
Abstract
Cardiovascular and metabolic diseases–specifically myocardial infarction, congestive heart failure, cerebrovascular disease, peripheral vascular disease, renal disease, and liver disease–are major public health concerns worldwide. However, studies examining how these diseases modify the relationship between long-term PM2.5 exposure and mortality remain scarce. Using a Cox regression model with a population-representative cohort from South Korea, we estimated the modifying effects of six major cardiovascular and metabolic diseases on PM2.5-mortality association in two cohorts: (1) individuals without underlying diseases (NoUD) and (2) those with only hypertension and/or diabetes (HTN/DM). The interaction between PM2.5 and each disease onset was used to estimate effect modification, with results presented as relative hazard ratios (RHRs) per 10 µg/m3 increase in PM2.5. Among 183,834 subjects, non-accidental deaths occurred in 18.0% of the NoUD (N = 134,584) and 25.7% of the HTN/DM (N = 49,250). In the NoUD cohort, renal disease (RHR: 1.58; 95% CI: 1.27–1.97), myocardial infarction (1.41; 1.15–1.73), and liver disease (1.40; 1.25–1.57) significantly modified the effect of PM2.5 on mortality. In the HTN/DM cohort, renal disease (1.74; 1.43–2.12), myocardial infarction (1.62; 1.29–2.05), and cerebrovascular disease (1.32; 1.17–1.51) showed higher RHRs. Our findings highlight the importance of consistent and preemptive care for renal disease and myocardial infarction and provide evidence for target-specific interventions to reduce the risk of PM2.5 on mortality.
Similar content being viewed by others

CCI, Charlson comorbidity index; CHF, congestive heart failure; CI, confidence interval; CPD, chronic pulmonary disease; CBVD, cerebrovascular disease; CVD, cardiovascular diseases; DM, diabetes mellitus; RHR, relative hazard ratio; HTN, hypertension; HTN/DM, individuals with only hypertension and/or diabetes mellitus during the screening; ICD-10, International Classification of Diseases, 10th revision; IHD, ischemic heart disease; LIVER, liver disease; MI, myocardial infarction; NHIS-NSC, National Health Insurance Service-National Sample Cohort; NoUD, individuals without major underlying cardiovascular and metabolic-related diseases, hypertension, or diabetes during the screening; PVD, peripheral vascular disease; RENAL, renal disease; RR, risk ratio; SD, standard deviation; WHO, World Health Organization.
Introduction
Cardiovascular and metabolic diseases have emerged as major global health challenges, imposing a considerable burden on individuals, healthcare systems, and societies. According to the World Health Organization (WHO), ischemic heart disease (IHD) and stroke were the two leading causes of death worldwide in 20191. These diseases rank second and fourth in South Korea (henceforth referred to as Korea), following cancer and pneumonia, respectively2. The worldwide prevalence of hypertension (HTN) in 2019 was 33.1%, and diabetes mellitus (DM) resulted in approximately 2.0 million deaths globally3. Moreover, previous studies reported that the intricate interplay between cardiovascular diseases (CVDs) and metabolic syndromes further amplifies mortality risk4.
Long-term exposure to PM2.5 (fine particulate matter with a diameter ≤ 2.5 μm) has been widely associated with elevated risks of cardiovascular and metabolic-related morbidity and mortality5, and a causal relationship between PM2.5 exposure and mortality has been examined6. In a review study, a 10 µg/m3 increase in long-term PM2.5 exposure was associated with an elevated risk of 23% for IHD mortality, 24% for cerebrovascular mortality, 13% for incident stroke, and 8% for incident myocardial infarction7. In a US Medicare cohort study examining PM2.5 and cause-specific mortality, cardiovascular mortality exhibited the highest risk ratio (RR) at 1.56, whereas respiratory mortality had a RR of 1.248. Associations between PM2.5 exposure and mortality related to metabolic diseases, such as diabetes, kidney disease, and liver disease, have also been reported9,10.
Previous studies have reported that inhalation of PM2.5 can induce pulmonary oxidative stress, systemic inflammation, vascular dysfunction, and atherosclerosis, thereby increasing the risk of cardiovascular disease11. Also, exposure to high level of PM2.5 or PM10 is linked to an increased risk of metabolic syndrome, hypertriglyceridemia, and high fasting blood glucose12,13, which could lead to metabolic and circulatory diseases. In addition, cardiovascular and metabolic diseases are major risk factors of mortality14. However, most previous studies have primarily focused on the direct link between exposure to PM2.5 and health outcomes5,6,7,8,9,10,11, with limited analysis of how these air pollution impacts are affected by the presence or occurrence of other diseases15,16. For example, a study examined effect modification by pre-existing cardiometabolic risk factors on the PM2.5-CVD mortality association, but did not account for new onsets of such diseases during the follow-up period15. This highlights the need for further scientific evidence on how PM2.5-related mortality risks vary depending on individuals’ health status—both pre-existing conditions and newly developed illnesses. Therefore, this study aims to examine the hypothesis that the onset of cardiovascular and metabolic diseases may modify the long-term association between PM2.5 and mortality, providing epidemiological evidence on the possible mechanisms and identifying demographically high-risk populations, using a population-representative nationwide cohort of individuals aged 50 and over in Korea, screened in 2002–2003 and followed from 2004 to 2019.
Methods
Health insurance cohort
This study used the National Health Insurance Service-National Sample Cohort (NHIS-NSC) with individuals aged 50 or over residing in all 226 inland second-level districts (si/gun/gu) in Korea (Research number: NHIS-2022-2-376). The median area of these districts is 397 km2, approximately 1.7 times the size of a ZIP code in the United States (233 km2)17. Under the National Medical Insurance Act, NHIS ensures universal healthcare coverage for all citizens residing in South Korea. However, individuals who moved abroad were ineligible for insurance coverage and were excluded from our cohort, resulting in 0.3% of participants dropping out of this study. The NHIS-NSC was built through systematic stratified random sampling across 1,476 strata, ensuring proportional representation based on age, sex, eligibility status, and income level. The NHIS-NSC included over one million beneficiaries, representing 2.2% of all eligible Korean citizens, between 2002 and 201918.
From this cohort, we obtained individual information, including the year of birth and death, sex, district of residence, income decile group, and medical treatment details, including the first day of treatment with principal and secondary diagnosis codes. This information was used to determine the presence of disease, identify the year and cause of death, and account for potential confounders/covariates.
Identification of the major cardiovascular and metabolic diseases
Exposure to PM is strongly associated with an increased risk of cardiovascular and metabolic diseases, including heart failure, hypertension, myocardial infarction, and type 2 diabetes. Numerous studies using methods like Mendelian randomization have provided causal evidence linking long-term PM exposure to the development and progression of these conditions19,20. Therefore, we decided to focus on these conditions based on many other previous studies and their high prevalence in Korea. To identify major cardiovascular and metabolic diseases potentially influencing the relationship between PM2.5 and mortality, we consulted the WHO report and guidelines, as well as the Charlson Comorbidity Index (CCI), a widely used tool for assessing mortality risk due to comorbidities21,22. The CCI includes 17 disease categories used to predict ten-year survival; however, for this study, we focused specifically on cardiometabolic diseases. We excluded sensitive conditions such as cancer and infectious diseases, as the NHIS masks the last digits of ICD codes for these conditions to protect personal information. Based on this rationale, we selected six major cardiovascular and metabolic-related diseases: myocardial infarction (MI), congestive heart failure (CHF), cerebrovascular disease (CBVD), peripheral vascular disease (PVD), renal disease (RENAL), and liver disease (LIVER). For each of these diseases, if a patient had a hospital visit with the corresponding principal diagnosis code, the individual was considered to have the disease from that point onward.
Disease onset and causes of death were identified based on the International Classification of Diseases, 10th Revision (ICD-10) codes. The primary outcome of our study was non-accidental mortality (A00–R99). Additionally, we examined cardiovascular deaths (I00–I99) in secondary analyses. We did not specifically assess whether the six major diseases were the cause of death, as our primary goal was to examine which disease onsets increase susceptibility to PM2.5-related mortality. This approach provides a more appropriate framework for understanding how PM2.5 contributes to mortality risk through complex disease trajectories, acknowledging the limitations of death certificates in capturing the biological pathway from exposure to death. A graphical description of disease onset and the specific ICD-10 codes used for disease definitions are provided in the Supplementary Information (1. Study design and disease definition).
Study population and design
We designed a closed cohort study to examine how the onset of major cardiovascular and metabolic diseases modifies the relationship between long-term exposure to PM2.5 and mortality. To exclude participants with potential underlying diseases, the study period was divided into a screening period (2002–2003) and a follow-up period (2004–2019). A two-year screening period was chosen to allow sufficient time to detect pre-existing conditions using hospital visit records, while preserving a long follow-up duration for mortality outcomes. Based on health status during the screening period, participants were classified into two sub-cohorts: (1) NoUD: individuals without hypertension, diabetes, or any of the six major cardiovascular and metabolic diseases, and (2) HTN/DM: individuals with hypertension and/or diabetes but without six major cardiovascular and metabolic diseases. We classified HTN/DM cohort separately because they are highly prevalent in middle-aged and older adults23,24,25 and represent earlier-stage conditions compared to the other six diseases, which reflect more advanced or critical stages. This stratification allowed us to investigate how additional comorbidities modify PM2.5-related mortality risk in populations with different baseline health statuses: one healthy and the other with common early-stage cardiometabolic risk factors. Both sub-cohorts were derived from a population-representative nationwide sample and differed only by the presence of hypertension and/or diabetes at baseline. By directly reflecting the population sample, we estimated the relative hazard ratios (i.e., measures of effect modification) using an interaction term between PM2.5 concentration and disease status. Specifically, for each disease that might modify the association between PM2.5 and mortality, disease status was included as an indicator variable (onset of disease = 1, otherwise = 0) in the interaction term.
This classification was possible by NHIS hospital visit records, which contain data about each visit, such as diagnosis code and visit date. We operationally defined the onset of major cardiovascular and metabolic diseases during the follow-up period based on the first hospital visit record with the principal diagnosis code. Each participant eligible for these two cohorts was followed-up from January 1, 2004, until either death or the end of the study period on December 31, 2019, whichever came first.
Air pollution estimates
We used air pollution data provided by a machine learning-based ensemble prediction model developed by the AiMS-CREATE network (Ai-Machine learning and Statistics Collaborative Research Ensemble for Air pollution, Temperature, and all types of Environmental exposures)26. Since 2015, Korea has operated approximately 150 PM2.5 monitoring stations, primarily located in urban metropolitan areas. To address the potential selection bias and estimate nationwide associations, we used an air pollution prediction model with excellent performance (cross-validated R2 = 0.87). Monthly concentration predictions were generated for ambient PM2.5, at a spatial resolution of 1 km2 across all 226 inland districts in contiguous Korea. These predictions were generated using a validated machine-learning ensemble model that incorporates three different algorithms (gradient boosting, random forest regression, and neural networks). To reduce the influence of extreme values, we excluded observations that exceeded the monitoring stations’ measurement limits when modeling monthly average PM2.5 concentrations. This approach is more robust to outliers compared to using daily averages and aligns with our focus on long-term exposure.
Monthly air pollution values were used to calculate the annual mean PM2.5. We assigned two-year moving average PM2.5 concentrations (Lag 0–1y) based on the district of residence for each year, following the approach of previous studies27,28,29. Additional details regarding the overall prediction model are provided in the Supplementary Information (2. Air pollution prediction data and Figure S1).
Confounders/Covariates
We included various potential time-varying (i.e. annually updated) individual- and district-level covariates in our analysis. As individual-level covariates, age was derived from the birth year and stratified into 5-year increments. Decile income levels were categorized as low (0–2), mid (3–7), and high (8–10), with zero deciles representing medical aid beneficiaries. Annual residential districts were divided into capital (Seoul, Incheon, Gyeonggi), midland (Daejeon, Sejong, Chungcheong, and Gangwon), and southern (Busan, Daegu, Gwangju, Ulsan, Gyeongsang, and Jeolla) areas based on their proximity to the capital and relative latitude. Jeju and Ulleung Island were excluded because of the unavailability of air pollution prediction data. To account for individuals diagnosed with more than one of the six diseases, we also included the individual-level time-varying onset status of hypertension, diabetes, chronic pulmonary disease (CPD), and the six major diseases described in Sect. Identification of the major cardiovascular and metabolic diseases as covariates in the Cox regression model, thereby controlling for the potential effects of comorbidities. We hypothesized that these conditions may modify the impact of PM2.5 on mortality1. In particular, although hypertension and diabetes often precede the six major diseases and modify susceptibility to air pollution-related mortality, they may also independently contribute to mortality and are sometimes recorded as primary causes of death (e.g., through diabetic shock). Given this dual role—as both potential mediators and independent risk factors—we considered them as time-varying covariates in our model. Additionally, sex was adjusted for as the only time-invariant individual-level indicator.
Furthermore, to address potential socioeconomic and environmental effects related to spatial trends, we included four time-varying district-level indicators based on individual residences, which were sourced from the Korea Community Health Survey: “annual unmet medically necessary services (%),” “older population (%),” “basic livelihood support recipients per 1,000 population,” and “parks per 1,000 population”30. These indicators may serve as potential confounders for CVD and mortality31,32,33. They operate through various pathways, including healthcare accessibility and timely treatment, socioeconomic factors affecting vulnerable populations, and environmental factors, such as the availability of parks and recreation spaces. In addition to these socioeconomic indicators, we also adjusted for annual mean temperature as a potential environmental confounder. We obtained daily mean temperature data from the ERA5-Land dataset available via Google Earth Engine, aggregated the 9-km resolution daily data to the yearly and district level, and incorporated it into our models34. Additional information on the aforementioned covariates and rationales of the selections is provided in the Supplementary Information (3. Covariates details and Figure S2).
Statistical analysis
For each cohort, we fitted the Cox regression model as the main analysis to estimate how associations between PM2.5 and mortality were modified by each of the six diseases, accounting for time-dependent exposures and confounders/covariates. To identify the effect modification of each cardiovascular and metabolic disease on PM2.5-related mortality, we added an interaction term between disease onset and PM2.5 in the model. This approach allows us to compare the risk of PM2.5-related mortality with and without a specific disease, expressed as the relative hazard ratio (RHR). Due to our primary goals–suggesting plausible mechanisms between PM2.5, disease onset, and mortality, along with identifying high-risk populations–and insufficient sample size, we did not apply matching methods to evaluate and compare the effect modification of disease onset. We estimated this using a per 10 µg/m3 increase in two-year moving average concentration of PM2.5 (Lag 0–1 y), along with 95% confidence intervals (CI). The analyses were conducted separately for the two cohorts.
We identified diseases that had the highest and statistically significant association with an increased risk of death due to PM2.5 in the two cohorts. This analysis was repeated for non-accidental and cardiovascular mortalities as separate outcomes. Furthermore, we performed subpopulation analyses based on sex and age at entry.
In addition, we evaluated the robustness of our results using several sensitivity analyses. First, as an alternative exposure time window, we examined the delayed air pollution effects by comparing current-year, one-year, and two-year lag periods, along with their moving averages for PM2.5. Second, we expanded the disease definition by including a secondary diagnosis in addition to a principal diagnosis. Secondary diagnosis refers to an additional medical condition that coexists with the principal diagnosis during a patient hospital visit, allowing us to encompass broader definitions of the disease. If a disease was identified as a secondary diagnosis, the patient was considered to have the disease in this analysis. This approach differs from the original analysis, which only considered the principal diagnoses. Third, we extended the screening period from two to three years to differentiate between the NoUD and HTN/DM cohorts. Fourth, we performed the main analysis in separate HTN-only and DM-only cohorts that only had each condition during the screening period, to assess whether PM2.5-related mortality risks differed by condition, given their distinct pathophysiology. Fifth, to address the potential for bias arising from adjusting for variables that may lie on the causal pathway from PM2.5 to mortality, we excluded the time-varying onset status of hypertension and diabetes from our model. Lastly, we focused on individuals who developed only a single disease during the follow-up period, using those without any of the six diseases as the reference group. This allowed us to more rigorously disentangle the effect of each disease from the influence of comorbidities on the PM2.5–mortality association, as our main analysis included individuals with multiple diseases to reflect real-world patterns of multimorbidity. Details of the sensitivity analysis are presented in the Supplementary Information (4. Sensitivity analyses). All statistical analyses were performed using SAS Enterprise Guide 8.3 (SAS Institute Inc., Cary, NC, USA).
Results
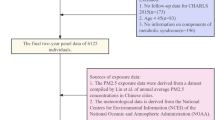
Figure 1 shows the flow diagram of the study population. Among the 183,834 individuals, 134,584 without major cardiovascular and metabolic diseases were assigned to the NoUD cohort, while 49,250 individuals with hypertension and/or diabetes were allocated to the HTN/DM cohort. Figure S1 and Figure S2 displays the geographical distribution of average PM2.5 concentrations and temperature in South Korea between 2004 and 2019.

Flow diagram of study population. The years 2002–2003 were used as a screening period to exclude individuals with pre-existing conditions. Follow-up for mortality outcomes began in 2004.
The participant characteristics for each cohort are listed in Table 1. Over a median follow-up of 16 years, the NoUD cohort experienced 24,178 non-accidental deaths and 5,372 cardiovascular deaths, while the HTN/DM cohort reported 12,639 non-accidental deaths and 3,463 cardiovascular deaths. The average PM2.5 concentrations exposed over the study duration were 29.5 µg/m³ (standard deviation [SD]: 2.3) in the NoUD and 29.6 µg/m³ (SD: 2.3) in the HTN/DM cohort. Throughout the study period, the most prevalent diseases in the NoUD cohort were CPD (63.9%), HTN (56.1%), and DM (28.9%). In the HTN/DM cohort, where HTN and/or DM were already present as underlying conditions, CPD (67.1%) and CBVD (37.3%) were the most frequently occurred diseases. Kaplan-Meier survival curves for both cohorts are displayed in Figure S3, and the NoUD cohort generally showed higher survival probabilities throughout the follow-up period.
Table 2 presents the association between long-term PM2.5 and mortality in the two cohorts across various lag periods. In the NoUD cohort, for every 10 µg/m3 increase in Lag 0–1 y PM2.5, the associations with PM2.5 were generally consistent for both non-accidental and cardiovascular mortality. However, in the HTN/DM cohort, the PM2.5-related risks were higher for cardiovascular mortality. We selected Lag 0–1 y PM2.5 as the main exposure for this study, as it aligned with methodologies from previous studies examining delayed or averaged effects up to the previous year27,28,29.
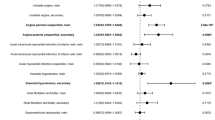
Figure 2 illustrates how the onset of each disease amplified the impact of PM2.5 on non-accidental mortality. In both the NoUD and HTN/DM cohorts, RENAL and MI exhibited the highest RHR, reaching 1.58 (95% CI: 1.27–1.97) for RENAL and 1.41 (1.15–1.73) for MI in the NoUD cohort, and 1.74 (1.43–2.12) for RENAL and 1.62 (1.29–2.05) for MI in the HTN/DM cohort. Although there were slight differences in order and effect size, the two cohorts generally showed a similar pattern of effect modification by the occurrence of cardiovascular and metabolic diseases. Figure S4 also depicts the modifications of cardiovascular mortality risk related to PM2.5, by disease onsets (corresponding to Fig. 2). Unlike the results from non-accidental deaths, CBVD and MI showed higher RHRs compared to those of RENAL.

Effect modification by major cardiovascular and metabolic-related diseases on the association between PM2.5 and non-accidental mortality. Values are presented as relative HRs (95% CI) per 10 µg/m3 increase in PM2.5 (individuals without the disease are assigned a reference HR of 1). Mortality rate per 1,000 person-years is calculated as the total number of deaths with each disease divided by the total person-years with the disease.
Meanwhile, we did not observe strong differences in effect modification patterns across age groups (50–64 y vs. 65 y or older) in either cohort (Fig. 3), in the NoUD cohort, LIVER exhibited a relatively higher RHR among individuals aged 50–64 y, whereas CBVD showed a higher RHR among those aged 65 y or older. We also performed a sex-stratified analysis reported in Fig. 4. The modification patterns were generally more pronounced in females across both cohorts except for LIVER in the NoUD cohort. Specifically, LIVER exhibited the highest effect modification among men and individuals aged 50–64 years in the NoUD cohort. This is further supported by double-stratified analyses in Tables S1, where LIVER showed the highest effect modification in males aged 50–64 years (RHR: 1.62, CI: 1.33–1.98).

Effect modification by major cardiovascular and metabolic-related diseases on the association between PM2.5 and non-accidental mortality, stratified by age at entry. Values are presented as relative HRs (95% CI) per 10 µg/m3 increase in PM2.5 (individuals without the disease are assigned a reference HR of 1). Mortality rate per 1,000 person-years is calculated as the total number of deaths with each disease divided by the total person-years with the disease.

Effect modification by major cardiovascular and metabolic-related diseases on the association between PM2.5 and non-accidental mortality, stratified by sex. Values are presented as relative HRs (95% CI) per 10 µg/m3 increase in PM2.5 (individuals without the disease are assigned a reference HR of 1). Mortality rate per 1,000 person-years is calculated as the total number of deaths with each disease divided by the total person-years with the disease.
The results of the sensitivity analysis were consistent with the main results. Our results were generally robust to alternative exposure windows (Figure S7). The inclusion of cases identified using secondary diagnostic codes and the use of a longer screening period did not change the main results (Figures S8 and S9). In the separate HTN-only and DM-only cohorts, the magnitude of effect modification showed greater variability compared to the NoUD and HTN/DM cohorts, likely due to insufficient sample sizes. Nevertheless, the direction of effect modification and the specific diseases showing high modification effects remained consistent (Table S3). Results from the single-disease population were also generally in line with the main findings. For some diseases, such as myocardial infarction and liver disease, the relative hazard ratios (RHRs) indicated slightly greater effect modification compared to the original cohorts (Table S4). Lastly, results from the model without adjustment for hypertension and diabetes were nearly identical to those from the fully adjusted model (Table S5).
Discussion
This study investigated the effect modifications by the onset of six major cardiovascular and metabolic diseases on the association between long-term exposure to PM2.5 and non-accidental and cardiovascular mortalities, using a nationwide, population-representative cohort from 2004 to 2019. We examined whether individuals who develop these major cardiovascular and metabolic-related diseases become more vulnerable to PM2.5-related mortality and identified which disease onsets may require greater management or preventive strategies in the context of PM2.5 exposure. In both cohorts, the effect modification estimates were highest with the onset of renal diseases and myocardial infarction on the association between PM2.5 and non-accidental death, and the effect modification pattern was more pronounced in women.
To our knowledge, this is the first and largest epidemiological study in Korea to investigate how diverse diseases modify the impact of long-term PM2.5 exposure on mortality. We used a population-representative cohort with more than 15 years of follow-up, incorporating time-varying air pollution and various covariates. Although several studies have assessed the role of air pollution in morbidity and mortality5,7,8,9,10, further studies are needed regarding the potential for diseases to amplify the risk of death associated with air pollution. In particular, this study explored the increased vulnerability to PM2.5, depending on underlying conditions, suggesting that both individuals with hypertension or diabetes and healthy individuals without these conditions may be susceptible, particularly with the onset of certain diseases. Furthermore, this study found that individuals aged 50–64 y and men showed greater effect modifications by liver disease and renal disease. The evidence is limited in this study, however, we cautiously conjecture that higher economic activities can be related to higher amount of exposure to PM2.526,35. Higher alcohol consumption and smoking rate in middle-aged population36 could be also associated with the results. Nevertheless, further studies should address this issue in-depth.
We found that the onset of renal diseases was associated with higher estimated impacts of PM2.5 on mortality in both the total and sub-populations. In Korea, an estimated 6.3% of adults aged 19 years or older and 26.5% of adults aged 70 years or older are reported to have chronic kidney disease in 202137. Although the underlying biological mechanisms connecting air pollution to renal diseases and death are not fully understood, several potential pathways exist. Inhaled air pollutants can enter the bloodstream, triggering inflammation, causing oxidative stress, and inflicting DNA damage to kidney tissue because the kidney concentrates most of the environmental toxins during filtration38,39. Consistent with our results, Jung et al. reported a statistically significant increase in PM2.5-related mortality risk in patients with chronic kidney disease40. Lee et al. also showed that long-term exposure to PM2.5 was related to the first hospitalization for chronic kidney disease and acute renal injury in the Medicare population in the United States28,29. We also found that renal diseases showed the second highest RHRs for cardiovascular death in NoUD (Figure S4) and surmised that these results might be based on the complex and close relationships between kidney diseases and cardiovascular diseases. In particular, it has been widely known that severe kidney diseases (acute kidney injury, end-stage kidney disease, etc.) have bi-directionally interactive impacts with severe cardiac events, such as myocardial infarction, heart failure, and/or cerebrovascular disease41, because blood circulates both organs. Therefore, our results indicate that stricter guidelines regarding outdoor PM2.5 exposures should be established for individuals who have severe kidney diseases, cardiovascular disease, or both.
Furthermore, we identified that myocardial infarction, congestive heart failure, and cerebrovascular diseases are major risk factors related to PM2.5 in our study. Long-term exposure to PM2.5 may contribute to inflammation in blood vessels, accelerating atherosclerosis. This association could be caused by the early-stage progression of intima-media thickness and coronary calcification, resulting in atherothrombotic changes. Additionally, inhaled PM2.5 can lead to an imbalance in the autonomic nervous system, potentially associated with heart rhythm disturbances5. Consistent with our findings, Liao et al. reported increased PM2.5-mortality risk in adults with a history of acute myocardial infarction or stroke42.
Moreover, our findings show that the onset of liver disease modified PM2.5-related mortality in both cohorts, particularly in men and individuals aged 50–64 years. We conjecture that lifestyle factors commonly observed in middle-aged individuals and men, such as higher alcohol consumption, smoking, and an unhealthy diet, may contribute to their elevated risk of liver disease43. Although liver disease is not typically recognized as an acute, severe condition directly linked to death, it is closely associated with severe or acute cardiovascular events, such as myocardial infarction and stroke44. Therefore, individuals with liver disease also should be carefully considered in intervention plans against air pollution.
In addition, although the estimated impact of disease on PM2.5-mortality associations for the NoUD and HTN/DM cohorts was not statistically different in general, we found that HTN/DM showed a pronounced interactive effect of major cardiovascular and metabolic diseases on the PM2.5-mortality association. Globally, approximately 1.28 billion individuals aged 30–79 years have hypertension, and approximately 10.5% of those aged 20–79 years have been diagnosed with diabetes23,24. Both conditions commonly occur in the middle-aged and older populations25, increasing the risk of complications, impairing regulatory mechanisms, and compromising the immune system45. In our study, women and individuals aged 50–64 years in the HTN/DM cohort exhibited a pronounced relative HR. This could be attributed to hormonal changes during menopause, as estrogen withdrawal negatively impacts cardiovascular function and metabolism. In particular, menopause in middle-aged women exacerbates traditional CVD risk factors, including increased body fat, reduced glucose tolerance, elevated blood pressure, endothelial dysfunction, and vascular inflammation46. This changes may interact with conditions such as hypertension or diabetes, potentially heightening the risk of adverse health outcomes47,48. We have corroborated prior findings indicating a heightened association between PM2.5 and mortality in individuals with hypertension and/or diabetes49,50.
This study had several strengths. First, it offers compelling evidence on how cardiovascular and metabolic-related diseases may modify the impact of PM2.5, using a large national sample cohort with time-varying PM2.5 and diverse individual- and district-level confounders/covariates over a 15-year follow-up period. Second, this study examined the roles of hypertension and diabetes in PM2.5-mortality associations and suggested different magnitudes of interactive roles. Thus, our results highlight the importance of the careful management of patients with hypertension and/or diabetes to prevent additional health complications related to air pollution. Third, by focusing on disease onset as an effect modifier rather than as an outcome, our study highlights the critical role of health status trajectories in shaping susceptibility to environmental stressors. The findings provide insight into which intermediate disease developments—such as the onset of myocardial infarction, kidney disease, or liver disease—require more proactive management in populations exposed to elevated PM2.5 levels. Understanding these modification patterns can inform targeted interventions to reduce air pollution-related health burdens in vulnerable subgroups. Fourth, we examined various cardiovascular diseases, metabolic diseases, and their combinations to quantify and compare their impacts on PM2.5-related mortality. Finally, the generalizability of our research is enhanced in Korea by the use of a large, nationwide, and population-representative long-term cohort that incorporates lifelong hospital visits and high-spatial-resolution air pollution data, contributing to the robustness of our findings.
Nevertheless, this study has several limitations. First, due to limited data availability, we could not address other types of major diseases listed in the CCI22, such as cancer, dementia, and other infectious or viral diseases that are prevalent in middle-aged and older individuals. The NHIS data masked diagnosis codes for over a hundred sensitive diseases to prevent the possibility of identifying a participant by merging information about rare-disease status, age, and residence18. Second, the ICD-10-based diagnosis (i.e. clinical diagnosis) used in this study may not accurately reflect the true disease status of participants because the NHIS database was primarily generated for health insurance claims. For example, in the case of CKD, in which symptoms often manifest late in the disease process, the median sensitivity and positive predictive value (PPV) were reported to be 41% and 78%, respectively, in a systematic review51. For stroke, only 70% of diagnoses exhibited a PPV exceeding 80% in the European Health Records52. However, considering that the six diseases investigated in this study were clinically serious and that the Korean national health insurance system may be able to provide affordable and accessible healthcare, symptomatic patients are likely to promptly seek medical attention, reducing the likelihood of underdiagnosis. Moreover, regular national checkups for individuals aged > 40 years can enhance early detection of the diseases addressed in this study. Nevertheless, our identification of disease onset was based on the first hospital record and may have missed patients with undiagnosed conditions. Third, determining the exact onset date of the disease was challenging because the data sourced from the claim records reflected the date of hospital visits and different claim date systems among hospitals rather than the actual disease onset. This challenge is especially pronounced for mild or chronic conditions because it depends on factors such as variations in access to healthcare facilities and symptoms that drive individuals to seek medical attention. For conditions such as hypertension and diabetes, where approximately 40–50% of individuals may be unaware of their condition23,24, establishing a chronological order based on diagnosis dates is challenging. This limited us from conducting advanced statistical analyses, such as multistate or pathway modeling, which require precise time information on disease onset53. Also, when time-varying confounders were affected by prior exposure and mediators, natural direct and indirect effects were not identified, thus causal mediation analysis was difficult in our settings54. Fourth, while hypertension and diabetes may act as mediators in the pathway from PM2.5 exposure to CVD and mortality, adjusting for them might interfere with part of this causal pathway and potentially lead to underestimation of the effect modification by the six major diseases. However, this mediating role may not fully apply in our context. Hypertension and diabetes often precede the six major diseases and increase vulnerability to air pollution, but they also independently contribute to mortality and are sometimes recorded as primary causes of death (e.g., diabetic shock). In our data, 27–30% of individuals with hypertension or diabetes died without developing any of the six major diseases, and in over 23% of these deaths, hypertension or diabetes was listed as a cause. These findings suggest that hypertension and diabetes may act not only as mediators between PM2.5 exposure and mortality via major diseases, but also as independent risk factors for mortality. Sensitivity analyses excluding HTN and DM yielded consistent results (Table S5), supporting our approach of including them as time-varying covariates. Fifth, the median size of the 226 districts used to allocate PM2.5 is 397 km2, which is approximately 1.7 times larger than a typical ZIP code in the United States, which may introduce potential measurement bias. This was the minimum geospatial resolution provided by the NHIS-NSC, leading to all existing studies utilizing NHIS-NSC data being conducted at district level. However, approximately half of our cohort reside in metropolitan cities where the average district size is relatively smaller (78.5 km2). Furthermore, 46.1% of the NoUD and 46.9% of the HTN/DM cohort resided in these metropolitan areas, with each cohort spending 44.5% and 45.2% of their follow-up time, respectively. Therefore, we conjecture that the potential measurement bias arising from large districts might be adequately mitigated. Sixth, owing to the limited sample size, matching methods (that might provide more accurate effect modification estimates by controlling observed or unobserved confounders/covariates) could not provide statistically reliable results in this study. Future studies should address this issue with a large cohort and suitable matching approaches. Seventh, access to individual health behaviors, such as alcohol consumption and smoking, which might be major confounders or covariates, was limited in the NHIS database, thus our results should be limitedly interpreted in relation to potential confounders. Therefore, further studies with larger cohorts including more various confounders should be performed in the future. Finally, as our study focused on the long-term impacts of PM2.5, it could not address acute effects from daily spikes or apply short-term methodological approaches, such as the time-stratified case-crossover design. Although moving averages help smooth short-term fluctuations, they may still include some acute effects—a limitation well recognized in the literature55. This highlights the need for advanced analytical models to disentangle short- from long-term health impacts.
Conclusions
This found that the evident associations between PM2.5 and mortality was modified by the onset of major cardiovascular and metabolic diseases. These findings have important implications for public health policies and suggest the potential for developing targeted interventions for individuals with specific conditions. Our results also inform strategies for mitigating disease severity, curbing healthcare expenditure, and improving the public health value of air pollution guidelines for high-risk populations.
Data availability
Air pollution projection data is publicly available upon reasonable request with permission on the AiMS-CREATE website (https://www.datascience4health.com/). The NHIS-NSC data is not publicly available but can be accessed with permission and a fee (http://nhiss.nhis.or.kr).
References
World Health Organization. The top 10 causes of death, (2020). https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
Statistics Korea. Statistics on Causes of Death in 2019 (2020).
World Health Organization. World Health Statistics 2023: Monitoring Health for the SDGs, Sustainable Development Goals (World Health Organization, 2023a).
Isomaa, B. et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 24, 683–689. https://doi.org/10.2337/diacare.24.4.683 (2001).
Hayes, R. B. et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 49, 25–35. https://doi.org/10.1093/ije/dyz114 (2019).
Yitshak-Sade, M., Kloog, I., Zanobetti, A. & Schwartz, J. D. Estimating the causal effect of annual PM2.5 exposure on mortality rates in the Northeastern and mid-Atlantic States. Environ. Epidemiol. 3, e052. https://doi.org/10.1097/ee9.0000000000000052 (2019).
Alexeeff, S. E. et al. PM2.5 exposure and risks of ischemic heart disease and stroke events: Review and Meta‐Analysis. J. Am. Heart Association. 10, e016890. https://doi.org/10.1161/JAHA.120.016890 (2021).
Pun, V. C., Kazemiparkouhi, F., Manjourides, J., Suh, H. H. & Long-Term PM2.5 exposure and respiratory, cancer, and cardiovascular mortality in older US adults. Am. J. Epidemiol. 186, 961–969. https://doi.org/10.1093/aje/kwx166 (2017).
Bowe, B., Xie, Y., Yan, Y. & Al-Aly, Z. Burden of Cause-Specific mortality associated with PM2.5 air pollution in the united States. JAMA Netw. Open. 2, e1915834–e1915834. https://doi.org/10.1001/jamanetworkopen.2019.15834 (2019).
Tsai, S. S., Hsu, C. T. & Yang, C. Risk of death from liver cancer in relation to long-term exposure to fine particulate air pollution in Taiwan. J. Toxicol. Environ. Health Part. A. 86, 135–143. https://doi.org/10.1080/15287394.2023.2168225 (2023).
Brook, R. D. et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American heart association. Circulation 121, 2331–2378. https://doi.org/10.1161/CIR.0b013e3181dbece1 (2010).
Eze, I. C. et al. Long-Term exposure to ambient air pollution and metabolic syndrome in adults. PloS One. 10, e0130337. https://doi.org/10.1371/journal.pone.0130337 (2015).
Wallwork, R. S. et al. Ambient fine particulate matter, outdoor temperature, and risk of metabolic syndrome. Am. J. Epidemiol. 185, 30–39. https://doi.org/10.1093/aje/kww157 (2017).
Malik, S. et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in united States adults. Circulation 110, 1245–1250. https://doi.org/10.1161/01.Cir.0000140677.20606.0e (2004).
Pope, C. A. et al. Relationships between fine particulate air pollution, cardiometabolic disorders, and cardiovascular mortality. Circul. Res. 116, 108–115. https://doi.org/10.1161/CIRCRESAHA.116.305060 (2015).
Zhang, S. et al. Exposure to air pollution during Pre-Hypertension and subsequent hypertension, cardiovascular disease, and death: A trajectory analysis of the UK biobank cohort. Environ. Health Perspect. 131, 17008. https://doi.org/10.1289/EHP10967 (2023).
Kang, C. et al. Beneficial impacts of residential greenness on sleep deprivation in adults aged 19 or older living in South Korea: A nationwide community health survey in 2011–2018. Sci. Total Environ. 914, 169700. https://doi.org/10.1016/j.scitotenv.2023.169700 (2024).
Lee, J., Lee, J. S., Park, S. H., Shin, S. A. & Kim, K. Cohort Profile: The National Health Insurance Service–National Sample Cohort (NHIS-NSC), South Korea. International Journal of Epidemiology 46, e15-e15, (2016). https://doi.org/10.1093/ije/dyv319
Gao, H. et al. Causal associations of environmental pollution and cardiovascular disease: A Two-Sample Mendelian randomization study. Global Heart. 19, 52. https://doi.org/10.5334/gh.1331 (2024).
Wang, Q. et al. Causality of particulate matter on cardiovascular diseases and cardiovascular biomarkers. Front. Public. Health. 11, 1201479. https://doi.org/10.3389/fpubh.2023.1201479 (2023).
World Health Organization. ICD-10 Version:2019, (2019). https://icd.who.int/browse10/2019/en
Hude, Q. et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care. 43, 1130–1139. https://doi.org/10.1097/01.mlr.0000182534.19832.83 (2005).
World Health Organization. Hypertension, (2023b). https://www.who.int/news-room/fact-sheets/detail/hypertension
International Diabetes Federation. IDF Diabetes Atlas – 10th edition. (2021).
Kim, Y., Park, S., Oh, K., Choi, H. & Jeong, E. K. Changes in the management of hypertension, diabetes mellitus, and hypercholesterolemia in Korean adults before and during the COVID-19 pandemic: data from the 2010–2020 Korea National health and nutrition examination survey. Epidemiol. Health. 45, e2023014. https://doi.org/10.4178/epih.e2023014 (2023).
Park, J. et al. Association of long-term exposure to air pollution with chronic sleep deprivation in South Korea: A community-level longitudinal study, 2008–2018. Environ. Res. 228, 115812. https://doi.org/10.1016/j.envres.2023.115812 (2023).
Shi, L. et al. Long-term effects of PM2·5 on neurological disorders in the American medicare population: a longitudinal cohort study. Lancet Planet. Health. 4, e557–e565. https://doi.org/10.1016/S2542-5196(20)30227-8 (2020).
Lee, W. et al. Associations between long term air pollution exposure and first hospital admission for kidney and total urinary system diseases in the US medicare population: nationwide longitudinal cohort study. BMJ Med. 1, e000009. https://doi.org/10.1136/bmjmed-2021-000009 (2022).
Lee, W. et al. Air pollution and acute kidney injury in the U.S. Medicare population: A longitudinal cohort study. Environ. Health Perspect. 131, 47008. https://doi.org/10.1289/ehp10729 (2023).
Kang, Y. W. et al. Korea community health survey data profiles. Osong Public. Health Res. Perspect. 6, 211–217. https://doi.org/10.1016/j.phrp.2015.05.003 (2015).
Kim, H. et al. Effects of long-term exposure to air pollution on all-cause mortality and cause-specific mortality in seven major cities of South Korea: Korean National health and nutritional examination surveys with mortality follow-up. Environ. Res. 192, 110290. https://doi.org/10.1016/j.envres.2020.110290 (2021).
Seo, S., Choi, S., Kim, K., Kim, S. M. & Park, S. M. Association between urban green space and the risk of cardiovascular disease: A longitudinal study in seven Korean metropolitan areas. Environ. Int. 125, 51–57. https://doi.org/10.1016/j.envint.2019.01.038 (2019).
Lee, W., Choo, J. Y., Son, J. Y. & Kim, H. Association between long-term exposure to air pollutants and prevalence of cardiovascular disease in 108 South Korean communities in 2008–2010: A cross-sectional study. Sci. Total Environ. 565, 271–278. https://doi.org/10.1016/j.scitotenv.2016.03.163 (2016).
Park, J., Kim, A., Bell, M. L., Kim, H. & Lee, W. Heat and hospital admission via the emergency department for people with intellectual disability, autism, and mental disorders in South Korea: a nationwide, time-stratified, case-crossover study. Lancet Psychiatry. 11, 359–367. https://doi.org/10.1016/S2215-0366(24)00067-1 (2024).
Lee, W. et al. Heat-mortality risk and the population concentration of metropolitan areas in Japan: a nationwide time-series study. Int. J. Epidemiol. 50, 602–612. https://doi.org/10.1093/ije/dyaa245 (2021).
Kim, D., Jeong, J., Ko, Y., Kwon, Y. & Kim, Y. T. The construction of database of community health outcomes and health determinants in the Republic of Korea. Public. Health Wkly. Rep. KCDC. 30, 979–983 (2018).
Agency, K. D. C. a. P. Trends in the prevalence of chronic kidney disease, 2011–2021. Public. Health Wkly. Rep. 16, 238–239. https://doi.org/10.56786/PHWR.2023.16.8.3 (2023).
Lai, C. Y. et al. Physicochemistry and cardiovascular toxicity of metal fume PM2.5: a study of human coronary artery endothelial cells and welding workers. Sci. Rep. 6, 33515. https://doi.org/10.1038/srep33515 (2016).
Zhang, Y., Liu, D. & Liu, Z. Fine particulate matter (PM2.5) and chronic kidney disease. Rev. Environ. Contam. Toxicol. 254, 183–215. https://doi.org/10.1007/398_2020_62 (2021).
Jung, J. et al. Effects of air pollution on mortality of patients with chronic kidney disease: A large observational cohort study. Sci. Total Environ. 786, 147471. https://doi.org/10.1016/j.scitotenv.2021.147471 (2021).
Jankowski, J., Floege, J., Fliser, D., Böhm, M. & Marx, N. Cardiovascular disease in chronic kidney disease. Circulation 143, 1157–1172. https://doi.org/10.1161/CIRCULATIONAHA.120.050686 (2021).
Liao, N. S. et al. Particulate air pollution and risk of cardiovascular events among adults with a history of stroke or acute myocardial infarction. J. Am. Heart Association. 10, e019758. https://doi.org/10.1161/jaha.120.019758 (2021).
Guo, B. et al. Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease. J. Hepatol. 76, 518–525. https://doi.org/10.1016/j.jhep.2021.10.016 (2022).
Alexander, M. et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults. BMJ (Clinical Res. ed.). 367, l5367. https://doi.org/10.1136/bmj.l5367 (2019).
Petrie, J. R., Guzik, T. J. & Touyz, R. M. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can. J. Cardiol. 34, 575–584. https://doi.org/10.1016/j.cjca.2017.12.005 (2018).
Rosano, G. M., Vitale, C., Marazzi, G. & Volterrani, M. Menopause and cardiovascular disease: the evidence. Climacteric 10 (Suppl 1), 19–24. https://doi.org/10.1080/13697130601114917 (2007).
Maas, A. H. & Franke, H. R. Women’s health in menopause with a focus on hypertension. Neth. Heart J. 17, 68–72. https://doi.org/10.1007/bf03086220 (2009).
Kim, H. M., Park, J., Ryu, S. Y. & Kim, J. The effect of menopause on the metabolic syndrome among Korean women: the Korean National health and nutrition examination survey, 2001. Diabetes Care. 30, 701–706. https://doi.org/10.2337/dc06-1400 (2007).
Yang, X. et al. Associations of long-term exposure to ambient PM2.5 with mortality in Chinese adults: A pooled analysis of cohorts in the China-PAR project. Environ. Int. 138, 105589. https://doi.org/10.1016/j.envint.2020.105589 (2020).
Pinault, L. et al. Diabetes status and susceptibility to the effects of PM2.5 exposure on cardiovascular mortality in a National Canadian cohort. Epidemiol. (Cambridge Mass). 29, 784–794. https://doi.org/10.1097/ede.0000000000000908 (2018).
Vlasschaert, M. E. O. et al. Validity of administrative database coding for kidney disease: A systematic review. Am. J. Kidney Dis. 57, 29–43. https://doi.org/10.1053/j.ajkd.2010.08.031 (2011).
Davidson, J., Banerjee, A., Muzambi, R., Smeeth, L. & Warren-Gash, C. Validity of acute cardiovascular outcome diagnoses recorded in European electronic health records: A systematic review. Clin. Epidemiol. 12, 1095–1111. https://doi.org/10.2147/CLEP.S265619 (2020).
Meira-Machado, L., de Uña-Alvarez, J., Cadarso-Suárez, C. & Andersen, P. K. Multi-state models for the analysis of time-to-event data. Stat. Methods Med. Res. 18, 195–222. https://doi.org/10.1177/0962280208092301 (2009).
VanderWeele, T. J. & Tchetgen Tchetgen, E. J. Mediation analysis with time varying exposures and mediators. J. R. Stat. Soc. B. 79, 917–938. https://doi.org/10.1111/rssb.12194 (2017).
Manisalidis, I., Stavropoulou, E., Stavropoulos, A. & Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public. Health. 8, 14. https://doi.org/10.3389/fpubh.2020.00014 (2020).
Acknowledgements
This work was supported by Pusan National University Research Grant, 2022.
Funding
This work was supported by Korea Environment Industry & Technology Institute (KEITI) through Climate Change R&D Project for New Climate Regime, funded by Korea Ministry of Environment (MOE) [RS-2022-KE002235]; the National Institute of Environmental Research (NIER) funded by the Ministry of Environment (MOE) of the Republic of Korea [NIER-2021-03-03-007]; and Institute of Information & communications Technology Planning & Evaluation (IITP) under the Artificial Intelligence Convergence Innovation Human Resources Development [IITP-2025-RS-2023-00254177] grant funded by the Korea government (MSIT).
Author information
Authors and Affiliations
Contributions
HJ conceived and designed the study and wrote the main manuscript. HJ and JP conducted the literature review. HJ performed statistical analyses with support from JM. IS, SA, AK, CK, JO, DK, JM, and EK contributed to data collection. EL, DK, MB, HK, and WL reviewed and edited the manuscript. HK and WL supervised the study and secured funding. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Institutional Review Board of Pusan National University (IRB number: PNU IRB/2022_154_HR). The requirement for informed consent was waived because the National Health Insurance Service–National Sample Cohort (Research number: NHIS-2022-2-376) database used in this study was anonymized according to strict confidentiality guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jang, H., Park, J., Lee, E.S. et al. Effect modification by cardiovascular and metabolic disease onset on long-term PM2.5 exposure and mortality: a nationwide cohort study. Sci Rep 15, 19570 (2025). https://doi.org/10.1038/s41598-025-04498-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-04498-z
