
Abstract
Physical activity is widely promoted to reduce mortality risks from all-cause and cardiovascular diseases, yet current guidelines rarely address sex-specific differences or distinguish between occupational (OPA) and non-occupational PA (Non-OPA). This study leverages NHANES 2007–2018 data to evaluate sex differences in mortality benefits from OPA and Non-OPA, with a specific focus on implications for women’s health. Participants were categorized into three activity levels: below (< 150 min/week), at (150–300 min/week), and above (> 300 min/week) the recommended guidelines. Multivariable Cox models yielded sex-specific hazard ratios (HRs), with nonlinear dose-response relationships explored through subgroup analyses by age and BMI. Our results reveal that females derive greater survival benefits than males at equivalent PA levels, particularly from Non-OPA, which supporting the “physical activity paradox”. For instance, Non-OPA showed stronger protective effects, with females achieving significant risk reductions at lower activity volumes than males. Notably, older adults (≥ 65 years) and individuals with obesity experienced enhanced benefits from Non-OPA. These findings underscore the need for sex-specific PA guidelines and highlight the importance of promoting Non-OPA to maximize health benefits across diverse populations, with specific implications for women’s health.
Similar content being viewed by others

Introduction
Physical activity (PA) is widely recognized for its associations with improved health outcomes and reduced mortality risks1,2,3. In 2020, the World Health Organization recommended that adults engage in 150–300 min of moderate-intensity PA (MPA) or 75–150 min of vigorous-intensity PA (VPA) per week to enhance health outcomes and improve life expectancy4. Generally, PA is defined as any movement produced by skeletal muscles that requires energy expenditure5,6 encompassing activities like jogging, swimming, team sports, heavy lifting, and active transportation such as walking or cycling. Although research has consistently validated the health promoting attributes of PA7,8,9,10 the relationship between different patterns of physical activity ‒particularly occupational and non-occupational physical activity (OPA and Non-OPA) ‒ and mortality remains unclear.
Notably, sex differences in the health benefits of PA have gained attention. Research by Paul J. et al.11 revealed that sex is associated with multidimensional role in cardiovascular disease (CVD), including variations in biological characteristics and cardiovascular health correlated with social, cultural, and behavioral factors. Moreover, significant differences in exercise endurance, muscle strength, hormone levels, and cardiovascular health between men and women may associate with the adaptive responses and health benefits of PA7,12. Recent meta-analyses further demonstrate sex-specific risks, with OPA associated with higher mortality in men but not women13 while socioeconomic contexts modulate these effects14. Therefore, focusing on sex differences in PA may inform the development of tailored exercise strategies to optimize potential health benefits across sexes. This study aims to clarify sex-specific associations of OPA and Non-OPA with mortality outcomes, offering insights to refine physical activity guidelines.
Appropriate physical activity classification criteria are essential to address this issue. While previous studies have primarily focused on leisure-time activities10,15,16,17,18 MPA and VPA or a combination of both (Moderate-to-vigorous intensity physical activity, MVPA)17,19,20,21,22,23,24 muscle-strengthening or aerobic activities7,9,10,16,25 and most of them included sex as a risk factor or subgroup analysis variable without domain-specific stratification. For instance, Feng et al.26 reported that men engaging in midday MVPA had lower risks of all-cause and CVD mortality. Another study highlighted distinct associations of leisure time physical activity (LTPA) and OPA with periodontitis, while LTPA found to reduce the risk of periodontitis, and conducted a subgroup analysis by gender27. A further study identified factors influencing PA in patients with coronary artery disease (CAD) via multiple linear regression, highlighting the need for personalized PA plans to increase PA levels in both male and female CAD patients5. Similarly, a cross-country comparison quantified LTPA benefits in diabetic adults, with adjustment and stratification for sex but without exploring the interaction between sex and the PA dose-response relationship28. Notably, few studies have explicitly examined sex differences in the association of PA with all-cause and cardiovascular mortality. Among them, Ji H et al.7 showing that women had greater reductions in all-cause and CVD mortality from PA than men did, which limited to LTPA. Furthermore, recent studies have highlighted the “physical activity paradox,” that OPA may be associated with increased risks of CVD and all-cause mortality, whereas LTPA is typically linked to reduced risks. For instance, Coenen P et al.13 Temporelli et al.29 and Holtermann et al.30 provided evidence supporting this paradox, suggesting that the health effects of PA vary significantly depending on its context and purpose. Building on these insights, we propose a novel classification framework: distinguishing OPA, which is related to the work environment, from Non-OPA, which is associated with both leisure-time and transport situations. Specifically, this study included both participants with and without a history of CVD, enabling a comprehensive investigation into the health benefits of physical activity across heterogeneous populations.
In summary, this study seeks to further refine research in physical activity epidemiology by proposing a domain-specific framework to distinguish between OPA and Non-OPA (including leisure-time and transport-related activities). Through a systematic assessment of sex differences in mortality associations under OPA and Non-OPA, along with stratified analyses across age and BMI subgroups, we aim to offer insights that could enhance the precision of PA guidelines. This is particularly relevant for women, who encounter unique biological and socioeconomic health determinants. Our findings may provide a basis for public health policies to consider domain-specific physical activity links, socioeconomic differences, and sex-dependent physiological adaptations. This, in turn, may support the development of health promotion strategies tailored to diverse populations.
Methods
Study population
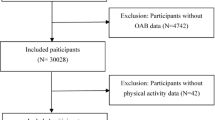
The National Health and Nutrition Examination Survey (NHANES) public database spanning from 2007 to 2008 to 2017–2018 was utilized for this study (https://www.cdc.gov/nchs/nhanes/). As a nationally representative cohort with complex multistage sampling design, NHANES provides high-quality, longitudinal data integrating demographic, clinical, and behavioral variables, enabling robust analysis of population-level health trends. The National Center for Health Statistics Disclosure Review Board approved the NHANES study31. A total of 59,842 participants were collected from this public dataset, and we linked their records to the National Death Index (NDI) records until December 31, 2019. This linkage of large-scale mortality data with detailed baseline assessments leverages the power of big data to minimize selection bias and enhance statistical precision in estimating long-term health outcomes.
Participants were excluded on the basis of the following criteria: (1) age under 18 years (n = 23,262); (2) ineligible mortality data (n = 119); (3) absence of physical activity data (n = 338); and (4) missing follow-up status, lifestyle factors, or chronic health conditions (n = 6,951). After exclusions, the study sample consisted of 29,172 participants, among whom 2,550 deaths were documented, including 738 cardiovascular disease-related fatalities. The large sample size and extended follow-up period ensured sufficient power to detect sex-specific associations even in subgroup analyses (e.g., age ≥ 65, obesity). To improve data integrity, an outlier analysis was performed, identifying any values that exceeded three standard deviations from the mean. The outliers were then replaced with the 75th percentile, leading to a more reliable data distribution32. This approach, combined with survey-weighted statistical models, preserved the representativeness of the NHANES complex sampling framework while mitigating the influence of extreme values.
Covariates
The demographic covariates included sex, age categorized as 18–44, 45–64, >=65, and race stratified into Hispanic, Non-Hispanic White, Non-Hispanic Black, and other groups. Education level was classified as less than a high school degree, a high school degree, more than a high school degree, or missing data. The lifestyle behaviors assessed included smoking status (defined as current, former, never smoker, or missing data) and alcohol consumption (defined as current, former, never drinker, or missing data). Body mass index (BMI), derived from weight in kilograms divided by the square of height in meters, was classified following the WHO Global Database on Body Mass Index criteria33: normal weight (< = 24.9), overweight (25–29.9), and obesity (≥ 30). To control for comorbidities34,35 we used data from the participants’ self-reported medical diagnoses of stroke, CVD, heart failure, cancer, bronchitis, emphysema, and diabetes status. Additionally, we accounted for the Healthy Eating Index 2015 (HEI-2015) and sedentary behavior in our analysis.
Assessment of PA
Information on the frequency, duration, and intensity of various physical activities was collected using the Global Physical Activity Questionnaire (GPAQ)36. The questionnaire assessed engagement in MVPA in occupational settings (e.g., heavy lifting, construction work), during leisure (e.g., sports, fitness activities), and for transportation (e.g., walking, cycling). It also evaluated sedentary behavior by assessing typical sitting duration, excluding sleep time. Intensity was exemplified through sweating, breathing, and heart rate references37.
In our study, PA patterns were categorized into OPA and Non-OPA. OPA was quantified by summing the duration of MPA and VPA physical activities associated with work, with the VPA duration being doubled to reflect its greater energy expenditure38. Non-OPA activities included LTPA and transport-related activities of similar intensities39. To evaluate the interplay between LTPA and OPA, we conducted stratified analyses of their combined exposures, enabling examination of co-existing activity patterns and their mortality associations. And to assess PA participation, we considered the frequency and duration of each activity session, as well as the overall intensity. The intensity was determined by the proportion of vigorous PA relative to total MVPA. MVPA engagement was quantified via the following formula: 2×VPA + MPA7,22,34. Participants were classified into three activity levels on the basis of their weekly MVPA according to the 2018 PA guidelines40: (1) Below: <150 min/week (inactive); (2) At: ≥150 and < 300 min/week (active); (3) Above: >300 min/week (excellent).
Statistical analysis
The analysis adhered to NHANES guidelines41 incorporating survey weights, primary sampling units, and strata to accurately reflect the population structure. Baseline characteristics were described separately for sexes. Categorical variables were analyzed using chi-square tests, while continuous variables, which were non-normally distributed, were presented as medians with interquartile ranges (IQRs).
Cox proportional hazards regression models were employed to assess the impact of PA on all-cause and CVD mortality, where age was parameterized as both continuous and categorical variables to mitigate confounding from differential CVD risk paths between sexes, and providing HRs with 95% confidence intervals (CIs). Three regression models with increasing levels of adjustment were used: Model 1 adjusted for age and race; Model 2 added sociodemographic variables (education), lifestyle factors (smoking, alcohol intake, HEI-2015), disease history (stroke, cardiovascular disease, heart failure, cancer, bronchitis, emphysema, diabetes), and BMI; Model 3 further adjusted for sedentary behavior42,43 the inclusion of sedentary behavior allows interpretation of PA effects through the lens of time substitution‒that is, estimating the health consequences of displacing sedentary time with PA engagement, consistent with isotemporal substitution principles44. Restricted cubic splines with 4 knots (at the 5th, 35th, 65th, and 95th percentiles) were used to explore potential nonlinear relationships between PA and mortality45. Sex differences in these associations were assessed via likelihood ratio tests and adjusted Z tests incorporating interaction terms for PA and sex.
Subgroup analyses were conducted to assess the robustness of findings. The main model was repeated by stratifying age into three levels (18–44, 45–64, ≥ 65 years), combining the 18–44 and 45–64 age groups due to low event rates in the youngest group. The relationship between PA and mortality was also examined across BMI subgroups (≤ 24.9, 25–29.9, ≥ 30), combining the first two levels for comparison with the highest BMI group. All analyses were performed using R v4.2.0, with a two-tailed P-value < 0.05 considered significant.
Results
Characteristics of participants
In our study, 29,172 participants [mean (SD) age, 48.5 [13.46] years; 14,794 [50.7%] females; 7,449(14.5%) Hispanic, 12,157 (66.5%) Non-Hispanic White, 6,267 (11.2%) Non-Hispanic Black, and 3,299(7.8%) Other individuals] were included. The baseline characteristics of 29,172 participants by physical activity group are displayed in Table 1. During a median follow-up duration of 6.7 years, corresponding to 195,452 person-years, a total of 2,550 all-cause deaths were observed, including 738 deaths attributed to CVD. Except for stroke status, emphysema, and sedentary time, where no significant differences were observed between males and females, there was a marked statistical divergence in all other measured indicators. The female participants were more likely to have a higher level of education, to be obese or overweight, to exhibit better dietary quality, to have a lower prevalence of smoking, and to have higher rates of diabetes and cardiovascular diseases.
Sex differences in OPA and Non-OPA associations with all-cause and CVD mortality
As detailed in Table 2, males engaging in OPA at recommended levels had multivariable-adjusted HRs of 0.85(95% CI: 0.57–1.27) for all-cause mortality and 1.41(95% CI: 0.77–2.58) for CVD mortality, while those exceeding recommendations were associated with improved outcomes improved outcomes (all-cause HR: 0.67, 95% CI: 0.56–0.80; CVD HR: 0.73, 95% CI: 0.52–1.03). In contrast, females exhibited stronger inverse associations with mortality for from OPA: at recommended levels, HRs were 0.60(95% CI: 0.40–0.91) for all-cause and 0.90(95% CI: 0.43–1.92) for CVD mortality, with further risk reductions observed at higher activity levels (all-cause HR: 0.74, 95% CI: 0.58–0.94; CVD HR: 0.57, 95% CI: 0.39–0.85). Women had a 25% lower all-cause mortality risk at 300 min/week OPA (p < 0.05, Z-test in Supplementary Table S1), though activity beyond this threshold was paradoxically associated with a 7% higher relative risk compared to men (Fig. 1). Only females showed a significant inverse association between supra-recommended OPA and CVD mortality(43% risk reduction).

Forest plot for the association between different PA patterns and mortality by sex. (A) Association between different causes of death and the OPA by sex. (B) Association between different causes of death and Non-OPA by sex. Estimates from the main adjusted model included the covariates of age, race, education, smoking, alcohol intake, HEI-2015 score, stroke, cardiovascular disease, heart failure, cancer, bronchitis, emphysema, diabetes, BMI, and sedentary behavior.
For Non-OPA, males at recommended levels had HRs of 0.68(95% CI: 0.54–0.85) for all-cause and 1.04(95% CI: 0.66–1.66) for CVD mortality, improving to 0.67(95% CI: 0.53–0.84) and 0.57(95% CI: 0.40–0.81) with higher activity. Females consistently showed stronger inverse associations with Non-OPA: at recommended levels, HRs were 0.62(95% CI: 0.47–0.82) for all-cause and 0.48(95% CI: 0.29–0.84) for CVD mortality, declining further to 0.50(95% CI: 0.38–0.66) and 0.38(95% CI: 0.24–0.62) with excess activity. This translated to a 6% greater all-cause mortality risk reduction in females versus males at guideline levels, escalating to 17% for those above the recommendations. While males required activity levels above guidelines to show CVD protection 0.57(95% CI: 0.40–0.81), females achieved significant reductions both at 0.48(95% CI: 0.29–0.84) and above 0.38(95% CI: 0.24–0.62) recommendations, with an incremental 10% risk decrease beyond target volumes. Additionally, our analysis of combined LTPA and OPA exposures (Supplementary Table S4) revealed stronger inverse associations in females compared to males, with adjusted hazard ratios of 0.54(95% CI: 0.39–0.74) versus 0.64(95% CI: 0.45–0.92) above the recommended levels.
Sex differences in the associations of all-cause and CVD mortality with the frequency, duration, and intensity of physical activity patterns
We observed that both men and women who engaged in physical activity at or above recommended levels with Non-OPA patterns had lower all-cause mortality risks, and higher activity volumes were associated with further risk reductions. Compared with inactive participants, a higher frequency (> = 1 session/week), longer duration per session (> = 1 min) and intensity of physical activity were associated with lower mortality. When examining the relationship specifically for Non-OPA with mortality, the sex difference was significant: at equivalent levels of physical activity frequency, session duration, and intensity, women had a 5–10% lower risk of both all-cause mortality and CVD mortality than men did (Table 3). Compared to Non-OPA, was associated with higher risks of all-cause and CVD mortality in both sexes, as shown in Supplementary Files: Table S2. All models accounted for the complex, multistaged survey sample design and refined by a primary adjustment model that incorporated a comprehensive set of covariates, including age, race, education, smoking, alcohol intake, HEI-2015, stroke, cardiovascular disease, heart failure, cancer, bronchitis, emphysema, diabetes, BMI, and sedentary behavior.
RCS analysis
An additional analysis employing restricted cubic splines was conducted to explore the relationships between different physical activity patterns and the risk of all-cause and CVD mortality. The graphic analysis delineates sex-specific optimal thresholds for the OPA and Non-OPA. For OPA, males were associated with the maximum health benefit, as evidenced by the lowest HRs for all-cause and CVD mortality, at a threshold of approximately 1500 min/week. Beyond this threshold, the HRs exhibit an increasing trend. In contrast, the optimal threshold for females is considerably lower, with an inflection point of approximately 300 min per week. Notably, in the case of Non-OPA individuals, the inflection points for both males and females are substantially lower, with a consistent downward trend in all-cause and CVD mortality as activity duration increases. (Fig. 2)

Sex differences in the dose‒response associations between different PA patterns and mortality outcomes. A: OPA and mortality outcomes by sex. (a-d) Dose‒response relationships between OPA and all-cause and CVD mortality in males and females. Panels (a) and (b) show the relationships for males, while panels (c) and (d) show the relationships for females. B: Non-OPA and mortality outcomes by sex. (a-d) Dose‒response relationships between Non-OPA and all-cause and CVD mortality in males and females. Panels (a) and (b) show the relationships for males, while panels (c) and (d) show the relationships for females. All models were adjusted for the complex survey design and covariates including age, race, education, smoking, alcohol intake, HEI-2015, stroke, cardiovascular disease, heart failure, cancer, bronchitis, emphysema, diabetes, BMI, and sedentary behavior.
Subgroup analysis
For subgroup analysis, we utilized the primary model from Table 2(Model 3) to examine the effects of age and BMI stratification on outcomes. Given the low event rate in the youngest age group (Age Level I, < 44 years, Age Level II, > 44 years and < 65 years, Age Levels III ≥ 65 years), we combined Age Levels I and II for comparative analysis with Age Level III. For all-cause mortality, males at Age III had significantly lower risks associated with physical activity, with HRs of 0.64(95% CI, 0.43–0.98) for activities at the recommended level and 0.61(95%CI, 0.49–0.76) for activities above the recommended level. These findings were consistent with the results observed in females. For CVD mortality, lower risks were observed only at Age III for activities above the recommended level, with HRs of 0.58(95% CI, 0.41–0.84) for males and 0.47(95% CI, 0.26–0.86) for females. Notably, the delayed CVD manifestation window in women is reflected in our stratified outcomes: while both sexes showed risk reduction at ≥ 65 years, the stronger risk reduction in older females (53% vs. 42%) aligns with their extended pre-clinical risk exposure. For BMI stratification, males across all BMI levels had lower all-cause mortality risks when exceeding recommended activity levels (49% lower risk for Levels I and II). Females had lower mortality risks associated with physical activity irrespective of adherence to recommendations. Within Non-OPA, both sexes showed lower all-cause and CVD mortality risks (36–71% reduction) when exceeding recommendations, with females exhibiting greater risk reductions than males. Mortality outcomes were more favorable in Age Level III vs. Levels I/II, and in combined BMI Levels I/II vs. Level III (Supplementary Table S3).
Additionally, we stratified participants by CVD history. Both subgroups (with and without CVD) derived health benefits from physical activity. However, individuals without prior CVD showed more pronounced risk reductions with Non-OPA (HR = 0.41, 95%CI, 0.29–0.58), whereas no significant risk reduction was observed for OPA in this subgroup (HR = 0.83, 95% CI, 0.62–1.11). For participants with pre-existing CVD, limited outcome data precluded definitive conclusions regarding CVD-specific mortality associations. (Supplementary Files: Table S5).
Discussion
This U.S. nationally cohort study, provides novel insights into sex-specific associations between domain-specific physical activity patterns and mortality outcomes. Three principal findings emerge: First, Non-OPA pattern are associated with stronger reductions in mortality risk than OPA across sexes, with women exhibiting greater risk reductions than men at equivalent activity levels. Second, a pronounced sex divergence exists in optimal physical activity thresholds, with females associated with maximal risk reduction at substantially lower Non-OPA volumes than males. Third, the mortality risk reduction gradient is more pronounced for Non-OPA across all age and BMI subgroups, particularly among older adults and individuals with obesity. These findings challenge the ‘one-size-fits-all’ approach in current guidelines and highlight the potential need for sex-specific physical activity recommendations, particularly for women.
The notion that PA is associated with mortality risk is well-established7,8,9,10,21,46,47,48 yet limited research has explored sex differences or distinguished between occupational and non-occupational(integrating leisure-time and transport activities) domains. Ji et al.7 reported a 24% lower all-cause mortality risk among women engaging in leisure time PA, compared to 15% in men. A systematic review and cohort dose-response meta-analysis39 demonstrated that achieving recommended levels of Non-OPA are associated with significantly lower risks of all-cause and CVD mortality in the general adult population. Our findings align with prior research indicating that women may derive greater health benefits from Non-OPA than men. Importantly, all analytical models were adjusted for age ‒ a key confounder since women typically develop CVD about 10 years later than men‒to mitigate confounding from sex-specific CVD risk trajectories. More over, by introducing the combined LTPA and OPA exposures, we further demonstrate a stronger inverse relationship between LTPA and mortality compared to OPA. This can be explained by experimental evidence showing that Non-OPA often involves dynamic movements that enhance cardiorespiratory fitness more effectively than OPA, which typically involves prolonged static loads without sufficient recovery29,30. This supports the “physical activity paradox” and emphasizes the importance of considering the context and purpose of physical activity when interpreting its health effects.
Our study indicates that female participants have lower mortality risks associated with relatively low levels of physical activity, while males typically show comparable risk reductions only at higher activity volumes. This sex-based discrepancy might be influenced by physiological differences, such as women’s greater type I muscle fiber composition and capillary density, which enhance blood perfusion and metabolic efficiency during exercise48,49. Furthermore, physiological studies suggest that females, despite lower baseline muscle strength, exhibit superior vascular conductance and increased blood flow during exercise, potentially linked to their higher capillary density. This physiological advantage is linked to greater capillary density within the skeletal muscle tissue of females than in their male counterparts50. Additionally, psychological and social factors may contribute to these differences, with women showing greater motivation for physical strength and health, whereas men may be more influenced by social incentives51.
In the subgroup analysis, participants over 65 years, irrespective of sex, had significantly lower mortality risks associated with Non-OPA engagement. These results highlight the importance of promoting physical activity in older adults, given its association with improved health outcomes. Meanwhile, individuals with higher BMIs showed stronger inverse associations between Non-OPA and CVD mortality, suggesting that such activities could be prioritized in interventions for populations with obesity. Additionally, our findings suggest that exercise intensity may be less strongly associated with mortality risk reductions than frequency and duration in both sexes. While high-intensity exercise is associated with some health benefits52,53 its association with mortality risk reduction is less pronounced than that of exercise frequency. Therefore, our findings support prioritizing exercise frequency and duration in public health guidelines.
Notably, our study population included individuals both with and without a history of CVD. This approach was adopted to capture the multifactorial essence of CVD in real-world settings and to investigate the health benefits of physical activity across heterogeneous populations. To address potential confounding by CVD history, we adjusted for prior CVD diagnoses in our models rather than stratifying the sample. Stratification would have fragmented the cohort and reduced statistical power. Supplementary Table S5 stratified analysis showed that the benefits of physical activity were somewhat attenuated in participants with CVD, though the limited number of events in this subgroup requires cautious interpretation. Specifically, we incorporated the medical history of coronary heart disease, cardiovascular disease, stroke, emphysema, chronic bronchitis, diabetes, and cancer as covariates into our statistical models. This approach enabled us to evaluate the independent association between physical activity patterns and the risk of CVD mortality while controlling for established risk factors. Our analysis indicated that physical activity is associated with a reduced risk of CVD mortality, even after considering the participants’ previous medical conditions. This finding further substantiates the potential benefits of physical activity for a broad spectrum of the population, including those with chronic diseases. Our results provide evidence supporting the integration of physical activity into disease management strategies, particularly for women.
Limitations
There are several limitations of this study. Firstly, the data collection methods present certain constraints. The PA information of the participants, including exercise frequency, duration, and intensity, was derived from questionnaires. While the NHANES questionnaires are meticulously designed for collecting personal lifestyle data, they are susceptible to participant bias. The increasing use of wearable devices for assessing PA provides a more precise alternative, and future research should consider integrating this approach where feasible. Secondly, despite considering the influence of comorbidities in our analysis, we did not exclude individuals for whom disease may have impaired exercise capacity, potentially affecting our outcomes. To counteract this, we managed extreme PA values by capping them at the 75th percentile to reduce their influence on the results. Thirdly, our study sample was derived from the U.S. nationally public database NHANES, which may differ in sociocultural contexts, healthcare systems, and demographic characteristics from other countries. Consequently, caution should be exercised in extrapolating these findings to global populations. Future studies should validate these associations through multinational cohorts to confirm their broader applicability. Lastly, recognizing the compositional nature of physical activity data, while we did not employ formal compositional data analysis (CoDA) methods, our adjustment for sedentary behavior in Model 3 provides a pragmatic approach to address time allocation interdependencies. By fixing sedentary time in the model, the reported PA associations approximate the health outcomes of reallocating time from sedentary behaviors to PA‒a simplified implementation of isotemporal substitution modeling28. This approach aligns with recent methodological guidance for activity epidemiology54 though we acknowledge that dedicated CoDA techniques (e.g., log-ratio transformations) could further refine these estimates in future studies.
Conclusions
This study highlights significant associations between PA and reduced mortality risks, with women exhibiting stronger inverse associations than men, particularly for Non-OPA. Our findings suggest that even modest PA levels are associated with substantial mortality risk reductions in women, whereas men may require higher volumes to achieve comparable effects. These observations support the consideration of sex-specific PA guidelines, emphasizing leisure-time and transport-related activities to optimize public health outcomes. Subgroup analyses further indicate that older adults and individuals with obesity show pronounced risk reductions with Non-OPA, underscoring its accessibility for high-risk populations. In summary, PA is a key component of health promotion strategies, with potential benefits across diverse populations, particularly women, older adults, and those with obesity.
Data availability
The dataset used in this study is available from the National Health and Nutrition Examination Survey (NHANES) public website (https://www.cdc.gov/nchs/nhanes/).
References
Lee, D. H. et al. Long-Term Leisure-Time physical activity intensity and All-Cause and Cause-Specific mortality: A prospective cohort of US adults. Circulation 146 (7), 523–534. https://doi.org/10.1161/CIRCULATIONAHA.121.058162 (2022).
Leroux, A. et al. NHANES 2011–2014: objective physical activity is the strongest predictor of All-Cause mortality. Med. Sci. Sports Exerc. 56 (10), 1926–1934. https://doi.org/10.1249/MSS.0000000000003497 (2024).
Lee, I. M. et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 380(9838):219–229. PMID: 22818936 (2012).
Bull, F. C. et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54 (24), 1451–1462. https://doi.org/10.1136/bjsports-2020-102955 (2020).
Huang, W. T., Liu, C. Y., Hung, H. F., Hsu, S. P. & Chiou, A. F. Gender differences in factors associated with physical activity in patients with coronary artery disease. J. Cardiovasc. Nurs. 37 (4), 368–377. https://doi.org/10.1097/JCN.0000000000000804 (2022).
Bailly, M. et al. Systematic review of COVID-19-Related physical Activity-Based rehabilitations: benefits to be confirmed by more robust methodological approaches. Int. J. Environ. Res. Public. Health. 19 (15), 9025. https://doi.org/10.3390/ijerph19159025 (2022).
Ji, H. et al. Sex differences in association of physical activity with All-Cause and cardiovascular mortality. J. Am. Coll. Cardiol. 83 (8), 783–793. https://doi.org/10.1016/j.jacc.2023.12.019 (2024).
Millard, L. A. C., Tilling, K., Gaunt, T. R., Carslake, D. & Lawlor, D. A. Association of physical activity intensity and bout length with mortality: an observational study of 79,503 UK biobank participants. PLoS Med 18(9), e1003757. https://doi.org/10.1371/journal.pmed.1003757 (2021).
Lee, D. H. et al. Physical activity and all-cause and cause-specific mortality: assessing the impact of reverse causation and measurement error in two large prospective cohorts. Eur. J. Epidemiol. 36 (3), 275–285. https://doi.org/10.1007/s10654-020-00707-3 (2021).
Zhao, M., Veeranki, S. P., Magnussen, C. G. & Xi, B. Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ. ;370:m2031. (2020). https://doi.org/10.1136/bmj.m2031(2020).
Connelly, P. J. et al. The importance of gender to understand sex differences in cardiovascular disease. Can. J. Cardiol. 37 (5), 699–710. https://doi.org/10.1016/j.cjca.2021.02.005 (2021).
Kraus, W. E. et al. Physical activity, All-Cause and cardiovascular mortality, and cardiovascular disease. Med. Sci. Sports Exerc. 51 (6), 1270–1281. https://doi.org/10.1249/MSS.0000000000001939 (2019).
Coenen, P. et al. Associations of occupational and leisure-time physical activity with all-cause mortality: an individual participant data meta-analysis. Br. J. Sports Med. 58 (24), 1527–1538. https://doi.org/10.1136/bjsports-2024-108117 (2024).
Luo, M., Gupta, N., Holtermann, A., Stamatakis, E. & Ding, D. Revisiting the ‘physical activity paradox’ in a Chinese context: occupational physical activity and mortality in 142,302 urban working adults from the China kadoorie biobank study. Lancet Reg. Health West. Pac. 23, 100457. https://doi.org/10.1016/j.lanwpc.2022.100457 (2022).
Wang, Y., Nie, J., Ferrari, G., Rey-Lopez, J. P. & Rezende, L. F. M. Association of physical activity intensity with mortality: A National cohort study of 403 681 US adults. JAMA Intern. Med. 181 (2), 203–211. https://doi.org/10.1001/jamainternmed.2020.6331 (2021).
Arem, H. et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 175 (6), 959–967. https://doi.org/10.1001/jamainternmed.2015.0533 (2015).
Sun, J., Wu, H., Zhao, M., Magnussen, C. G. & Xi, B. Dose-response association of leisure time physical activity with mortality in adults with major chronic diseases. Front. Nutr. 9, 1048238. https://doi.org/10.3389/fnut.2022.1048238 (2022).
Lin, D. et al. Associations between Leisure-Time physical activity level and peripheral immune cell populations in the US general population, analysis of the National health and nutrition examination survey data, 1999–2018. Sports Med. Open. 9 (1), 101. https://doi.org/10.1186/s40798-023-00643-y (2023).
O’Donovan, G., Lee, I. M., Hamer, M. & Stamatakis, E. Association of weekend warrior and other leisure time physical activity patterns with risks for All-Cause, cardiovascular disease, and Cancer mortality. JAMA Intern. Med. 182 (5), 579. https://doi.org/10.1001/jamainternmed.2022.0668 (2022).
Dempsey, P. C. et al. Physical activity volume, intensity, and incident cardiovascular disease. Eur. Heart J. 43 (46), 4789–4800. https://doi.org/10.1093/eurheartj/ehac613 (2022).
Mu, X. et al. Associations of physical activity intensity with incident cardiovascular diseases and mortality among 366,566 UK adults. Int. J. Behav. Nutr. Phys. Act. 19 (1), 151. https://doi.org/10.1186/s12966-022-01393-y (2022).
Dos Santos, M. et al. Association of the weekend warrior and other Leisure-time physical activity patterns with All-Cause and Cause-Specific mortality: A nationwide cohort study. JAMA Intern. Med. 182 (8), 840–848. https://doi.org/10.1001/jamainternmed.2022.2488 (2022).
Khurshid, S., Al-Alusi, M. A., Churchill, T. W., Guseh, J. S. & Ellinor, P. T. Accelerometer-Derived weekend warrior physical activity and incident cardiovascular disease. JAMA 330 (3), 247–252. https://doi.org/10.1001/jama.2023.10875 (2023).
Jackson, J. L. et al. Gender differences in physical activity engagement among adolescents with congenital heart disease. J. Pediatr. Psychol. 47 (8), 859–869. https://doi.org/10.1093/jpepsy/jsab114 (2022).
Romero, S. A., Minson, C. T. & Halliwill, J. R. The cardiovascular system after exercise. J Appl Physiol ().122(4):925–932.).122(4):925–932. (1985). https://doi.org/10.1152/japplphysiol.00802 (2016).
Feng, H. et al. Associations of timing of physical activity with all-cause and cause-specific mortality in a prospective cohort study. Nat. Commun. 14 (1), 930. https://doi.org/10.1038/s41467-023-36546-5 (2023). Published 2023 Feb 18.
Marruganti, C. et al. Leisure-time and occupational physical activity demonstrate divergent associations with periodontitis: A population-based study. J. Clin. Periodontol. 50 (5), 559–570. https://doi.org/10.1111/jcpe.13766 (2023).
Tarp, J. et al. Leisure-time physical activity and all-cause mortality and cardiovascular disease in adults with type 2 diabetes: Cross-country comparison of cohort studies. J Sport Health Sci 13(2):212–221. https://doi.org/10.1016/j.jshs.2023.10.004(2024).
Temporelli, P. L. Is physical activity always good for you? The physical activity paradox. Eur. Heart J. Suppl. E168–E171. https://doi.org/10.1093/eurheartj/suab115 (2021). 23(Suppl E).
Holtermann, A., Schnohr, P., Nordestgaard, B. G. & Marott, J. L. The physical activity paradox in cardiovascular disease and all-cause mortality: the contemporary Copenhagen general population study with 104 046 adults. Eur. Heart J. 42 (15), 1499–1511. https://doi.org/10.1093/eurheartj/ehab087 (2021).
Tsai, J. et al. Exposure to secondhand smoke among nonsmokers -United states, 1988–2014. MMWR Morb Mortal. Wkly. Rep. 67 (48), 1342–1346. https://doi.org/10.15585/mmwr.mm6748a3 (2018).
Kleipool, R. P. et al. Difference in orientation of the Talar articular facets between healthy ankle joints and ankle joints with chronic instability. J. Orthop. Res. 40 (3), 695–702. https://doi.org/10.1002/jor.25068 (2022).
GBD et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med. 377(1):13–27. (2015). https://doi.org/10.1056/NEJMoa1614362(2017).
Liang, J. H. et al. Whether weekend warrior activity and other leisure-time physical activity pattern reduce the risk of depression symptom in the representative adults? A population-based analysis of NHANES 2007–2020. J Affect. Disord 340:329–339. https://doi.org/10.1016/j.jad.2023.07.113(2023).
O’Donovan, G. et al. Associations of the ‘weekend warrior’ physical activity pattern with all-cause, cardiovascular disease and cancer mortality: the Mexico City prospective study. Br. J. Sports Med. 58 (7), 359–365. https://doi.org/10.1136/bjsports-2023-107612 (2024).
Cao, C., Friedenreich, C. M. & Yang, L. Association of Daily Sitting Time and Leisure-Time Physical Activity With Survival Among US Cancer Survivors. JAMA Oncol. 8(3):395–403. PMID: 34989765 (2022).
Dsouza, N. et al. Exploring residents’ perceptions of neighborhood development and revitalization for active living opportunities. Prev. Chronic Dis. 19, E56. https://doi.org/10.5888/pcd19.220033 (2022).
Wang, Y., Nie, J., Ferrari, G., Rey-Lopez, J. P. & Rezende, L. F. M. Association of Physical Activity Intensity With Mortality: A National Cohort Study of 403 681 US Adults. JAMA Intern Med. 181(2):203–211. PMID: 33226432 (2021).
Garcia, L. et al. Non-occupational physical activity and risk of cardiovascular disease, cancer and mortality outcomes: a dose-response meta-analysis of large prospective studies. Br. J. Sports Med. 57 (15), 979–989. https://doi.org/10.1136/bjsports-2022-105669 (2023).
Zach, S., Fernandez-Rio, J., Zeev, A., Ophir, M. & Eilat-Adar, S. Physical activity, resilience, emotions, moods, and weight control, during the COVID-19 global crisis. Isr J Health Policy Res. 10(1):52. PMID: 34474685 (2021).
National Center for Health Statistics. NHANES Analytic Guidelines. Centers for Disease Control and Prevention. (2017–2018). Available from: https://www.cdc.gov/nchs/nhanes/analytic_guidelines.htm
Matthews, C. E. et al. Physical activity, sedentary behavior, and cause-specific mortality in black and white adults in the Southern community cohort study. Am. J. Epidemiol. 180 (4), 394–405. https://doi.org/10.1093/aje/kwu142 (2014).
Li, Y. et al. Television viewing time and the risk of colorectal Cancer mortality among Japanese population: the JACC study. Cancer Res. Treat. 53 (2), 497–505. https://doi.org/10.4143/crt.2020.327 (2021).
Farrahi, V. et al. Replacing sedentary time with physical activity and sleep: associations with cardiometabolic health markers in adults. Scand. J. Med. Sci. Sports. 33 (6), 907–920. https://doi.org/10.1111/sms.14323 (2023).
Marrie, R. A., Dawson, N. V. & Garland, A. Quantile regression and restricted cubic splines are useful for exploring relationships between continuous variables. J Clin Epidemiol. 62(5):511-7.e1. PMID: 19135859 (2009).
Stamatakis, E. et al. Vigorous intermittent lifestyle physical activity and Cancer incidence among nonexercising adults: the UK biobank accelerometry study. JAMA Oncol. 9 (9), 1255–1259. https://doi.org/10.1001/jamaoncol.2023.1830 (2023).
Mok, A., Khaw, K. T., Luben, R., Wareham, N. & Brage, S. Physical activity trajectories and mortality: population based cohort study. BMJ 365, l2323. https://doi.org/10.1136/bmj.l2323 (2019).
Posadzki, P. et al. Exercise/physical activity and health outcomes: an overview of Cochrane systematic reviews. BMC Public Health. 20(1):1724. PMID: 33198717 (2020).
Hunter, S. K., Angadi, S. & Bhargava, S. The biological basis of sex differences in athletic performance: consensus statement for the American college of sports medicine. Med. Sci. Sports Exerc. 55 (12), 2328–2360. https://doi.org/10.1249/MSS.0000000000003300 (2023).
Nuzzo, J. L. Sex differences in skeletal muscle fiber types: A meta-analysis. Clin. Anat. 37 (1), 81–91. https://doi.org/10.1002/ca.24091 (2024).
Beltrame, T., Villar, R. & Hughson, R. L. Sex differences in the oxygen delivery, extraction, and uptake during moderate-walking exercise transition. Appl. Physiol. Nutr. Metab. 42 (9), 994–1000. https://doi.org/10.1139/apnm-2017-0097 (2017).
Liang, W. et al. Effects of High-Intensity Interval Training on the Parameters Related to Physical Fitness and Health of Older Adults: A Systematic Review and Meta-Analysis. Sports Med Open. ;10(1):98. (2024). https://doi.org/10.1186/s40798-024-00767-9 (2024).
Yue, T., Wang, Y., Liu, H., Kong, Z. & Qi, F. Effects of High-Intensity Interval vs. Moderate-Intensity Continuous Training on Cardiac Rehabilitation in Patients With Cardiovascular Disease: A Systematic Review and Meta-Analysis. Front Cardiovasc Med. 9:845225. PMID: 35282360 (2022).
Zhang, L. et al. Bayesian compositional generalized linear mixed models for disease prediction using Microbiome data. BMC Bioinform. 26 (1), 98. https://doi.org/10.1186/s12859-025-06114-3 (2025).
Acknowledgements
We extend our heartfelt gratitude to all the participants and staff of the NHANES for their invaluable contributions and dedication.
Author information
Authors and Affiliations
Contributions
This study was conceptualized by A.H, Y.W, and L.Z; Data accessed and verified by A.H, Y.W; Methodology was designed by A.H, Y.W, C.D; Formal analysis were performed by A.H, the result verification was completed by Y.W, J.W and L.Z. The statistical method design was completed by Y.W, Z.L; The original draft of the writing was completed by A.H, and reviewed and edited by L.Z, C.D, Y.W, W.J, D.K, Y.Z, Z.L, H.C; L.Z, W.J and G.B provided supervision for this study. A.H and Y.W contributed equally to this work as first authors. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
He, A., Wang, Y., Du, C. et al. Sex differences in the association of physical activity patterns with all-cause and cardiovascular mortality: a prospective cohort study from NHANES 2007–2018. Sci Rep 15, 22197 (2025). https://doi.org/10.1038/s41598-025-06056-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06056-z
Keywords
This article is cited by
-
Sex Differences in the Impact of Physical Activity Across the Spectrum of Cardiovascular Disease
Current Cardiology Reports (2026)
