
Abstract
As the recommended drugs for first-line regimens in HIV-1 infections, reverse-transcriptase inhibitors (RTIs) are widely used around the world. To escape from the selective pressure imposed by RTIs, HIV-1 constantly mutates to adapt to its environment. However, it is unclear how resistance mutations emerging in response to RTIs affect drug susceptibility in strains of different subtypes. To explored this phenomenon, typical RTI-induced drug resistance mutations (DRMs) were selected to test their effects on the susceptibility of different subtype strains. The same RTI-induced DRMs were introduced into infectious clones of subtypes B and CRF01_AE, and phenotypic resistance tests were performed to compare the differences in susceptibilities to various RTIs. The experimental results revealed that mutations such as M41L and V106M were more likely to occur in the CRF01_AE subtype. However, phenotypic analysis of reconstructed clones containing these resistance mutations revealed that CRF01_AE exhibited significantly lower sensitivity to RTIs than did subtype B. For azvudine (FNC), a novel nucleoside reverse transcriptase inhibitor (NRTI), the resistance level of CRF01_AE was significantly lower than that of subtype B. In conclusion, the same mutation affecting resistance to RTIs can have significantly different impacts depending on the subtype of the HIV-1 strain. This finding serves as a reference for guiding rational drug use in the future. Moreover, relying solely on phenotypic experimental results from subtype B to evaluate resistance levels of unclear mutations in other subtypes may be inappropriate and should be approached with caution.
Similar content being viewed by others


Introduction
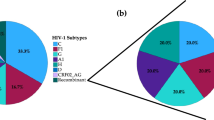
HIV is characterized by high mutation, replication and recombination rates, which lead to its rich genetic polymorphism1. Previous studies have divided HIV into groups, subtypes and sub-subtypes based on phylogenetic analysis to distinguish different genetic background variants2,3. HIV-1 is prevalent worldwide, and the prevalent strains vary widely between countries and regions, with subtype B dominating in high-income regions such as the United States and Western Europe, whereas the proportion of circulating recombinant form (CRF) is very high in some regions4. In China, a wide variety of CRFs and novel recombinant viruses continue to emerge. An analysis of 31 provinces in China revealed that the CRF01_AE strain, which accounted for 32.1% of HIV-1 infections from 2004 to 2023 and was widely distributed in all regions of China, has become one of the dominant epidemic strains in China5.
At present, viral replication is controlled mainly by lifelong antiretroviral therapy (ART), and there is no effective and widely available cure. In 2023, 77% [61–89%] of people living with HIV received antiretroviral therapy, which represented an increase over the previous year6. Studies have shown that factors such as HIV-1 gene mutations and poor drug-regimen compliance severely affect the therapeutic results of ART against HIV, which can lead to ART treatment failure7,8. According to the China CDC weekly report, the overall incidence of primary drug resistance in China increased significantly from 2.6% in 2004–2007 to 7.8% in 2020–2022, which represented a moderate increase9. Therefore, it is very important to detect drug resistance before treatment, as it can be an important reference for clinicians to adjust the treatment regimen over time. Although most of the drugs recommended for ART are based on experimental data from subtype B, their associated treatment regimens have been extended to endemic areas such as China where non-B subtypes predominate10. Therefore, research currently focuses on issues such as assessing disease progression, evolution of drug resistance, and treatment efficacy in different subtypes of HIV-1.
The effects of different subtypes on therapeutic outcomes have been extensively studied. Owing to the influence of HIV gene polymorphisms, the propensity to develop resistance mutation sites varies between subtypes under the selective pressure of drugs11,12,13. For example, compared with other subtypes, HIV-1 subtype C viruses are more likely to develop K65R-mediated resistance to tenofovir11. However, these major resistance mutation sites may also interact with other subtype-specific domains, leading to the development of significantly varying levels of resistance14. Therefore, the drug susceptibility conferred by the same DRM to non-subtype B strains is not well defined at present. In this study, we selected typical major resistance mutations induced by RTIs to investigate whether there is a significant difference in the activity of RTIs when they emerge in subtypes B and CRF01_AE. These findings will provide additional experimental data to support HIV prevention and treatment in areas where CRF01_AE is endemic and reference values for the selection and implementation of ART.
Materials and methods
HIV-1 infectious cloning plasmid
The wild-type infectious cloning pNL4-3 plasmid of HIV-1 subtype B was kindly provided by Professor Shan Lu of the University of Massachusetts Medical School, USA. The wild-type infectious cloning plasmid pGX002 of CRF01_AE is a full-length genomic infectious clone of the HIV-1 CRF01_AE strain, which was constructed by the local laboratory of the Academy of Military Medical Sciences15. Both plasmids are suitable for packaging infectious virus particles and contain an ampicillin resistance gene.
Reverse transcriptase inhibitors
The following drugs were purchased from Selleck Company in powder form and had purities greater than 99.8%: zidovudine (AZT, Cat. No. S2579), lamivudine (3TC, Cat. No. S1706), tenofovir disoproxil fumarate (TDF, Cat. No. S1400), abacavir (ABC, Cat. No. S3165), emtricitabine (FTC, Cat. No. S1704), nevirapine (NVP, Cat. No. S1742), etravirine (ETR, Cat. No. S3080) and efavirenz (EFV, Cat. No. S4685). FNC was kindly provided by Genuine Biotech Limited. All drugs were dissolved in dimethyl sulfoxide and diluted to 10 mM in phosphate buffered saline (PBS) (Gibco, Cat. No. 10010002).
Cell culture
The human embryonic kidney 293T (HEK293T) cell line is commonly used to package lentiviruses, and expression plasmids containing the full-length HIV-1 genome are transfected into these cells to obtain stable infectious HIV-1 viruses16. This cell line was purchased from the American Type Culture Collection (ATCC) in 2017 and was maintained after culture expansion and preservation. TZM-BL cells carry a fluorescein reporter gene regulated by the HIV-1 tat element, and the infection and replication efficiency of HIV-1 can be evaluated by assessing the expression of luciferase according to this property17. This cell line was kindly provided by Professor Shan Lu, University of Massachusetts Medical School, USA. Both cell lines were cultured in Dulbecco’s modified Eagle’s medium (DMEM, Gibco, Cat. No. 26010074) supplemented with 10% fetal bovine serum (Gibco, Cat. No. 26010074) and 1% penicillin-streptomycin (Gibco, Cat. No. 2199828). The cells were passaged every 3‒4 days and maintained at 37 °C under 5% CO2 in a cell incubator.
Selection of RTI DRMs
The HIV-1 CRF01_AE and subtype B Pol region sequences were downloaded from the HIV Sequence Database (https://www.hiv.lanl.gov/) according to the following criteria: (1) from database creation to December 31,2023; (2) country labeled as CN (China) or US (United States); (3) complete information (geographic location, year the sequence was sampled, earliest sequence taken from same subject) available; and (4) contained the Pol region. The genotype resistance analysis was performed by uploading the Stanford HIV Drug Resistance Database (https://hivdb.stanford.edu/) after trimming with BioEdit v7.2.5 software alignment. In this study, the top five drug resistance sites were selected through a combination of the Stanford HIV Drug Resistance Database and its drug resistance interpretation tool. A single site of the circulating RTI DRMs was introduced into HIV-1 infectious cloning plasmids by site-directed mutagenesis for in vitro phenotypic drug susceptibility testing.
Construction of infectious clones containing resistance mutation sites
Site-directed mutagenesis containing resistance sites was performed on HIV-1 pNL4-3 and pGX002 using the Q5® Site-Directed Mutagenesis Kit (NEB, Cat. No. E0554S) in accordance with the manufacturer’s instructions18. The primer sequences and annealing temperatures were generated by the official NEB tool NEBaseChanger™ (https://nebasechanger.neb.com/). The mutants were transformed into Stabl3 competent cells (TransGen, Cat. No. CD521-02) and inoculated on LB agar plates containing ampicillin (100 µg/ml; TransGen, Cat. No. GG101-01) for amplification. Positive clones were picked and amplified in LB broth containing ampicillin, followed by Sanger sequencing (by SinoGenoMax). The plasmids containing the resistance sites were extracted with the Endotoxin-Free Plasmid Small Extraction Medium Kit (TIANGEN, Cat No. DP118-02). The wild-type and drug-resistant plasmids were stored in a freezer at -20 °C in preparation for packaging the corresponding virus.
Packaging of HIV-1 derived viruses and TCID50 determination
Eight million HEK293T cells were plated in 10-cm cell culture dishes, 10 ml of medium was added, and the cells were cultured overnight to 70–90% confluence. One hour before transfection, the medium was changed to nonresistant medium, 25 µg of the plasmid and 70 µl of Lipofectamine™ 2000 were each diluted to 125 µl with Opti-MEM (Gibco, Cat. No. 31985070), and the mixed plasmid and liposomes were co − transfected into cells after incubation at room temperature for 20 min. The transfected cell culture dishes were transferred to a BSL-3 laboratory and cultured in a cell constant temperature incubator at 37 °C and 5% CO2 for 48 h. The culture supernatants were collected and stored in a − 80 °C freezer.
The virus was gradient diluted in transparent 96-well plates. The virus was diluted 10-fold as the highest concentration, and then a 3-fold gradient was used to dilute the virus to well 7, with the last well used as a blank control. The diluted virus was added to 96-well containing with TZM-bl cells, with four replicate wells for each virus dilution. After incubation for 48 h in a thermostatically controlled cell incubator, the relative luminescence units (RLU) of the cells were determined on an EnSpire plate reader by adding a Bright-Glo fluorescence mixture (Promega, Cat. No. E2650). With 2.5 times the RLU of the blank control wells used as the cut-off, a well was considered positive when the RLU of the test well was greater than the cut-off. Median tissue culture infective dose (TCID50) values were calculated for each virus strain according to Eqs. (1) and (2).
Assessment of the phenotypic resistance of HIV-1 strains to RTIs
All nine drugs used in the experiment had a maximum final concentration of 1 mM and were then sequentially diluted in a 5-fold gradient series to a minimum final concentration of 0.02 nM. Gradient diluted drugs were added to a 96-well plate containing 9900 TZM-bl cells per well, with 2 duplicate wells for each drug. After 48 h of incubation in a constant-temperature incubator, CellTiter-Glo® (Promega, Cat. No. G7573) was added to assess cell viability to confirm the cytotoxicity of each drug.
Each drug was diluted to the working concentration. The gradient diluted drug and 200 TCID50 of virus were added to a 96-well plate containing 9900 TZM-bl cells per well, with two duplicate wells for each drug and virus, and the experiment was repeated three times. After incubation in a thermostatic incubator for 48 h, the Bright-Glo fluorescence mixture was added, the relative chemiluminescence of the cells was determined on an EnSpire multiplate reader, and the half maximal inhibitory concentration (IC50) value was calculated with GraphPad Prism v9.0.0.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics 25 (SPSS v25.0) to calculate the mean and standard deviation of the IC50 from triplicate experiments for each drug and strain, and the Shapiro‒Wilk test was used to confirm that the data followed a normal distribution. The multiplicity of the IC50 of the resistant strain relative to the wild-type strain was calculated as the fold change (FC). The FC classifications were as follows: susceptible, ≤ 4 FC; resistant, > 4 to 10 FC; and high-level resistance, > 10FC19. In GraphPad Prism v9.0.0, the effect of the same resistance mutation on antiretroviral activity between genetic backgrounds of different subtypes was assessed by a parametric unpaired Student’s t-test with Welch’s correction, which does not assume equal standard deviations.
Results
Screening of DRMs associated with RTIs
A total of 8654 subtype B sequences (76.36% from the USA) and 10,551 CRF01_AE sequences (0.07% from the USA) were obtained after sorting and were sampled from 1978 to 2023. In subtype B, the top five prevalent mutation sites for NTRI were as follows: 184 (17.40%), 215 (15.24%), 41 (10.77%), 67 (9.33%) and 219 (7.15%) for NRTI DRMs. For non-nucleoside reverse transcriptase inhibitor (NNRTI)the most prone to developing resistance were 103 (11.61%), 181 (4.63%), 190 (3.37%), 106 (2.40%) and 138 (2.36%). In CRF01_AE, the top five mutation sites for NRTI DRMs were: 68 (6.45%), 184 (2.26%), 67 (0.86%), 215 (0.75%), and 65 (0.68%). With respect to mutations associated with resistance to NNRTIs, the most prevalent sites were 179 (5.27%), 106 (2.46%), 103 (1.54%), 190 (1.20%), and 181 (1.16%). Because mutations at positions 219 and 68 alone did not confer significant resistance, these two resistance sites were excluded from this study. Finally, a total of eight major RTI drug–resistance mutations, M41L, K65R, D67N, M184V, T215Y, K103N, V106M, and G190A, were successfully introduced into infectious cloning plasmids to construct drug–resistant recombinant viruses. The mutation primer sequences and annealing temperatures are detailed in Table S1. The NCBI repository accession numbers for the AE/B recombinants are: PQ735970–PQ735985.
RTIs technical cut-off and fold change classifications
The baseline in vitro phenotypic susceptibilities of the wild-type subtype B (NL4-3) and CRF01_AE (GX002) strains to RTIs were calculated with GraphPad Prism v9.0.0 and are detailed in Table 1. An standard error of mean (SEM) of 0.00 indicates a value of less than 0.001. Among the NRTIs, FNC had a much lower baseline value than that of other NRTIs, and the IC50 of FNC was 10− 4 nM (NL4-3WT IC50 = 0.0002673 nM; GX002WT IC50 = 0.000273 nM) regardless of the subtype. This value was 10,000 times lower than the IC50 value of AZT, which was the next most potent NRTI. There was no significant difference in the baseline IC50 between subtype B and CRF01_AE for the same drug (p > 0.05) (Table 1).
Susceptibility of single DRMs to NRTIs
The IC50 and FC values of the NL4-3 and GX002 recombinant strains containing single NRTI DRMs treated with NRTIs are detailed in Table S2; the phenotypic resistance results were basically consistent with the predictions of the Stanford HIV resistance database, although the phenotypic resistance results of GX002 revealed several contradictions.
GX002M41L was significantly less sensitive to AZT, TDF, and ABC than NL4-3M41L was (Table 2), but its level of resistance classification did not differ (Fig. 1). However, it should be noted that for ABC, NL4-3M41L showed increased sensitivity (FC = 0.75 ± 0.004), but GX002M41L did not show increased sensitivity (FC = 1.20 ± 0.08), which was maintained a slightly higher level than that of the wild-type strain (GX002WT) (Fig. 1). Compared with NL4-3, GX002K65R was significantly more sensitive to TDF and less sensitive to FTC (Table 2). However, there was no difference in the classification of the level of resistance between the two subtypes (Fig. 1). The sensitivity of GX002T215Y to TDF was significantly lower than that of NL4-3, and there was no significant difference in the level of resistance to TDF. The ABC results were paradoxical. Although both subtypes of the T215Y mutant recombinant virus strains were sensitive to ABC, GX002T215Y exhibited an increased sensitivity to ABC (FC = 0.53 ± 0.002) (Fig. 1c).
As a novel antiviral drug, FNC is clearly distinct from other NRTIs. The five resistance mutations tested were all significantly more sensitive to FNC in the context of GX002 than in the context of NL4-3 (Table 2), but their levels of resistance did not differ (Fig. 1e). 3TC also exhibited unique characteristics; except for M184V, which had a FC beyond the detection range because of an excessive level of resistance, the other resistance sites had significantly higher FCs in the context of GX002 than in the context of NL4-3 (Table 2). Moreover, the level of resistance of GX002K65R, GX002D67N, and GX002T215Y was significantly greater than that of the corresponding recombinant strains of NL4-3(Fig. 1f). In addition, except for M41L, there were notably no significant differences in FC values for AZT when subtype B carried the same resistance mutation as CRF01_AE did (Table 2).

NRTIs susceptibility of single NRTI DRMs. Green areas indicate susceptibility to the corresponding drug, yellow indicates resistance, and red areas indicate high resistance. NRTIs: nucleoside reverse transcriptase inhibitors, DRM: drug resistance mutation.
Susceptibilities of strains with single NNRTI DRMs to NNRTIs
The IC50 values and FCs of NL4-3 and GX002 recombinant strains containing single NNRTI DRMs treated with NNRTIs are detailed in Table S3. The in vitro phenotypic resistance results obtained in this experiment were in general agreement with the predictions of the Stanford HIV resistance database, but there were still notable inconsistencies.
Although there were significant differences in FCs between different subtypes with the K103N mutation for NVP and EFV and with the V106M mutation for NVP (K103N for NVP, p = 0.0039; K103N for EFV, p = 0.0025; V106M for NVP, p = 0.0039), the level of resistance was considered highly resistant regardless of the subtype (Fig. 2a, b), which was consistent with the Stanford HIV Resistance Database prediction. Although the two subtypes with the K103N mutation differed in FC when treated with ETR (p = 0.0241), both were sensitive to ETR, but the two subtypes with the V106M mutation clear differed in sensitivity to ETR (p = 0.0147). NL4-3V106M was sensitive to ETR (FC = 2.23 ± 0.03), but GX002V106M was resistant to ETR (FC = 7.93 ± 1.21) (Fig. 2b). In addition, CRF01_AE with the G190A mutation was significantly more resistant to NVP, EFV, and ETR than subtype B with the same mutation (NVP, EFV, p < 0.0001; ETR, p = 0.0027), but its degree of resistance classification did not differ (Fig. 2).

NNRTIs susceptibility of subtypes with single NNRTI DRMs. The green areas indicate susceptibility to the corresponding drug, the yellow areas indicate resistance, and the red areas indicate high resistance. NNRTI: non-nucleoside reverse transcriptase inhibitor, DRM: drug resistance mutation.
Discussion
Previous studies have shown that different subtypes have different propensities to generate resistance mutation sites, for example, CRF01_AE is more likely than subtype B to generate thymidine analog mutations (TAMs)20. In the presence of TAMs, CRF01_AE exhibits greater AZT resistance than subtype B. This is primarily because wild-type CRF01_AE usually contains the polymorphic resistance sites G335D and A371V and contains A400T, which can affect the resection efficiency of AZT-5’-monophosphate (AZTMP) termination by the RNA template strand21,22. The GX002 infectious clone of wild-type CRF01_AE used in this experiment was found to contain G335D and A371V and had a threonine at position 400. However, the NL4-3 infectious clone of wild-type B used in this experiment did not contain G335D or A371V and had alanine at position 400. When CRF01_AE contained M41L, it was more resistant to most drugs, with the exception of FNC, than subtype B. This finding suggests that the resistance level of a person infected with a CRF01_AE strain containing the M41L resistance mutation site may be significantly underestimated when it is determined by the subtype B criteria. This may be somewhat misleading for drug selection and counseling of the infected individuals. However, the resistance site mutations of T215Y and D67N did not confer a difference in the level of resistance to AZT between the two subtypes. The presence of the T215Y resistance site can increase the susceptibility to ABC when it exists alone in CRF01_AE. However, in general, T215Y usually coemerges with M41L and L210W23, and its mechanism of action needs to be further explored.
The results of this study are consistent with those of previous studies showing that the K65R resistance mutation site is significantly more common in CRF01_AE than in subtype B and that S68G often cooccurs with K65R11,24,25. However, S68G only acts as a compensatory mutation, which improves the replication ability of the K65R mutant and does not affect sensitivity to NRTIs24. The GX002 and NL4-3 plasmids used in this study did not contain the S68G mutation. When CRF01_AE contained K65R alone, it was less sensitive to 3TC and FTC but more sensitive to TDF and FNC than subtype B was, and its mechanism of action has not yet been studied in detail.
In addition, two NRTIs, 3TC, FNC were notable in this study. With the exception of M184V, the other NRTI DRMs evaluated in this study conferred a greater level of 3TC resistance to CRF01_AE than to subtype B. This observation may suggest that 3TC exerts a comparatively diminished therapeutic effect on CRF01_AE compared with subtype B. This finding also suggests that we should be more cautious when assessing the level of resistance of CRF01_AE to 3TC. For FNC, regardless of the resistance mutation site, the level of resistance in CRF01_AE was significantly lower than that in subtype B. The resistance to FNC was more than 500-fold greater than that in the wild type regardless of the subtype or resistance mutation site. Therefore, follow-up experiments are needed to confirm its resistance site. This may be because FNC has a much lower baseline than the other NRTIs do, and the IC50 of FNC was 10− 4 nM (NL4-3WT IC50 = 0.0002673 nM; GX002WT IC50 = 0.000273 nM) regardless of the subtype. This value was 10,000 times lower than the IC50 of AZT, which was the next most potent NRTI, and thus, it remains to be debated whether the cut-off value currently used for resistance levels is applicable to this emerging NRTI.
In NRT-treated patients infected with subtype C virus, the mutation rate of K103N was found to be lower than that in patients infected with other subtypes25, and the results of the analysis in this present study were consistent with this finding. K103N, when present alone, conferred greater EFV, NVP and ETR sensitivities to CRF01_AE than to subtype B. This finding suggests that the likelihood of mutation at a resistance site in a subtype is correlated with its level of resistance. This was also demonstrated by V106M. Compared with subtype B, CRF01_AE was more susceptible when carrying V106M in the results of this study, and when V106M was present alone in CRF01_AE, it also conferred a greater level of NVP, ETR, and EFV resistance. In contrast, the G190A mutation was slightly less likely to be present in CRF01_AE than in subtype B, but it conferred a level of resistance to NNRTIs that was greater than that of subtype B. However, there was no difference in the overall resistance classification between the two subtypes.
This study offers some degree of support for the hypothesis that the genetic background of different subtypes may affect the resistance level of DRMs to the corresponding drugs. However, this study is not without its limitations. First, the vector used in this study was a single infectious cloning plasmid, and only single point mutations were investigated. Additionally, possible differences were investigated only at the cellular level in vitro. Therefore, further investigation is necessary to determine the effects of combined mutations on resistance levels in a more diverse genetic background. The use of an in vivo animal model, such as treating humanized mice infected with HIV with ART, in subsequent studies would better mimic the in vivo system of HIV-infected individuals with functional immune pressure.
In conclusion, this study revealed that the same drug-resistant mutations exhibited differences in various subtype strains, and therefore, it is not suitable to use the same skeletal virus for evaluating the performance of the same mutation on various subtype strains. As transmissible drug resistance becomes more prevalent, there is an increasing need for pretreatment resistance testing26, which necessitates the provision of an accurate resistance assay. Presently most established genotype and phenotype tests are based on experimental data from subtype B and such tests have been promoted widely in many laboratories. However, the results of this study suggest that this approach is no longer scientifically sound. Therefore, there is an urgent need to develop subtype-specific genotype and phenotype assays to provide more accurate estimates of clinical resistance.
Data availability
The sequences generated during the current study are available in the NCBI repository, PQ735970-PQ735985. Additional data are available in the supplementary material.
References
Abram, M. E. et al. Nature, position, and frequency of mutations made in a single cycle of HIV-1 replication. J. Virol. 84 (19), 9864–9878 (2010).
Mansky, L. M. & Temin, H. M. Lower in vivo mutation rate of human immunodeficiency virus type 1 than that predicted from the fidelity of purified reverse transcriptase. J. Virol. 69 (8), 5087–5094 (1995).
Ndung’u, T. & Weiss, R. A. On HIV diversity. Aids 26 (10), 1255–1260 (2012).
Hemelaar, J. et al. Country level diversity of the HIV-1 pandemic between 1990 and 2015. J. Virol. 95(2) 10–1128 (2020).
Dong et al. Vital surveillances: National and regional molecular epidemiology of HIV-1 China, 2004–2023. China CDC Wkly. 6 (48), 1257–1263 (2024).
Organization, W. H. HIV data and statistics. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics (2024).
Hashempour, A. et al. Predictors of antiretroviral treatment failure to the first line therapy: A cross-sectional study among Iranian HIV-positive adults. BMC Infect. Dis. 24 (1), 358 (2024).
Kapustin, D. V. et al. Patterns of HIV-1 drug resistance among HIV-infected patients receiving first-line antiretroviral therapy in Novosibirsk region, Russia. J. Glob. Antimicrob. Resist. 35, 1–5 (2023).
Liu, X. et al. Changes in HIV-1 subtypes/sub-subtypes, and transmitted drug resistance among ART-naïve HIV-infected individuals–China, 2004–2022. China CDC Wkly. 5 (30), 664–671 (2023).
Organization, W. H. Treat all: Policy adoption and implementation status in countries. World Health Organization: (2017). Available from:https://iris.who.int/handle/10665/258538.
Brenner, B. G. et al. HIV-1 subtype C viruses rapidly develop K65R resistance to tenofovir in cell culture. Aids. 20(9), F9–F13 (2006).
Cilento, M. E. et al. HIV-1 resistance to Islatravir/tenofovir combination therapy in wild-type or NRTI-resistant strains of diverse HIV-1 subtypes. Viruses 15(10), 1990 (2023).
Reddy, N. et al. K103N, V106M and Y188L significantly reduce HIV-1 subtype C phenotypic susceptibility to doravirine. Viruses 16(9), 1493 (2024).
Huang, A. et al. Global comparison of drug resistance mutations after first-line antiretroviral therapy across human immunodeficiency virus-1 subtypes. Open. Forum Infect. Dis. 3 (2), ofv158 (2016).
Jia, D. The Molecular Epidemiological Study on HIV Prevalent in Shenzhen and Construction of Infectious Clone of Dominant Strainin in China (Anhui Medical University, 2017).
Lee, M. J. & Park, J. H. Pathway analysis in HEK 293T cells overexpressing HIV-1 Tat and nucleocapsid. J. Microbiol. Biotechnol. 19 (10), 1103–1108 (2009).
Sun, J. et al. Detection of phenotypic drug-resistance of HIV-1 strains by TZM-bl cell lines in China. Chin. J. AIDS STD. 14 (5), 439–449 (2008).
Dickinson, D. J. et al. Engineering the Caenorhabditis elegans genome using Cas9-triggered homologous recombination. Nat. Methods. 10 (10), 1028–1034 (2013).
Xu, M. et al. Clinical detection of HIV-1 drug resistance using a novel HIV-1 phenotypic resistance system. Virol. Sin. 4, p8 (2014).
Santoro, M. M. et al. Comparative analysis of drug resistance among B and the most prevalent non-B HIV type 1 subtypes (C, F, and CRF02_AG) in Italy. AIDS Res. Hum. Retroviruses. 28 (10), 1285–1293 (2012).
Delviks-Frankenberry, K. A. et al. Subtype-specific differences in the human immunodeficiency virus type 1 reverse transcriptase connection subdomain of CRF01_AE are associated with higher levels of resistance to 3’-azido-3’-deoxythymidine. J. Virol. 83 (17), 8502–8513 (2009).
Tanuma, J. et al. Impact of CRF01_AE-specific polymorphic mutations G335D and A371V in the connection subdomain of human immunodeficiency virus type 1 (HIV-1) reverse transcriptase (RT) on susceptibility to nucleoside RT inhibitors. Microbes Infect. 12 (14–15), 1170–1177 (2010).
Boyer, P. L. et al. Analysis of the Zidovudine resistance mutations T215Y, M41L, and L210W in HIV-1 reverse transcriptase. Antimicrob. Agents Chemother. 59 (12), 7184–7196 (2015).
Li, S. et al. The S68G polymorphism is a compensatory mutation associated with the drug resistance mutation K65R in CRF01_AE strains. BMC Infect. Dis. 20 (1), 123 (2020).
Lam, E. P. et al. Antiretroviral resistance after First-Line antiretroviral therapy failure in diverse HIV-1 subtypes in the SECOND-LINE study. AIDS Res. Hum. Retroviruses. 32 (9), 841–850 (2016).
Johnson, J. A. et al. Minority HIV-1 drug resistance mutations are present in antiretroviral treatment-naïve populations and associate with reduced treatment efficacy. PLoS Med. 5 (7), e158 (2008).
Acknowledgements
The authors thank all of the participants and peer workers.
Funding
The financial support in this study derived from the National Key Research and Development Program of China under Grant numbers (2022YFC2304903,2022YFC2305202,2022YFC2304403), the National Natural Science Foundation of China under Grant number (82173583), and Science and Technology Program of Shijiazhuang (231200103 A).
Author information
Authors and Affiliations
Contributions
Conceptualization, L.L. and H.Y.; methodology, H.L. and J.H.; formal analysis, K.S. Y.L. and L.Z.; investigation, X.L. L.J.; resources, L.L. H.L.; data curation, K.S. B.Z.; software, X.W. writing—original draft preparation, K.S.; writing—review and editing, H.L. L.L. H.Y.; visualization, J.L.; project administration, H.L. H.Y. and L.L.; funding acquisition, H.L. L.L. JLand E.D. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, H., Shen, K., Han, J. et al. In vitro comparison of the susceptibilities of the same drug resistance mutations to reverse-transcriptase inhibitors of subtype B and CRF01_AE HIV-1 strains. Sci Rep 15, 35936 (2025). https://doi.org/10.1038/s41598-025-04144-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-04144-8
