
Abstract
The rising prevalence of histidine-rich protein 2 (PfHRP2) gene deletions (pfhrp2-) poses a threat to the accuracy of PfHRP2-based rapid diagnostic tests (RDTs). However, evidence of this deletion is scarce in Indonesia. We examined the prevalence of pfhrp2 and its paralogue histidine-rich protein 3 (PfHRP3) gene deletions (pfhrp3-) in blood samples collected from a study assessing three PfHRP2-based RDTs conducted between December 2022 and April 2023 in Timika, Papua. Out of 2157 symptomatic-patients enrolled, 566 P. falciparum mono-infection cases were included for pfhrp2/3 exon 2 genotyping. We detected nine samples (1.59%, 95% CI 0.73–3.00%) with pfhrp2-/pfhrp3-, of which eight were PfHRP2-RDTs positive. Of three pfhrp2- samples (0.53%, 95% CI 0.11–1.54%), one was PfHRP2-RDTs positive. In contrast, 201 samples (35.51%, 95% CI 31.57–39.61%) had pfhrp3-, five of which were pfhrp2 + but PfHRP2-RDT negative; however, four exhibited low parasitemia. Five PfHRP2-RDTs negative samples with pfhrp2 + /pfhrp3 + were sequenced alongside two pfhrp2 + with PfHRP2-RDTs positive samples. We found more repeat-type variations in pfhrp2 compared to pfhrp3. Seven unique repeat types in pfhrp2 and one unique repeat type in pfhrp3 amino acid sequences were characterized in single or multiple copies per sample. These results demonstrated the low prevalence of pfhrp2- 2.12% (95% CI 1.10–3.67%) suggesting PfHRP2-based RDTs remain suitable for malaria diagnosis in Timika, Papua, Indonesia.
Similar content being viewed by others
Introduction
Malaria remains a major public health burden in tropical countries, specifically in Indonesia. The Indonesian government targets national malaria elimination in 2030, and in 2017, 72% of the population lived in malaria-free zones. This achievement is possible due to the implementation of artemisinin combination therapy after the discovery of chloroquine resistance1,2,3, malaria screening in high transmission areas, development of rapid response protocol to suppress transmission foci and implementation of evidence-based policy across all sectors of the government4. All of these efforts lead to a reduction of the national annual parasite index (API) towards 0.9 cases per 1000 population5. However, malaria cases have plateaued since 20144. In the eastern part of Indonesia, particularly Papua, contributes to nearly 92% of the national malaria cases, with heterogeneous distribution of malaria transmission across different regions, requiring tailored malaria elimination effort6. One of the districts in Papua, Mimika, had increasing malaria cases annually with the second-highest API reaching 440.65 cases per 1000 individuals at risk as reported in the National Malaria Surveillance System (www.sismal.malaria.id). To intensify malaria elimination efforts in Mimika, a malaria diagnostic strategy needs to be prioritized in the high endemicity setting, such as increasing the deployment of RDTs to complement microscopy.
Microscopy and RDTs have been widely used as malaria diagnostic tools in Indonesia, following the WHO guidelines7. Initially, microscopy was the gold standard for detecting malaria parasites and their species. However, malaria microscopy has highlighted challenges: it is time-consuming and requires skilled expertise to identify Plasmodium parasites and their species4. Hence, RDTs have been utilized across Indonesia as an alternative diagnostic tool since 20108. The ease-of-use and simple result interpretations further improved feasibility and accessibility of RDT, unlike microscopy. Previous studies assessing RDTs performance to detect P. falciparum in Papua has shown a similar sensitivity and specificity compared to the microscopy and qPCR9,10, indicating that RDTs can be reliably used as an alternative diagnostic tool. Since malaria incidence in Papua has been rising since 2015 up to 2020, with P. falciparum becoming dominant in 2019 cases6, development of novel RDTs is urgent to detect any missed P. falciparum infections due to the absence of certain antigens used in previously available RDT.
Over the past decades, RDTs have been continuously developed and evaluated to improve their specificity and sensitivity. The main antigen targets in RDTs are Plasmodium lactate dehydrogenase (pLDH), which captures pLDH produced by the four common human Plasmodium and P. falciparum histidine-rich protein 2 (PfHRP2) which specifically detect P. falciparum parasite11. However, both types of RDTs have limitations. pLDH-detecting RDTs is relatively low sensitive12,13 and heat-unstable14. Moreover, PfHRP2-based RDTs can detect the presence of PfHRP2 in patient blood after treatment for several weeks15,16,17 which can potentially elevate false positives. A homologous protein of PfHRP2, called PfHRP3, is also circulating in P. falciparum-infected patients and share similar epitopes that can be detected by PfHRP2-based RDTs. In recent times, many combo RDTs combined antibodies against pLDH and PfHRP2 in a single cassette to distinguish between P. falciparum and non-falciparum infection.
Despite their utility and improvement, increasing reports of pfhrp2/3 gene deletions threaten the use of PfHRP2-based RDTs. A high prevalence of pfhrp2 gene deletion has been reported in many countries in Latin America and Horn of Africa, such as Peru18, Eritrea19,20, and Djibouti21 causing high levels of false negative RDT results. Several countries in Asia have also reported circulation of these gene deletions, which include India, Cambodia and Myanmar measured at up to 25%, 2.4% and 9.4%, respectively22,23,24. In response to the threat, WHO has recommended that countries assess the prevalence of pfhrp2/3 deleted parasites causing false negative RDT results, and switch away from HRP2-based RDTs when the prevalence reaches a threshold ≥ 5%11. For example, countries with high prevalence of pfhrp2/3 gene deletions have been suggested to use alternative non-HRP2-based RDT, such as pLDH or aldolase-based18,19,21.
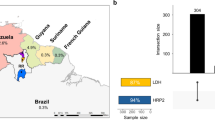
In Indonesia, there is a paucity of information regarding the surveillance of these mutant parasites. Only one study conducted by the MalariaGEN Pf project included Indonesian isolates and found 4% of pfhrp2 gene deletion25. While the study demonstrated the presence of gene-deleted parasites in Indonesia, their impact on RDT results was not examined. The relatively small sample size does not allow accurate assessment of the prevalence of gene deleted parasites and does not meet the minimal sample size requirement indicated by WHO26. In addition, those samples were collected seven years ago and did not reflect the situations at the time of the study. In 2021, the Ministry of Health of The Republic of Indonesia has included pfhrp2/3 surveillance as one of the priorities in malaria research to accelerate the elimination, especially in high-endemic settings4. Therefore, we aimed to contribute to this surveillance to determine the updated proportion of pfhrp2/3 gene deletions circulating in Timika, Mimika District, Papua Province alongside their genetic diversity.
Methods
Study design
Detection of pfhrp2/3 gene deletion was part of a cross-sectional study conducted over four months to assess RDTs performance in collaboration with the Foundation for Innovative New Diagnostics (FIND), Geneva. The study was conducted in Timika, Papua where three health facilities with the highest malaria incidences were selected as the enrollment sites. Patients seeking treatment for suspected-malaria symptoms were asked for their consent prior to the blood collection. The sample size was calculated from a larger study (not published) in collaboration with FIND, based on the requirement of the “Technical Specifications Series for submission to WHO Prequalification – Diagnostic Assessment TSS-3” document27. In 2021, the estimated malaria prevalence in Timika was 25%, therefore the sample size was targeted to include a minimum of 2180 participants.
Patient enrollment and sample collection
Any patient aged 5 years or older who presented at a study-selected health facility with a fever (infrared forehead temperature of ≥ 37.5 °C) or a history of fever within the last 48 h was eligible to participate in this study. Patients who showed symptoms of severe malaria and/or central nervous system illness were excluded. For biological sample collection, a 3 mL venous blood was drawn from each participant via syringe for malaria RDTs testing, sub-microscopic speciation by real-time PCR based on Mangold et al.28, and pfhrp2/3 genotyping. Additionally, finger prick blood samples were collected for microscopy examination.
Identification of malaria cases
A 5 μl aliquot of venous blood was used to detect malaria infection by RDT. In total, three commercial RDTs were evaluated: two PfHRP2-based RDTs (SD Bioline™ Malaria Ag Pf, #05FK50 and SD Bioline™ Malaria Ag Pf/Pv, #05FK80) and one PfHRP2/Pf pLDH/Pv pLDH-based RDT combining detection of P. falciparum and P. vivax infection in a single cassette test (SD Bioline™ Malaria Ag Pf/Pf/Pv, #05FK120). All RDTs were provided by FIND, Geneva, Switzerland and manufactured by Abbott Diagnostics Korea Inc.
As the national gold standard, blood smear was prepared using Giemsa staining and examined by a certified microscopist at the study site who was blinded to the RDT results. Also, a second reading was done by an expert microscopist who was blinded to the first reader and RDT results. Parasite identification and parasitemia were determined by microscopy using the Obare Method Calculator, developed by the Worldwide Antimalarial Resistance Network (WWARN), to assess the result agreement between readers29. Discrepancies between the two readers were resolved by a third reader to obtain the final species and parasitemia. For simplicity, parasitemia was classified as low parasitemia (< 100 parasites/µL), medium parasitemia (100–1000 parasites/µL), and high parasitemia (> 1000 parasites/µL).
Molecular approaches were performed to validate the microscopy result. The genomic DNA (gDNA) was extracted from 200μL of whole blood by QIAGEN QIAamp DNA Blood Mini Kit and eluted at 150 μl. Identification of the malaria cases was determined by real-time PCR using BRYT Green® Dye with cycling conditions as published previously28. Malaria-negative sample was defined by a cycling threshold (Ct) above 33. Meanwhile, the Plasmodium species from positive samples were determined by comparing their melt temperature against the positive controls. Any disagreement results between microscopic and real-time PCR were re-evaluated by conventional PCR30.
pfhrp2/3 genotyping and sequencing
Only mono-infection cases of P. falciparum confirmed by both microscopic and molecular tests were selected to examine the pfhrp2/3 gene deletion. A confirmatory PCR step by single copy genes, including glutamate-rich protein (glurp) and erythrocyte binding antigen 175 region IV (eba175-RIV), was performed to assess the DNA quality of the samples. A nested PCR of glurp gene was conducted as instructed by Brockman et al.31, whereas single-step PCR was done for eba175-RIV gene. The primer set of eba175-RIV was designed in-house with 5ʹ-CAT GAA GAG GTG AAA GAA CAT AC-3ʹ as forward sequence (EBA175-R4-F) and 5ʹ-CTT CAT CCA AGC TAC TAG AAG G-3ʹ as reverse sequence (EBA175-R4-R). A total volume of 25 μl for eba175-RIV PCR reaction was mixed, consisting of 1X PCR Buffer, 2.5 mM MgCl2, 0.1 mM dNTPs Mix, 2.4 μM Primer set, and 0.75 U DNA Taq Polymerase. The cycling condition of eba175-RIV was performed as follows: Pre-Denaturation at 94 °C for 10 min; Denaturation/Annealing/Extension at 94 °C/55 °C/70 °C for 50 secs/50 secs/1 min (30 cycles); and Holding step at 15 °C.
Successful amplification of the samples for both single-copy genes were further analyzed for pfhrp2/3 genotyping. For this study, exon 2 region of pfhrp2/3 genes was investigated by conventional PCR as described elsewhere32, with modification on performing only the second-nest PCR. The prevalence of pfhrp2/3 gene deletion was calculated and categorized into 4 outcomes, including single deletion of pfhrp2 (pfhrp2-/pfhrp3 +) and pfhrp3 (pfhrp2 + /pfhrp3-), double deletion (pfhrp2-/pfhrp3-), and no deletion (pfhrp2 + /pfhrp3 +).
Sanger sequencing was conducted on pfhrp2 + or pfhrp3 + samples with medium/high parasitemia, but negative by PfHRP2-RDTs. The hrp2/3 sequence from these samples were then compared to PfHRP2-RDTs positive samples and samples from other studies in order to investigate possible novel repeat sequences that might cause the false negative results. Samples were defined as PfHRP2-RDTs negative if all three PfHRP2-RDTs tested negative. Sequences from the pfhrp2/3 positive but PfHRP2-RDTs negative samples were aligned against pfhrp2/3 + and PfHRP2-RDT positive samples by the MUSCLE 5.1 alignment software and their repeat-type variations assessed according to previous publications32,33.
Results
Demography and baseline data
Between December 2022 and April 2023, a total of 2184 individuals were enrolled. Patient numbers varied across the three health facilities, with the highest number of samples collected from Wania (n = 889) followed by Timika (n = 804) and Timika Jaya (n = 491). The majority of P. falciparum mono-infection samples (78.69%) were derived from the adult participant group (19–59 years old; Table 1). The median age amongst participants was 29 years with 57% males and 43% females. Out of 582 P. falciparum mono infection cases, 389 (66.83%) samples had high parasitemia by microscopy (Table 1), while the median parasitemia was 2836 parasites/µL (IQR at 450.5–22,500 parasites/µL).
P. falciparum mono-infection cases
A total of 2157 blood samples were collected. A total of 615 participants (28.51%) had P. falciparum mono-infection detected by microscopy. Prior to pfhrp2/3 genotyping, a real-time PCR was performed to confirm the Plasmodium species. The final number of P. falciparum mono-infections was 582 samples (26.98%) in agreement between microscopy and real-time PCR results (Fig. 1).

A flow diagram showing the number of samples collected and included in pfhrp2/3 genotyping. Amplification of single copy genes was conducted after species identification for quality control, reducing the sample size to be pfhrp2/3 genotyped at 566 samples. The bottom level of the flowchart outlines the prevalence of pfhrp2/3 gene deletion.
pfhrp2/3 genotyping
Amplification of single-copy genes (i.e. glurp and eba175-RIV) was performed in 582 samples. Sixteen samples (2.75%) that failed to amplify either one or both single-copy genes, which indicate degraded DNA quality. Thus, a total of 566 samples (97.25%) were selected for amplification of exon 2 regions of pfhrp2/3 genes (Figs. 1 and 2).

The arrangement of repeat-type variations of pfhrp2/3 sequences found in all samples; (a) pfhrp2 sequence and (b) pfhrp3 sequence. Sample ID 2016 and 2014 were tested positive by PfHRP2-based RDTs (showed in italic font) whereas others were negative. The color-coded number illustrates the repeat sequence as described in Table S1, according to previous publications32,33. 3D7 acted as reference sequence in both pfhrp2 (NCBI Accession Number: NC_004329) and pfhrp3 (NCBI Accession Number: XM_002809080). Some repeat-types highlighted in yellow were a unique repeat that were not reported yet in other publications (see Table S2). However, the unique type 6 repeat found in sample 2016, 3063, and 2377 were reported previously34,35 (see Table S2).
The prevalence of the pfhrp2/3 gene deletion identified in this study varied. Overall, pfhrp2 deletion was observed at 2.12% (95% CI 1.1–3.67%), whereas pfhrp3 deleted samples were 37.1% (95% CI 33.11–41.23%). The distribution of pfhrp2/3 gene deletion was also illustrated (using ggplot2 3.5.1) according to their parasite density and PfHRP2-RDTs results in Fig. 3. Only three samples were found to have single pfhrp2 gene deletion (0.53%, 95% CI 0.11–1.54%), with one PfHRP2-RDTs positive. In contrast, a high prevalence of pfhrp2 + /pfhrp3- was observed in 201 samples (35.51%, 95% CI 31.57–39.61%). Among single pfhrp3 gene deletion cases, five samples were PfHRP2-RDTs negative, with four having low parasitemia (Fig. 3). Lastly, a low proportion of pfhrp2-/pfhrp3- were detected in nine samples (1.59%, 95% CI 0.73–3%), with eight having positive PfHRP2-RDTs results (Fig. 3).

Parasite density of various pfhrp2/3 gene deletion status (n = 566) with blue and red representing positive and negative PfHRP2-RDTs status, respectively. Thresholds for low, medium, and high parasitemia are < 100 parasites/µL, 100–1000 parasites/µL, and > 1000 parasites/µL, respectively.
We also investigated the parasite density of samples in regards to pfhrp2/3 deletion status and PfHRP2-RDTs result. On samples with non-deleted pfhrp2/3, the median [IQR] parasitemia was 80 [52–102] and 4784 [1144–26,875] parasites/μL with PfHRP2-RDTs negative and positive results, respectively. While on samples with deleted pfhrp2/3, the median [IQR] parasitemia was 32 [28–76] and 2808 [680–27,500] parasites/μL with PfHRP2-RDTs negative and positive results, respectively.
pfhrp2/3 repeat-sequence variations
We further investigated high-parasitemia samples with no pfhrp2/3 deletion but PfHRP2-RDTs negative by Sanger sequencing to confirm the presence and structure of these genes. We sequenced seven pfhrp2 positive samples, five of which were PfHRP2-RDTs negative, and four pfhrp3 positive samples, three of which were PfHRP2-RDTs negative.
The arrangement of repeats in pfhrp2/3 sequences for each sample is illustrated in Fig. 2. The length of the exon 2 region in pfhrp2 sequences ranged from 689 to 824 base pairs, whereas the length of the exon 2 region in pfhrp3 sequences ranged from 471 to 501 base pairs. The repeat-type sequences in pfhrp2 varied across the samples (Fig. 2a), yet similar arrangements were found in pfhrp3 (Fig. 2b). The majority of the samples in pfhrp2 and pfhrp3 shared the same repeat-type code as reported elsewhere32,33 (Table S1). However, unique repeat-type variants were also observed in some samples (highlighted in yellow in Fig. 2). Some of these unique types, including repeat types 6 and 7 (Table S2), have been observed in previous publications34,35.
Discussion
As a response to the emergence of pfhrp2/3 gene deletion reports, WHO has announced a standardized protocol for detecting the prevalence of pfhrp2 deletion. A threshold of 5% of false negative PfHRP2-based RDT results caused by gene deletions has been recommended as a trigger to change the malaria diagnostic strategy away from PfHRP2-based RDT11,26. For instance, a high proportion of pfhrp2 deletion in Peru, Eritrea and Djibouti have led these countries to switch to non-PfHRP2-based RDTs18,19,20,21. This highlights the importance of identifying the prevalence of pfhrp2/3 gene deletion to inform country malaria diagnosis policy.
In our study, we identified 615 P. falciparum mono-infection cases by microscopy. Further confirmation by PCR was performed to verify the species and ensure the DNA quality within the samples (i.e. any fragmented or degraded gDNA might negatively affect the pfhrp2/3 deletion results)36,37. After excluding samples that failed to amplify two single-copy genes, a total of 566 samples were selected for pfhrp2/3 genotyping.
We identified different proportions of pfhrp2/3 gene deletion across the population. In this study, pfhrp2 deletions were found at 2.12% (95% CI 1.1–3.67%), while a previous report from the MalariaGEN Pf project reported a deletion of 3.75% (95% CI 0.78–10.57%)38. This might be due to the higher sample size that we assessed, different sampling methods, or laboratory assays used to determine the pfhrp2 gene deletion39. Three of these pfhrp2 deleted samples tested negative in all three RDTs, with one of them having a parasitemia above 100 parasites/µL, indicating that the pfhrp2 gene deletion might be responsible for this false negative result21,40. Alternatively, this might be due to the lower sensitivity of the RDTs in detecting low level of parasitemia. In contrast, a high proportion of pfhrp3 deletions were observed in 210 out of 566 samples (37.1%, 95% CI 33.11–41.23%), higher than the 25% (95% CI 15.99–35.94%) pfhrp3 deletion prevalence reported by the MalariaGEN study in Indonesian isolates38. Similarly, this pattern, where the pfhrp3 deletion is higher than pfhrp2 deletion, was detected in several countries, including Northeast Tanzania and Peru18,41. Of the single pfhrp3- samples, only 5/201 (2.48%) samples were negative by RDTs. These samples had low parasitemia (< 100 parasites/µL by microscopy); hence, these false negative results are caused by low parasite densities42,43. However, this pattern of higher hrp3 deletion prevalence compared to hrp2 in different countries warrants a further investigation into the impact of hrp3 deletion towards the malaria elimination effort. Finally, pfhrp2/3 double deletion was detected at 9/566 (1.59%, 95% CI 0.72–3.00%) samples, compared to no identified double deletion in the MalariaGEN Pf study38. Nevertheless, 8/9 (88%) double-deleted samples tested positive by RDTs, suggesting that either a recent infection with pfhrp2 + parasite or multiple infections might explain this incidence44. However, we found that all of these patients have not had recent infections diagnosed over the past year according to the clinical records, indicating that this hypothesis is less likely, although they may have had asymptomatic infections in the recent past. Quantifying PfHRP2 in these samples can inform on the possibility of unreported P. falciparum infections that left traces of the antigen, and it can enable the assessment of the RDTs performance by comparing the antigen levels to samples with concordant results. Future studies can probe further into the relatedness of these parasites using identity-by-descent (IBD) methods, which might reveal P. falciparum populations that carry certain hrp2/3 deletion characteristics. However, this requires selection of appropriate markers to avoid introducing bias to the IBD estimates45.
To investigate possible causes of false negative RDT results for several samples with medium/high parasite densities, we assessed the repeat-type variations across the pfhrp2/3 exon 2 region with medium/high parasitemia samples (> 150 parasites/µL) that were undetected by PfHRP2-based RDTs. Of the five pfhrp2/3 samples sequenced, only one sample had a parasitemia below 250 parasites/µL. pfhrp2 exhibited greater sequence diversity compared to pfhrp3, consistent with global isolates44. We observed that all the samples contained type 2 and 7 repeats in their sequences. These two repeats have been reported to play a key role in RDT positivity32. However, the results show clearly that the cause of false negative PfHRP2-based RDTs results in these samples were not due to pfhrp2 variations. Some studies have shown that the diversity of pfhrp2/3 may not contribute to false negative results44,46. Additional genotyping of the hrp2/3 flanking genes might add more information in the characterization of the deletions found in this study. Another possibility that can cause false negative RDT results might be explained by poor quality or degradation of RDTs due to poor transport and storage conditions and anomalies (such as red background). However, we did not find such discrepancies within these samples. There might be a possibility that non-deleted and deleted parasites co-exist within individuals, where a lower number of non-deleted parasites were detected by PCR since it has a higher sensitivity compared to RDT. Using more sensitive deletion detection methods such as digital droplet PCR47,48 can confirm the pfhrp2/3 deletion status on suspected multiple clone cases.
We also investigated the relationship between parasitemia, pfhrp2/3 deletion, and PfHRP2-RDTs results by comparing the median parasitemia between the different pfhrp2/3 deletion and PfHRP2-RDTs result combination. We found that the median parasitemia for negative PfHRP2-RDTs results was 32 and 80 parasites/µL for non-deleted and deleted pfhrp2/3 samples, respectively. This might suggest that negative PfHRP2-RDT results are more likely to be caused by lower sensitivity of RDTs to low parasitemia samples in this study. When looking at samples with positive PfHRP2-RDT results, the median parasitemia was 2808 and 4784 parasites/µL for non-deleted and deleted pfhrp2/3 samples, respectively. We suspect that pfhrp2/3 deleted samples with higher parasitemia accommodate for the loss of either pfhrp2 or pfhrp3 by having a high enough antigen level to be detected by PfHRP2-RDTs. Future studies might assess the association between PfHRP2-RDT results, parasitemia, and pfhrp2/3 deletion by sampling from areas with a high pfhrp2/3 deletion prevalence setting, enabling high-precision estimates on the impact of pfhrp2/3 deletion.
During this study, some limitations were encountered. First, the PfHRP2-based RDTs that we used were not the RDTs used in the National Malaria Control Program. In addition, this study was originally designed to evaluate RDTs performance, where sampling was conducted in three sites instead of the minimum of ten health facilities according to the WHO guideline for hrp2/3 deletion. Future studies should also increase the range of sample sites to better represent the deletion prevalence in Papua province. Lastly, we did not perform any immunoassays to detect and quantify the PfHRP2/3 antigen circulating within the samples, unlike other studies22,39,49. This data may have been beneficial in selecting the samples for pfhrp2/3 according to the presence of PfHRP2/3 antigens, as applied by some studies39,49,50.
Conclusion
This is the first pfhrp2/3 genotyping study to assess PfHRP2-based RDT performance in Indonesia, providing the current pfhrp2/3 deletion prevalence in a high transmission setting, Timika, Papua. A low proportion of pfhrp2 deletion was observed in this symptomatic population. However, some of the RDT readings were not affected by the deletion of pfhrp2 exon 2, leading to cases of pfhrp2 cryptic absence. This indicates that the PfHRP2-based RDTs tested in this study remain suitable since the false negative RDT rate due to pfhrp2/3 deletion is below the WHO threshold for changing the diagnostic strategy (≥ 5%). Overall, the prevalence of single and double pfhrp2/3 deletions in this study highlights the importance and urgency to conduct further surveillance following the WHO survey protocol in order to cover hrp2/3 deletion prevalence in other regions in Indonesia, especially the Papua province. This also allows monitoring of the performance of PfHRP2-based RDTs used in Indonesia, providing further information on whether the current national RDT used remain reliable. These outcomes will inform the NMCP on hrp2/3 deletion prevalence in Indonesia, and guide the continuing development of the national malaria diagnostic policy.
Data availability
The data sets used during this study are available upon reasonable request to the corresponding author.
References
Poespoprodjo, J. R. et al. Therapeutic response to dihydroartemisinin–piperaquine for P. falciparum and P. vivax nine years after its introduction in Southern Papua, Indonesia. Am. J. Trop. Med. Hyg. 98, 677–682 (2018).
Pava, Z. et al. Molecular surveillance over 14 years confirms reduction of Plasmodium vivax and falciparum transmission after implementation of Artemisinin-based combination therapy in Papua, Indonesia. PLoS Negl. Trop. Dis. 14, e0008295 (2020).
Marfurt, J. et al. Longitudinal ex vivo and molecular trends of chloroquine and piperaquine activity against Plasmodium falciparum and P. vivax before and after introduction of artemisinin-based combination therapy in Papua, Indonesia. Int. J. Parasitol. Drugs Drug Resist. 17, 46–56 (2021).
Directorate General of Disease Prevention and Control, Ministry of Health of The Republic of Indonesia. National Action Plan for Acceleration of Malaria Elimination 2020–2026 (Revision). (2023).
Sitohang, V. et al. Malaria elimination in Indonesia: Halfway there. Lancet Glob. Health 6, e604–e606 (2018).
Fadilah, I. et al. Quantifying spatial heterogeneity of malaria in the endemic Papua region of Indonesia: Analysis of epidemiological surveillance data. Lancet Reg. Health Southeast Asia 5, 100051 (2022).
World Health Organization. WHO guidelines for malaria. (2023).
Ahmed, R. et al. Performance of four HRP-2/pLDH combination rapid diagnostic tests and field microscopy as screening tests for malaria in pregnancy in Indonesia: A cross-sectional study. Malar. J. 14, 420 (2015).
Unwin, V. T. et al. Use of a highly-sensitive rapid diagnostic test to screen for malaria in pregnancy in Indonesia. Malar. J. 19, 28 (2020).
Fransisca, L. et al. Comparison of rapid diagnostic test Plasmotec Malaria-3, microscopy, and quantitative real-time PCR for diagnoses of Plasmodium falciparum and Plasmodium vivax infections in Mimika Regency, Papua, Indonesia. Malar. J. 14, 103 (2015).
World Health Organization. Response Plan to Pfhrp2 Gene Deletions (World Health Organization, 2019).
Opoku Afriyie, S. et al. Accuracy of diagnosis among clinical malaria patients: Comparing microscopy, RDT and a highly sensitive quantitative PCR looking at the implications for submicroscopic infections. Malar. J. 22, 76 (2023).
Ranadive, N. et al. Limitations of rapid diagnostic testing in patients with suspected malaria: A diagnostic accuracy evaluation from Swaziland, a low-endemicity Country aiming for malaria elimination. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 64, 1221 (2017).
The Use of Malaria Rapid Diagnostic Test. (WHO, Geneva, 2004).
Iqbal, J., Siddique, A., Jameel, M. & Hira, P. R. Persistent histidine-rich protein 2, parasite lactate dehydrogenase, and panmalarial antigen reactivity after clearance of Plasmodium falciparum monoinfection. J. Clin. Microbiol. 42, 4237–4241 (2004).
Mayxay, M., Pukrittayakamee, S., Chotivanich, K., Looareesuwan, S. & White, N. J. Persistence of Plasmodium falciparum HRP-2 in successfully treated acute falciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 95, 179–182 (2001).
Marquart, L., Butterworth, A., McCarthy, J. S. & Gatton, M. L. Modelling the dynamics of Plasmodium falciparum histidine-rich protein 2 in human malaria to better understand malaria rapid diagnostic test performance. Malar. J. 11, 74 (2012).
Gamboa, D. et al. A large proportion of P. falciparum isolates in the Amazon Region of Peru Lack pfhrp2 and pfhrp3: Implications for malaria rapid diagnostic tests. PLoS ONE 5, e8091 (2010).
Berhane, A. et al. Major threat to malaria control programs by Plasmodium falciparum lacking histidine-rich protein 2, Eritrea. Emerg. Infect. Dis. 24, 462–470 (2018).
Mihreteab, S. et al. Increasing artemisinin-resistant HRP2-negative malaria in Eritrea. N. Engl. J. Med. 389, 1191–1202 (2023).
Iriart, X. et al. Misdiagnosis of imported falciparum malaria from African areas due to an increased prevalence of pfhrp2/pfhrp3 gene deletion: The Djibouti case. Emerg. Microbes Infect. 9, 1984–1987 (2020).
Bharti, P. K. et al. Prevalence of pfhrp2 and/or pfhrp3 gene deletion in Plasmodium falciparum Population in eight highly endemic states in India. PLoS ONE 11, e0157949 (2016).
Stabler, T. C. et al. Gene coverage count and classification (GC3): A locus sequence coverage assessment tool using short-read whole genome sequencing data, and its application to identify and classify histidine-rich protein 2 and 3 deletions in Plasmodium falciparum. Malar. J. 21, 357 (2022).
Gibbons, J. et al. Lineage-specific expansion of Plasmodium falciparum parasites With pfhrp2 deletion in the Greater Mekong Subregion. J. Infect. Dis. 222, 1561–1569 (2020).
MalariaGEN et al. Pf7: An open dataset of Plasmodium falciparum genome variation in 20,000 worldwide samples. Wellcome Open Res. 8, 22 (2023).
World Health Organization. Master Protocol for Surveillance of Pfhrp2/3 Deletions and Biobanking to Support Future Research (World Health Organization, 2020).
World Health Organization. Malaria Rapid Diagnostic Tests (World Health Organization, 2017).
Mangold, K. A. et al. Real-time PCR for detection and identification of Plasmodium spp. J. Clin. Microbiol. 43, 2435–2440 (2005).
World Health Organization & UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases. Microscopy for the Detection, Identification and Quantification of Malaria Parasites on Stained Thick and Thin Blood Films in Research Settings (Version 1.0): Procedure: Methods Manual. (World Health Organization, Geneva, 2015).
Snounou, G. et al. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol. Biochem. Parasitol. 61, 315–320 (1993).
Brockman, A. et al. Application of genetic markers to the identification of recrudescent Plasmodium falciparum infections on the northwestern border of Thailand. Am. J. Trop. Med. Hyg. 60, 14–21 (1999).
Baker, J. et al. Genetic diversity of Plasmodium falciparum histidine-rich protein 2 (PfHRP2) and its effect on the performance of PfHRP2-based rapid diagnostic tests. J. Infect. Dis. 192, 870–877 (2005).
Kumar Bharti, P. et al. Sequence variation in Plasmodium falciparum histidine rich proteins 2 and 3 in Indian isolates: Implications for malaria rapid diagnostic test performance. Sci. Rep. 7, 1308 (2017).
Lê, H. G. et al. Genetic variations in histidine-rich protein 2 and histidine-rich protein 3 of Myanmar Plasmodium falciparum isolates. Malar. J. 19, 388 (2020).
Alemayehu, G. S. et al. Genetic variation of Plasmodium falciparum histidine-rich protein 2 and 3 in Assosa zone, Ethiopia: its impact on the performance of malaria rapid diagnostic tests. Malar. J. 20, 394 (2021).
Viana, G. M. R. et al. Histidine-rich protein 2 (pfhrp2) and pfhrp3 gene deletions in Plasmodium falciparum isolates from select sites in Brazil and Bolivia. PLoS ONE 12, e0171150 (2017).
Góes, L. et al. Evaluation of histidine-rich proteins 2 and 3 gene deletions in Plasmodium falciparum in endemic areas of the Brazilian Amazon. Int. J. Environ. Res. Public. Health 18, 123 (2021).
Ahouidi, A. et al. An open dataset of Plasmodium falciparum genome variation in 7,000 worldwide samples [version 2; peer review: 2 approved]. Wellcome Open Res. (2021).
Rogier, E. et al. Plasmodium falciparum pfhrp2 and pfhrp3 gene deletions among patients enrolled at 100 health facilities throughout Tanzania: February to July 2021. Sci. Rep. 14, 8158 (2024).
Funwei, R. et al. Molecular surveillance of pfhrp2 and pfhrp3 genes deletion in Plasmodium falciparum isolates and the implications for rapid diagnostic tests in Nigeria. Acta Trop. 196, 121–125 (2019).
Kaaya, R. D. et al. Deletions of the Plasmodium falciparum histidine-rich protein 2/3 genes are common in field isolates from north-eastern Tanzania. Sci. Rep. 12, 5802 (2022).
World Health Organization. Meeting Report of the WHO Evidence Review Group on Low-Density Malaria Infections. 30 https://cdn.who.int/media/docs/default-source/malaria/mpac-documentation/mpac-oct2017-erg-malaria-low-density-infections-session29dbaa145bf0c4195ab2d4b84d72fa062.pdf?sfvrsn=69b6e0b2_2&download=true (2017).
Mills, C. D., Burgess, D. C., Taylor, H. J. & Kain, K. C. Evaluation of a rapid and inexpensive dipstick assay for the diagnosis of Plasmodium falciparum malaria. Bull. World Health Organ. 77, 553 (1999).
Baker, J. et al. Global sequence variation in the histidine-rich proteins 2 and 3 of Plasmodium falciparum: Implications for the performance of malaria rapid diagnostic tests. Malar. J. 9, 129 (2010).
Guo, B. et al. Strong positive selection biases identity-by-descent-based inferences of recent demography and population structure in Plasmodium falciparum. Nat. Commun. 15, 2499 (2024).
Gendrot, M., Fawaz, R., Dormoi, J., Madamet, M. & Pradines, B. Genetic diversity and deletion of Plasmodium falciparum histidine-rich protein 2 and 3: A threat to diagnosis of P. falciparum malaria. Clin. Microbiol. Infect. 25, 580–585 (2019).
Vera-Arias, C. A. et al. High-throughput Plasmodium falciparum hrp2 and hrp3 gene deletion typing by digital PCR to monitor malaria rapid diagnostic test efficacy. Elife 11, e72083 (2022).
Kamaliddin, C. et al. A countrywide survey of hrp2/3 deletions and kelch13 mutations co-occurrence in Ethiopia. J. Infect. Dis. 230, e1394–e1401 (2024).
Rogier, E. et al. Plasmodium falciparum pfhrp2 and pfhrp3 gene deletions from persons with symptomatic malaria infection in Ethiopia, Kenya, Madagascar, and Rwanda. Emerg. Infect. Dis. 28, 608–616 (2022).
Herman, C. et al. Multiplex malaria antigen detection by bead-based assay and molecular confirmation by PCR shows no evidence of Pfhrp2 and Pfhrp3 deletion in Haiti. Malar. J. 18, 380 (2019).
Acknowledgements
The authors sincerely thank the health workers involved in this study during the sample enrollment and all participants who agreed to join the study. We also acknowledge the support from Dinas Kesehatan Kabupaten Mimika for allowing us to conduct this study. The study was implemented by FIND (Study Code: 7876/2-2) with funding from Bill and Melinda Gates Foundation (BMGF). We thank Fiqry Hasan Kleib for their valuable input in statistical analyses.
Author information
Authors and Affiliations
Contributions
R.N., A.M.P, E.Sutanto, L.T., R.Ahmed, E.O., L.C planned and wrote the study protocol; R.N. E.K., J.R.P., and L.T. supervised and authorized the sample collection in the study sites; R.Amalia, F.A.N., A.M.P., and L.T. collected the samples; A.M.P., K.S., R.Amalia, and F.A.N. performed the experiments; R.N., A.M.P., K.S., Q.C., K.T., E.Sidhartha, and E.Sutanto analyzed the data; A.M.P., E.Sutanto, R.N. wrote the original draft of the manuscript. Q.C provided inputs on data analysis. All authors reviewed the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol was approved by the ethics committee of Eijkman Institute for Molecular Biology (EIMB) and Atma Jaya Catholic University of Indonesia (Ethical Clearance Numbers: 170/EIREC/2021 and 0008U/III/PPPE.PM.10.05/10/2022, respectively). The informed consent was written in English, then translated to the national language, Bahasa Indonesia, to ensure all information was correctly delivered to eligible participants. In addition, the informed consent was prepared in three age categories: child (5–12 y.o.), adolescent (13–17 y.o.), and adult (above 18 y.o.). For illiterate individuals, the informed consent process was conducted with an impartial witness where the participant thumb-printed and the witness signed the form. For children, assent was obtained from the child and the participant’s parents or guardians would either sign or thumb-print if consented to participate. All experiments were conducted following the relevant guidelines and regulations in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Puspitasari, A.M., Sutanto, E., Syauqi, K. et al. Cryptic absence and genetic variation of Plasmodium falciparum PfHRP2 and PfHRP3 from isolates in Papua, Indonesia. Sci Rep 15, 19511 (2025). https://doi.org/10.1038/s41598-025-02834-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02834-x
