
Abstract
Heart failure represents a substantial public health challenge, affecting over 64 million individuals worldwide. Effective adherence is essential to enhance patient quality of life and mitigate the risks of hospitalization associated with these progressive conditions. This study aims to assess the magnitude of non-adherence and identify associated factors among Chronic Heart Failure patients receiving follow-up care. A multicenter prospective cross-sectional institutional-based study involving 360 adult CHF patients was conducted from December 2023 to April 2024. Data were systematically collected utilizing a pretested abstraction format. Non-adherence rates were quantized, and multivariate logistic regression analysis was performed to identify significant predictors of non-adherence, with effect size measured by odds ratio. The study identified a non-adherence rate of 17.7% among the cohort. Key factors associated with increased non-adherence include irregular follow-up visits (AOR 1.11, CI 1.06–1.16), presence of orthopnea (AOR 5.02, CI 1.04–12.21), and cor pulmonale (AOR 12.00, CI 1.14–15.30). These findings suggest that experiencing orthopnea and those with irregular follow-ups are markedly more likely to have poor adherence to prescribed therapies. Improving medication adherence through regular follow-up and symptom management is crucial for better outcomes and reducing healthcare burdens in CHF patients.
Similar content being viewed by others
Introduction
Chronic heart failure is a significant public health characteristic issue caused by the heart’s inability to pump blood effectively, resulting in symptoms such as fatigue, dyspnea, and fluid overload1,2. The World Health Organization estimated that CHF covers 64 million people globally, with its prevalence expected to rise as the population ages3. Effective management of CHF is critical; it not only enhances patients’ quality of life but also reduces the risk of hospitalizations and mortality4,5. Pharmacological treatment is central to managing CHF, with a variety of medications available to alleviate symptoms and improve prognosis6,7,8. However, adherence to prescribed regimens remains a persistent challenge9,10,11. A study indicated that the non-adherence rate among CHF patients can range from 23 to 47%11,12. The non-adherence can lead to detrimental health outcomes, including exacerbation of the conditions, an increased rate of hospitalizations, and higher healthcare costs.
Furthermore, studies have linked poor adherence to increased mortality, emphasizing the urgency of addressing the issue12,13. Various factors contribute to non-adherence in CHF patients. Patient-related factors include demographic variables such as age, cognitive functions, and psychosocial conditions like depression and anxiety14,15,16. Older patients in particular may struggle with complex medication regimens due to polypharmacy and cognitive decline17. A lack of understanding regarding the disease and the importance of adherence can significantly influence patients’ behavior, leading them to miss the doses or the complete discontinuity of therapy. Medications-related factors also play a critical role in adherence. Complex dosing schedules, potential side effects, and the burdens of managing multiple medications can discourage patients from the prescribed treatments.
Additionally, healthcare factors such as infrequent follow-up limited access to medications, and insufficient patients’ educations can further exacerbate the adherence issue18. The interplay of these factors creates a complex landscape that healthcare providers must navigate to support their patients effectively19. Ultimately, enhancing adherence among CHF patients is vital not only for individual health outcomes but also for reducing the overall healthcare system20. Non-adherence not only compromises the patient’s health but also leads to increased expenditure and resource utilization21. So, this study aims to assess the magnitude of non-adherence and identify associated factors among CHF patients receiving follow-up care.
Methods
Study setting, period, and design
This multicenter, institutional-based cross-sectional study was conducted from December 1, 2023, to April 30, 2024, to assess medication non-adherence among chronic heart failure (CHF) patients. Data was collected at three hospitals in Northwest Ethiopia: Felegehiwot Comprehensive Specialized Hospital (FHCSH), Tibebe Ghion Comprehensive Specialized Hospital (TGCSH), and Debre Tabor Comprehensive Specialized Hospital (DTCSH).
These hospitals are located as follows:
-
Debre Tabor Comprehensive Specialized Hospital (DTCSH) is situated in Debre Tabor Town, the capital of South Gondar Zone, southwest of Gondar Zone in the Amhara Region, approximately 667 km from Addis Ababa and 100 km from Bahir Dar. Established in 1920, DTCSH serves over three million people as an outpatient and inpatient facility.
-
Felegehiwot Comprehensive Specialized Hospital (FHCSH) is located in Bahir Dar, the capital of the Amhara Regional State, 565 km from Addis Ababa. Founded in 1963, FHCSH provides clinical services to an estimated 7 million people in its catchment area.
-
Tibebe Ghion Comprehensive Specialized Hospital (TGCSH) is located in East Gojjam, about 565 km from Addis Ababa and Bahir Dar. It serves more than 7 million people and offers both outpatient and inpatient care.
The cross-sectional design allowed for the examination of medication non-adherence and its associated factors at a single time point, providing a snapshot of the situation within these hospitals, while the prospective element involved following patients during the study period to capture relevant information. The multicenter approach enhanced the generalizability of the findings by including a more diverse patient population.
Population, inclusion, and exclusion criteria
The study population included all adult patients aged 18 years and older with chronic heart failure who were followed up at the participating hospitals during the study period. Patients were excluded from the study if they refused to participate, died during the study period, or had less than two follow-up visits.
Sample size and sampling technique
The required sample size for this study was calculated using the single population proportion formula, considering a 95% confidence level, a margin of error of 5%, and an estimated prevalence of medication non-adherence of 37%, based on previous regional data11. After adjusting for a 10% non-response rate, the final sample size was determined to be 360 patients.
The total population of chronic heart failure (CHF) patients who began follow-up during the study period across the three hospitals was 3,669. To ensure representativeness from each hospital, proportional allocation was used based on the number of CHF patients in each hospital: Debre Tabor Comprehensive Specialized Hospital (DTCSH) with 1,125 patients, Felegehiwot Comprehensive Specialized Hospital (FHCSH) with 1,673 patients, and Tibebe Ghion Comprehensive Specialized Hospital (TGCSH) with 871 patients.
The proportional sample sizes from each hospital were calculated as follows:
-
DTCSH: (1125 / 3669) × 360 ≈ 110 patients
-
FHCSH: (1673 / 3669) × 360 ≈ 164 patients
-
TGCSH: (871 / 3669) × 360 ≈ 86 patients
To select participants within each hospital, a systematic random sampling technique was employed. This involved the following steps:
-
1.
Compile a complete list of CHF patients registered for follow-up during the study period at each hospital.
-
2.
Calculate the sampling interval (k) for each hospital by dividing the total number of eligible patients by the allocated sample size. For example, at DTCSH, the sampling interval k = 1125/110 ≈ 10.
-
3.
Select a random starting point between 1 and k using a lottery method.
-
4.
Starting from this random starting point, select every kth patient on the list until the required sample size for that hospital is reached.
The baseline total number of heart failure cases for the preceding 5 months of the study period from the registration logbook was allocated to the respondents proportionally within the study areas (Fig. 1).

The schematic representation of the proportional allocation of sample populations.
Study variables
Dependent variable
Non-adherence to heart failure medications.
Independent variables
Independent variables are associated with non-adherence to medications among heart failure patients. Demographic variables included age, sex, residence (rural vs. urban), employment status, marital status, education status, and family history of heart failure. Clinical characteristics encompassed admission unit, NYHA classification and stage of HF, ejection fraction, and the presence of conditions such as acute pulmonary edema, cardiomegaly, hepatomegaly reflux, neck vein distension, orthopnea, a third heart sound, ankle edema, dyspnea on exertion, hepatomegaly, nocturnal cough, and pleural effusion. Additional clinical variables included comorbidities, such as pneumonia, pericardial effusion, and dilated cardiomyopathy. Behavioral factors examined were cigarette smoking status, khat chewing, alcohol consumption, and regular physical activity. Lastly, the study also considered follow-up factors, specifically the pattern of follow-up.
Data collection instruments and procedures
By using a pretested abstraction format, data were collected by three trained nurses. The data abstraction format was prepared by reviewing similar studies. Data regarding demographic variables, medical history, clinical presentation on admission, echocardiographic and laboratory findings, and in-hospital treatment were collected through medical chart review and recorded in the data abstraction format.
Data quality assurance
The data collection instrument format was developed in English, and the collected data was checked for completeness and consistency of information. A pre-test was conducted before the actual data collection days to assess the understandability and applicability of the instrument in a health facility before the main study on 5% of the main sample size. The principal investigator (PI) was regularly reviewed for completeness and summarized on the same day of the data collection.
Data processing and statistical analysis
Data entry was performed using Epi-data V.4.6, and the exported data was analyzed using STATA V.17. For continuous variables, the first normality was assessed using the Shapiro–Wilk’s test. Then parametric continuous data were described with mean and standard deviation, while median and interquartile range (IQR) were employed to describe values of the non-parametric continuous variables. Data on medication non-adherence were collected using the Medication Adherence Rating Scale (MARS-5), which assessed various factors, including demographics and treatment regimens. Adherence was categorized as follows: a score below 20 indicated poor adherence, while a score of 20 or above indicated good adherence22. Statistical analysis was performed in Stata version 17 using a binary logistic regression model. Statistically, significance was determined at p < 0.05, with an adjusted odds ratio (AOR) including crude odds ratios (COR) less than with a p-value of 0.25 for potential determinants factors23. The model’s robustness was evaluated through the Hosmer–Lemeshow test for goodness of fit and assessments of logistic regression assumptions.
Ethics approval and consent to participate
Ethical clearance and approval were obtained from the institutional review board (IRB) of Debre Tabor University (Ref No. 812/2023). Oral informed consent was obtained from the participants after explaining the study objective. Each subject was made aware that engagement was optional and that they could terminate the study at any time if they felt uncomfortable with the questionnaires. The confidentiality of patients is maintained by omitting patient identification and code numbers. All rules and regulations were followed according to the Helsinki Declaration.
Operational definition and definition of terms
-
Non-adherence to medications: The extent to which a patient’s behavior does not coincide with the prescribed treatment plan agreed upon by the patient and the healthcare provider. This may include not taking the prescribed dosage, missing doses, taking medications at the wrong time, or discontinuing medication use without consulting a healthcare provider19.
-
CHF: individual diagnosis of heart failure that persists for at least three months despite optimal medical treatment.
-
Regular follow-up to public hospitals: regular visits by the patients to hospitals’ health care facilities for monitoring and treatment of their CHF.
-
Income levels in Ethiopia can be classified into three categories: Low Income, defined as a monthly income below 1,500 ETB; Middle Income, ranging from 1,500 to 15,000 ETB; and High Income, which encompasses monthly earnings exceeding 15,000 ETB.
-
Cost tiers for medications are classified into three categories: Tier 1, defined as medications priced below 100 ETB; Tier 2, defined as those priced between 100 ETB and 1000 ETB; and Tier 3, defined as medications priced above 1,000 ETB, representing low-cost, middle-cost, and high-cost medications, respectively.
-
Orthopnea: Difficulty in breathing when lying flat, relieved by sitting or standing24.
-
Cor pulmonale: A condition in which the right side of the heart fails due to high blood pressure in the pulmonary arteries, often caused by chronic lung diseases25.
-
Dyspnea on exertion: Shortness of breath that occurs during physical activity.
-
Ankle edema: Swelling in the ankles due to fluid retention, commonly associated with heart failure26.
-
Hepatomegaly: Enlargement of the liver, which can occur due to various conditions, including heart failure27.
-
Pleural effusion: Accumulation of fluid in the pleural space around the lungs, which can cause breathing difficulties28.
-
Neck vein distension: A physical sign where the veins in the neck appear swollen, often indicating increased pressure in the heart29.
-
Third heart sound: An extra heart sound that may indicate heart failure or fluid overload30.
Result
Sociodemographic characteristics
This study revealed a comprehensive analysis of populations’ demographic characteristics and substance use behaviors, focusing on non-adherence to their medications. It revealed that the major population was male 202 (56.11) and the overall mean age was 55 years. In addition, most individuals had an admitted history in a cardiac unit, and in terms of residual address, a significant majority lives in rural areas 278 (77.22%). Likewise, occupational status: farmers are in the most category 138 (38.33%), followed by employers 105 (29.17%). Regarding marital status, it was revealed that most of the participants were married (227 (63.06%), followed by divorced 59 (16.39%). In terms of substance use, the large majority never smoked cigarettes 301 (83.61%), and more than half had a history of drinking alcohol. The mean monthly income of the study participants was 5022 ETB (± 3325.16 SD), with a wide range of socioeconomic status within this participant. From prescribed medications categorization the most common tiers were 257 (71.39%) (Table 1).
Clinical characteristics of chronic heart failure
This study showed insight into heart failure characteristics and associated comorbidity within populations. The current study reported that the majority of participants had reduced ejection fractions of 173 (48.06%), followed by preserved ejection fractions of 143 (39.72%). Likewise, most participants’ chronic heart failure was opposed to de novo heart failure. In terms of functional status, most participants fell into ACC/NYHA class II 311 (86.39%), and most participants were into structural stage C 343 (95.28%). In addition, pulmonary edema 192 (53.33%), cardiomegaly 228 (63.33%), and hepatomegaly 214 (59.44%) were experienced during the follow-up period. Regarding comorbidity, a high prevalence was observed (349, 996.94), reporting at least one comorbidity with the highest comorbidity being ischemic heart disease 125 (34.72%). This study highlights critical aspects of heart failure, reflecting the complexity of managing this population and indicating a need for comprehensive care strategies (Table 2).
Medication use and prescriptions class
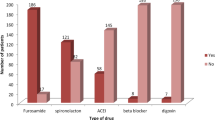
The current study revealed that diuretics 111 (30.85%), ACEI/ARBs 247 (78.41%), and beta blockers 198 (62.86%) were prescribed and refilled during follow-up. While overall ACEI/ARBS and beta blockers were commonly used across the Ethiopian landscape, this implies an area for potential improvements in medication management for this population (Table 3).
ACEI/ARB-angiotensin converting enzyme inhibitors/angiotensin receptor blockers, SGLTI-sodium glucose cotransporters inhibitors
This study reported a range of medications were incorporated into several therapeutic classes, including loop diuretics, ACEI beta blockers, and antiplatelets. In terms of administration routes, significant medications were primarily given per-oral, with furosemide 354 (98%), enalapril 256 (71%), and spironolactone 249 (69%), regarding the cost tiers 1, most medications fell into tiers indicating low cost, and NPH insulin 25 (7%) and UFH 24 (5%) were categorized as tier 2. Additionally, a small number, such as dapagliflozin 59 (16%) were classified in tier 3 as highest highest-cost medications (Table 4).
Self-reported medications adherence
A current study on 360 participants found that a majority of patients rarely or never forget their prescribed medications for heart failure (CHF), with a mean score of 4.02. The study also found that a significant number of participants rarely or never stopped taking their medications for a while, missed their daily dose, or took less than instructed (Fig. 2). The overall MARS-5 adherence score was 21.49, with most participants scoring 20 or higher, indicating adherence, and below 20 was non-adherence (Fig. 3).

MARS-5 descriptive statistics among chronic heart failure patients with follow-up at selected public hospitals in Ethiopia from December 2023 to April 2024 (n = 360). MARS1 = “I forget to take them”. MARS2 = “I alter the dose”. MARS3 = “I stop taking them for a while”. MARS4 = “I decide to miss out a dose”. MARS5 = “I take less than instructed”.

Medication adherence levels based on MARS-5 scores among chronic heart failure patients in Northwest Ethiopia from December 2023 to April 2024 (N = 360).
Predictors of non-adherence
This study revealed that Irregular follow-up emerged as a significant factor, with an AOR of 1.11, CI 1.06–1.116, indicating that irregular follow-up was contributing to non-adherence to prescribed medications. In terms of primary medication payers, insurance had (AOR 1.84, CI 0.58–5.77) and out-of-pocket payers (AOR 1.92, CI 0.54–6.76), although neither significant nor insignificant non-adherences had marginal factors. Regarding orthopnea, participants had clinical orthopnea significantly associated with medication non-adherence 5 times (AOR 5.02, CI 1.04–12.21). Implies that experience orthopnea was more likely to be non-adherent. Similarly, cor pulmonale was associated with non-adherence 12 times (AOR 12.00 CI 1.14–15.30), indicating that it had strong factors for medication non-adherence behaviors in chronic heart failure. Overall, this study highlighted that irregular follow-up, orthopnea, and cor pulmonale were contributing to non-adherence among patients with CHF, indicating potential areas for targeting interventions to improve adherence in this population (Table 5).
Discussion
Main findings and prevalence of medication non-adherence
A multicenter study found that approximately 18% of CHF patients in northwest Ethiopia were non-adherent to their prescribed medications. Key predictors include irregular follow-up visits and clinical factors like orthopnea and cor pulmonale. The majority were male, lived in rural areas, and had reduced ejection fractions. Medication use patterns showed high prescription rates of ACE inhibitors /ARBs, beta-blockers, and mineralocorticoid receptor antagonists. The study suggests multidiscipline care, patient education, and culturally sensitive interventions are essential, and simplified treatment regimens may help reduce pill burden.
Chronic heart failure requires careful management, and adherence to treatment regimens to prevent adverse health outcomes, increased mortality, and hospitalization31,32,33. The current study revealed that 17.7% of CHF patients report non-adherence to their medication, a significant rate compared to previous research indicating a 30% to 50% rate34,35. This contrast is possibly due to patient education or intervention effectiveness, but it highlights the need for targeted interventions like improved patient education.
Behavioral and cognitive challenges of MARS-5
The implications of poor medication adherence can lead to increased disease exacerbations, hospitalizations, and higher mortality rates36,37. The analysis of MARS-5 items revealed that while most participants rarely forget or alter their medication, a significant minority struggle with specific adherence behaviors38. This study revealed that 11.7% of patients with CHF are not taking their prescribed medications as directed, indicating the need for targeted interventions to address the unique barriers faced by these patients and support their treatment regimens39. The study found that non-adherence to medications was high in North Showa and North Gondar, Ethiopia, at 44% and 24%, respectively11,40. The study’s low non-adherence rate of 18% compared to higher rates of 44% and 24% in other studies suggests a need for closer examination due to differences in study populations and settings.
Regional and socioeconomic factors
The current study reports that socioeconomic factors, particularly monthly income and medication cost, significantly influence medication adherence among CHF patients. The mean monthly income in this study participants was around 5022 ETB, reflecting substantial variability in patients’ economic capacity. Medications were categorized into three tiers, low-cost, medium, and high-cost. A significant portion of patients faced the burden of higher-cost drugs, which may adversely affect adherence. Higher medication costs and inadequate insurance coverage significantly contribute to non-adherence among patients41. Non-adherence due to these socioeconomic barriers was associated with worse clinical outcomes, including increased hospitalizations and mortality in heart failure patients11. Interventions aimed at improving adherence should incorporate strategies to reduce the cost burden on patients, such as expanding insurance coverage, enhancing essential medications, and providing socioeconomic support42.
Healthcare system barriers
The finding of this study identified irregular follow-up visits as a critical factor that negatively impacts medication adherence among patients with CHF. Specifically, patients with irregular follow-up visits had an 11% higher likelihood of medication adherence compared to those with regular visits. This underscores the vital roles of consistent follow-up appointments, which provide healthcare providers with essential opportunities to monitor patients’ health, reinforce the importance of adherence, and address any emerging concerns. Regular and frequent follow-ups also enhance communication between patients and healthcare terms, allowing early identification of barriers to adherence such as medication side effects, misunderstanding about regimens, or the emotional challenge of managements CHF. Supporting this, research has consistently shown that structured follow-up care improves patients’ outcomes, and satisfaction, and reduces hospital readmission related to heart failure.
To address these challenges, target interventions are necessary. Patients’ education programs should be enhanced to emphasize the importance of medication adherence and to correct common misconceptions. Implementing structured follow-up protocols including appointments and medication refill reminders can ensure patients receive continuous monitoring and support. Additionally, peer support groups may foster s sense of community among CHF patients, encourage adherence through shared Experience and accountability. Proactive, multicenter strategies, such as patient-centered education, symptom-focused therapies, adherence counseling, and coordinated multipipeline care are essential to improve adherence outcomes in this study population. This approach, supported by previous studies43,44,45,46, can collectively strengthen the support system around CHF patients, and ultimately improve treatment adherence and clinical outcomes.
Patient-related factors
This study identified a significant association between orthopnea and medication adherence in patients with CHF. This is explained by orthopnea is difficulty breathing when lying flat with distressing and important clinical indicators of worsening cardiac function and pulmonary congestion. From a medical perspective, orthopnea reflects elevated left ventricular filling pressures and fluid overload, which necessitate optimized treatment adherence to prevent disease progression. However, the discomfort and anxiety caused by orthopnea can lead patients to avoid medications or healthcare appointments, thereby exacerbating their condition. Addressing orthopnea through targeted education and counseling is therefore essential. A multidisciplinary approach involving cardiologists, pulmonologists, and nursing staff can help develop individualized care plans that effectively manage both heart failure and respiratory symptoms, improving patient comfort and adherence47,48,49,50,51,52,53.
This study also reported that cor pulmonale was a critical factor influencing medication adherence. Medically, cor pulmonale signifies advanced cardiovascular and respiratory compromise, often associated with severe symptoms, complex treatment regimens, and increased risk of morbidity and mortality. From a healthcare perspective, patients with cor pulmonale face multifaceted challenges including cognitive impairment, psychosocial stress, medication side effects, and socioeconomic barriers, all of which can diminish adherence55. Comprehensive care plans that address the underlying pulmonary pathology, optimize pharmacotherapy, encourage lifestyle modifications, coordinate specialist referrals, and strengthen patient support systems are vital to improving adherence and outcomes in this high-risk group. Empowering patients with knowledge and support can improve their confidence in managing their conditions54,56,57,58.
Conclusion and recommendation
This study revealed that, a significant 18% non-adherence rate among chronic heart failure patients, largely due to irregular follow-ups and symptoms like cor pulmonale and orthopnea. It calls for targeted interventions to improve patient education, follow-up care, and address specific symptoms. This multifaceted approach can optimize treatment outcomes and reduce hospitalization.
Strength and limitation
The study on medication non-adherence in chronic heart failure patients in the Northwest Amhara region used a multicenter design, including three major public hospitals, to ensure representativeness and generalizability. The data collection process was comprehensive, capturing demographic, clinical, behavioral, and medication-related variables. However, the study’s reliance on self-reported adherence and cross-sectional design may introduce biases, such as social desirability and recall bias. Self-reported adherence using the MARS-5 scale may lead to an overestimation of adherence due to patients’ tendency to report favorable behaviors. Additionally, the cross-sectional design limits causal inference between predictors and non-adherence, as data were collected at single time points. As recommendations, longitudinal studies to explore temporal and causal relationships. Furthermore, the absence of qualitative data and socioeconomic factors like health literacy and social support may also confound the findings. Future research should incorporate objective adherence measures and mixed-method approaches.
Data availability
Data will be available upon reasonable request from correspondent authors.
Abbreviations
- AOR:
-
Adjusted odds ratio
- ACEI:
-
Angiotensin converting enzyme inhibitor
- AHF:
-
Acute heart failure
- ARB:
-
Angiotensin receptor blocker
- BB:
-
Beta blocker
- CHF:
-
Chronic heart failure
- CI:
-
Confidence interval
- CRVDH:
-
Chronic Respiratory and Vascular Disease Hospital
- DTCSH:
-
Debre Tabor Comprehensive Specialized Hospital
- ETB:
-
Ethiopian Birr
- FHCSH:
-
Felegehiwot Comprehensive Specialized Hospital
- HF:
-
Heart failure
- HR:
-
Heart rate
- IRB:
-
Institutional Review Board
- IQR:
-
Interquartile range
- M:
-
Mean
- MARS:
-
Medication Adherence Rating Scale
- MRA:
-
Mineralocorticoid Receptor Antagonist
- N:
-
Total number of participants
- NYHA:
-
New York Heart Association
- P:
-
Prevalence
- SD:
-
Standard deviation
- SGLTI:
-
Sodium-glucose cotransporter inhibitor
- TGCSH:
-
Tibebe Ghion Comprehensive Specialized Hospital
- LOHS:
-
Length of Hospital Stays
References
McDonagh, T. A. et al. 2023 Focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Wi. Eur. Heart J. 44(37), 3627–3639 (2023).
Yc, W. et al. ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure. J. Am. Coll. Cardiol. 70(6), 776–803. https://doi.org/10.1016/j.jacc.2017.04.025 (2017).
Shahim, B., Kapelios, C. J., Savarese, G. & Lund, L. H. Global public health burden of heart failure: An updated review. Card. Fail. Rev. 9, e11 (2023).
Sapna, F. et al. Advancements in heart failure management: A comprehensive narrative review of emerging therapies. Cureus 15(10), e46486 (2023).
Hafkamp, F. J. et al. Optimal effectiveness of heart failure management—An umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure. Heart Fail. Rev. 27(5), 1683–1748. https://doi.org/10.1007/s10741-021-10212-8 (2022).
Auty, R. Pharmacological management of chronic heart failure in adults: A review of the literature. Malawi Med. J. 16(1), 22–26 (2004).
Marini, M. et al. Acute heart failure: Differential diagnosis and treatment. Eur. Hear J. Suppl. 25(C), C276–C282. https://doi.org/10.1093/eurheartjsupp/suad027 (2023).
Heidenreich, P. A. et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145(18), E895-1032 (2022).
Kassaw, A. T., Sendekie, A. K., Minyihun, A. & Gebresillassie, B. M. Medication regimen complexity and its impact on medication adherence in patients with multimorbidity at a comprehensive specialized hospital in Ethiopia. Front. Med. 6, 1–11 (2024).
Martin, L. R., Williams, S. L., Haskard, K. B. & Dimatteo, M. R. The challenge of patient adherence. Ther. Clin. Risk Manag. 1(3), 189–199 (2005).
Seid, M. A., Toleha, H. N. & Sema, F. D. Medication nonadherence and associated factors among Heart Failure Patients at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. Int. J. Chronic Dis. 2023, 1824987 (2023).
Jarrah, M. et al. Medication adherence and its influencing factors among patients with heart failure: A cross-sectional study. Medicina (Kaunas) 59(5), 85 (2023).
Walsh, C. A. et al. The association between medication non-adherence and adverse health outcomes in aging populations: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 85(11), 2464–2478 (2019).
Poletti, V., Pagnini, F., Banfi, P. & Volpato, E. The role of depression on treatment adherence in patients with heart failure systematic review of the literature. Curr. Cardiol. Rep. 24(12), 1995–2008 (2022).
Dolansky, M. A. et al. Association between poorer cognitive function and reduced objectively monitored medication adherence in patients with heart failure. Circ. Hear Fail. 9(12), e002475. https://doi.org/10.1161/CIRCHEARTFAILURE.116.002475 (2016).
MacMahon, K. M. A. & Lip, G. Y. H. Psychological factors in heart failure: A review of the literature. Arch. Intern. Med. 162(5), 509–516. https://doi.org/10.1001/archinte.162.5.509 (2002).
Liu, J. et al. Risk factors for self-reported medication adherence in community-dwelling older patients with multimorbidity and polypharmacy: A multicenter cross-sectional study. BMC Geriatr. 23(1), 75. https://doi.org/10.1186/s12877-023-03768-7 (2023).
Awad, A., Alhadab, A. & Albassam, A. Medication-related burden and medication adherence among geriatric patients in Kuwait: A cross-sectional study. Front. Pharmacol. 11, 1–13 (2020).
Wu, J. R., Moser, D. K., Lennie, T. A. & Burkhart, P. V. Medication adherence in patients who have heart failure: A review of the literature. Nurs. Clin. North Am. 43(1), 133–153 (2008).
Wideqvist, M., Cui, X., Magnusson, C., Schaufelberger, M. & Fu, M. Hospital readmissions of patients with heart failure from the real world: timing and associated risk factors. ESC Hear Fail. 8(2), 1388–1397 (2021).
Deaton, C. Understanding medication adherence in patients with heart failure: Commentary. Eur. J. Cardiovasc. Nurs. 23(6), e104–e105 (2024).
Andavar, M., Natarajan, M. & Selvam, M. P. Assessment of medication adherence using medication adherence rating scale-5 in patients with major non-communicable diseases at tertiary care hospital. Int. J. Basic Clin. Pharmacol. 9(9), 1412 (2020).
Kupper, L. L., Hosmer, D. W. & Lemeshow, S. Applied regression. J. Am. Stat. Assoc. 85, 901 (1990).
Mukerji, V. Dyspnea, orthopnea, and paroxysmal nocturnal dyspnea. Clin. Methods Hist. Phys. Lab. Exam. 8, 78–80 (1990).
WHO_TRS_213 of 33.pdf.
Abassi, Z., Khoury, E. E., Karram, T. & Aronson, D. Edema formation in congestive heart failure and the underlying mechanisms. Front. Cardiovasc. Med. 9, 933215 (2022).
Xanthopoulos, A., Starling, R. C., Kitai, T. & Triposkiadis, F. Heart failure and liver disease: Cardiohepatic interactions. JACC Hear Fail. 7(2), 87–97 (2019).
Karkhanis, V. S. & Joshi, J. M. Pleural effusion: Diagnosis, treatment, and management. Open Access Emerg. Med. 4, 31–52 (2012).
Chua Chiaco, J. M. S., Parikh, N. I. & Fergusson, D. J. The jugular venous pressure was revisited. Cleve Clin. J. Med. 80(10), 638–644 (2013).
Reddy, P. S. The third heart sound. Int. J. Cardiol. 7(3), 213–221 (1985).
Austin, M. A. et al. Guidelines of the National Heart, Lung, and Blood Institute Working Group on blood drawing, processing, and storage for genetic studies. Am. J. Epidemiol. 144(5), 437–441. https://doi.org/10.1093/oxfordjournals.aje.a008948 (1996).
Virani, S. S. et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 148(9), e9-119. https://doi.org/10.1161/CIR.0000000000001168 (2023).
Seferovic, P. M. et al. Clinical practice update on heart failure 2019: pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 21(10), 1169–1186. https://doi.org/10.1002/ejhf.1531 (2019).
Ho, P. M., Bryson, C. L. & Rumsfeld, J. S. Key issues in outcomes research medication adherence its importance in cardiovascular outcomes. Circulation 119, 3028–3035 (2009).
Ho, P. M., Bryson, C. L. & Rumsfeld, J. S. Medication adherence: Its importance in cardiovascular outcomes. Circulation 119(23), 3028–3035 (2009).
Simpson, S. H. et al. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 333(7557), 15 (2006).
Cutler, D. M. & Everett, W. Thinking outside the pillbox–medication adherence as a priority for health care reform. N. Engl. J. Med. 362(17), 1553–1555 (2010).
Aggarwal, B., Pender, A., Mosca, L. & Mochari-Greenberger, H. Factors associated with medication adherence among heart failure patients and their caregivers. J. Nurs. Educ. Pract. 5(3), 22–27 (2015).
Silavanich, V., Nathisuwan, S., Phrommintikul, A. & Permsuwan, U. Relationship of medication adherence and quality of life among heart failure patients. Hear Lung 48(2), 105–110 (2019).
Hussein, D. et al. Medication adherence and associated factors among chronic heart failure patients on follow-up in north Shewa public hospitals, Oromia region, Ethiopia. BMC Cardiovasc. Disord. 24(1), 444. https://doi.org/10.1186/s12872-024-04090-9 (2024).
Rohatgi, K. W. et al. Medication adherence and characteristics of patients who spend less on basic needs to afford medications. J. Am. Board Fam. Med. 34(3), 561–570 (2021).
Nieuwlaat, R. et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 11, CD000011 (2014).
Aremu, T. O., Oluwole, O. E., Adeyinka, K. O. & Schommer, J. C. Medication adherence and compliance: Recipe for improving patient outcomes. Pharm (Basel, Switzerland) 10(5), 106 (2022).
Tokazewski, J. T., Peifer, M. & Howell, J. T. 3rd. Leveraging and improving refill protocols at your health system. Appl. Clin. Inform. 13(5), 1063–1069 (2022).
Tunje Tanga, A. & Shegaze Shimbre, M. Perspective chapter: The importance of collaborative care in community health settings. In Rijeka (eds Bassanello, M. et al.) (IntechOpen, 2024). https://doi.org/10.5772/intechopen.115212.
Kenis, I., Van Hecke, A. & Foulon, V. The impact of a patient-centered care pathway for patients treated with oral anticancer drugs: A multicentre pre−posttest study in Flanders. J. Eval. Clin. Pract. 6, 10–34 (2024).
Ogungbe, O. et al. Medication adherence interventions for cardiovascular disease in low- and middle-income countries: A systematic review. Patient Prefer. Adher. 15, 885–897 (2021).
Motiwala, S. R. et al. Abstract 18405: Patient-reported orthopnea is associated with worse quality of life across NYHA classes. Circulation 136(1), A18405–A18405. https://doi.org/10.1161/circ.136.suppl_1.18405 (2017).
Celano, C. M., Villegas, A. C., Albanese, A. M., Gaggin, H. K. & Huffman, J. C. Depression and anxiety in heart failure: A review. Harv. Rev. Psychiatry 26(4), 175–184 (2018).
Morton, G., Masters, J. & Cowburn, P. Multidisciplinary team approach to heart failure management. Heart 104, 2016 (2017).
Jaarsma, T. Inter-professional team approach to patients with heart failure. Heart 91(6), 832–838 (2005).
Yancy, C. W. et al. ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 62(16), e147-239. https://doi.org/10.1016/j.jacc.2013.05.019 (2013).
Wu, J. R. & Moser, D. K. Medication adherence mediates the relationship between heart failure symptoms and cardiac event-free survival in patients with heart failure. J. Cardiovasc. Nurs. 33(1), 40–46 (2018).
Humbert, M. et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur. Heart J. 43(38), 3618–3731. https://doi.org/10.1093/eurheartj/ehac237 (2022).
Kassaw, A. T., Sendekie, A. K., Minyihun, A. & Gebresillassie, B. M. Medication regimen complexity and its impact on medication adherence in patients with multimorbidity at a comprehensive specialized hospital in Ethiopia. Front Med. 11, 1369569 (2024).
Ajayi, A. A., Sofowora, G. G. & Ladipo, G. O. Explaining heart failure hyper-mortality in Sub-Saharan Africa: Global genomic and environmental contribution review. J. Natl. Med. Assoc. 112(2), 141–157 (2020).
Bhattad, P. B. & Pacifico, L. Empowering patients: Promoting patient education and health literacy. Cureus 14(7), e27336 (2022).
Paterick, T. E., Patel, N., Tajik, A. J. & Chandrasekaran, K. Improving health outcomes through patient education and partnerships with patients. In Proceedings, vol. 30, 112–3. (Baylor University, Medical Center, 2017).
Acknowledgements
We acknowledge all the data collectors, respective office administrators and patients/care give of all health care center
Funding
The author(s) declare did not get any funding for this research work.
Author information
Authors and Affiliations
Contributions
GYT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Writing—original draft. FND: Project administration, Supervision, Validation, Writing—review & editing. DGD: Methodology, Software, Supervision, Writing—original draft. SSA: Formal analysis, Software, and writing—original draft. TAM: Project administration, Investigation, writing—review & editing. SST: Resources, Visualization, Writing—review & editing. ZAA: Formal analysis, Software, Writing—review & editing. BEB: Data curation, Investigation, Project administration, Resources, Visualization, Writing—review & editing MFS- Software, Supervision, Methodology, Writing—review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tarekegn, G.Y., Dagnew, F.N., Moges, T.A. et al. Medication non-adherence and its predictors among chronic heart failure patients in Northwest Amhara region. Sci Rep 15, 19968 (2025). https://doi.org/10.1038/s41598-025-03748-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03748-4
