumab or Monalizumab in patients with unresectable, stage III Non-Small-Cell lung Cancer. J. Clin. Oncol. 40 (29), 3383–3393. https://doi.org/10.1200/JCO.22.00227 (2022).
Sangro, B. et al. Four-year overall survival update from the phase III HIMALAYA study of Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. Ann. Oncol. 35 (5), 448–457. https://doi.org/10.1016/j.annonc.2024.02.005 (2024).
Shu, Y. et al. Hematological toxicities in PARP inhibitors: A real-world study using FDA adverse event reporting system (FAERS) database. Cancer Med. 12 (3), 3365–3375. https://doi.org/10.1002/cam4.5062 (2023).
van Puijenbroek, E. P. et al. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol Drug Saf. 11 (1), 3–10. https://doi.org/10.1002/pds.668 (2002).
Evans, S. J., Waller, P. C. & Davis, S. Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol Drug Saf. 10 (6), 483–486. https://doi.org/10.1002/pds.677 (2001).
Bate, A. et al. A bayesian neural network method for adverse drug reaction signal generation. Eur. J. Clin. Pharmacol. 54 (4), 315–321. https://doi.org/10.1007/s002280050466 (1998).
Szarfman, A., Machado, S. G. & O’Neill, R. T. Use of screening algorithms and computer systems to efficiently signal higher-than-expected combinations of drugs and events in the US FDA’s spontaneous reports database. Drug Saf. 25 (6), 381–392. https://doi.org/10.2165/00002018-200225060-00001 (2002).
Shu, Y., Chen, J., Ding, Y. & Zhang, Q. Adverse events with Risankizumab in the real world: postmarketing pharmacovigilance assessment of the FDA adverse event reporting system. Front. Immunol. 14, 1169735. https://doi.org/10.3389/fimmu.2023.1169735 (2023).
Zhang, Y. et al. Efficacy and safety of consolidation durvalumab after chemoradiation therapy for stage III non-small-cell lung cancer: a systematic review, meta-analysis, and meta-regression of real-world studies. Front. Pharmacol. 14, 1103927. https://doi.org/10.3389/fphar.2023.1103927 (2023).
Yang, H. et al. Safety and efficacy of durvalumab (MEDI4736) in various solid tumors. Drug Des. Devel Ther. 12, 2085–2096. https://doi.org/10.2147/DDDT.S162214 (2018).
Li, D. H. & Xiong, X. Z. Immune checkpoint Inhibitor-Associated systemic sclerosis in the treatment of a small cell lung Cancer patient with durvalumab: A case report. Clin. Cosmet. Investig Dermatol. 17, 663–669. https://doi.org/10.2147/CCID.S451386 (2024).
He, W. et al. Activated pulmonary tuberculosis in a patient with melanoma during PD-1 Inhibition: a case report. Onco Targets Ther. 11, 7423–7427. https://doi.org/10.2147/OTT.S178246 (2018).
Hirano, S. et al. A case of pulmonary tuberculosis that developed during nivolumab and ipilimumab treatment for pulmonary adenocarcinoma that recurred two months after completion of anti-tuberculous treatment. Chin. Clin. Oncol. 13 (3), 43. https://doi.org/10.21037/cco-23-153 (2024).
Lee, J. J., Chan, A. & Tang, T. Tuberculosis reactivation in a patient receiving anti-programmed death-1 (PD-1) inhibitor for relapsed Hodgkin’s lymphoma. Acta Oncol. 55 (4), 519–520. https://doi.org/10.3109/0284186X.2015.1125017 (2016).
Fujita, K., Terashima, T. & Mio, T. Anti-PD1 antibody treatment and the development of acute pulmonary tuberculosis. J. Thorac. Oncol. 11 (12), 2238–2240. https://doi.org/10.1016/j.jtho.2016.07.006 (2016).
Barber, D. L., Mayer-Barber, K. D., Feng, C. G., Sharpe, A. H. & Sher, A. CD4 T cells promote rather than control tuberculosis in the absence of PD-1-mediated Inhibition. J. Immunol. 186 (3), 1598–1607. https://doi.org/10.4049/jimmunol.1003304 (2011).
Sakai, S. et al. CD4 T Cell-Derived IFN-gamma plays a minimal role in control of pulmonary Mycobacterium tuberculosis infection and must be actively repressed by PD-1 to prevent lethal disease. PLoS Pathog. 12 (5), e1005667. https://doi.org/10.1371/journal.ppat.1005667 (2016).
Tezera, L. B. et al. Anti-PD-1 immunotherapy leads to tuberculosis reactivation via dysregulation of TNF-alpha. Elife 9. https://doi.org/10.7554/eLife.52668 (2020).
Shimabukuro-Vornhagen, A. et al. Cytokine release syndrome. J. Immunother Cancer. 6 (1), 56. https://doi.org/10.1186/s40425-018-0343-9 (2018).
Shiraishi, Y. et al. Five cases of cytokine release syndrome in patients receiving cytotoxic chemotherapy together with nivolumab plus Ipilimumab: A case report. J. Thorac. Oncol. 19 (2), 337–343. https://doi.org/10.1016/j.jtho.2023.10.010 (2024).
Tay, S. H. et al. Cytokine release syndrome in Cancer patients receiving immune checkpoint inhibitors: A case series of 25 patients and review of the literature. Front. Immunol. 13, 807050. https://doi.org/10.3389/fimmu.2022.807050 (2022).
Lee, D. W. et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood 124 (2), 188–195. https://doi.org/10.1182/blood-2014-05-552729 (2014).
Ceschi, A., Noseda, R., Palin, K. & Verhamme, K. Immune checkpoint Inhibitor-Related cytokine release syndrome: analysis of WHO global pharmacovigilance database. Front. Pharmacol. 11, 557. https://doi.org/10.3389/fphar.2020.00557 (2020).
Panneerselvam, K. et al. Clinicopathologic features, treatment response, and outcomes of immune checkpoint Inhibitor-Related esophagitis. J. Natl. Compr. Canc Netw. 19 (8), 896–904. https://doi.org/10.6004/jnccn.2020.7675 (2021).
Acero Brand, F. Z. et al. Severe immune mucositis and esophagitis in metastatic squamous carcinoma of the larynx associated with pembrolizumab. J. Immunother Cancer. 6 (1), 22. https://doi.org/10.1186/s40425-018-0332-z (2018).
Acknowledgements
The authors would like to thank The Third Affiliated Hospital of Guangxi Medical University.
Funding
This study was a self-funded research project of the Health Commission of Guangxi Zhuang Autonomous Region [Z-A20241032], chaired by An-Ju Tan.
Author information
Authors and Affiliations
Contributions
Author contributionsAn-Ju Tan, Wan-Ying Liu, and Dun-Chang Mo conceptualized this article and decided on the content. An-Ju Tan, Wan-Ying Liu, Dun-Chang Mo, and Jun-Li Lu analyzed the data. An-Ju Tan, Wan-Ying Liu, and Dun-Chang Mo wrote the manuscript, and Qing-Ying Tan and Yu-Yan prepared the figures and form. An-Ju Tan, Wan-Ying Liu, and Dun-Chang Mo revised this article. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Ethical approval was not required for this study because it used the FAERS database, which is a free open-access database.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tan, AJ., Liu, WY., Lu, JL. et al. A pharmacovigilance analysis of post-marketing safety of durvalumab. Sci Rep 15, 16661 (2025). https://doi.org/10.1038/s41598-025-01583-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01583-1
