
Abstract
Although changes in insular function have been thought to play a central role in the pathophysiology of anorexia nervosa (AN), due to factors such as insufficient sample size, there have been no studies examining changes in resting-state functional connectivity (rsFC) between insula and whole brain in AN, based on functional localization of insula. Here, we subdivided insula into 6 regions per side based on functional localization and reanalyzed previously published functional magnetic resonance imaging data from 114 female patients with AN and 135 female healthy controls (HC). We calculated the rsFCs between ROIs and compared the results between groups, with the 12 insular regions serving as seed ROIs and 142 regions of the whole brain as target ROIs. Compared to HC, AN patients had a increased rsFC between dorsal anterior insula (daIC) and amygdala, and a decreased rsFC between posterior division of dorsal middle insula (pdmIC) and opercular cortex (false discovery rate [FDR] corrected p-value < 0.05 with analysis-level correction, which means that FDR correction was applied to all seed ROIs and all target ROI combinations). These rsFC changes may be the neurological basis for AN symptoms, such as hypersensitivity to negative stimuli, taste disorder, and enhanced taste aversion learning.
Similar content being viewed by others


Introduction
The potential link between anorexia nervosa (AN) features and changes in insular function is an important one that warrants investigation. AN is a severe psychiatric disorder characterized by food restriction leading to weight loss, fear of obesity, and body image disorders and has the highest mortality rate of all psychiatric disorders, with approximately 5% of patients dying within four years of diagnosis1,2. The pathophysiology of AN is maintained by a vicious cycle between diet and impaired self-perception, in which food restriction leads to starvation, which causes deterioration of mental health including anxiety, further strengthening fear of obesity and body dissatisfaction, ultimately leading to even greater food restriction3. The insular cortex is a key node involved in this vicious cycle, because it is not only the site of perception of one’s own body, visceral sensations such as gastrointestinal distension and hunger, and subjective emotions such as disgust and fear4, but also contains primary gustatory cortex and is associated with food-related reward processing3,5. Indeed, previous studies investigating resting-state functional connectivity (rsFC) in AN have repeatedly observed abnormalities in insular rsFCs in using network-of-interest ICA-based or graph analysis methods6,7,8,9,10,11,12. The volume of insula has also been found to be positively correlated with the severity of AN symptoms and to be increased in AN who have recovered from acute weight loss13,14.
The observed limitations in previous analyses underscore the urgent need for a refined approach that subdivides insula into functionally distinct regions to enhance the accuracy of connectivity studies in AN. In our recent study, to comprehensively and reliably elucidate the changes in rsFC associated with AN, we conducted a region of interest (ROI) to-ROI cross-sectional analysis using the largest sample size to date—114 participants with AN and 135 healthy controls—with all regions of the whole brain as seed and target ROIs15. Although ROI-to-ROI analysis using the whole brain as both seed and target ROIs requires a sufficiently large sample size, it enables a comprehensive and straightforward elucidation of rsFC changes occurring between all brain regions, including insular cortex. This contrasts with the network-of-interest independent component analysis (ICA), which only verifies rsFCs between constituent regions of any network extracted by ICA (e.g., Default Mode Network) and the selected region like insula, and graph analysis, which can analyze the entire brain but yields results that are difficult to interpret. Contrary to expectations, however, none of insular-related rsFC changes were found in the above recent research, even though the study found rsFC changes among 45 regions of the whole brain. This may be because of the lack of consideration for functional differentiation within insula when defining it as a single ROI using the Harvard-Oxford cortical and subcortical atlas, the default atlas for CONN.
Previous studies have shown high functional localization in insula: a meta-analysis of functional neuroimaging experiments revealed that the anterior insula responds specifically to socioemotional tasks ventrally and cognitive tasks dorsally16. In another meta-analysis, the left dorsal anterior insula, in particular, was found to be the only region that reliably responds to food stimuli, whether gustatory, olfactory, or visual, suggesting an important role of this region in the cognitive processing of food stimuli17. The posterior part of insula is closely involved in phonological and auditory hedonic processing with the auditory cortex18,19, in addition to responding specifically to sensorimotor tasks16. As for mid-insula, while previous meta-analyses have shown that the ventral part of mid-insula is associated with language representation20, many studies suggest that the dorsal part plays a vital role in speech perception and interoception20,21,22,23,24, and is also part of the primary gustatory cortex. Although it has been considered that the primary gustatory cortex in dorsomedial insula is located anteriorly22,25,26, the latest 7 Tesla ultra-high resolution fMRI study found that specific brain activity in response to each of sweet, salty, and sour tastes is found posteriorly in dorsomedial insula27. These previous studies suggest that insula is divided into ante-ventral, ante-dorsal, posterior, mid-ventral, and mid-dorsal functions, and given that the primary gustatory cortex may be localized in the mid-dorsal insular cortex, the mid-dorsal cortex may have different functions in the anterior and posterior parts. Each of these six regions has also been found to have different structural connectivity, as verified by diffusion MRI combined with tractography28. In summary, to accurately elucidate the rsFC changes in insular cortex in AN, it seems to be necessary to establish separate seed ROIs for insula, subdivided into six regions (ante-ventral, ante-dorsal, posterior, mid-ventral, mid-dorsal anterior half, and mid-dorsal posterior half) according to functional localization.
Hence, in this study, we performed ROI-to-ROI analysis on the dataset previously used in our cross-sectional study, using insula divided into six regions per side according to functional localization as seed ROIs and all regions of the whole brain as target ROIs. This study aims to elucidate the full extent of functional changes in insula, which is thought to be the vital node of the vicious cycle of AN between diet and impaired self-perception and plays an essential role in AN pathophysiology.
Methods
Participants
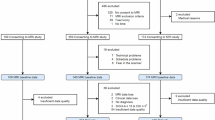
Participants in the study were recruited from outpatient clinics at five Japanese hospitals, namely (a) Chiba University Hospital (CHB), (b) Hospital of the University of Occupational and Environmental Health (UEH), (c) Tohoku University Hospital (THK), (d) Kyushu University Hospital (KYS), and (e) Kyoto University Hospital (KYU), and through participant recruitment websites and notifications from each hospital. Sites (a) through (d) recruited participants between July 2015 and March 2021 as part of A Multi-Site Study on the Brain of Eating Disorder Patients, while site (e) recruited participants between March 2014 and February 2019. Sample sizes per site are detailed in Table S1. Although race information was not collected, the vast majority of participants were Japanese females. Eligibility criteria included meeting the Diagnostic and Statistical Manual, 5th Edition (DSM-5) diagnostic criteria for AN, and HC participants were required to be at least 12 years old with no history of mental disorders, confirmed by psychosomatic physicians or psychiatrists. Diagnosis and AN subtype classification were based on structured DSM-5 interviews conducted by psychosomatic physicians or psychiatrists. Exclusion criteria encompassed claustrophobia, head trauma, neurological disorders, substance abuse, imminent thoughts of death. Comorbidity or a medical history of depression, bipolar disorder, obsessive-compulsive disorder, anxiety disorder, and personality disorder was permitted; however, those with comorbidity or a medical history of any other psychiatric disorders were excluded from participation in the study. Although we were careful to check that the participants in the patient group did not meet the exclusion criteria, we did not record any complications in the patient group participants. Due to the scarcity of male AN patients, only 2 male AN participants were recruited, and male AN patients were ultimately excluded from the study, along with 36 male HC participants. The final number of participants was 114 in the AN group (61 with AN of restricting type [AN-R] and 53 with AN of binge-eating/purging type [AN-BP]) and 135 in the HC group. The age range of participants in each group was as follows: 13–57 years (mean age: 28.9 years, standard deviation [SD]: 11.8) in the AN-R group, 16–64 years (mean age: 36.7 years, SD: 10.7) in the AN-BP group, and 17–58 years (mean age: 31.0 years, SD: 11.2) in the HC group. Twenty-two of the 61 AN-R patients and 27 of the 53 AN-BP patients were taking medication. Although we did not collect data on the psychological therapies the patients were receiving, it is likely that most patients were not receiving structured psychological therapy, because typical psychological therapies for AN, such as Enhanced Cognitive Behavioral Therapy (CBT-E), are not covered by insurance in Japan. All participants provided an informed consent form after receiving a full verbal and written explanation of the aims and procedures of the study. The study was approved by the ethics committee of the National Centre for Psychiatric and Neuropsychiatric Research (NCNP) and conducted in accordance with the ethical standards of the relevant national and institutional committees on human experimentation and the 1975 Declaration of Helsinki, as revised in 2008.
Physical and psychological assessment
Participants underwent height and weight measurements on the same day as their MRI scans. Additionally, within a two-week timeframe before and after the MRI, participants completed psychological assessments, including the Japanese version of the National Adult Reading Test (JART), the State-Trait Anxiety Inventory (STAI), the Beck Depression Inventory-II (BDI-II), and the Eating Disorder Examination Questionnaire (EDE-Q). The EDE-Q comprises four subscales (restraint, eating concern, shape concern, and weight concern), with the global score representing the average of these subscales’ scores. These self-reported psychological scales were utilized to characterize the participants and conduct correlation analyses between these scales and the rsFCs that displayed intergroup disparities.
Dataset
The dataset we used in this study is a secondary release dataset identical to the one analyzed by Sudo et al. (2024). We have also previously published studies analyzing primary release datasets14. The secondary release dataset incorporates additional information absent in the primary release dataset, including (1) duration of illness, psychotropic medication usage, JART scores, BDI-II scores, and STAI scores for all participants; and (2) data from MRI scans, JART scores, EDE-Q scores, BDI-II scores, STAI scores, age, height, and weight measurements collected at CHB for 12 patients with AN and 15 HC subjects.
MRI acquisition and preprocessing
Brain MRI scans were conducted using 3.0 Tesla scanners across all sites (THK and KYS: Philips Achieva; CHB and UEH: GE Discovery MR750; KYU: Siemens MAGNETOM TrioTim). Resting-state fMRI scans lasted 10 min and 10 s at KYU and 7 min at the other four facilities. Detailed parameters, including the total scan time for acquiring T1-weighted images and resting-state functional MRI (rsfMRI), are provided in Table S2. Preprocessing and quality control procedures were carried out using Statistical Parametric Mapping-12 (SPM12) and NITRC Functional Connectivity Toolbox (CONN) 18b. To ensure magnetic field stability, the initial five volumes of rsfMRI data with a repetition time (TR) of 3000 milliseconds and the initial six volumes with a TR of 2500 milliseconds were excluded. Subsequently, the default preprocessing pipeline of CONN was applied, encompassing functional realignment and unwarping, functional center to coordinates, correction for slice timing, identification of functional outliers, functional direct segmentation and normalization, structural center to coordinates, structural segmentation and normalization, and functional smoothing.
Functional network construction
The computation of region-to-region rsFCs was conducted utilizing CONN and the anatomical component-based noise correction (aCompCor) method in MATLAB R2022a. To remove confounding factors (white matter, cerebrospinal fluid, six realignment parameters, first-order temporal derivatives of motion, and outlier scans), we employed CONN’s default denoising pipeline, incorporating aCompCor regression29. Subsequently, bandpass filtering (0.008–0.09 Hz) was applied to the fMRI data to attenuate both high- and low-frequency noise components. Seed ROIs were bilateral insula (12 ROIs) defined by the Brainnetome atlas. The Brainnetome atlas uses multimodal MRI data consisting of structural MRI, diffusion MRI combined with tractography, and resting-state fMRI to segment the whole brain into 246 areas, with 6 areas per side for insula28. The atlas not only reveals many previously overlooked anatomical subdivisions but also clarifies what mental processes each region of the atlas is responsible for by referring to the BrainMap database. Therefore, this atlas has been used in various functional brain imaging studies in recent years30,31,32, and it was judged that using this atlas to define the seed ROIs was the best way to achieve the aim of this study, which was to set insula regions subdivided by functional localization as seed ROIs. Target ROIs were defined for insula by the Brainnetome atlas (12 ROIs) and for brain regions other than insula by the CONN atlas consisting of the Harvard-Oxford cortical and subcortical atlas (104 ROIs) and the AAL cerebellar atlas (26 ROIs). We used the default atlas for CONN rather than the Brainnetome atlas to define target ROIs in brain regions other than the insula and provide continuity with our previous study, which examined rsFC changes occurring in AN in all brain regions. During the ROI-to-ROI connectivity analysis, we computed a bivariate correlation individually on the BOLD time series of each ROI pair, with the resulting correlation coefficients then transformed into Fisher’s Z-scores. Consequently, the output for each participant consisted of a 12 × 142 matrix representing the Fisher-transformed correlation coefficients of ROI-to-ROI rsFCs.
Statistical analysis
Demographic and clinical characteristics
Demographic characteristics were assessed and compared using SPSS (Statistical Package for Social Science version 30.0. IBM Corp., Armonk, NY). Variables were examined for normal distribution using the Shapiro-Wilk test. Non-normally distributed variables (age, body mass index [BMI], and results from the psychological tests: JART, EDE-Q, STAI, and BDI-II) were compared between groups using the Kruskal-Wallis test, followed by Dunn’s test for multiple comparisons. The duration of illness was analyzed using the Mann-Whitney U test. The chi-square test was employed to compare groups based on psychotropic medication usage. Total intracranial volume (TIV), which was normally distributed and found to be equally distributed by the Levene test, was compared between groups using one-way ANOVA, followed by Bonferroni’s multiple comparison test. All statistical analyses were two-tailed, with a significance level set at p < .05.
Combat harmonization and intergroup comparison of functional networks
We performed Combat harmonization using the neuroCombat Python package to correct for rsFC values between ROIs for each participant to address potential site effects in the multicentre database33. Notably, the number of AN patients recruited from UEH and KYS was lower than other sites. However, site effects in multi-site databases are predominantly attributed to differences in the phase encoding direction and variations in fMRI manufacturers34. Thus, we organized the batches in Combat harmonization based on the fMRI manufacturer, which governs the phase encoding direction. Moreover, as indicated in Table S2, fMRI scans were conducted with participants keeping their eyes closed at THK, unlike at the other sites. However, we still prioritized the differences in phase encoding direction in harmonization because the impact of differences in imaging conditions due to eye-opening and closing on rsFC is deemed limited35. Specifically, we assigned the data acquired by the GE Discovery MR750 to batch 1, those obtained with a Philips Achieva were assigned to batch 2, and data imaged by Siemens MAGNETOM TrioTim were assigned to batch 3. Additionally, age, group (AN-R, AN-BP, or HC), BMI, and TIV measured by Brain Anatomical Analysis using Diffeomorphic Deformation version 4.3.2 (BAAD; Shiga University of Medical Science, Otsu, Japan) were included as covariates. Following Combat harmonization, the ROI-to-ROI rsFCs of each participant were reintegrated into CONN. Subsequently, group-level analysis was performed using the general linear model, with group comparisons of ROI-to-ROI rsFCs conducted by analysis of covariance (ANCOVA) with age as a covariate. The significance of group comparisons was assessed using a two-sided false discovery rate corrected p-value (p-FDR) < 0.05 with analysis-level correction, which means that the FDR correction was applied to all seed ROIs and all target ROI combinations. However, because this is a considerably conservative correction, we also used the seed-level corrected two-sided p-FDR < 0.05 criterion, which applies the false discovery rate correction to each seed ROI individually to prevent oversights by false negative. We did not examine potential interaction effects between the diagnostic groups and covariates such as age, BMI, TIV, or duration of illness. That is because these covariates were incorporated into the model for the purpose of controlling for confounding factors in group comparisons, and no specific interaction hypotheses were formulated a priori.
Correlation analysis between rsFCs with intergroup differences and self-reported psychological scales
We conducted correlation analyses between self-reported psychological scales (EDE-Q, BDI-II, STAI) and the rsFCs exhibiting significant intergroup differences between AN and HC. Spearman’s rank correlation coefficient was computed between the ROI-to-ROI rsFC values of AN patients in these connectivities and their scores on the self-reported psychological scales using SPSS version 30.0. The significance of the correlation was determined by a two-sided p-FDR < 0.05.
Correlation analysis between BMI and psychological scales and between psychological scales
To evaluate the validity of the self-reported psychological scales in the AN patient group of this study, we conducted correlation analyses between BMI and the psychological scales as well as among the psychological scales in AN patient group. Spearman’s rank correlation coefficients were calculated using SPSS version 30.0 to assess these relationships. The significance of the correlation was determined by a two-sided p-FDR < 0.05.
Results
Demographics and clinical characteristics
Table 1 displays the demographic characteristics and psychological test outcomes of the participants. AN-BP had a slightly higher mean age than AN-BP, whereas the mean BMI was notably higher in HC. The mean duration of illness was longer in AN-BP than in AN-R. HC had higher mean JART scores than AN patients. Concerning the mean EDE-Q scores, both the global and subscale scores followed the order: AN-BP > AN-R > HC. AN patients also exhibited higher mean scores across STAI and BDI-II than HC.
Comparison of rsFCs between AN and HC
Table 2; Figs. 1, and 2 present the rsFCs that exhibited significant differences between AN (AN-R and AN-BP) and HC (two-sided p-FDR < 0.05 with analysis-level correction or seed-level correction). The rsFC between left dorsal agranular insula (corresponding to dorsal anterior insula : daIC) and right amygdala was increased and the rsFC between right dorsal granular insula (corresponding to posterior division of dorsal mid-insula: pdmIC) and right parietal opercular cortex was decreased in AN (p-FDR < 0.05, analysis-level correction). The decreased rsFCs were also observed between left pdmIC and right central to parietal opercular cortex and between right daIC and cerebellar flocculus (lobule X) (p-FDR < 0.05, seed-level correction).

Connectome showing the rsFC changes in AN. This figure presents the connectome showing rsFCs altered in AN relative to HC. The red lines indicate significantly increased rsFCs and the blue lines indicate significantly decreased rsFCs in AN patients (114 females) relative to HC (135 females). Group comparison of ROI-to-ROI rsFCs was done by ANCOVA using age as a covariate. Red or blue lines connecting brain region names highlighted in yellow indicate that the rsFC between these regions was significant at false discovery rate corrected p-value [p-FDR] < 0.05 with analysis-level correction, meaning that FDR correction was applied across all combinations of seed and target ROIs. In contrast, red or blue lines connecting brain regions without yellow highlights indicate that the rsFC between these regions was significant at the p-FDR < 0.05 with seed-level correction, where FDR correction was applied separately for each seed ROI. The “r” after each region indicates right, and the “l” shows left. pdmIC, posterior division of dorsal mid-insular cortex; daIC, dorsal anterior insular cortex; Cereb, cerebellar; AMG, amygdala; PO, parietal opercular cortex; CO, central opercular cortex.

Schematic diagram showing the rsFC changes in AN. This figure presents a schematic diagram showing the rsFC changes in AN patients (114 females) relative to HC (135 females) based on a sagittal brain section. The left side of the figure corresponds to the frontal region, and the right side corresponds to the occipital region. The left and right sides of the brain are not clearly shown in this figure. The oval in the middle of the diagram shows the insular cortex, and the six fractions of the oval are respectively dorsal anterior (dorsal agranular) insular cortex: daIC, posterior division of dorsal middle (dorsal granular) insular cortex: pdmIC, dorsal dysgranular insular cortex, ventral agranular insular cortex, ventral granular insular cortex, hypergranular insular cortex. The intergroup comparison of ROI-to-ROI rsFCs was done by ANCOVA using age as a covariate. A solid red lines represent significantly increased rsFC in AN, while a solid blue line represent significantly decreased rsFC in AN, both at the p-FDR < 0.05 level after analysis-level correction, where FDR correction is applied across all seed and target ROI combinations. Dashed blue lines indicate significantly decreased rsFC at the p-FDR < 0.05 level after seed-level correction, where FDR correction is applied separately for each seed ROI.
Comparison of rsFCs between AN-R and HC
Table 3; Fig. 3a present the rsFC that exhibited significant differences between AN-R and HC (two-sided p-FDR < 0.05 with seed-level correction or seed-level correction). The rsFCs between left daIC and right amygdala or right hippocampus were increased, and the rsFC between left daIC and right frontal opercular cortex was decreased in AN-R compared to HC (p-FDR < 0.05, seed-level correction).

Connectome showing the rsFC changes in AN-R or AN-BP. (A) This figure shows the connectome representing rsFCs that were altered in AN-R patients (61 females) compared to HC (135 females). The red lines indicate significantly increased rsFCs and the blue line indicates significantly decreased rsFC in AN-R patients relative to HC. Group comparison of ROI-to-ROI rsFCs was done by ANCOVA using age as a covariate. Red or blue lines connecting brain regions indicate that the rsFC between these regions was significant at the p-FDR < 0.05 with seed-level correction, where FDR correction was applied separately for each seed ROI. The “r” after each region indicates right, and the “l” shows left. daIC, dorsal anterior insular cortex; AMG, amygdala; HPC, hippocampus; CO, central opercular cortex. (B) This figure shows the connectome representing rsFCs that were altered in AN-BP patients (53 females) compared to HC (135 females). The blue lines indicate significantly decreased rsFCs in AN-BP patients relative to HC. Group comparison of ROI-to-ROI rsFCs was done by ANCOVA using age as a covariate. Blue lines connecting brain region names highlighted in yellow indicate that the rsFC between these regions was significant at the p-FDR < 0.05 with analysis-level correction, meaning that FDR correction was applied across all combinations of seed and target ROIs. The “r” after each region indicates right, and the “l” shows left. pdmIC, posterior division of dorsal mid-insular cortex; PO, parietal opercular cortex.
Comparison of rsFCs between AN-BP and HC
Table 3; Fig. 3 (b) present the rsFC that exhibited significant differences between AN-BP and HC (two-sided p-FDR < 0.05 with seed-level correction or seed-level correction). The rsFCs between bilateral pdmICs and right parietal opercular cortex were decreased in AN-BP compared to HC (p-FDR < 0.05, analysis-level correction).
Comparison of rsFCs between AN subtypes (AN-R vs. AN-BP)
As a result of comparing the subtypes of AN, there were no rsFCs that showed statistical significance between AN-R and AN-BP (p-FDR, seed-level correction).
Correlations between rsFCs with intergroup differences and self-reported psychological scales
Table S3 displays correlation coefficients between the identified rsFCs exhibiting group disparities between HC and AN and the self-reported psychological scale scores (EDE-Q, BDI-II, STAI). No significant correlations were observed between the rsFCs that differed between HC and AN and the scores on each psychological scale at p-FDR < 0.05.
Correlations between BMI and psychological scales and between psychological scales
The results of the correlation analysis between BMI and psychological scales and between psychological scales in the AN patient group are shown in Table S4. Positive correlations were found between BMI and the global score and restraint score of EDE-Q (p-FDR < 0.05). High positive correlations were found between EDE-Q subscales, between BDI-II and EDE-Q scores, between STAI and EDE-Q scores, and between BDI-II and STAI scores (p-FDR < 0.05).
Discussion
This study subdivided insula, which is thought to be the key node of the vicious cycle of AN between food restriction and impaired self-perception, according to anatomical and functional connection by using the Brainnetome atlas, set them as the ROIs, and examined the rsFCs between them and all other brain regions. Compared to HC, the rsFC between left daIC and right amygdala was increased, and the rsFC between right pdmIC and right parietal opercular cortex was decreased in AN. Although less statistically reliable than these rsFC changes, rsFC between left pdmIC and right opercular corte, and between right daIC and cerebellar flocculus, were also decreased in AN. Furthermore, comparisons between HC and each of the AN-R and AN-BP groups separately revealed that the increased rsFC between right amygdala and left daIC occurred primarily in AN-R, while decreased rsFCs between bilateral pdmICs and the parietal opercular cortex were mainly observed in AN-BP. These results are consistent with trends shown in previous studies, namely, that increased rsFCs have been frequently reported between brain regions including anterior insula (e.g., increased anterior insular rsFC in cerebellar networks6, increased rsFC between anterior insula and lingual gyrus7), while decreased rsFCs have been frequently reported between brain regions including posterior insula (e.g., decreased rsFC in the cerebellar–posterior insular-parietal-cingular subnetwork8, decreased rsFC in the thalamus-posterior insular subnetwork9,36. On the other hand, the present study was the first to show that rsFCs between insula and amygdala, opercular cortex, and cerebellar flocculus were changed in AN. These discoveries have been made possible because, unlike previous studies, we employed ROI-to-ROI analysis with a sufficient sample size for whole brain regions, and the seed ROIs were set finely according to the functional localization of insula. Furthermore, as discussed later, these rsFC changes observed in AN may contribute to maintaining the vicious cycle between dietary restriction and impaired self-perception in AN through mechanisms such as taste disorder and enhanced taste aversion learning. In the following paragraphs, firstly, we delve into the implications of the changes in rsFC observed in AN compared to HC, followed by a discussion of the differences rsFC changes when comparing AN-R and AN-BP and HC individually. Then, we consider the implications of the absence of correlation between rsFCs manifesting group disparities and psychological scales. Finally, we discuss the clinical implications of our findings and the limitations of this study.
The increased rsFC between daIC and amygdala may be involved in the intensity of hypersensitivity to negative stimuli in AN. Both anterior insular cortex and amygdala are components of the salience network responsible for evaluation and emotion-processing in response to stimuli, and lesions of anterior insular cortex have been found to reduce excitability to both positive and negative visual stimuli, while lesions of amygdala reduce excitability to negative visual stimuli37. Indeed, ventral/dorsal anterior insular cortex is selectively responsive to visual aversive stimuli38 and is also involved in sympathetic activity during fearful stimuli, and functional connectivity between anterior insular cortex and amygdala has been found to increase during horror film viewing39. Our present finding of increased rsFC between daIC and amygdala in AN aligns well with these prior observations, suggesting that such enhanced connectivity could underlie the heightened sensitivity to aversive stimuli seen in AN.
The increased rsFC between daIC and amygdala may also suggest enhanced conditioned taste aversion (CTA) in AN. Animal studies in rats have shown that anterior insula and basolateral amygdala are essential for CTA and that reciprocal connections between the two regions play an essential role in the retention of CTA40,41. Furthermore, it has been found that anterior insula, amygdala and prelimbic cortex are synchronously activated during CTA42, and the induction of long-term potentiation in basolateral amygdaloid nucleus-anterior insula pathway enhances the retention of memories of CTA43. The fact that the rsFC changes between daIC and amygdala in the present study were found only in left insula also provides collateral evidence for CTA enhancement in AN, given that meta-analyses have shown that left daIC is the seat of cognitive processing to food stimuli17.
The decreased rsFCs between pdmIC and right opercular cortex suggest that abnormal gustatory processing occurs in AN. This may be explained by magnetoencephalography and fMRI studies which have suggested that the human primary gustatory cortex is located in the middle part of dorsal insula and the overlying frontal to parietal opercular cortex. Specifically, a magnetoencephalography study reported that NaCl- and saccharin-responsive areas are located in parietal opercular cortex and insular transition zones44. An fMRI study similarly showed NaCl-responsive activity in parietal and insular transition areas as well as frontal opercular cortex45. In addition, a multi-voxel pattern analysis study using fMRI found that activity patterns distinguishing sweet, bitter, salty, and sour tastes are located in anterior to mid-dorsal insula and the overlying opercular cortex25. A 7-Tesla ultra-high resolution fMRI study also demonstrated taste-responsive activity (sweet, salty, and sour) in dorsomedial mid-insular cortex27. The observed reduction in rsFCs between these regions in AN may indicate a disruption in the neural circuits involved in gustatory perception.
The decreased rsFC between daIC and cerebellar flocculus may be involved in overreacting to taste stimuli, which is associated with high emotional susceptibility in AN. This decreased rsFC may also play a role in increased disgust with nausea in AN. In a study examining how high emotional susceptibility affects responses to taste stimuli in healthy subjects, a decreased rsFC between left anterior insula and left cerebellar cortex predicted high emotional susceptibility, and subjects with emotional susceptibility did not discriminate between pleasant/displeasing and neutral taste stimuli, exhibiting strong left anterior insula responses to all types of taste stimuli46. Moreover, in a study examining the effects of acupuncture on disgust, defined as a subjective emotion accompanied by strong visceral sensations such as nausea, acupuncture’s effect on reducing disgust was associated with increased rsFC between the cerebellar flocculus and anterior insula47. Thus, the diminished rsFCs observed in AN between daIC and cerebellar flocculus may underpin the abnormal gustatory responses and heightened disgust in AN.
The finding that decreased rsFCs between pdmIC and bilateral parietal opercular cortex were observed only in AN-BP, when comparing AN-R and AN-BP separately with HC, suggests that the brain functional changes responsible for taste abnormalities in AN may gradually develop as the disorder becomes more chronic. Patients with AN-BP tend to be older than those with AN-R, and it is commonly observed that patients initially diagnosed with AN-R transition to AN-BP, while transitions from AN-BP to AN-R are rare48. It has also been shown that the transition from AN-R to AN-BP leads to a longer duration of illness and worsens prognosis49. In other words, AN-BP has characteristics of a more chronic form of AN. Consistent with this, in the present study, the AN-BP group was older and had a longer duration of illness compared to the AN-R group. Taken together, the fact that decreased rsFC between the pdmIC and the bilateral parietal opercular cortex was not observed in the comparison between AN-R and HC, but was found with high statistical robustness in the comparison between AN-BP and HC, may indicate that the neural changes underlying taste abnormalities in AN gradually develop as the illness becomes chronic. Supporting this interpretation, a prior study assessing taste sensitivity to fat content in dairy solutions found no significant differences between AN-R patients and healthy controls, whereas AN-BP patients exhibited heightened sensitivity to fat50.
The lack of correlation between rsFCs which showed changes in AN compared to HC and EDE-Q scores, may be due to EDE-Q not being appropriate for symptom evaluation of the AN patients in this study. In a previous survey of 350 hospitalized AN patients (mean BMI 15.7 kg/m2), a positive correlation was found between the patients’ BMI and EDE-Q scores; in other words, the lower the BMI and the more severe the condition of the patient, the lower the EDE-Q score51. This may be due to the low awareness of the illness in AN patients, and several studies have shown that the lower the BMI and the more severe the condition of AN patients, the less awareness of the illness52,53. The BMI of the patients in this study was markedly low, with the average BMI of the 61 patients in the AN-R group being 14.3 kg/m2 and the average BMI of the 53 patients in the AN-BP group being 15.3 kg/m2, which corresponds to “severe” and “extreme” on the DSM-5 severity scale54, respectively. Therefore, most patients in this study had remarkably impaired awareness of their illness, and their EDE-Q scores did not increase despite the actual severity of their condition. This is considered to be the reason why no correlation was observed between the rsFCs that showed intergroup differences and EDE-Q scores. As shown in Table S4, the positive correlations observed in the patient group between BMI and the restraint and global scores of EDE-Q support this reasoning.
The lack of correlation between rsFCs which demonstrated group differences and psychological scales for depression and anxiety supports the notion that the rsFC variations identified in this study reflect the pathophysiology of AN rather than general psychiatric symptoms. In the current research, rsFCs that exhibited significant differences between AN and HC encompassed rsFCs previously linked to depression and anxiety in prior research. For example, the rsFC change between left insula and left amygdala has been reported in subthreshold depression55. The strength of the rsFC between anterior insula and amygdala has also been found to be positively correlated with state anxiety56. Hence, there is apprehension that rsFCs influenced by depression and anxiety may have been included in those rsFCs exhibiting discrepancies between groups. Nonetheless, the absence of correlation between the rsFCs that differed between groups and the scores on BDI-II or STAI in this study suggests the absence of confounding effects from rsFCs associated with depression and anxiety, which are prevalent yet nonspecific psychiatric symptoms in individuals with AN.
The results of this study provide new insights from the perspective of taste into the mechanism of the behavior of continuing to restrict food intake despite being underweight, which is the biggest problem symptom in the clinical setting of AN. It has been suggested that this core symptom of AN, dietary restriction, may be influenced not only by fear of gaining weight or distorted body image but also by abnormal responses to taste stimuli57,58. It is known that AN patients have an overreaction of the reward circuit consisting of the prefrontal cortex and insular cortex to taste stimuli, which is related to avoidance of the stimuli and is presumed to be due to a tendency to feel anxiety about unpleasant stimuli58. In addition, changes in taste thresholds occurring in AN patients are also thought to contribute to food intake restriction57. The present study’s findings—specifically, the increased rsFC between daIC and amygdala, which may reflect heightened sensitivity to negative stimuli and enhanced CTA, and the decreased rsFC between pdmIC and opercular cortex, which may reflect abnormalities in primary gustatory processing—support these previous researches and suggest that abnormal responses to taste stimuli may be a key factor contributing to food restriction in individuals with AN.
Some limitations should be discussed. Because this was a cross-sectional study, it was not possible to discern whether the observed intergroup differences in rsFCs were related to AN development or merely reflected changes in brain function derived from starvation over time. Regarding demographic data, the biggest concern is the lack of data on participants’ comorbidities. In particular, the distribution of depression and anxiety, the most common comorbidities in AN59,60, should have been clarified, as well as how the comorbidity of depression and anxiety affected the study results. However, since no significant correlation was found between the depression and anxiety scores (BDI-II and STAI) and rsFCs that showed intergroup differences in this study, the influence of comorbid depression and anxiety was likely relatively small. Other limitations of this study are as follows. Participants in this study were almost entirely Japanese women. Therefore, it remains unclear to what extent the results of this study can be extrapolated to other racial groups, men, or gender-diverse groups. In addition, we could not collect self-reported psychological measures for all participants, which may have introduced bias due to missing data in the correlation analysis between rsFCs and psychological measures. Moreover, 49 of the 114 AN patients were receiving medication, but the specific medications administered were not recorded, so we could not investigate the effect of drugs on the outcomes. Future studies will be necessary to address this issues, including longitudinal research before and after treatment and international collaborative efforts. Indeed, our team is currently conducting one such longitudinal study61.
Conclusion
In this study, rsFCs were analyzed in the whole brain using a large sample collected at a multicenter site, with insula subdivided according to functional localization as seed ROIs. The results showed that in AN, rsFC was increased between left daIC and right amygdala, and decreased between right pdmIC and right parietal opercular cortex. Additionally, rsFC was decreased between left pdmIC and its covering opercular cortex and between right daIC and cerebellar flocculus, though the statistical robustness was somewhat less. These rsFC alterations may be the neurological basis of multiple symptoms and features of AN, such as hypersensitivity to negative stimuli, taste disorders, and enhanced taste aversion learning, and may contribute to the vicious cycle between food restriction and impaired self-perception in AN.
Data availability
The data of demographics, psychological scale scores, and individual-level of rsFC used in this study are available from corresponding author upon reasonable request. The raw data of T1-weight MRI images and resting-state fMRI are not publicly available because consent for disclosure has not been obtained from the participants.
References
Harris, C. & Barraclough, B. Excess mortality of mental disorder. Br. J. Psychiatry. 173, 11–53 (1998).
Meczekalski, B., Podfigurna-Stopa, A. & Katulski, K. Long-term consequences of anorexia nervosa. Maturitas 75, 215–220 (2013).
Frank, G. K. W., DeGuzman, M. C. & Shott, M. E. Motivation to eat and not to eat – The Psycho-Biological conflict in anorexia nervosa. Physiol. Behav. 206, 185–190 (2019).
Bud & (Craig, A. D. How do you feel — now? The anterior Insula and human awareness. Nat. Rev. Neurosci. 10, 59–70 (2009).
Frank, S., Kullmann, S. & Veit, R. Food related processes in the insular cortex. Front. Hum. Neurosci. 7, 499 (2013).
Amianto, F. et al. Intrinsic connectivity networks within cerebellum and beyond in eating disorders. Cerebellum 12, 623–631 (2013).
Boehm, I. et al. Increased resting state functional connectivity in the fronto-parietal and default mode network in anorexia nervosa. Front. Behav. Neurosci. 8, 346 (2014).
Gaudio, S., Olivo, G., Beomonte Zobel, B. & Schiöth, H. B. Altered cerebellar–insular–parietal–cingular subnetwork in adolescents in the earliest stages of anorexia nervosa: a network–based statistic analysis. Transl Psychiatry. 8, 1–10 (2018).
Geisler, D. et al. Abnormal functional global and local brain connectivity in female patients with anorexia nervosa. J. Psychiatry Neurosci. JPN. 41, 6–15 (2016).
Gondo, M. et al. Effects of integrated hospital treatment on the default mode, salience, and frontal-parietal networks in anorexia nervosa: A longitudinal resting-state functional magnetic resonance imaging study. PLOS ONE. 18, e0283318 (2023).
Kullmann, S. et al. Aberrant network integrity of the inferior frontal cortex in women with anorexia nervosa. NeuroImage Clin. 4, 615–622 (2014).
Lord, A. et al. Brain parcellation choice affects disease-related topology differences increasingly from global to local network levels. Psychiatry Res. Neuroimaging. 249, 12–19 (2016).
Arold, D. et al. Predicting long-term outcome in anorexia nervosa: a machine learning analysis of brain structure at different stages of weight recovery. Psychol. Med. 1–10. https://doi.org/10.1017/S0033291723001861 (2023).
Tose, K. et al. Systematic reduction of Gray matter volume in anorexia nervosa, but relative enlargement with clinical symptoms in the prefrontal and posterior insular cortices: a multicenter neuroimaging study. Mol. Psychiatry. https://doi.org/10.1038/s41380-023-02378-4 (2024).
Sudo, Y. et al. Comprehensive Elucidation of resting-state functional connectivity in anorexia nervosa by a multicenter cross-sectional study. Psychol. Med. 1–14. https://doi.org/10.1017/S0033291724000485 (2024).
Kurth, F., Zilles, K., Fox, P. T., Laird, A. R. & Eickhoff, S. B. A link between the systems: functional differentiation and integration within the human Insula revealed by meta-analysis. Brain Struct. Funct. 214, 519–534 (2010).
Huerta, C. I., Sarkar, P. R., Duong, T. Q., Laird, A. R. & Fox, P. T. Neural bases of food perception: Coordinate-Based Meta-Analyses of neuroimaging studies in multiple modalities. Obes. Silver Spring Md. 22, 1439–1446 (2014).
Fletcher, P. D. et al. Auditory hedonic phenotypes in dementia: A behavioural and neuroanatomical analysis. Cortex J. Devoted Study Nerv. Syst. Behav. 67, 95–105 (2015).
Noesselt, T., Shah, N. J. & Jäncke, L. Top-down and bottom-up modulation of Language related areas – An fMRI study. BMC Neurosci. 4, 13 (2003).
Oh, A., Duerden, E. G. & Pang, E. W. The role of the Insula in speech and Language processing. Brain Lang. 135, 96–103 (2014).
Avery, J. A. et al. Major depressive disorder is associated with abnormal interoceptive activity and functional connectivity in the Insula. Biol. Psychiatry. 76, 258–266 (2014).
Avery, J. A. et al. A common gustatory and interoceptive representation in the human mid-insula. Hum. Brain Mapp. 36, 2996–3006 (2015).
Haruki, Y. & Ogawa, K. Role of anatomical insular subdivisions in interoception: interoceptive attention and accuracy have dissociable substrates. Eur. J. Neurosci. 53, 2669–2680 (2021).
Nord, C. L., Lawson, R. P. & Dalgleish, T. Disrupted dorsal Mid-Insula activation during interoception across psychiatric disorders. Am. J. Psychiatry. 178, 761–770 (2021).
Chikazoe, J., Lee, D. H., Kriegeskorte, N. & Anderson, A. K. Distinct representations of basic taste qualities in human gustatory cortex. Nat. Commun. 10, 1048 (2019).
Rolls, E. T. Functions of the anterior Insula in taste, autonomic, and related functions. Brain Cogn. 110, 4–19 (2016).
Avery, J. A. et al. Taste quality representation in the human brain. J. Neurosci. Off J. Soc. Neurosci. 40, 1042–1052 (2020).
Fan, L. et al. The human brainnetome atlas: A new brain atlas based on connectional architecture. Cereb. Cortex N Y N 1991. 26, 3508–3526 (2016).
Behzadi, Y., Restom, K., Liau, J. & Liu, T. T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. NeuroImage 37, 90–101 (2007).
Li, Y. et al. Mapping intrinsic functional network topological architecture in major depression disorder after electroconvulsive therapy. J. Affect. Disord. 311, 103–109 (2022).
Nij Bijvank, J. A. et al. Impaired saccadic eye movements in multiple sclerosis are related to altered functional connectivity of the oculomotor brain network. NeuroImage Clin. 32, 102848 (2021).
Zhang, S. et al. Effects of 12-week Escitalopram treatment on resting‐state functional connectivity of large‐scale brain networks in major depressive disorder. Hum. Brain Mapp. 44, 2572–2584 (2023).
Fortin, J. P. et al. Harmonization of multi-site diffusion tensor imaging data. NeuroImage 161, 149–170 (2017).
Yamashita, A. et al. Harmonization of resting-state functional MRI data across multiple imaging sites via the separation of site differences into sampling bias and measurement bias. PLOS Biol. 17, e3000042 (2019).
Patriat, R. et al. The effect of resting condition on resting-state fMRI reliability and consistency: a comparison between resting with eyes open, closed, and fixated. NeuroImage 78, 463–473 (2013).
Ehrlich, S. et al. Reduced functional connectivity in the thalamo-insular subnetwork in patients with acute anorexia nervosa. Hum. Brain Mapp. 36, 1772–1781 (2015).
Berntson, G. G. et al. The Insula, the amygdala and evaluative processes. Psychol. Sci. 22, 80–86 (2011).
Deen, B., Pitskel, N. B. & Pelphrey, K. A. Three systems of insular functional connectivity identified with cluster analysis. Cereb. Cortex. 21, 1498–1506 (2011).
Yoshihara, K. et al. Neural correlates of fear-induced sympathetic response associated with the peripheral temperature change rate. NeuroImage 134, 522–531 (2016).
Cubero, I., Thiele, T. E. & Bernstein, I. L. Insular cortex lesions and taste aversion learning: effects of conditioning method and timing of lesion. Brain Res. 839, 323–330 (1999).
Yamamoto, T., Shimura, T., Sako, N., Yasoshima, Y. & Sakai, N. Neural substrates for conditioned taste aversion in the rat. Behav. Brain Res. 65, 123–137 (1994).
Uematsu, A., Kitamura, A., Iwatsuki, K., Uneyama, H. & Tsurugizawa, T. Correlation between activation of the prelimbic cortex, basolateral amygdala, and agranular insular cortex during taste memory formation. Cereb. Cortex. 25, 2719–2728 (2015).
Escobar, M. L. & Bermúdez-Rattoni, F. Long-term potentiation in the insular cortex enhances conditioned taste aversion retention. Brain Res. 852, 208–212 (2000).
Kobayakawa, T. et al. Spatio-temporal analysis of cortical activity evoked by gustatory stimulation in humans. Chem. Senses. 24, 201–209 (1999).
Ogawa, H. et al. Functional MRI detection of activation in the primary gustatory cortices in humans. Chem. Senses. 30, 583–592 (2005).
Ebisch, S. J. H. et al. Emotional susceptibility trait modulates Insula responses and functional connectivity in flavor processing. Front Behav. Neurosci 9 (2015).
Bai, L. et al. The role of insula-cerebellum connection underlying aversive regulation with acupuncture. Mol. Pain. 14, 1744806918783457 (2018).
Peat, C., Mitchell, J. E., Hoek, H. & Wonderlich, S. Validity and utility of subtyping anorexia nervosa. Int. J. Eat. Disord. 42, 590–594 (2009).
Serra, R. et al. The transition from restrictive anorexia nervosa to binging and purging: a systematic review and meta-analysis. Eat. Weight Disord - Stud. Anorex Bulim Obes. 27, 857–865 (2022).
Sunday, S. R. & Halmi, K. A. Taste perceptions and hedonics in eating disorders. Physiol. Behav. 48, 587–594 (1990).
Berner, L. A., Shaw, J. A., Witt, A. A. & Lowe, M. R. The relation of weight suppression and body mass index to symptomatology and treatment response in anorexia nervosa. J. Abnorm. Psychol. 122, 694 (2013).
Gorwood, P., Duriez, P., Lengvenyte, A., Guillaume, S. & Criquillion, S. Clinical insight in anorexia nervosa: associated and predictive factors. Psychiatry Res. 281, 112561 (2019).
Konstantakopoulos, G. et al. Development and validation of the schedule for the assessment of insight in eating disorders (SAI-ED). Psychiatry Res. 292, 113308 (2020).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Publishing, 2013).
Peng, X., Lau, W. K. W., Wang, C., Ning, L. & Zhang, R. Impaired left amygdala resting state functional connectivity in subthreshold depression individuals. Sci. Rep. 10, 17207 (2020).
Baur, V., Hänggi, J., Langer, N. & Jäncke, L. Resting-state functional and structural connectivity within an insula-amygdala route specifically index state and trait anxiety. Biol. Psychiatry. 73, 85–92 (2013).
Kinnaird, E., Stewart, C. & Tchanturia, K. Taste sensitivity in anorexia nervosa: A systematic review. Int. J. Eat. Disord. 51, 771–784 (2018).
Kaye, W. H., Wierenga, C. E., Bailer, U. F., Simmons, A. N. & Bischoff-Grethe, A. Nothing tastes as good as skinny feels: the neurobiology of anorexia nervosa. Trends Neurosci. 36, 110–120 (2013).
Swinbourne, J. M. & Touyz, S. W. The co-morbidity of eating disorders and anxiety disorders: a review. Eur. Eat. Disord Rev. 15, 253–274 (2007).
Ulfvebrand, S., Birgegård, A., Norring, C., Högdahl, L. & von Hausswolff-Juhlin, Y. Psychiatric comorbidity in women and men with eating disorders results from a large clinical database. Psychiatry Res. 230, 294–299 (2015).
Hamatani, S. et al. Eating disorder neuroimaging initiative (EDNI): a multicentre prospective cohort study protocol for elucidating the neural effects of cognitive–behavioural therapy for eating disorders. BMJ Open. 11, e042685 (2021).
Funding
This work was supported by the Agency for Medical Research and Development (grant number JP19dm0307104) and Japan Society for the Promotion of Science KAKENHI (grant number JP25460884), (grant number JP17K09286) and grants from the Japanese Ministry of Health, Labour and Welfare (H29-nanbyo-ippan).
Author information
Authors and Affiliations
Contributions
Y.Su. - Conceptualization, Data curation, Formal analysis, Visualization, Writing - original draft. R.K. - Data curation, Investigation. T.T. - Data curation, Formal analysis. S.H. - Investigation. N.N. - Investigation. K.M. - Investigation, Resources. Y.Sa. - Conceptualization, Funding acquisition, Investigation, Writing - review and editing. Y.H. - Investigation. T.S. - Investigation. T.M- Investigation. M.Sug. - Supervision. S.F. - Supervision. M.K. - Data curation, Investigation, Writing – review and editing. M.Sun.- Data curation, Investigation, Writing – review and editing. T.N. - Data curation, Investigation, Writing – review and editing. K.T. - Data curation, Investigation, Writing – review and editing. M.I. - Conceptualization, Data curation, Investigation, Writing – review and editing. N.K. - Data curation, Investigation, Resources. S.K. - Investigation, Methodology, Resources. M.T. - Investigation, Resources. H.A. - Writing – review and editing. S.T. - Investigation, Resources. M.G. - Investigation, Resources. K.Y. - Investigation, Resources. Y. M. - Supervision. E.S. - Investigation, Resources. A.S. - Conceptualization, Data curation, Funding acquisition, Investigation, Project Administration, Writing – original draft, Writing – review & editing. Y.H. - Investigation, Methodology, Project administration, Writing – review & editing.
Corresponding author
Ethics declarations
Competing interests
Yoshiya Moriguchi is employed by Lundbeck Japan, KK. All other authors have no conflicts of interest to declare.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sudo, Y., Kamashita, R., Takamura, T. et al. A multicenter cross-sectional study to elucidate altered resting-state functional connectivity of the insular cortex in anorexia nervosa, segmented by functional localization. Sci Rep 15, 19118 (2025). https://doi.org/10.1038/s41598-025-03641-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03641-0
